
Figure 1.
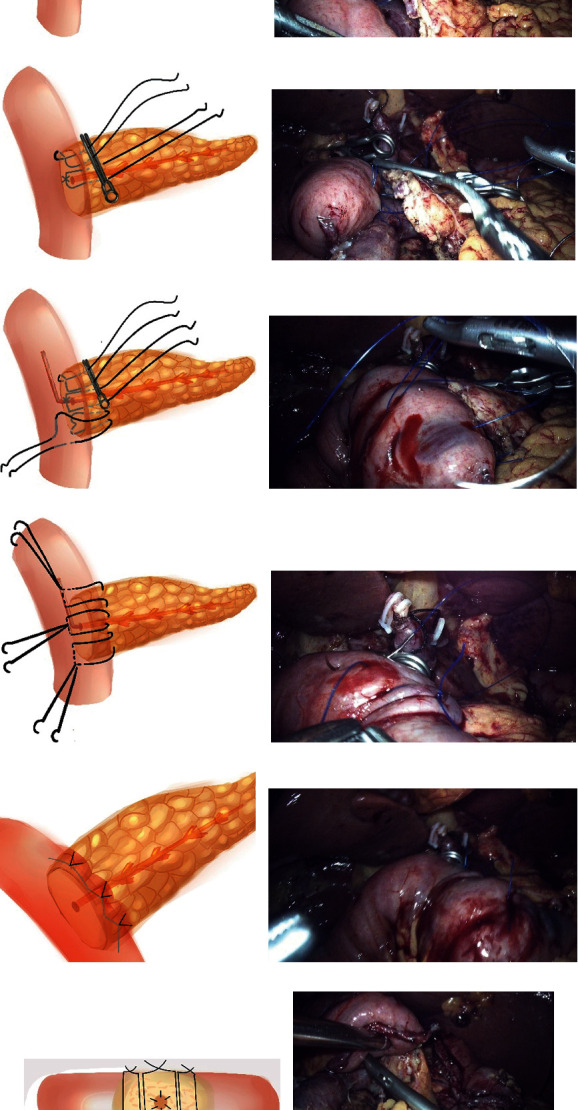
Half-invagination pancreaticoenterostomy. (a, b) Suture A: the two needles were sutured perpendicular to the long axis of the jejunum to the sarcoplasmic muscularis, about 1 cm away from the pancreatic stump, and the full-thickness of the pancreas parenchyma. (c, d) Fixed the suture A with vascular clamp (the suture is not knotted), so as to facilitate the anastomosis of pancreatic duct to mucosa without tension; suture B: two needles were parallel to the long axis of the jejunum to suture jejunum sarcoplasmic layer and then were inserted from the head side and tail side of pancreatic duct through paries posterior about 1 cm from the pancreatic stump. The pancreatic parenchyma was sutured in full thickness without knots. (e, f) Pancreatic duct to the mucosa anastomosis was performed after appropriate pancreatic duct stent tubes were placed. Used suture C to suture symmetrically with the suture A. (g, h) From the tail to the head, C, B, and A sutures were sequentially used to suture the jejunoplasmic muscle layer in a symmetrical manner with the dorsal side of the pancreatic stump and knot separately. (i, j) Completed the insertion of the ventral side of the pancreatic stump. (k) Side view post suture. (l) Dorsal side of the pancreaticointestinal anastomosis, the jejunal serosal layer was inserted into the pancreatic stump.