
Figure 2.
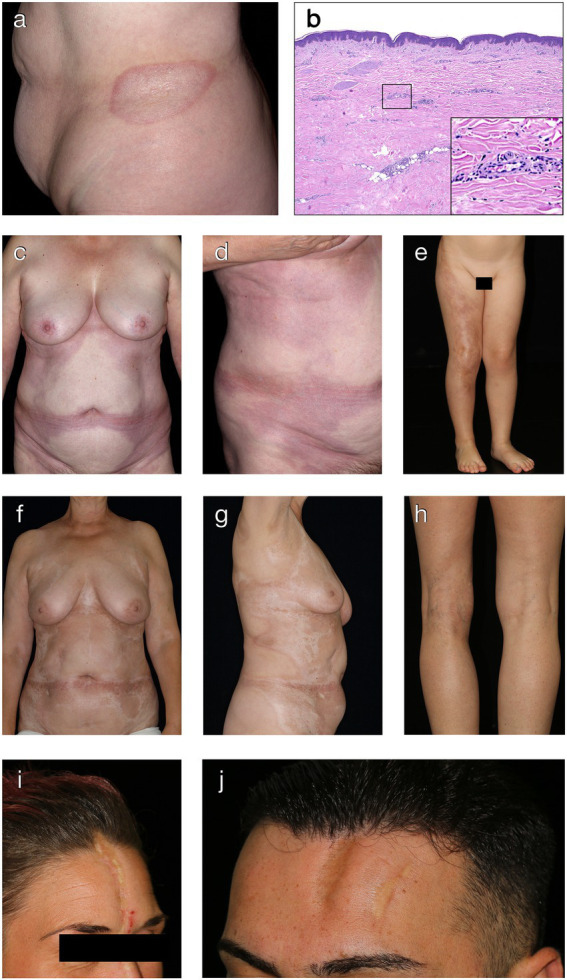
Clinical and histological hallmarks of morphea. (A) Well-defined oval patch with a central ivory white area surrounded by an erythematous violaceous rim (“lilac ring”) in a patient with plaque-type morphea. (B) The histology from a cutaneous biopsy from a sclerotic morphea lesion typically showing a thin epidermis, basal keratinocytes displaying pigment, scarce lymphocytic inflammatory infiltrates in the papillary dermis and around the vessels, with significant sclerosis in the reticular dermis and atrophy of the adnexal structures (H&E staining, 40×). Magnification displaying minimal periadnexal lymphocytic inflammatory infiltrates in the papillary dermis and thick, hyalinized, eosinophilic collagen bundles in the reticular dermis with entrapped atrophic adnexal structures (H&E staining, 200×). (C,D) Extensive, well-demarcated, coalescing erythematous violaceous patches on the trunk indicative of an early, inflammatory stage of generalized morphea. (E) Band-like, atrophic, hyperpigmented plaque in a blaschko-linear distribution in a child with linear morphea of the limb. (F,G) Ill-defined, coalescing, pink erythematous patches with important central sclerosis in a patient with generalized morphea, sclerotic disease stage. (H) Atrophy of the underlying tissue with asymmetry of the limbs in a patient with deep morphea. (I,J) Median and paramedian linear depressed, sclerotic plaques of morphea en coup de sabre with the presence of cicatricial alopecia.