

Abstract
STUDY QUESTION
What are the associations between baseline BMI (Study 1) and change in body weight (Study 2) with the likelihood of pregnancy in women with polycystic ovary syndrome (PCOS).
SUMMARY ANSWER
In women with PCOS, higher baseline BMI was associated with a lower chance of pregnancy; however, weight loss was associated with an increased chance of pregnancy versus maintaining a stable weight or gaining weight.
WHAT IS KNOWN ALREADY
Two studies in large cohorts of Danish women with the intention to become pregnant showed a decline in fecundability ratios with higher BMI. Furthermore, a meta-analysis found that overweight/obesity significantly worsened metabolic and reproductive outcomes in women with PCOS.
STUDY DESIGN, SIZE, DURATION
Data were extracted from the UK Clinical Practice Research Datalink GOLD database. Patients included women aged 18–45 years with BMI ≥18.5 (Study 1) or ≥25 kg/m2 (Study 2) at time of PCOS diagnosis (index date). The primary outcome was the time to first pregnancy recorded during 36-months’ follow-up, analysed with Cox proportional hazard models and presented as hazard ratios (HRs).
PARTICIPANTS/MATERIALS, SETTING, METHODS
Study 1 included 9955 women with PCOS. Study 2 included 7593 women with PCOS and median BMI of 34.0 kg/m2.
MAIN RESULTS AND THE ROLE OF CHANCE
Higher BMI was associated with a lower chance of pregnancy in the 3 years following diagnosis. It was estimated that 41% of women with normal weight (18.5–24.9 kg/m2) would become pregnant compared to 17% of women with obesity class III (BMI ≥40.0 kg/m2) during follow-up. Furthermore, the chance of pregnancy for women with obesity class III was estimated to be 63% lower than for women with normal weight, with the same age and glycaemic status (HR 0.37, 95% CI 0.31–0.44; P < 0.0001). A significant inverse association was found between BMI change and chance of pregnancy: 10% weight loss was estimated to increase the chance of pregnancy by 68% for women with baseline BMI of 40 kg/m2 (HR 1.68, 95% CI 1.49–1.90).
LIMITATIONS, REASONS FOR CAUTION
Multiple factors influence the chance of pregnancy (the ability and willingness to become pregnant), which was addressed by exclusion criteria employed. The real-world nature of the study means that use of non-prescription contraceptives was not available. Bias may have been introduced by the fact that only around 40% of women with PCOS in the CPRD GOLD database had their BMI recorded during the year prior to PCOS diagnosis. BMI categories used in the analyses may not be applicable to women of all ethnicities. The study population was only representative of women in the UK and results may not be generalizable to other regions. PCOS diagnoses were based on codes entered into the system by primary care providers, and no information was available regarding the criteria used for diagnosis, although symptoms used to diagnose PCOS have not changed over time.
WIDER IMPLICATIONS OF THE FINDINGS
Our observations provide further evidence of the benefits of weight loss in women with overweight/obesity and PCOS who are seeking to become pregnant.
STUDY FUNDING/COMPETING INTEREST(S)
Novo Nordisk A/S. A.H.B. declares fees for consultancy from Novo Nordisk. P.N.L. and C.L.H. are employees of Novo Nordisk. V.S. and A.V. are employees of, and hold shares in, Novo Nordisk.
TRIAL REGISTRATION NUMBER
N/A.
Keywords: polycystic ovary syndrome, BMI, fecundity, overweight, obesity, weight loss, pregnancy, cohort study
Introduction
Polycystic ovary syndrome (PCOS) is a common cause of infertility, predominantly due to a lack of regular ovulation (Balen et al., 2016). It is the most prevalent endocrine disorder among women of reproductive age, affecting 8–13% of premenopausal women, although estimates vary depending on the population studied and the diagnostic criteria used (Rotterdam ESHRE/ASRM-sponsored PCOS consensus workshop group, 2004; Bozdag et al., 2016; Skiba et al., 2018; Teede et al., 2018).
Several studies have demonstrated an association between obesity and increased time to pregnancy. For example, two studies in large cohorts of Danish women planning pregnancies reported an inverse relationship between increasing BMI and fecundability ratios, although PCOS diagnoses were not reported (Ramlau-Hansen et al., 2007; Wise et al., 2010).
It is estimated that between 38% and 88% of women with PCOS have overweight/obesity, depending on the demographics of the population studied (Barber et al., 2019). The association between PCOS and obesity is complex and is thought to include interactions between multiple factors (Barber et al., 2019). In a meta-analysis, overweight/obesity was shown to significantly worsen metabolic and reproductive outcomes in women with PCOS compared with their normal weight counterparts (Lim et al., 2013).
International guidelines recommend lifestyle modification, including weight management, as the first-line treatment for most women with PCOS and overweight/obesity, with or without infertility (Balen et al., 2016; Teede et al., 2018), as weight loss in women with PCOS has been shown to improve hyperandrogenism, reproductive function and metabolic parameters (Cena et al., 2020). While there is evidence on the impact of weight loss on improving fertility and outcomes in women with overweight/obesity (Legro et al., 2016; Best et al., 2017), it is challenging to conduct large studies that show clear clinical benefits (Lie Fong et al., 2021), and there is limited evidence on the effects of weight change on pregnancy rates in women with PCOS and overweight/obesity (Kim and Lee, 2022).
We performed a retrospective, real-world study in women with PCOS and overweight/obesity to evaluate the associations between (i) baseline BMI and chance of pregnancy, and (ii) body weight loss and chance of pregnancy.
Materials and methods
Study design and population
This was a retrospective cohort study of patient data extracted from the UK Clinical Practice Research Datalink (CPRD) GOLD database (January 2021 version; N = 19 483 855 research-acceptable patients; Clinical Practice Research Datalink, 2021). The CPRD GOLD database contains longitudinal anonymized data from routinely collected electronic health records (from September 1987 onwards) from a network of primary care practices across the UK maintained by the UK Government Medicines and Healthcare Products Regulatory Agency and the National Institute for Health Research (Clinical Practice Research Datalink, 2021). The data from the database were also linked to the Hospital Episode Statistics (HES) data for outpatient appointments (linkage set 18) to identify additional PCOS diagnoses made by specialists. PCOS diagnoses from GOLD were based on Read codes C164.00, C164.12, C165.00. PCOS diagnoses from HES were based on ICD-10 code E28.2.
The cohort included women aged 18–45 years at the index date (defined as the time of earliest PCOS diagnosis during the current registration period (the period starting from the latest date that a patient registered with a practice)) with a recorded BMI during the baseline period (the 12 months prior to the index date) of ≥18.5 kg/m2 (Study 1) and ≥25 kg/m2 (Study 2). Participants were excluded if they had an intrauterine contraceptive device, cancer, pregnancy or thyroid disorder (i.e. conditions that could affect body weight or study outcome) during the baseline period, or if they had a prescription for contraceptives or ovulation induction drugs at the index date.
This article follows the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) reporting guidelines for cohort studies.
Outcomes and assessments
Sociodemographic and clinical characteristics (including age, weight, BMI and smoking status (ever/never)) were extracted from the CPRD GOLD database.
The primary outcome in both Studies 1 and 2 was the time to first pregnancy recorded during 36-months’ follow-up, analysed with Cox proportional hazard models and presented as hazard ratios (HRs). More specifically, time to first recorded pregnancy was the input to our Cox proportional hazard models; the output comprised HRs reflecting the relative chance of pregnancy at a given time point when comparing two patients. The results presented are thus the relative chance of pregnancy. Data on time to first pregnancy were obtained from the CPRD GOLD Pregnancy Register, with the time of event defined by the recorded pregnancy start date. The exposure (or risk factor) in Study 1 was BMI at baseline, whereas in Study 2 the exposure was change in BMI from baseline, which was used as a measure of change in body weight.
Patient records were censored during follow-up at the time of the first of the following events: estimated start of pregnancy as per the pregnancy register; first prescription of contraceptives or ovulation-inducing drugs; at record end in the database; or after 36 months of follow-up. The mean BMI recorded during the baseline period was used as the mean baseline BMI and was also used to define baseline BMI category for analyses performed in Study 1.
In addition, baseline levels of high-density lipoprotein cholesterol, low-density lipoprotein cholesterol, total cholesterol, triglycerides, glycated haemoglobin and blood pressure were extracted for participants with a measurement recorded during the baseline period. In addition, data on ethnicity and socioeconomic status (represented by the 2010 English Index of Multiple Deprivation; UK Government Ministry of Housing, Communities & Local Government, 2010) were extracted from linked Hospital Episode Statistics data. These data were only available for a subset of practices in England that had consented to participate in the linkage scheme.
Statistical methods
Baseline sociodemographic and clinical characteristics were described using summary statistics.
In Study 1, two Cox proportional hazard models, with calendar time as the underlying time variable, were used to estimate the chance of pregnancy, including baseline BMI analysed either as a categorical or continuous variable, with results presented as HRs with 95% CIs. In the first model, baseline BMI was analysed as a categorical variable, using the World Health Organization categories: 18.5–24.9 kg/m2 (normal weight), 25.0–29.9 kg/m2 (overweight), 30.0–34.9 kg/m2 (obesity class I), 35.0–39.9 kg/m2 (obesity class II) and ≥40.0 kg/m2 (obesity class III). The ‘normal weight’ category was used as the reference. Additional covariates were: glycaemic status, included as a categorical variable (yes/no) based on the presence/absence of either prediabetes or diabetes, defined by a diabetes diagnosis (type 1 or type 2) or a baseline glycated haemoglobin level ≥6.0% (the lower threshold for prediabetes according to the UK National Institute for Health and Care Excellence); and a quadratic term for age at index date. A sensitivity analysis was performed in which other potential confounders—smoking status, ethnicity and socioeconomic status—were added to the model (conducted among the cohort of women with complete ethnicity and index of multiple deprivation data). The second model included baseline BMI as a continuous variable. Glycaemic status, quadratic terms for both BMI and age, and an interaction term between BMI and age were included as covariates.
In Study 2, a Cox proportional hazard model was used to evaluate the association between change in BMI and chance of pregnancy, with calendar time as the underlying time variable. Results are presented as HRs with 95% CIs. The main covariate was change in BMI relative to baseline BMI, modelled as a time-varying covariate. Additional covariates were: baseline BMI; glycaemic status; baseline age as a categorical variable based on four categories (18–24, 25–29 (reference age), 30–35 and 36–45 years); and an interaction term between the change in BMI and the baseline BMI.
In both studies, proportional hazards assumptions were verified via scaled Schoenfeld residuals for all models. Martingale residuals were calculated to test for non-linearity of continuous variables. The cumulative pregnancy rate was estimated using the Kaplan–Meier estimator. In both studies, the chance of pregnancy estimated by the Cox models is the chance of pregnancy observation in clinical practice and may be influenced by other confounders that were not possible to adjust for, such as willingness, action, ability to become pregnant and use of non-prescription contraceptives.
All statistical analyses were carried out using the R environment for statistical computing and visualization (version 4.1.0). No imputation for missing data was performed in any of the statistical analyses.
Role of the funding source
The funder designed the study and extracted and analysed the data. This article was drafted under the guidance of the authors, with medical writing and editorial support paid for by the funder.
Results
Patient demographics and characteristics
Study 1 cohort: evaluation of the association between BMI and chance of pregnancy
The Study 1 cohort included 9955 women with a median (quartile 1–quartile 3 (Q1–Q3)) age of 27 (22–31) years (Table I;Supplementary Table SI). Approximately 60% of women with a PCOS diagnosis within the appropriate timeframe for the study and who were aged 18–45 years, were excluded due to the absence of a recorded BMI measurement during the year prior to PCOS diagnosis (Supplementary Fig. S1). The median age in the obesity class III group was slightly higher than for those in the normal weight group (28 versus 26 years, respectively). At the time of PCOS diagnosis, 2068 (20.8%) women had overweight and 5525 (55.5%) had obesity. Median body weight (Q1–Q3) and median (Q1–Q3) BMI were 83.5 (67.9–102.0) kg and 31.2 (25.3–37.3) kg/m2, respectively.
Table I.
Baseline characteristics of the Study 1 (association between BMI and chance of pregnancy) and Study 2 (association between weight loss and chance of pregnancy) cohorts.
| Characteristics for total population |
Characteristics by BMI category (kg/m2) |
||||||
|---|---|---|---|---|---|---|---|
| Study 1 | Study 2 | ||||||
| Study 1 only | Studies 1 and 2 |
||||||
| Total N = 9955 | Total N = 7593 | Normal (18.5–24.9) N = 2362 | Overweight (25.0–29.9) N = 2068 | Obesity class I (30.0–34.9) N = 2129 | Obesity class II (35.0–39.9) N = 1768 | Obesity class III (≥40) N = 1628 | |
| Age, years | 27 (22–31) | 27 (23–32) | 26 (22–30) | 27 (23–31) | 26 (22–31) | 27 (22–32) | 28 (23–33) |
| Body weight, kg | 83.5 (67.9–102.0) | 91.8 (79.0–107.0) | 59.5 (55.0–64.0) | 73.6 (69.0–78.5) | 87.0 (82.0–93.0) | 101.6 (95.0–108.0) | 119.0 (110.0–129.7) |
| BMI, kg/m2 | 31.2 (25.3–37.3) | 34.0 (29.6–39.1) | 21.9 (20.5–23.5) | 27.5 (26.2–28.7) | 32.4 (31.2–33.6) | 37.2 (36.0–38.6) | 43.8 (41.5–46.8) |
| Ever smoked, n (%) | 4270 (42.9) | 3364 (44.3) | 906 (38.4) | 844 (40.8) | 919 (43.2) | 827 (46.8) | 774 (47.5) |
| Comorbidities, n (%) | |||||||
| Type 2 diabetes | 166 (1.7) | 160 (2.1) | 6 (0.3) | 10 (0.5) | 40 (1.9) | 44 (2.5) | 66 (4.1) |
| Diabetes or glycated haemoglobin ≥6.0% | 327 (3.3) | 292 (3.8) | 35 (1.5) | 41 (2.0) | 77 (3.6) | 74 (4.2) | 100 (6.1) |
| Hypertension | 430 (4.3) | 383 (5.0) | 47 (2.0) | 51 (2.5) | 81 (3.8) | 93 (5.3) | 158 (9.7) |
| Dyslipidaemia | 185 (1.9) | 167 (2.2) | 18 (0.8) | 35 (1.7) | 39 (1.8) | 47 (2.7) | 46 (2.8) |
| Asthma | 2144 (21.5) | 1736 (22.9) | 408 (17.3) | 404 (19.5) | 456 (21.4) | 434 (24.5) | 442 (27.1) |
| Median follow-up, months | 10.5 (3.2–31.2) | 12.0 (3.7–35.5) | 6.7 (2.2–19.0) | 8.3 (2.8–26.5) | 10.3 (3.2–31.0) | 14.1 (4.3–36.0) | 18.9 (6.7–36.0) |
| Pregnancy before index date, n (%) | 3167 (31.8) | 2581 (34.0) | 586 (24.8) | 680 (32.9) | 738 (34.7) | 587 (33.2) | 576 (35.4) |
| Contraceptives during 12 months prior to index date, n (%) | 3301 (33.2) | 2279 (30.0) | 1022 (43.3) | 811 (39.2) | 702 (33.0) | 468 (26.5) | 298 (18.3) |
| Metformin during 12 months prior to index date, n (%) | 578 (5.8) | 544 (7.2) | 34 (1.4) | 88 (4.3) | 130 (6.1) | 145 (8.2) | 181 (11.1) |
| Ethnicity* | n = 4506 | n = 3337 | n = 1169 | n = 994 | n = 943 | n = 754 | n = 646 |
| White, n (%) | 3989 (88.5) | 2954 (88.5) | 1035 (88.5) | 840 (84.5) | 814 (86.3) | 686 (91.0) | 614 (95.0) |
| South Asian, n (%) | 278 (6.2) | 208 (6.2) | 70 (6.0) | 82 (8.2) | 80 (8.5) | 32 (4.2) | 14 (2.2) |
| Black, n (%) | 150 (3.3) | 118 (3.5) | 32 (2.7) | 41 (4.1) | 34 (3.6) | 27 (3.6) | 16 (2.5) |
| East Asian, n (%) | 89 (2.0) | 57 (1.7) | 32 (2.7) | 31 (3.1) | 15 (1.6) | 9 (1.2) | 2 (0.3) |
| 2010 English IMD* | n = 5075 | n = 3740 | n = 1335 | n = 1127 | n = 1076 | n = 826 | n = 711 |
| IMD 1st quartile, n (%) | 1020 (20.1) | 672 (18.0) | 348 (26.1) | 239 (21.2) | 202 (18.8) | 134 (16.2) | 97 (13.6) |
| IMD 2nd quartile, n (%) | 1194 (23.5) | 857 (22.9) | 337 (25.2) | 269 (23.9) | 231 (21.5) | 206 (24.9) | 151 (21.2) |
| IMD 3rd quartile, n (%) | 1275 (25.1) | 960 (25.7) | 315 (23.6) | 271 (24.0) | 289 (26.9) | 212 (25.7) | 188 (26.4) |
| IMD 4th quartile, n (%) | 1586 (31.3) | 1251 (33.4) | 335 (25.1) | 348 (30.9) | 354 (32.9) | 274 (33.2) | 275 (38.7) |
IMD, Index of Multiple Deprivation. The 2010 English IMD is an overall measure of multiple deprivation at the area level in England (UK Government Ministry of Housing, Communities & Local Government, 2010). It is derived from several domains related to socioeconomic deprivation and is calculated as a weighted sum of the domain indices. The socioeconomic status of patients was determined by linking the postcode of their residence to the corresponding IMD (1st quartile: least deprived 4th quartile; most deprived). Data are presented as median (quartile 1–quartile 3) unless stated otherwise. *Data were not available for all patients; percentages represent the proportion among the cohort of patients with available data.
The median (Q1–Q3) follow-up time was 10.5 (3.2–31.2) months (median (Q1–Q3) index date: 16 August 2010 (12 October 2006–19 May 2014)). A total of 1720 (17.3%) women had a pregnancy recorded during the follow-up period (Supplementary Table SI). A higher median follow-up time was associated with a higher BMI category; median follow-up (Q1–Q3) was 6.7 (2.2–19.0) months in the normal weight category and 18.9 (6.7–36.0) months in the obesity class III category (Table I). The shorter mean follow-up time recorded in the normal BMI category compared with the obesity class I–III categories can be attributed to the higher rate of pregnancy and greater number of prescriptions for contraceptives among normal weight women versus those with obesity (Supplementary Table SI).
The prevalence of all comorbidities was generally low, apart from asthma recorded in 2144 (21.5%) women. There was an association between higher BMI categories and a higher prevalence of comorbidities (Table I). Analysis of available biomarker data showed a higher PCOS disease burden (lower high-density lipoprotein cholesterol, higher triglyceride levels and higher blood pressure) in higher BMI categories (Supplementary Table SII).
Smoking (ever) prior to the index date was recorded for 4270 (42.9%) women. The proportion of women who had ever smoked was highest in the obesity class III category (774/1628; 47.5%) and lowest in the normal weight category (906/2362; 38.4%) (Table I). Data on ethnicity and socioeconomic status were available for 4506 (45.3%) and 5075 (51.0%) women, respectively. Higher body weight categories were associated with lower socioeconomic status (Table I). The proportion of white women was lower in the normal weight category (1035/1169; 88.5%) than the obesity class III category (614/646; 95.0%).
Study 2: evaluation of the association between weight loss and chance of pregnancy
The Study 2 cohort included 7593 women with baseline BMI ≥25 kg/m2 from the Study 1 population (Table I, Supplementary Fig. S1). The demographics and characteristics of the Study 2 population were comparable to those of the Study 1 population, except for the expected greater baseline body weight and BMI, and slightly higher prevalence of comorbidities (Table I). In the Study 2 population, the median index date was 27 August 2010 and the median follow-up was 12.0 months (Q1–Q3: 3.7–35.5). Of these women, 1228 (16.3%) had a pregnancy during follow-up (Supplementary Fig. S1).
Association between BMI and chance of pregnancy (Study 1)
Supplementary Fig. S2 shows the proportion of women that became pregnant during the follow-up period by BMI at the time of PCOS diagnosis. The highest prevalence of pregnancies (>20%) was observed among women with a BMI of 22–28 kg/m2. The proportion of women with pregnancies was observed to be lower at higher BMI, with <10% of women with a BMI >45 kg/m2 becoming pregnant (Supplementary Fig. S2).
Kaplan–Meier analysis indicated that the cumulative proportion of women with pregnancies over the follow-up period was lower with higher BMI (Fig. 1). This analysis estimated that 41% of women with normal weight would become pregnant after 3 years of follow-up compared with 17% of women with class III obesity.
Figure 1.

Estimated cumulative incidence of pregnancies for women with polycystic ovary syndrome (PCOS) by BMI category in the with 3-year follow-up. Analysis performed using data from the Study 1 cohort (N = 9955), which was sampled to evaluate the association between BMI and chance of pregnancy. The cumulative pregnancy rate during follow-up of up to 3 years across the five BMI categories was estimated using the Kaplan–Meier method. The lines indicate the cumulative estimated mean proportion of patients with pregnancy. The shaded areas show the 95% CI.
The chance of pregnancy for a woman with BMI ≥40 kg/m2 was estimated to be 63% lower compared with a woman with normal weight of the same age and glycaemic status (HR 0.37, 95% CI 0.31–0.44; P < 0.0001) (Fig. 2). Age (as a quadratic term) significantly contributed to the model estimating the association between BMI category and chance of pregnancy (P < 0.0001), whereas glycaemic status did not (P = 0.066) (Fig. 2).
Figure 2.

Chance of pregnancy by baseline BMI category. Analysis performed using data from the Study 1 cohort (N = 9955), which was sampled to evaluate the association between BMI category and chance of pregnancy relative to normal weight. Diamonds indicate hazard ratios for pregnancy by baseline BMI categories, calculated using a Cox proportional hazard model. The horizontal lines indicate the 95% CIs. The model was adjusted for glycaemic status (diabetes or glycated haemoglobin ≥6.0%; HR 0.74, 95% CI 0.54–1.02; P = 0.066) and age as a quadratic term (HR 0.990, 95% CI 0.988–0.991; P < 0.0001). HR, hazard ratio.
Estimated chance of pregnancy across the range of ages at PCOS diagnosis (18–45 years) for the five BMI categories are shown in Figure 3, using a woman with normal weight aged 27 years at PCOS diagnosis as the reference. This figure illustrates the association between age and chance of pregnancy. For example, for a woman with obesity class II (BMI 35–39.9 kg/m2) aged 31 years at PCOS diagnosis, the chance of pregnancy was half that of a woman with normal weight aged 27 years but was similar to that for a woman with normal weight aged 35 years at diagnosis.
Figure 3.

Chance of pregnancy across the range of ages at polycystic ovary syndrome (PCOS) diagnosis by BMI category. Analysis performed using data from the Study 1 cohort (N = 9955), which was sampled to evaluate the association between BMI and chance of pregnancy. This plot shows the hazard ratios at different ages for the five BMI categories (18.5–24.9 kg/m2 (normal weight), 25.0–29.9 kg/m2 (overweight), 30.0–34.9 kg/m2 (obesity class I), 35.0–39.9 kg/m2 (obesity class II) and ≥40.0 kg/m2 (obesity class III)), as estimated by the Cox proportional hazard model, using women with normal BMI and an age of 27 at PCOS diagnosis as the reference. The plot allows identification of women with different ages and BMI categories who are estimated to have equal chance of pregnancy, as illustrated by the highlighted data points for women aged 35 years with normal weight and women aged 31 years with obesity class II.
In the sensitivity analysis (in which smoking status, ethnicity and socioeconomic status were added to the model, and the cohort was limited to women with full data for ethnicity and socioeconomic status (N = 4402)), the association between BMI category and chance of pregnancy was similar to that seen in the model for the full cohort (Supplementary Fig. S3).
When modelled as a continuous variable, a significant relationship between increasing BMI and decreasing chance of pregnancy was found (HR 0.96, 95% CI 0.95–0.97; P < 0.0001). The estimated chance of pregnancy for a woman with a BMI of 43 kg/m2 was half that for a woman with a BMI of 31 kg/m2 (Supplementary Fig. S4). Similarly, when modelled as a continuous variable, a significant relationship between age and chance of pregnancy was found (HR 0.990, 95% CI 0.988–0.991; P < 0.0001). The estimated chance for a woman aged 35 years was half that of a woman aged 27 years (Supplementary Fig. S4). Supplementary Fig. S5 illustrates the association between BMI, age, and chance of pregnancy from this model, as a 2D contour plot. For example, a 70% lower chance of pregnancy relative to a woman aged 27 years with a BMI of 22 kg/m2 was estimated for three combinations: age 39 years with BMI 22 kg/m2, age 33 years with BMI 40 kg/m2 and age 27 years with BMI 47 kg/m2.
Association between body weight change and chance of pregnancy (Study 2)
Among the 7593 patients with BMI ≥25 kg/m2, during follow-up 26.4% gained body weight, 26.0% lost weight and 56.5% had stable weight (no weight change recorded). Percentages sum to >100% as weight gain and loss groups are not mutually exclusive; some patients both gained and lost weight during follow-up.
A significant inverse association was found between change in body weight and chance of pregnancy (HR 0.96, 95% CI 0.95–0.97; P < 0.0001) (Supplementary Table SIII)—increase in body weight was associated with lower chance of pregnancy, while decrease in body weight was associated with an increased chance of pregnancy.
Significant associations were seen with baseline BMI, age, and chance of pregnancy (Supplementary Table SIII). Estimated HR for pregnancy for subgroups of patients with various categories of body weight change is shown in Fig. 4. A body weight gain of 5% after PCOS diagnosis was associated with a significantly decreased chance of pregnancy compared with no weight change, whereas weight losses of 5–15% after PCOS diagnosis were associated with an increased chance of pregnancy (Fig. 4). The impact of weight loss on the relative chance of pregnancy was more pronounced in patients with higher baseline BMI (Figs 4 and 5).
Figure 4.
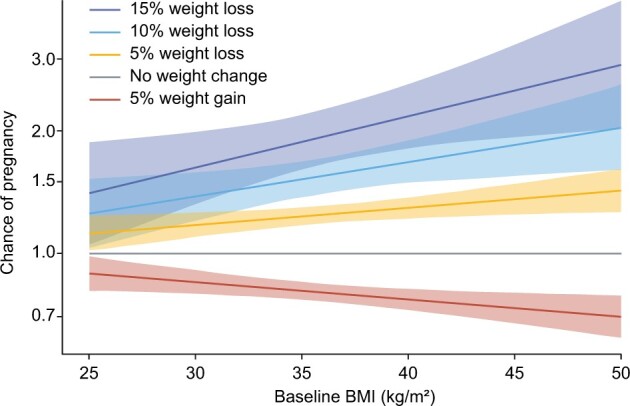
Chance of pregnancy for selected body weight changes by baseline BMI. Analysis performed using data from the Study 2 cohort (N = 7593), which was sampled to evaluate the association between weight loss and chance of pregnancy. The plot illustrates the chance of pregnancy, as estimated by the Cox proportional hazard model, across the full baseline BMI range for selected body weight changes (5% weight gain and 5%, 10% and 15% weight loss). The reference is stable weight (no weight change) as shown by the grey line. The estimated chance of pregnancy was calculated with the 95% CIs for each individual BMI value and visualized as continuous lines across the full range.
Figure 5.

Chance of pregnancy for selected body weight changes for three example baseline BMIs. Analysis performed using data from the Study 2 cohort (N = 7593), which was sampled to evaluate the association between weight loss and chance of pregnancy. The three plots illustrate the chance of pregnancy, as estimated by the Cox proportional hazard model, with 95% CI (shaded areas) for selected example baseline BMIs of 30, 40 and 50 kg/m2, relative to stable weight (no weight change), as depicted by the grey data point. These data represent a subset of the data reported in Figure 4. By assumption, the model prescribes a log-linear relationship between weight change and the chance of pregnancy, and due to this log-linear relationship, a straight line can be drawn through the point estimates at 5% weight gain and 5%, 10% and 15% weight loss.
Supplementary Fig. S6A illustrates the association between weight change, baseline BMI and chance of pregnancy from this model, as a 2D contour plot. For example, following a 10% weight loss, the chance of pregnancy for a woman with a baseline BMI of 45 kg/m2 was the same as for a woman with a BMI of 35 kg/m2 who maintained stable weight (Supplementary Fig. S6).
Discussion
This large, retrospective, cohort analysis investigated the association between BMI and the chance of pregnancy in women with PCOS and overweight/obesity. The results showed that higher BMI was associated with a lower chance of pregnancy, confirming the findings from earlier research. The present analysis also demonstrated that weight loss was associated with an increased chance of pregnancy compared with maintaining a stable weight or weight gain. There was a clear association between greater magnitude of weight loss and higher chance of pregnancy. Furthermore, the impact of weight loss on the relative chance of pregnancy appeared to be more pronounced in patients with higher baseline BMI, although it is important to note that the absolute chance of pregnancy is reduced at a higher BMI compared with a normal BMI.
There are multiple mechanisms by which obesity may impair reproductive health. Weight loss may improve fertility outcomes and increase the chance of a healthy pregnancy by mediating improvements in hormone profiles, ovulation rates, oocyte health, endometrial receptivity, insulin resistance and other metabolic parameters (Norman et al., 2004; Cena et al., 2020). Preclinical data suggest that obesity can affect the oocyte and preimplantation embryo, with disrupted spindle formation and mitochondrial function (Dunning et al., 2014; Wu et al., 2015; Broughton and Moley, 2017). Excess free fatty acids may also have a toxic effect in reproductive tissues, leading to cellular damage and chronic low-grade inflammation (Broughton and Moley, 2017). Adipose tissue also acts as an endocrine tissue, releasing adipokines that interact with multiple molecular pathways of insulin resistance and inflammation, leading to hypertension, increased coagulability and cardiovascular risk (Silvestris et al., 2018; Jafari-Gharabaghlou et al., 2021). Altered levels of adipokines, such as increased leptin, may affect the endometrium, leading to impaired stromal decidualization and placental abnormalities that may then result in miscarriage, stillbirth or preeclampsia (Jafari-Gharabaghlou et al., 2021).
Consistent with the results of the present study, several smaller studies have reported beneficial effects of weight loss on outcomes related to reproductive potential in women with PCOS and overweight/obesity (Tang et al., 2006; Legro et al., 2015, 2016). A previous study randomized women to: (i) continuous oral contraceptive pills, (ii) lifestyle modification to reduce weight (‘Lifestyle’) or (iii) both (‘Combined’; Legro et al., 2015). Those in both the Lifestyle and Combined groups achieved significant weight loss compared with the contraceptive pill arm of the study (P < 0.0001 for both), and greater cumulative ovulation rates per treatment cycle (P = 0.002 and P = 0.06 for Lifestyle and Combined, respectively; Legro et al., 2015). The number of live birth rates and pregnancies were insufficient to demonstrate a significant improvement in these parameters. A post hoc comparison analysis also demonstrated a benefit in delaying fertility treatment until after pre-treatment with lifestyle modification for weight loss (Legro et al., 2016). In a separate study in women with PCOS receiving advice on diet and exercise, with or without metformin, an improvement in menstrual regularity was observed in those who lost weight. Metformin use did not significantly improve weight loss or menstrual regularity versus placebo (Tang et al., 2006).
Interestingly, the present study found that in women with PCOS and overweight/obesity, achievement of weight loss was associated with a greater chance of pregnancy relative to maintaining stable weight, even when BMI at the end of follow-up was the same in those losing weight and those maintaining stable weight. For example, a 10% weight loss in a woman with baseline BMI of 45 kg/m2 (i.e. to 40.5 kg/m2) led to a greater chance of pregnancy than for a woman with a baseline BMI of 40.5 kg/m2 maintaining stable weight. The reasons for this are unknown but it may be that individuals may have different set points (or body weights) at which reproductive function may change and an improvement may enable a re-establishment of normal endocrine and metabolic pathways, even if BMI is still elevated.
While maternal complications and pregnancy outcomes were not evaluated in the present study, obesity is a known risk factor in the general population and among women with PCOS (Boomsma et al., 2008; Catalano and Shankar, 2017; Bahri Khomami et al., 2019a,b). Weight loss in women with PCOS and overweight/obesity may not only improve the chance of pregnancy, as found in this study but could also improve maternal health and pregnancy outcomes. Further studies are needed in this regard.
This was a cohort study with a large population and a real-world design based on data from electronic medical records representative of clinical practice. Pregnancy was the assessed endpoint, representing a definitive outcome, in contrast to earlier studies investigating the effect of weight loss on improvement in biomarkers associated with fertility and ovulation. Since weight management is a recommended first-line treatment for women with PCOS and obesity (Balen et al., 2016; Teede et al., 2018), it is likely that weight loss observed during the follow-up period was intentional. Furthermore, women achieving weight loss may have represented a subgroup trying harder to become pregnant than women maintaining stable weight, which could have influenced the results. Significant clinical differences associated with ethnicity have been observed in both PCOS phenotype and BMI (Wijeyaratne et al., 2013; Heymsfield et al., 2016; Engmann et al., 2017), with the South Asian population in the UK being notable for a greater metabolic disturbance than white counterparts (Wijeyaratne et al., 2013). In sensitivity analyses, ethnicity was not found to affect the association between BMI and chance of pregnancy, but these data were not available for all patients in the cohort.
The estimated rates of pregnancy over 36 months in our study were comparable to those previously reported over a 36-month period among women with likely PCOS (Collins et al., 1995). A long-term population-based study in Sweden found that the cumulative probability of childbirth (up to age 44 years) was similar in women with and without PCOS; however, women with PCOS had a longer time to first pregnancy and gave birth to fewer children than women without PCOS (Persson et al., 2019). Unfortunately, the latter study did not adjust for the effects of BMI and did not capture data on time from intention-to-conceive to first childbirth.
There are several limitations that should be noted. The main limitation of this study is that there are multiple factors influencing the chance of pregnancy, such as the ability and willingness to become pregnant. This was addressed by excluding women with intrauterine device use during the baseline period and censoring records at the time of a first prescription for contraceptives during the follow-up period; however, the real-world nature of our study means that information on factors such as sexual orientation and activity, relationship status, and the use of non-prescription contraceptives was not available to us. Bias may have been introduced by the fact that only around 40% of women with PCOS in the CPRD GOLD database had their BMI recorded during the year prior to PCOS diagnosis. Furthermore, the BMI categories used in the analyses may not be applicable to women of all ethnicities. The study population was only representative of women in the UK and therefore the results may not be generalizable to other regions. PCOS diagnoses were based on codes entered into the system by primary care providers, and no information was available regarding the criteria used for diagnosis. As the primary care database spanned three decades, the criteria and codes used for PCOS diagnosis may have changed over time. However, the symptoms used by primary care practitioners to diagnose PCOS have not changed over time, and any alterations in diagnostic codes will have applied equally to all BMI groups.
In conclusion, in this large cohort of women with PCOS and overweight/obesity from clinical practice, higher BMI was associated with lower chance of pregnancy. Furthermore, weight loss following PCOS diagnosis was associated with an increased chance of pregnancy compared with maintaining a stable weight or weight gain.
Supplementary Material
Acknowledgements
Medical writing support was provided by Beth Degg of Axis, a division of Spirit Medical Communications Group Limited, and funded by Novo Nordisk A/S, Denmark, in accordance with Good Publication Practice 3 (GPP3) guidelines (www.ismpp.org/gpp3).
Authors’ roles
All authors contributed to the study concept and design. V.S. received data from the CPRD for the purposes of this study and conducted statistical analyses. All authors had full access to all the data in the study and had final responsibility for the decision to submit for publication. All authors contributed to data interpretation and manuscript writing (assisted by a medical writer paid for by the funder), approved the final version of the manuscript and vouch for data accuracy.
Funding
This work was supported by Novo Nordisk A/S, Denmark.
Conflict of interest
A.H.B. declares fees for consultancy from Novo Nordisk. P.N.L. and C.L.H. are employees of Novo Nordisk. V.S. and A.V. are employees of, and hold shares in, Novo Nordisk.
Contributor Information
Christiane Lundegaard Haase, Novo Nordisk, Søborg, Denmark.
Anette Varbo, Novo Nordisk, Søborg, Denmark.
Peter Nørkjær Laursen, Novo Nordisk, Søborg, Denmark.
Volker Schnecke, Novo Nordisk, Søborg, Denmark.
Adam H Balen, Leeds Centre for Reproductive Medicine, Leeds Teaching Hospitals, Leeds, UK.
Data availability
This study is based on data from the Clinical Practice Research Datalink obtained under licence from the UK Medicines and Healthcare products Regulatory Agency. The data are provided by patients and collected by the UK National Health Service as part of their care and support. The interpretation and conclusions contained in this study are those of the author/s alone. Electronic health records are classified as ‘sensitive data’ by the UK Data Protection Act; therefore, information governance restrictions prevent data sharing via public deposition. Information about access to CPRD data are available here: https://www.cprd.com/research-applications (accessed on 13 June 2022).
References
- Bahri Khomami M, Joham AE, Boyle JA, Piltonen T, Arora C, Silagy M, Misso ML, Teede HJ, Moran LJ.. The role of maternal obesity in infant outcomes in polycystic ovary syndrome—a systematic review, meta-analysis, and meta-regression. Obes Rev 2019a;20:842–858. [DOI] [PubMed] [Google Scholar]
- Bahri Khomami M, Joham AE, Boyle JA, Piltonen T, Silagy M, Arora C, Misso ML, Teede HJ, Moran LJ.. Increased maternal pregnancy complications in polycystic ovary syndrome appear to be independent of obesity—a systematic review, meta-analysis, and meta-regression. Obes Rev 2019b;20:659–674. [DOI] [PubMed] [Google Scholar]
- Balen AH, Morley LC, Misso M, Franks S, Legro RS, Wijeyaratne CN, Stener-Victorin E, Fauser BCJM, Norman RJ, Teede H.. The management of anovulatory infertility in women with polycystic ovary syndrome: an analysis of the evidence to support the development of global WHO guidance. Hum Reprod Update 2016;22:687–708. [DOI] [PubMed] [Google Scholar]
- Barber TM, Hanson P, Weickert MO, Franks S.. Obesity and polycystic ovary syndrome: implications for pathogenesis and novel management strategies. Clin Med Insights Reprod Health 2019;13:1179558119874042. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Best D, Avenell A, Bhattacharya S.. How effective are weight-loss interventions for improving fertility in women and men who are overweight or obese? A systematic review and meta-analysis of the evidence. Hum Reprod Update 2017;23:681–705. [DOI] [PubMed] [Google Scholar]
- Boomsma CM, Fauser BC, Macklon NS.. Pregnancy complications in women with polycystic ovary syndrome. Semin Reprod Med 2008;26:72–84. [DOI] [PubMed] [Google Scholar]
- Bozdag G, Mumusoglu S, Zengin D, Karabulut E, Yildiz BO.. The prevalence and phenotypic features of polycystic ovary syndrome: a systematic review and meta-analysis. Hum Reprod 2016;31:2841–2855. [DOI] [PubMed] [Google Scholar]
- Broughton DE, Moley KH.. Obesity and female infertility: potential mediators of obesity's impact. Fertil Steril 2017;107:840–847. [DOI] [PubMed] [Google Scholar]
- Catalano PM, Shankar K.. Obesity and pregnancy: mechanisms of short term and long term adverse consequences for mother and child. BMJ 2017;356:j1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Cena H, Chiovato L, Nappi RE.. Obesity, polycystic ovary syndrome, and infertility: a new avenue for GLP-1 receptor agonists. J Clin Endocrinol Metab 2020;105:e2695–e2709. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Clinical Practice Research Datalink. CPRD GOLD January 2021 Dataset (Version 2021.01.001). 2021. 10.11581/V8HP-QA82 (13 June 2022, date last accessed) [dataset]. [DOI]
- Collins JA, Burrows EA, Wilan AR.. The prognosis for live birth among untreated infertile couples. Fertil Steril 1995;64:22–28. [PubMed] [Google Scholar]
- Dunning KR, Russell DL, Robker RL.. Lipids and oocyte developmental competence: the role of fatty acids and β-oxidation. Reproduction 2014;148:R15–R27. [DOI] [PubMed] [Google Scholar]
- Engmann L, Jin S, Sun F, Legro RS, Polotsky AJ, Hansen KR, Coutifaris C, Diamond MP, Eisenberg E, Zhang H. et al. ; Reproductive Medicine Network. Racial and ethnic differences in the polycystic ovary syndrome metabolic phenotype. Am J Obstet Gynecol 2017;216: 493.e1–493.e.13. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Heymsfield SB, Peterson CM, Thomas DM, Heo M, Schuna JM Jr. Why are there race/ethnic differences in adult body mass index-adiposity relationships? A quantitative critical review. Obes Rev 2016;17:262–275. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Jafari-Gharabaghlou D, Vaghari-Tabari M, Oghbaei H, Lotz L, Zarezadeh R, Rezaei YR, Ranjkesh M, Nouri M, Fattahi A, Nikanfar S. et al. Role of adipokines in embryo implantation. Endocr Connect 2021;10:R267–R278. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kim CH, Lee SH.. Effectiveness of lifestyle modification in polycystic ovary syndrome patients with obesity: a systematic review and meta-analysis. Life (Basel) 2022;12:308. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Legro RS, Dodson WC, Kris-Etherton PM, Kunselman AR, Stetter CM, Williams NI, Gnatuk CL, Estes SJ, Fleming J, Allison KC. et al. Randomized controlled trial of preconception interventions in infertile women with polycystic ovary syndrome. J Clin Endocrinol Metab 2015;100:4048–4058. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Legro RS, Dodson WC, Kunselman AR, Stetter CM, Kris-Etherton PM, Williams NI, Gnatuk CL, Estes SJ, Allison KC, Sarwer DB. et al. Benefit of delayed fertility therapy with preconception weight loss over immediate therapy in obese women with PCOS. J Clin Endocrinol Metab 2016;101:2658–2666. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Lie Fong S, Douma A, Verhaeghe J.. Implementing the international evidence-based guideline of assessment and management of polycystic ovary syndrome (PCOS): how to achieve weight loss in overweight and obese women with PCOS? J Gynecol Obstet Hum Reprod 2021;50:101894. [DOI] [PubMed] [Google Scholar]
- Lim SS, Norman RJ, Davies MJ, Moran LJ.. The effect of obesity on polycystic ovary syndrome: a systematic review and meta-analysis. Obes Rev 2013;14:95–109. [DOI] [PubMed] [Google Scholar]
- Norman RJ, Noakes M, Wu R, Davies MJ, Moran L, Wang JX.. Improving reproductive performance in overweight/obese women with effective weight management. Hum Reprod Update 2004;10:267–280. [DOI] [PubMed] [Google Scholar]
- Persson S, Elenis E, Turkmen S, Kramer MS, Yong E-L, Sundström-Poromaa I.. Fecundity among women with polycystic ovary syndrome (PCOS)— a population-based study. Hum Reprod 2019;34:2052–2060. [DOI] [PubMed] [Google Scholar]
- Ramlau-Hansen CH, Thulstrup AM, Nohr EA, Bonde JP, Sørensen TI, Olsen J.. Subfecundity in overweight and obese couples. Hum Reprod 2007;22:1634–1637. [DOI] [PubMed] [Google Scholar]
- Rotterdam ESHRE/ASRM-sponsored PCOS consensus workshop group. Revised 2003 consensus on diagnostic criteria and long‐term health risks related to polycystic ovary syndrome (PCOS). Hum Reprod 2004;19:41–47. [DOI] [PubMed] [Google Scholar]
- Silvestris E, de Pergola G, Rosania R, Loverro G.. Obesity as disruptor of the female fertility. Reprod Biol Endocrinol 2018;16:22. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Skiba MA, Islam RM, Bell RJ, Davis SR.. Understanding variation in prevalence estimates of polycystic ovary syndrome: a systematic review and meta-analysis. Hum Reprod Update 2018;24:694–709. [DOI] [PubMed] [Google Scholar]
- Tang T, Glanville J, Hayden CJ, White D, Barth JH, Balen AH.. Combined lifestyle modification and metformin in obese patients with polycystic ovary syndrome. A randomized, placebo-controlled, double-blind multicentre study. Hum Reprod 2006;21:80–89. [DOI] [PubMed] [Google Scholar]
- Teede HJ, Misso ML, Costello MF, Dokras A, Laven J, Moran L, Piltonen T, Norman RJ; International PCOS Network. Recommendations from the international evidence-based guideline for the assessment and management of polycystic ovary syndrome. Fertil Steril 2018;110:364–379. [DOI] [PMC free article] [PubMed] [Google Scholar]
- UK Government Ministry of Housing, Communities & Local Government. The English Indices of Deprivation 2010. 2010. https://www.gov.uk/government/statistics/english-indices-of-deprivation-2010 (13 June 2022, date last accessed).
- Wijeyaratne CN, Dilini Udayangani SA, Balen AH.. Ethnic-specific polycystic ovary syndrome: epidemiology, significance and implications. Expert Rev Endocrinol Metab 2013;8:71–79. [DOI] [PubMed] [Google Scholar]
- Wise LA, Rothman KJ, Mikkelsen EM, Sørensen HT, Riis A, Hatch EE.. An internet-based prospective study of body size and time-to-pregnancy. Hum Reprod 2010;25:253–264. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Wu LL, Russell DL, Wong SL, Chen M, Tsai TS, St John JC, Norman RJ, Febbraio MA, Carroll J, Robker RL.. Mitochondrial dysfunction in oocytes of obese mothers: transmission to offspring and reversal by pharmacological endoplasmic reticulum stress inhibitors. Development 2015;142:681–691. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Data Availability Statement
This study is based on data from the Clinical Practice Research Datalink obtained under licence from the UK Medicines and Healthcare products Regulatory Agency. The data are provided by patients and collected by the UK National Health Service as part of their care and support. The interpretation and conclusions contained in this study are those of the author/s alone. Electronic health records are classified as ‘sensitive data’ by the UK Data Protection Act; therefore, information governance restrictions prevent data sharing via public deposition. Information about access to CPRD data are available here: https://www.cprd.com/research-applications (accessed on 13 June 2022).