

Abstract
Nitric oxide can activate neutrophils and macrophages, facilitate the synthesis of collagen, which allows significantly accelerating the regeneration of traumatized tissues. We studied the effects of nitric oxide-containing gas flow generated by plasma-chemical device “Plason” in a rat model of full-thickness wounds. Histological and morphometric analyses revealed that Plason treated wounds expressed significantly fewer signs of inflammation and contained a more mature granulation tissue on day 4 after the operation. Considering the results of the experimental study, we applied the Plason device in sports medicine for the treatment of lower limb bruises of 34 professional soccer players. Athletes were asked to assess the intensity of pain with the Visual Analogue Scale. Girths of their lower limbs were measured over the course of rehabilitation. Nitric oxide therapy of full-thickness wounds inhibited inflammation and accelerated the regeneration of skin and muscle tissues. Compared with the control, we observed a significant reduction in pain syndrome on days 2–7 after injuries, edema, and hematoma, and shortened treatment duration. This pilot study indicates that the use of nitric oxide is a promising treatment method for sports injuries.
Keywords: contusion, gaseous nitric oxide, nitric oxide therapy, nitric oxide-containing gas flow, plasma-chemical nitric oxide generation, soccer, sportsports injury, therapy, wound healing
INTRODUCTION
Soccer is a full-contact sport with a large number of physical interactions between players during training and match plays. Union of European Football Associations reported that the incidence of injury was 8 injuries over 1000 hours of football related activities.1 The main types of injuries are sprains of muscles and ligaments, bruises and abrasions. However, even minor injuries may cause both physical and psychological discomfort and worsen the recovery process of the players. Therefore, it is extremely important to develop effective tools and methods to reduce the recovery time after bruises and abrasions.2,3,4,5,6,7
Nitric oxide (NO) is a gaseous signaling molecule produced by NO synthase.8 The discovery of its synthesis in the body was a major contribution to biology and medicine, for which F. Furchgott, L.J. Ignarro, and F. Murad were awarded the Nobel Prize in 1998. Numerous studies have demonstrated that NO signaling mediates physiological and pathophysiological processes in the body.9,10,11,12,13,14 NO promotes wound cleaning through the formation of peroxynitrite, deamination of DNA and S-nitrosirovanietiols on the surface of cell membranes, oxidative damage to DNA and lipid peroxidation.15,16,17,18,19 During the proliferation phase of wound healing, NO increases angiogenesis, and accelerates fibroblast proliferation, maturation and fibrotic transformation of granulation tissue.15,20,21,22,23
This discovery led to the creation of the air-plasma device “Plason” in 1998 by a group of scientists from the Bauman Moscow State Technical University and the Sechenov Moscow Medical Academy (currently, Sechenov University).24,25 This device forms an air-plasma flow enriched with NO from the atmospheric air, and allows local exposure bringing the necessary concentration of NO to the site of injury or other disease.26,27,28 Since 2000, the device manufactured by the company “CVTM at MSTU named After N. E. Bauman” has been supplied to medical organizations in Russian Federation, Ukraine, Belarus, Slovakia, etc. The main advantages of this device are: 1) possibility of producing NO in therapeutically significant concentrations,26,27,28 2) low content of side compounds (O3-, NO2, OH-, O-),26,27,28,29,30 and 3) the procedure is painless for patients, since the gas flow temperature is 25°C, which eliminates thermal damage to tissues and allows the faster delivery of NO to the damaged area.27
NO penetrates the skin, mucous membranes and cornea, which widens its range of applications to not only open, but also deep lesions.11,12 Plason has been used in practical medicine in purulent disease,31,32 abdominal surgery,33,34 maxillofacial surgery,35 military medicine,36 gynecology,37 ophthalmology,38 otolaryngology,39,40 dentistry41 and sports medicine,42 as well as in the treatment of post-radiation complications.43,44 Previously, it was shown the effectiveness of NO-therapy for the treatment of injuries to the tendons of the knee joint and Achilles tendon in athletes.42,45
Pathological tissue disorders associated with sports injuries, including soccer trauma (tissue necrosis, edema, impaired microcirculation, and hemorrhage with subsequent tissue regeneration), resemble tissue alterations occurring during wound healing.46,47
The NO-therapy provides mobile help, allowing it to be applied during training camp tours and competitions. The method is non-invasive, does not significantly affect the parameters determined by doping control, and has practically no contraindications. However, it is still to be investigated how exogenous NO impacts more severe sport-associated conditions including tendon ruptures and fractures. Hypothetically, the mobile and easy-to-use device can be overused in the field and cause misdiagnosis due to its pain revealing effect.
Considering this, we studied the impact of NO generated by Plason on the injury process in experimental cutaneous-muscular wounds, and subsequently, based on the experimental data, determined the effectiveness of NO-therapy in the treatment of sports injuries (bruises) in soccer players.
MATERIALS, PARTICIPANTS, AND METHODS
Ethics concern
The animal study was approved by the Local Ethics Committee of the Sechenov First Moscow State Medical University, Russian Federation (Protocol No. 15-19) on November 25, 2019 (Additional file 1 (120.6KB, pdf) ). All animal studies were conducted in full conformity with the International Guiding Principles for Biomedical Research Involving Animals (Geneva, 1990). The clinical study was conducted following the Declaration of Helsinki and was approved by the Clinical Research Ethics Committee of the Sechenov First Moscow State Medical University, Russian Federation (Protocol No. 02-20) on February 5, 2020 (Additional file 2 (238.6KB, pdf) ). All the individuals participating in the study expressed written informed consent (Additional file 3 (66.8KB, pdf) ).
Animal study
Modeling and intervention
The required number of animals was calculated with ClinCalc.com sample size calculator. Based on the preliminarily evaluated morphometry of control and Plason treated wounds, the required sample size was 5 with a confidence level of 95% and 5% margin of error. As an experimental model, a full-thickness skin wound was modeled in 15 male Wistar rats, weighing 160–180 g, with a bounding ring. Anesthesia was performed by intraperitoneal administration of a solution of Zoletil 100 (6 mg/kg; VIRBAC, Carros, France). In the inter-scapular space, a circle with a diameter of 18–20 mm was excised down to the muscle tissue. A Teflon ring (Center BMSTU, LLC, Moscow, Russian Federation) was implanted into the formed defect. The outer part of the ring was covered with a perforated plastic film (Chetak Packaging, Gujarat, India) with 20–25 perforations up to 0.5 mm in size, to prevent drying, contamination, and premature contraction of the injury. Injuries had a standard size of 3 cm2.
All the animals were randomly divided into three groups, with five rats in each group (Table 1). In the control group, the injuries were left without specific treatment for spontaneous healing. On days 1, 2, and 3 after the surgery, 60 seconds exposure group received anesthesia solution of Zoletil 100 intraperitoneally, the protective film was removed from the surface of the ring, after which the surface of the injuries was blown by NO-containing gas flow in a circular motion at a distance of 14 cm from the outlet of the manipulator of Plason (Figure 1) for 60 seconds. A similar procedure was performed in 120 seconds exposure group, and the wounds were blown for 120 seconds. Axial parameters of NO-containing gas flow were 1.68 (mg/s), 1200 ppm (NO), 130 ppm (NO2), 10.0 m/s and 280C.
Figure 1.

Operation set for NO therapy with Plason.
Note: NO: Nitric oxide.
Histological examination
On the 4th day after the injury, the animals were removed from the experiment and the injured tissues were taken for morphological analysis. The animals were anesthetized by intramuscular injection of a solution of Zoletil 100 (6 mg/kg body) and were euthanized by the injection of a solution of Zoletil 100 (60 mg/kg). The biological materials were fixed in 10% neutral formaldehyde and embedded in paraffin. Paraffin sections, 4–5 μm thick, were stained with hematoxylin and eosin (Cat# ab245880, Abcam, Cambridge, UK). The resulting microscopic images were examined with a universal microscope LEICA DM4000 B LED (Leica Microsystems, Wetzlar, Germany) equipped with digital video camera LEICA DFC7000 T (Leica Microsystems) by two experienced pathologists (AVB and ABS).
A semi-quantitative (score) method for evaluating morphological findings was used to objectify the results.22 In each sample, signs of inflammation (exudation, presence of bacterial colonies, inflammatory infiltration, microcirculation disorders) and regeneration (neoangiogenesis, fibroblast proliferation, prevalence, and maturity of granulation tissue) were evaluated on a 4-point scale: 0 – absence, 1 – low, 2 – medium, 3 – high, 4 – maximum severity. Morphometry was conducted by an independent blinded pathologist.
Clinical study
Study design
This interventional, single-centered, simple randomized, open-label, controlled, parallel-group study was carried out for a period of 1 year (March 2020 – May 2021).
Recruitment and treatment
The sample size was calculated with ClinCalc.com calculator. Based on the preliminarily evaluated morphometry of control and Plason treated wounds, the required sample size was 17 with a confidence level of 95% and 5% margin of error. The study included 34 professional soccer players (males, 22 ± 2.5 years) with the following anthropometric characteristics: height 180 ± 5.7 cm, weight 76 ± 3.7 kg, leg length 101.5 ± 4.8 cm, lower leg length 43.5 ± 2.4 cm, lower leg circumference 36.0 ± 1.7 cm. Inclusion criteria: lower leg bruises (harm score 2–3), admission of a sports doctor to participate in training and competitions, the rank is higher than the Candidate for Master of Sports, compliance with anti-doping rules. Exclusion criteria: the presence of open bleeding, hypotension, the presence of concomitant diseases, inability or disagreement to sign an informed consent.
Athletes were randomly divided into 2 groups, with 17 athletes in each. In group I, NO therapy and external medicines such as non-steroidal anti-inflammatory ointments and gels were prescribed. In group II, only the drugs were prescribed. The study included athletes with lower leg injuries sustained in collision with other players during the soccer match. All athletes had bruises on the shins.
All players had complaints: pain around the area of impact, accompanied by edema and limited function on the injured leg. When examining the area impacted by the collision, we observed hematomas on the player’s skin accompanied by edema of the injured segment of the lower limb and strongly marked soreness. Due to the bruises of the lower extremities and the exclusion of the risk of re-injury, the players were transferred to an individual training regime.
All athletes complained about pain in the lower leg after colliding with another player and had restricted movement associated with edema of soft tissues and ligamentous apparatus. On examination, there was a hematoma at the site of the injury, which was accompanied by rapidly increasing tissue edema.
Measurements
The intensity of pain was assessed with the Visual Analogue Scale (VAS) (Figure 2). Each athlete was asked to mark the area of injury which corresponded to the severity of pain. In current study, one centimeter corresponded to one point on the 0-to-10 scale.48
Figure 2.

Visual Analogue Scale applied to measure the intensity of pain.
Anthropometry of the lower limbs was performed to determine the dynamics of soft tissue edema. The measurement of lower leg girths was calculated as the arithmetic mean of five measurements of girths evenly distributed along the length of the corresponding segment of the lower limb.
The study excluded the athletes who showed signs of hypotension (below 100/50 mmHg when measuring blood pressure), which is a contraindication for NO therapy.
Treatment with plasma-chemical NO was performed at a distance of 14 cm from the output channel of the Plason device, with the flow moving along a concentric trajectory from the perifocal zone to the center of pain. The exposure time was 10–15 seconds/cm2. The procedure was performed once a day for 5 consecutive days. The sports doctor turned on the source of air-plasma flow, held the manipulator in his hand, and blew the injured area, focusing on the sensations that occurred during the procedure. NO was applied to both the affected and unaffected skin along the main vessels of the lower leg.
The criteria for stopping the treatment were the complete disappearance of pain, visual and palpatory indicators, and finally, admission to the general training group.
Statistical analysis
Statistical analysis of experimental data was performed using the standard software package GraphPad Prism version 8.00 for Windows (GraphPad Software, Inc., San Diego, CA, USA). Normal distribution of quantitative data (sum of inflammation points, sum of regeneration points) was checked using the Shapiro-Wilk’s test for the normality of the distribution. The intergroup differences were analyzed using the Kruskal-Wallis test with Dunn’s correction (for abnormally distributed data). The results were presented as boxes with whiskers with 95% confidence intervals. The significant level of P differences was estimated at < 0.05.
Statistical analysis of pain intensity and anthropometrical measurements was conducted with Student’s t-test. The results were presented as linear graphs with mean values and 95% confidence intervals.
RESULTS
NO therapy promotes the repair of skin and muscle injuries in rats
In the control group, the injured surface was covered with a fairly thick fibrin clot. Microvascular disorders were vividly expressed in the underlying tissue: stasis, erythrocyte sludge, hemorrhages. The number of fibroblasts was small, the cells were arranged in a disordered manner. In the centers of immature granulation tissue, collagen fibers were almost completely absent (Figure 3A).
Figure 3.

Effect of nitric oxide therapy on the repair of skin and muscle injuries in rats.
Note: (A–C) Morphological observation of wound tissue samples (hematoxylin and eosin staining). (A) Control group: Thick fibrin clot (arrow), immature granulation tissue with hemorrhage foci (*). (B) 60 seconds exposure group: Moderately mature granulation tissue with lymphocyte and macrophage infiltration (*) and moderate fibroblast proliferation. (C) 120 seconds exposure group: A large number of newly formed capillaries (*), an increase in the number of fibroblasts and collagen fibers, and the partial fibrosis of granulation tissue (arrow). Scale bars: 100 μm. (D) Morphological scores. Data are expressed as mean ± 95% confidence interval (n = 5). *P < 0.05 (Kruskal-Wallis test).
In the 60 seconds exposure group, the thickness of the fibrin clot differed insignificantly from the control group. In the underlying tissues, there was a moderate infiltration with lymphocytes, macrophages, and singular neutrophils. Granulation tissue occupied a larger area than in the control group. It consisted of longitudinally arranged fibroblasts and chaotically arranged capillaries, in some places consisting of disordered fibroblasts (Figure 3B).
In the 120 seconds exposure group, the fibrin clot was much less pronounced than in the control group. Fibrin was loosely oriented, and the total number of infiltrating cells was relatively small. There was a relatively thick layer of granulation tissue between the adipose tissue and the fibrin clot. Its maturity was much more pronounced than in the control, the volume was also increased. Most fibroblasts were oriented along the wound surface, the content of collagen fibers was increased, and there were almost no signs of microcirculation disorders (Figure 3C).
Figure 3D showed a decrease in the severity of signs of inflammation (the maximum total score of signs was 6 and 8, respectively) in 120 seconds exposure group compared with the control group, where the maximum total scores of inflammation and regeneration were 13 and 6 (P < 0.05). There were no significant differences between 60 and 120 seconds exposure groups.
NO-therapy promotes the repair of bruises in soccer players
NO-therapy accelerated resorption of hematoma and removal of edema in athletes of the experimental group compared with the control group. Figure 4 shows that the intensity of pain decreased significantly in the control and experimental groups. At the same time, in the experimental group using NO-therapy, recovery was faster (P < 0.05). On the 4th day, the players of the experimental group began the training process in the general group with minor restrictions, from the fifth day they trained without restrictions. The control group players on average started the training process with restrictions in 45 minutes in the general group on the 6th day and resumed the entire training process on the 7th day after the injury.
Figure 4.
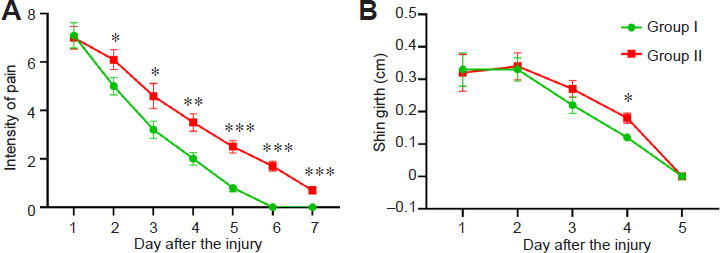
Effect of nitric oxide therapy on the repair of bruises in soccer players.
Note: (A) Visual Analogue Scale. (B) Dynamics in the average value of the shin girth after injury. Data are expressed as mean ± 95% confidence interval (n = 17). *P < 0.05, **P < 0.01, ***P < 0.001, vs. group I (Student's t-test).
During the study, there were no signs of hypotension in the examined athletes.
DISCUSSION
In the present study, we treated sports traumas of soccer players with exogenous NO. The observed beneficial clinical effects of NO-therapy are based on mechanisms that are universal for a wide range of pathologies.21,38,49 Activation of NO-related signaling pathways accelerates regenerative processes and inhibits inflammation27 A key observation that combines experimental and clinical research is a significant shortening of the duration of wound healing and rehabilitation of injured athletes. This period was reduced from 7 days to 4–5 days. The impact of NO-containing gas flows on patients’ well-being is majorly associated with the elimination of edema, hemorrhages and necrosis.
The obtained results show exogenous NO treatment to be a promising tool in athletic health care assistance. However, a detailed study of the mechanisms of action of exogenous NO in sport traumas, the development of indications and contraindications for its use in athletes, the testing of therapeutic modalities in different disciplines should be the subject of further research.
The limitation of the present study was the choice of only one regime of NO-therapy. We previously demonstrated that the effectiveness of exogenous NO application in the acceleration of wound healing is dose-dependent.22 These correlations will be studied in our future research. It is important to emphasize that the reported effects were achieved with the Plason device and could differ from other commercial and experimental air-plasma generators since they vary in construction design and gas composition, especially in NO concentration.
The application of a NO-containing gas flow produced by the Plason device for the treatment of skin and muscle injuries in the experiment normalized microvascular disorders, activated the lymph-macrophage reaction, accelerated the transition of the inflammatory phase of the wound process to the proliferative phase, enhanced angiogenesis, fibroblast proliferation, and collagen fibrogenesis. These results made it possible to apply NO-therapy for the treatment of lower limb contusions in soccer players. The effectiveness of treatment has been proven by accelerating the reduction and disappearance of pain, edema and hematoma, reducing the duration of rehabilitation in comparison with the use of exclusively external anti-inflammatory drugs. NO-therapy has a vast unexplored potential in sports injuries.
Additional files
Additional file 1 (120.6KB, pdf) : Animals study ethics approval (Russian).
Additional file 2 (238.6KB, pdf) : Hospital ethics approval (Russian).
Additional file 3 (66.8KB, pdf) : Informed consent form (Russian).
Footnotes
Funding: This work was supported by the Ministry of Science and Higher education of Russian Federation within the framework of state support for the creation and development of World-Class Research Centers “Digital Biodesign and Personalized Healthcare” (N. 075-15-2020-926).
Conflicts of interest
The authors declare no conflict of interest.
Availability of data and materials
All data generated or analyzed during this study are included in this published article and its supplementary information files.
REFERENCES
- 1.Ekstrand J, Hägglund M, Waldén M. Injury incidence and injury patterns in professional football: the UEFA injury study. Br J Sports Med. 2011;45:553–558. doi: 10.1136/bjsm.2009.060582. [DOI] [PubMed] [Google Scholar]
- 2.DeKosky ST, Ikonomovic MD, Gandy S. Traumatic brain injury--football, warfare, and long-term effects. N Engl J Med. 2010;363:1293–1296. doi: 10.1056/NEJMp1007051. [DOI] [PubMed] [Google Scholar]
- 3.Milenković D. Speed as an important component of football game. Acta Kinesiol. 2011;4:57–61. [Google Scholar]
- 4.Woods C, Hawkins R, Hulse M, Hodson A. The Football Association Medical Research Programme: an audit of injuries in professional football-analysis of preseason injuries. Br J Sports Med. 2002;36:436–441. doi: 10.1136/bjsm.36.6.436. discussion 441. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Hawkins RD, Hulse MA, Wilkinson C, Hodson A, Gibson M. The association football medical research programme: an audit of injuries in professional football. Br J Sports Med. 2001;35:43–47. doi: 10.1136/bjsm.35.1.43. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Dvorak J, Junge A. Football injuries and physical symptoms. A review of the literature. Am J Sports Med. 2000;28:S3–9. doi: 10.1177/28.suppl_5.s-3. [DOI] [PubMed] [Google Scholar]
- 7.Kalinin EM, Vlasov AE, Paniko VV, Chigirintseva OV. Elite footballer’s competitive performance rating criteria. Theory Pract Phys Cult. 2019:26. [Google Scholar]
- 8.Gluvic ZM, Obradovic MM, Sudar-Milovanovic EM, et al. Regulation of nitric oxide production in hypothyroidism. Biomed Pharmacother. 2020;124:109881. doi: 10.1016/j.biopha.2020.109881. [DOI] [PubMed] [Google Scholar]
- 9.Vodovotz Y, Barccellos-Hoff MH. Basel: Birkhäuser Basel; 2001. Direct and indirect modulation of the inducible nitric oxide synthase by nitric oxide: feedback mechanisms in inflammation. In: Salvemini D, Billiar TR, Vodovotz Y, eds. Nitric Oxide and Inflammation; pp. 41–58. [Google Scholar]
- 10.Muhl H, Dinarello CA. Cytokine regulation of nitric oxide production. In: Fang FC, editor. Kluwer Academic Plenum Publishers; 1999. [Google Scholar]
- 11.Moncada S, Higgs EA. Endogenous nitric oxide: physiology, pathology and clinical relevance. Eur J Clin Invest. 1991;21:361–374. doi: 10.1111/j.1365-2362.1991.tb01383.x. [DOI] [PubMed] [Google Scholar]
- 12.Förstermann U, Sessa WC. Nitric oxide synthases: regulation and function. Eur Heart J. 2012;33:829–837. doi: 10.1093/eurheartj/ehr304. 837a-837d. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Han G, Nguyen LN, Macherla C, et al. Nitric oxide-releasing nanoparticles accelerate wound healing by promoting fibroblast migration and collagen deposition. Am J Pathol. 2012;180:1465–1473. doi: 10.1016/j.ajpath.2011.12.013. [DOI] [PubMed] [Google Scholar]
- 14.Wan X, Liu S, Xin X, et al. S-nitrosated keratin composite mats with NO release capacity for wound healing. Chem Eng J. 2020;400:125964.. [Google Scholar]
- 15.Witte MB, Barbul A. Role of nitric oxide in wound repair. Am J Surg. 2002;183:406–412. doi: 10.1016/s0002-9610(02)00815-2. [DOI] [PubMed] [Google Scholar]
- 16.Ridnour LA, Thomas DD, Mancardi D, et al. The chemistry of nitrosative stress induced by nitric oxide and reactive nitrogen oxide species. Putting perspective on stressful biological situations. Biol Chem. 2004;385:1–10. doi: 10.1515/BC.2004.001. [DOI] [PubMed] [Google Scholar]
- 17.Yur’eva OV, Dubrovina VI, Potapov VA, et al. Immunotropic properties of an experimental synthetic selenium-organic compound. Bull Exp Biol Med. 2020;169:40–42. doi: 10.1007/s10517-020-04819-4. [DOI] [PubMed] [Google Scholar]
- 18.Schwentker A, Vodovotz Y, Weller R, Billiar TR. Nitric oxide and wound repair: role of cytokines? Nitric Oxide. 2002;7:1–10. doi: 10.1016/s1089-8603(02)00002-2. [DOI] [PubMed] [Google Scholar]
- 19.Thomas DD, Heinecke JL, Ridnour LA, et al. Signaling and stress: The redox landscape in NOS2 biology. Free Radic Biol Med. 2015;87:204–225. doi: 10.1016/j.freeradbiomed.2015.06.002. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Malone-Povolny MJ, Maloney SE, Schoenfisch MH. Nitric oxide therapy for diabetic wound healing. Adv Healthc Mater. 2019;8:e1801210. doi: 10.1002/adhm.201801210. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Thomas DD, Ridnour LA, Isenberg JS, et al. The chemical biology of nitric oxide: implications in cellular signaling. Free Radic Biol Med. 2008;45:18–31. doi: 10.1016/j.freeradbiomed.2008.03.020. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Shekhter AB, Pekshev AV, Vagapov AB, et al. Dose-dependent effect of plasma-chemical NO-containing gas flow on wound healing. An experimental study. Clin Plasma Med. 2020:100101, 19–20. [Google Scholar]
- 23.Afzali H, Khaksari M, Norouzirad R, Jeddi S, Kashfi K, Ghasemi A. Acidified nitrite improves wound healing in type 2 diabetic rats: Role of oxidative stress and inflammation. Nitric Oxide. 2020;103:20–28. doi: 10.1016/j.niox.2020.07.001. [DOI] [PubMed] [Google Scholar]
- 24.Shekhter AB, Kabisov RK, Pekshev AV, Kozlov NP, Perov YL. Experimental and clinical validation of plasmadynamic therapy of wounds with nitric oxide. Bull Exp Biol Med. 1998;126:829–834. [PubMed] [Google Scholar]
- 25.Kabisov R, Sokolov VV, Shekhter A, Pekshev A, Maneylova M. Experience in application of exogenous NO therapy for treatment of postoperative wounds and radioreactions in oncological patients. Russ Oncol J. 2000:24–29. [Google Scholar]
- 26.Pekshev AV, Shekhter AB, Vagapov AB, Sharapov NA, Vanin AF. Study of plasma-chemical NO-containing gas flow for treatment of wounds and inflammatory processes. Nitric Oxide. 2018;73:74–80. doi: 10.1016/j.niox.2017.06.002. [DOI] [PubMed] [Google Scholar]
- 27.Shekhter AB, Pekshev AV, Vagapov AB, et al. Physicochemical parameters of NO-containing gas flow affect wound healing therapy. An experimental study. Eur J Pharm Sci. 2019;128:193–201. doi: 10.1016/j.ejps.2018.11.034. [DOI] [PubMed] [Google Scholar]
- 28.Shekhter AB, Serezhenkov VA, Rudenko TG, Pekshev AV, Vanin AF. Beneficial effect of gaseous nitric oxide on the healing of skin wounds. Nitric Oxide. 2005;12:210–219. doi: 10.1016/j.niox.2005.03.004. [DOI] [PubMed] [Google Scholar]
- 29.Heuer K, Hoffmanns MA, Demir E, et al. The topical use of non-thermal dielectric barrier discharge (DBD): nitric oxide related effects on human skin. Nitric Oxide. 2015;44:52–60. doi: 10.1016/j.niox.2014.11.015. [DOI] [PubMed] [Google Scholar]
- 30.Duchesne C, Banzet S, Lataillade JJ, Rousseau A, Frescaline N. Cold atmospheric plasma modulates endothelial nitric oxide synthase signalling and enhances burn wound neovascularisation. J Pathol. 2019;249:368–380. doi: 10.1002/path.5323. [DOI] [PubMed] [Google Scholar]
- 31.Marakhonich LA, Bordenyuk VI, Pekshev AV, Vagapov AB. Effective clinical use of no-containing gas flow generated by air-plasma in outpatient settings. Ambul Surg. 2016:97–101. [Google Scholar]
- 32.Vyrenkov Y, Esipov A, Musalinov V. The application of nitrogen oxide in the surgical practice. Russ J Physiother Balneol Rehabil. 2014;13:33–40. [Google Scholar]
- 33.Achkasov EE, Esipov AV, Pekshev AV, Musailov VA. Use of an exogenous nitric oxide generator for treatment of peritonitis. Biomed Eng. 2018;52:64–67. [Google Scholar]
- 34.Suzdaltsev I, Pykhtin Y, Pusty S, Panchenko A, Minaev S. Clinical and laboratory assessment of Nitric Oxide-containing gas flow application in programmed laparosanizations in patients with advanced purulent peritonitis. Med Bull North Caucasus. 2017;12:401–403. [Google Scholar]
- 35.Maltsev P, Zhuravlev V, Darwin V. The application of Nitric Oxide in minimally invasive surgical treatment of abscesses and phlegmon of soft tissues of the maxillofacial region. Bull Smolensk State Med Acad. 2010;9:93–95. [Google Scholar]
- 36.Marakhonich L, Moskalenko V, Bespalko V. Comparative evaluation of the biological effect of physical plasma energy on the course of the wound process in a soft-tissue and musculoskeletal gunshot wound: materials of the All-Russian scientific. Mater All-Russian Sci Conf SPb. 1998:54–55. [Google Scholar]
- 37.Davydov A, Kuchukhidze S, Shekhter A, Khanin A, Pekshev A. Clinical evaluation of intraoperative application of air-plasma flow enriched with Nitric Oxide in operations on the uterus and its appendages. Quest Gynecol Obstet Perinatol. 2004;3:12–17. [Google Scholar]
- 38.Kvasha O, Bykov V, Sinelshchikova I, Borhanov A, Al-Daravish D. NO-therapy in the complex treatment of burn conjunctival ischemia (clinical studies) J Media Al. 2013;3:12–17. [Google Scholar]
- 39.Nosova O. Treatment of inflammatory middle ear diseases with exogenous nitrogen oxide. Clin Med Alm. 2010:25–28. [Google Scholar]
- 40.Svistushkin V, Shevchik E, Rogatkin D, et al. The application of NO-therapy in the early stages after tympanoplasty. Clin Med Alm. 2010:68–73. [Google Scholar]
- 41.Osipyan E, Gandylyan K. The effectiveness of the complex treatment of patients with osteomyelitis of the lower jaw of odontogenic or traumatic origin (Clinical and experimental study) Med Bull North Caucasus. 2008;12:43–46. [Google Scholar]
- 42.Zaborova V, Seluyanov V. Exogenous nitric oxide in the treatment of ligaments of the knee joint and achilles tendon tendonitis in athletes. Sport Adapt Lab. 2020 [Google Scholar]
- 43.Kabisov R, Sokolov V, Shekhter A, Pekshev A, Maneylova M. The first experience of exogenous NO-therapy for the treatment of postoperative wounds and radiation reactions in cancer patients. Russ Oncol J. 2000;1:24–29. [Google Scholar]
- 44.Reshetov I, Kabisov R, Kravtsov S.O.M. In coll. “NO-therapy: theoretical aspects, clinical experience and problems of the use of exogenous nitric oxide in medicine.”. Publ House; 2001. Features of the clinical application of air-plasma Plason device for reconstructive plastic surgery in oncology; pp. 74–76. [Google Scholar]
- 45.Maffulli N, Longo UG, Kadakia A, Spiezia F. Achilles tendinopathy. Foot Ankle Surg. 2020;26:240–249. doi: 10.1016/j.fas.2019.03.009. [DOI] [PubMed] [Google Scholar]
- 46.Xiao W, Liu Y, Chen P. Macrophage depletion impairs skeletal muscle regeneration: the roles of pro-fibrotic factors, inflammation, and oxidative stress. Inflammation. 2016;39:2016–2028. doi: 10.1007/s10753-016-0438-8. [DOI] [PubMed] [Google Scholar]
- 47.Zheng L, Liu X, Chen P, Xiao W. Expression and role of lncRNAs in the regeneration of skeletal muscle following contusion injury. Exp Ther Med. 2019;18:2617–2627. doi: 10.3892/etm.2019.7871. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 48.Huskisson EC. Measurement of pain. Lancet. 1974;2:1127–1131. doi: 10.1016/s0140-6736(74)90884-8. [DOI] [PubMed] [Google Scholar]
- 49.Osipyan E, Gandylyan K. The effectiveness of the complex treatment of patients with osteomyelitis of the lower jaw of odontogenic or traumatic origin (Clinical and experimental study) Med Bull North Caucasus. 2008;12:43–46. [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.