

Abstract
Background:
Prolonged computer use and poor ergonomics among IT professionals are considered risk factors for musculoskeletal disorders. This research aims to analyze the degree of forward head posture and workplace ergonomics in young IT professionals to assess the risk for a neck disability.
Methods:
A prospective study was carried out by assessing the sitting posture at work, neck disability in the cervical region, quality of life, physical activity, and ergonomics of the workspace in 73 young IT professionals (32.56±5.46 years).
Results:
The score for the cervical functional disability index (NDI) showed a mild neck disability (8.19±7.51). The craniovertebral angle has an average value of 32.01±11.46, corresponding to a light forward head posture, and it positively correlated with age and work experience and negatively correlated with ROSA (r=0.24, p<0.05). The NDI positively correlated with physical activity (r =00.32 p<0.05) and with ROSA (r= 0.24, p<0.05).
Conclusions:
In IT professionals, neck disability is associated with the lack of workspace ergonomics and the amount of physical activity. Forward head posture correlated with age, work experience, and poor workspace ergonomics. According to our findings, there are real concerns about the influence of head posture and workplace ergonomics on health among IT professionals. We consider that it is necessary to adopt preventive measures to address neck disability and improve workspace ergonomics.
Keywords: Neck disability, craniovertebral angle, musculoskeletal disorders, workspace ergonomics, software engineers, COVID-19 pandemic
1. Introduction
Prolonged use of computers for professional purposes often involves frequent and extended periods at the workplace that are not always ergonomically designed. Moreover, among IT professionals, sedentary activity due to long static periods at the computer affects all body systems [1]. Due to the COVID-19 pandemic, all professional activities have been affected, many of them resorting to teleworking. However, in the case of IT professionals, these changes proved to be unfavorable, being a determining factor in the prevalence of musculoskeletal disorders and cervical pain [2]. Essential aspects in managing and preventing work-related musculoskeletal disorders in the case of IT professionals include postural assessments, workstation ergonomic interventions, and work-break time frames [3, 4].
In the literature, studies of professional computer users show that these static postures seriously impact the functionality of the upper torso and the cervical region, implicitly often identified in posture changes in the sagittal plane [5]. The most commonly identified posture in computer users is described by the anterior projection of the head, defined as the anterior position of the head relative to the gravitational line – recognized in the scientific literature as forward head posture [6]. In addition, forward head posture is considered one of the main risk factors in developing musculoskeletal disorders among IT professionals [7, 8].
According to the literature, head posture assessment among computer users is often performed sagittally due to the positioning of the computer workstation (the monitor and auxiliary devices) in the frontal plane [6]. From a clinical point of view, the assessment of postural deficiencies of the head and neck from the sagittal plane should be performed by measuring angles such as the craniovertebral angle (CVA), head positioning angle, head tilt angle, and cranial rotation angle [9].
Recent scientific work considers that the primary method for analyzing the anterior projection of the head is the determination of the craniovertebral angle through photogrammetry [6, 10], which can be evaluated with the help of Posture Screen Mobile software [11, 12].
The means for assessing the workspace ergonomics described in the literature involve various observational methods such as the Rapid Office Strain Assessment (ROSA) checklist [13]. In the scientific literature, several types of questionnaires assess cervical musculoskeletal disorders using patient-reported instruments, the Neck Disability Index (NDI) being the most commonly used for measuring the status of neck pain and the level of disability secondary to pain [14, 15].
This research aims to analyze the degree of forward head posture and the ergonomics of the workplace in young IT professionals to assess the risk for a neck disability.
2. Methods
Informed consent was obtained from all participants involved in the study. We conducted this prospective study between November 15, 2021, and February 15, 2021, in the context of the COVID-19 pandemic.
2.1. Participants
We invited twelve IT companies to participate in the current research by contacting their human resources department; nine of them accepted our invitation. One hundred fifty-two employees received a letter of invitation and the study protocol. Inclusion criteria were:
Professional activity in the field of IT;
At least two years of relevant work experience in the field of IT;
Minimum age of 23 years;
Written confirmation for participation in the study.
Exclusion criteria were:
Any history of cervical pathologies independently of the profession, present before the initiation to the study: diagnosed degenerative and inflammatory disorders of the cervical spine (such as spondylosis, ankylosing spondylitis), cervical traumas, and surgical interventions in the cervical area;
Absence to any of the stages of the study (regardless of the reason).
All volunteers signed informed consent to participate in the study. The local ethics committee approved the study protocol, which respected the Helsinki Declaration.
2.2. Study Protocol
The study protocol was divided into three stages: Stage I – which consisted of a 20 min survey, followed by Stage II – an objective assessment of the sitting posture at work, and Stage III – the evaluation of the workspace ergonomics.
2.2.1. Stage I - Survey Implementation
The survey comprised four sections: (i) demographic data and details about the professional activity; (ii) neck disability assessment; (iii) quality of life; (iv) physical activity assessment.
1. Demographic data (gender, age, height, weight, dominant hand) and details about the professional activity (work experience, duration of weekly working days, and the average number of hours spent on the computer, place of professional activity – at the office (within the company) or home (remotely), number and duration of daily breaks, information about the alternation of office position and data about the current state of health).
2. The neck disability assessment was performed using the Neck Disability Index (NDI) questionnaire – it contains ten items that refer to neck pain (intensity) and the level of ability to manage daily living activities (personal care, reading, lifting, headache, work, concentration, driving, sleep and recreation) [14]. The NDI score is interpreted as 0-4=no disability, 5-14=mild disability, 15-24=moderate disability, 25-34=severe disability, and over 34= total disability, where a score of 50 converted to percentiles represents 100% [15]. According to Kumari et al., the NDI score is calculated as follows: total score/total possible score, transformed to percentage multiplied by 100=% points [16].
3. The quality of life was evaluated by applying the SF-36 quality of life questionnaire composed of 8 scales (36 questions): physical functioning, bodily pain, role limitations due to physical health problems, role limitations due to personal or emotional problems, general mental health, social functioning, energy/fatigue or vitality, and general health perceptions [17]. The results can vary between 0 and 100, with a higher score representing a better general state of health [18]. The SF-36 questionnaire is frequently used as a valuable tool in determining health status [19].
4. Physical activity assessment: the participants’ type, frequency, and volume of physical activity.
2.2.2. Stage II - Evaluation of the Sitting Posture at Work
Head and neck posture assessments were performed at the workstation of each participant, either at their home office setup or within the company office by an independent investigator. All images were taken with the same camera placed on a tripod 1.5 m away from the participant and adjusted at shoulder level. The camera recorded a 60 minutes video of the participant during the work time activity. In order to reduce potential false working postures, participants were asked to continue their professional activity while the camera was recording. The video analysis was performed by a second investigator who selected a frame of the most relevant posture (the posture maintained by the participants for the most extended period).
The photographic analysis was done in the second part of the first working day of the week (or immediately after a holiday) to obtain relevant results and implicitly reduce the bias. In addition, we used the Posture Screen Mobile Software (PSM) [11] to obtain accurate and more detailed measurements of the craniovertebral angle and to analyze the head’s position.
After selecting the images of all participants, these were uploaded into the PSM software. The height and weight were entered into the PSM software after creating a record of each participant. The digitization process involves specific landmarks that were placed on the lateral view in the following points: the top part of the monitor, the bottom part of the monitor, the lateral canthus of the eye, the correct interior of the external acoustic meatus, the center base of the neck at the cervicothoracic junction, spinous process of the C7 vertebrae, seventh thoracic vertebrae, the center of the thorax – approximately at T6-T8 level, the center of the mid-lower torso at T10-L1 level, elbow, wrist, hand (center of distal metacarpals), the center of the hip - great trochanter, knee - lateral of the tibiofemoral joint and ankle - the center of the malleolus (Figure 1). All points were marked using reflective stickers placed according to the above body landmarks.
Figure 1.
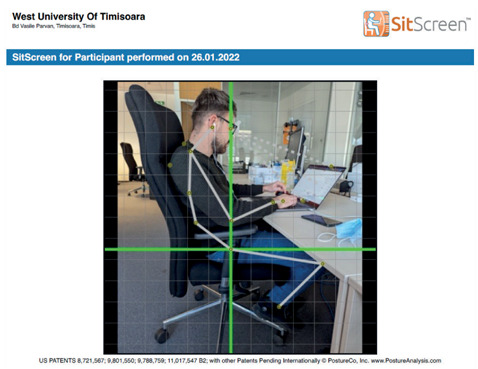
Anatomical landmarks, digitisation process in PSM.
The craniovertebral angle was analyzed with two anatomical landmarks (the spinous process of the C7 cervical vertebrae and the outer part of the ear-tragus). This angle is formed by the horizontal line passing through the seventh cervical (C7) vertebra’s spinous process and the line between the C7 vertebra’s spinous process and the ear’s tragus [20]. According to Shaghayegh Fard et al., values <48-50° of the craniovertebral angle imply a greater rate of occurrence of forward head posture [21]. Therefore, the craniovertebral angle is considered normal when higher than 50°, light when it is between 30°-50°, and severe when it is below 30° [22].
During the process of digitization, the PSM software measures the craniovertebral angle (CVA), head-neck angle (neck flexion angle), head-tilt angle (relative to horizontal), gaze angle, high thoracic angle, neck posture angle, elbow angle, wrist angle, trunk-thigh angle, thigh angle, and lower leg angle. The results obtained using the PSM software present the relation between the sitting posture of the participant and workspace ergonomics.
2.2.3. Stage III - Assessment of the Workspace Ergonomics
The workspace was assessed using an independent investigator’s Rapid Office Strain Assessment (ROSA) checklist, blind to the previous evaluation stages. ROSA is an observational method that assesses chair height, pan depth, armrest, back support, duration of sitting, and postures when using the telephone, monitor, keyboard, and mouse, all results producing an overall score that will be analyzed with a scoring chart. A final score higher than 5 implies an increased ergonomic risk factor and a high level of discomfort [13]. Statistical analysis was performed using SPSS Version 26. A bivariate (1-tailed) Pearson correlation test was used to observe the relation between the measured parameters.
3. Results
From the 105 IT specialists recruited in the study, we enrolled 73 (39 men and 34 women). Eight participants were excluded due to medical conditions mentioned in the exclusion criteria, and 24 participants dropped out after the first stage of the study protocol. The demographic characteristics of the group are shown in Table 1.
Table 1.
Characteristics of the study group.
| Parameter | Mean±Standard deviation (n=73) |
|---|---|
| Age (yrs.) Body Mass Index (kg/m2) Professional experience (yrs.) |
32.56±5.46 23.52±3.56 9.32±5.56 |
Due to the COVID-19 pandemic, 33 (45.21%) participants adopted a remote work style and, in some cases, a hybrid mode (remote work combined with office work). Many participants spend, on average, 6-8 hours/day at the computer (n=31, 42.47%). Many participants (n=33, 45.21%) also reported that they work from home (remotely), followed by a large number who adopted a hybrid mode (n=28, 38.36%), whereas only 16.44% (n=12) conducted their professional activity at the office. Among those adopting a hybrid regime, 12.3% worked 1-2 days from home/week, 23.2% worked 2-4 days from home, whereas 47.9% worked 4-6 days a week from home.
Break frequency during a working day was relatively high, with 36.9% stating that they take 3-4 breaks/day, each lasting about 5-10 minutes long (61.6% of the participants).
According to the Occupational Safety and Health Administration (OSHA), sitting still for prolonged periods when working at the computer is unhealthy, and they recommend changing this position frequently.
Sources of information about office ergonomics vary widely. Most participants (n=53, 72.6%) know workspace ergonomics, obtained through online research, specialized courses, ergonomic specialists, friends, colleagues, or social media. The most commonly used device among the IT professionals in our research is the laptop (n=67, 91.78%), with only a few using a computer (n=6, 8.10%). For most of their professional activity, 54.7% (n=40) of the participants used two monitors.
In terms of physical activity, a large number of participants (n=35, 47.9%) stated that they join in physical activities several times a week, and only a few participants (n=4, 5.48%) from the entire group do not join any physical activities. 42.47% (n=31) of the participants stated that they endorse physical activities several times a week with a frequency of 3-4 workouts/week, followed by 27.4% (n=20) with a frequency of 1-2 workouts/week. 15.07% (n=11) of the entire group is sedentary, and 5.48% (n=4) practice high-performance sports. 9.59% (n=7) of the participants have daily physical activities such as walking or cycling to work. For statistical analysis, physical activity was coded with 1 – daily physical activity, 2 – physical activity several times a week, 3 – physical activity several times a month, 4 – physical activity several times a year, and 5 – never.
The correlations between the measured parameters are presented in Table 2. The mean value of the cervical functional disability index (NDI) is 8.19±7.51 (Table 2), which, according to Vernon, represents a mild disability score [15]. The mean craniovertebral angle measured using the Posture Screen Mobile software has an average value of 32.01±11.46 (Table 2).
Table 2.
Descriptive Statistics and 1-Tailed Bivariate Pearson Correlations for Manifest Variables.
| Variables | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | 11 | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 | CVA | - | ||||||||||
| 2 | Head Neck Angle | -0.94** | - | |||||||||
| 3 | Gaze Angle | -0.35** | 0.32** | - | ||||||||
| 4 | Thorax Angle | -0.06 | 0.12 | 0.00 | - | |||||||
| 5 | Age | 0.28** | -0.26* | -0.19 | 0.04 | - | ||||||
| 6 | Neck Disability Index | -0.06 | 0.13 | 0.19 | 0.06 | -0.15 | - | |||||
| 7 | Work Experience | 0.23* | -0.21* | -0.21* | 0.10 | 0.87** | -0.08 | - | ||||
| 8 | Gender | -0.10 | 0.13 | 0.02 | 0.00 | -0.05 | 0.02 | 0.02 | - | |||
| 9 | Physical Activity | -0.13 | 0.06 | 0.04 | -0.02 | -0.05 | 0.32* | -0.09 | 0.11 | - | ||
| 10 | Device Type | -0.13 | 0.10 | -0.22* | -0.01 | 0.06 | -0.09 | 0.09 | 0.14 | 0.13 | - | |
| 11 | ROSA | -0.24* | 0.29** | 0.21* | 0.00 | 0.01 | 0.24* | 0.00 | -0.11 | 0.04 | .17 | - |
| Mean | 32.01 | 57.02 | 19.49 | 157.99 | 32.56 | 8.19 | 9.32 | 1.53 | 2.32 | 1.06 | 3.37 | |
| SD | 11.46 | 11.57 | 11.15 | 15.37 | 5.46 | 7.51 | 5.56 | .50 | .87 | .25 | .87 |
M=mean; SD=standard deviations; *=p<0.05; **=p<0.01.
The craniovertebral angle was positively correlated with age (r=0.28, p<0.01) and work experience (r=0.23, p<0.05) and negatively correlated with ROSA (r=0.24, p<0.05). The head-neck angle was negatively correlated with age (r=-0.26, p<0.05) and with work experience (r=-0.21, p<0.05) and positively correlated with ROSA (r=0.29, p<0.01). The gaze angle was negatively correlated with work experience (r=-0.21, p<0.05) and the device used – laptop/computer (r=-0.22, p<0.05), and positively correlated with ROSA (r=0.21, p<0.05). Finally, the NDI was positively correlated with physical activity (r =0.32 p<0.05) and with ROSA (r=0.24, p<0.05).
4. Discussion
Our study aimed to assess the level of cervical disability among young IT specialists by assessing the relationship between cervical spine posture during professional activities, age, work experience, level of physical activity, and the impact of workspace ergonomics. The results obtained provide valuable information on these topics. In addition, Lamba et al. also confirmed the development of neck and upper limb disabilities among IT specialists using computers more than 40 hours per week [23].
Aegerter et al. noticed that the number of daily breaks and workstation ergonomics could influence the level of neck disability [24]. Therefore, they conducted a longitudinal study starting from 2 hypotheses – neck pain prevalence is influenced by working from home, and workstation ergonomics, break time during computer use. The total amount of time spent at the computer could increase neck pain intensity and neck disability. For their study, they collected data before the COVID-19 pandemic started and made a follow-up during the lockdown. The findings of their study show that a higher number of breaks during computer use could reduce the degree of a neck disability and that there is an association between neck pain intensity and the number of hours spent at the computer.
We have chosen to evaluate the forward head posture by measuring the craniovertebral angle as per the findings of Kim & Kim, who stated that this method is reliable when investigating the functionality of the neck region [25]. In addition, recent scientific work considers the primary method for analyzing the anterior projection of the head by determining the craniovertebral angle using photogrammetry as a validated, reliable, and objective method [6, 10, 20]. Following the posture’s photographic analysis, the craniovertebral angle measurement can be done with the help of Posture Screen Mobile [11, 12], a non-invasive, easy-to-use, and portable way that allows optimal assessment and does not require experience in obtaining accurate and reliable measurements.
According to the study by Szucs & Brown, the Posture Screen Mobile software has strong reliability and validity in scientific research and for clinical purposes [12]. Natural numbers with finite decimals represent the result of the measured craniovertebral angle when using the Posture Screen Mobile app. A study by Boland et al. showed that postural assessments analyzed with the PSM software are clinically relevant, especially when diagnosing the forward head posture [11]. Other scientific studies assessing poor postures among computer users, implicitly the forward head posture, by measuring the craniovertebral angle, concluded that the photogrammetry technique analysis using the PSM software is reliable and conclusive [26, 27]. The equipment chosen and the assessment method applied were considered unobtrusive/non-invasive and feasible in the COVID-19 pandemic context.
Even though the mean age of the studied group indicated a relatively young group (32.56±5.46 years), we noticed that the CVA degree is positively correlated with age and work experience, consistently with the findings of Sun et al. [28].
Implicitly, some misalignments can be noticed with a poor posture, such as an anterior projected head. According to Hansraj, as the weight of the head is shifted anteriorly in the forward head posture, not only the craniovertebral angle worsens/is affected, but it also changes and can be seen in the gaze angle, dropping below the horizontal line – which is considered to represent a level of comfort. Our study has identified significant results when correlating parameters such as the CVA, gaze angle, and head-neck flexion angle [29].
Nejati et al. conducted a study regarding the relationship between poor postures (forward head posture) and the prevalence of cervical pain, respectively the degree of cervical disability, in two groups of participants (a symptomatic group with cervical pain and an asymptomatic group without cervical pain)[30]. Following the measurements of the craniovertebral angle, the differences between the symptomatic and asymptomatic groups were minor (UCV=23.00±0.70 in the symptomatic group, respectively UCV=28.40±12.40 in the asymptomatic one). The study concludes that the value of the craniovertebral angle does not directly influence the degree of cervical disability and, implicitly, by the degree of forward head posture.
In compiling the online survey, we chose both the Neck Disability Index and SF-36 as per the results of Pontes et al., which show that these are reliable and valid tools for evaluating disability and neck pain [31]. In addition, a review conducted by Bobos et al. demonstrated that the Neck Disability Index questionnaire has from moderate to excellent level of reliability in test-retest and is supported by the qualitative results of the content [32]. Although the Neck Disability Index was published first in 1991 by Vernon et al., the only change that has been made was the word “neck” that was added to the term “pain” to specify that the question referred to the “neck pain” of the individual taking the survey. The scientific literature regarding ways of treating and preventing neck pain, and, all the more, neck disability, highly recommend specific exercises that follow outcomes, such as strengthening or stretching the involved region. In our study group, participants more involved in physical activities had a lower level of neck disability, the NDI being correlated to physical activity.
According to Lindegård et al. [33] and Jun et al. [34], the NDI can be influenced by multifactorial causes, such as ergonomic risk factors, psychosocial factors, and individual factors. A specific method of assessing ergonomic workplace risk factors among computer users is the Rapid Office Strain Assessment (ROSA) checklist published by Sonne & Andrews [13], and according to the findings of Panchal et al., it is highly applicable among IT specialists [7].
Our results support Sonne et al., who demonstrated a relationship between the level of discomfort and a higher ROSA score; in our study, significant correlations were noticed between the ROSA score and NDI [35]. Our conclusions are also consistent with the findings of Aegerter et al., i.e., that neck disability can be positively influenced by increasing the number of breaks during computer use and when physically active [24], and with those of Barkhordarzadeh et al., suggesting that great focus should be oriented towards an ergonomic intervention, to reduce work-related musculoskeletal disorders and cervical disability [36].
The use of the questionnaire method is considered an appropriate approach in scientific research because it allows the collection of a large amount of information by obtaining accurate and easily measurable data in the shortest possible time and with the least possible need for resources; however, there are disadvantages such as a low response rate and a high level of subjectivity on the part of the participants. Nowadays, the vast majority of IT specialists are working remotely, which, according to scientific literature findings, can harm them. Out of 73 participants, only a small number do not know if they change their position (13.6%) or do not change it during a working day.
Strengths and Limitations
To our knowledge, this is the first study that uses the Posture Screen Mobile software to assess the craniovertebral angle in IT specialists. We consider our method to be not only non-invasive but also highly applicable in the case of remote workers. Furthermore, we consider our survey to be original in its approach, as we did not find any other study analyzing the correlation between neck disability, quality of life, and workspace ergonomics.
The study has the following limitations: the self-reported data obtained in the first stage of the study protocol cannot be independently verified; in the second stage of the study protocol, the participants’ posture could have been influenced by the awareness that they were video-recorded. Also, we consider that recording the posture during work time for a more extended period, in different timeframes of the working day and the week, would lead to more relevant results.
5. Conclusion
In IT professionals, the degree of neck disability is associated with the lack of workspace ergonomics and the amount of physical activity. The forward head posture positively correlates with age, work experience, and poor workspace ergonomics. According to our findings, there are real concerns about the influence of head posture and workplace ergonomics on health among IT professionals. We consider that it is necessary to adopt preventive measures to address neck disability and improve workspace ergonomics.
Institutional Review Board Statement:
The study was conducted according to the guidelines of the Declaration of Helsinki, and approved by approved by The Scientific Council of University Research and Creation by West University of Timisoara (approval number: 62876/ November 11, 2021).
Informed Consent Statement:
Informed consent was obtained from all subjects involved in the study.
Declaration of Interest:
The authors declare no conflict of interest.
References
- Daneshmandi H, Choobineh A, Ghaem H, Karimi M. Adverse Effects of Prolonged Sitting Behavior on the General Health of Office Workers. J Lifestyle Med. 2017;7(2):69–75. doi: 10.15280/jlm.2017.7.2.69. Doi:10.15280/jlm.2017.7.2.69. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Stîncel O-R, Niţ A, Oraviţan M. The impact of home office setup due to COVID-19 pandemic on IT professionals′ physical health: a systematic review. Timisoara Phys Educ Rehabil J. 2021;14(26):7–16. Doi:10.2478/tperj-2021-0001. [Google Scholar]
- Mohammadipour F, Pourranjbar M, Naderi S, Rafie F. Work-related Musculoskeletal Disorders in Iranian Office Workers: Prevalence and Risk Factors. J Med Life. 2018;11(4):328–333. doi: 10.25122/jml-2018-0054. Doi:10.25122/jml-2018-0054. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Luger T, Maher CG, Rieger MA, Steinhilber B. Work-break schedules for preventing musculoskeletal symptoms and disorders in healthy workers. Cochrane database Syst Rev. 2019;7(7):CD012886. doi: 10.1002/14651858.CD012886.pub2. Doi:10.1002/14651858.CD012886.pub2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Lee HS, Chung HK, Park SW. Correlation between trunk posture and neck reposition sense among subjects with forward head neck postures. Biomed Res Int. 2015;2015:689610. doi: 10.1155/2015/689610. Doi:10.1155/2015/689610. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Molaeifar S, Yazdani F, Yoosefinejad AK, Karimi MT. Correlation between craniovertebral angle in the sagittal plane and angles and indices measured in the frontal plane at the moment of inducing forward head posture. Work. 2021;68(4):1221–1227. doi: 10.3233/WOR-213451. Doi:10.3233/WOR-213451. [DOI] [PubMed] [Google Scholar]
- Panchal S, Viramgami AP, Pingle S. Prevalence and Determinants of Musculoskeletal Disorders among Information Technology Sector Employees of Ahmedabad, Gujarat. J Compr Heal. 2020;8(2):1–6. https://ezproxy2.library.colostate.edu/login?url=https://search.ebscohost.com/login.aspx?direct=true&AuthType=cookie,ip,url,cpid&custid=s4640792&db=aph&AN=146186851&site=ehost-live. [Google Scholar]
- Redivo VS, Olivier B. Time to re-think our strategy with musculoskeletal disorders and workstation ergonomics. South African J Physiother. 2021;77(1):1–10. doi: 10.4102/sajp.v77i1.1490. Doi:10.4102/sajp.v77i1.1490. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Szczygieł E, Fudacz N, Golec J, Golec E. The impact of the position of the head on the functioning of the human body: a systematic review. Int J Occup Med Environ Health. 2020;33(5):559–568. doi: 10.13075/ijomeh.1896.01585. Doi:10.13075/ijomeh.1896.01585. [DOI] [PubMed] [Google Scholar]
- Worlikar AN, Shah MR. Incidence of forward head posture and associated problems in desktop users. Int J Heal Sci Res. 2019;9(2):96–100. [Google Scholar]
- Boland DM, Neufeld EV, Ruddell J, Dolezal BA, Cooper CB. Inter- and intra-rater agreement of static posture analysis using a mobile application. J Phys Ther Sci. 2016;28(12):3398–3402. doi: 10.1589/jpts.28.3398. Doi:10.1589/jpts.28.3398. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Szucs KA, Brown EVD. Rater reliability and construct validity of a mobile application for posture analysis. J Phys Ther Sci. 2018;30(1):31–36. doi: 10.1589/jpts.30.31. Doi:10.1589/jpts.30.31. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Sonne M, Andrews DM. The Rapid Office Strain Assessment (ROSA): Validity of online worker self-assessments and the relationship to worker discomfort. Occup Ergon. 2011;10(3):83–101. Doi:10.3233/OER-2012-0194. [Google Scholar]
- Vernon H, Mior S. The Neck Disability Index: a study of reliability and validity. J Manipulative Physiol Ther. 1991;14(7):409–415. [PubMed] [Google Scholar]
- Vernon H. THE NECK DISABILITY INDEX: STATE-OF-THE-ART, 1991-2008. doi: 10.1016/j.jmpt.2008.08.006. Published online 2008:491-502. Doi:10.1016/j.jmpt.2008.08.006. [DOI] [PubMed] [Google Scholar]
- Kumari S, Kumar R, Sharma D. Text Neck Syndrome: The Pain of Modern Era. Int J Health Sci Res. 2021;(November) Doi:10.52403/ijhsr.20211121. [Google Scholar]
- Ware JEJ, Sherbourne CD. The MOS 36-item short-form health survey (SF-36). I. Conceptual framework and item selection. Med Care. 1992;30(6):473–483. [PubMed] [Google Scholar]
- Ware JE. The MOS 36-item short-form health survey (SF-36) I. Conceptual framework and item selection. 2014;(June) [PubMed] [Google Scholar]
- Boerger T, Alsouhibani A, Mowforth O, et al. Health-related quality of life (SF-36) in back pain: a population-based study, Campinas, São Paulo State, Brazil. Cad Saude Publica. 2021;37(2):1–12. doi: 10.1590/0102-311X00206019. Doi:10.1590/0102-311X00206019. [DOI] [PubMed] [Google Scholar]
- Cote R, Vietas C, Kolakowski M, Lombardo K, Prete J, Dashottar A. Inter and Intra-Rater Reliability of Measuring Photometric Craniovertebral Angle Using a Cloud-Based Video Communication Platform. Int J Telerehabilitation. 2021;13(1):1–9. doi: 10.5195/ijt.2021.6346. Doi:10.5195/ijt.2021.6346. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Shaghayegh fard B, Ahmadi A, Maroufi N, Sarrafzadeh J. Evaluation of forward head posture in sitting and standing positions. Eur Spine J. 2016;25(11):3577–3582. doi: 10.1007/s00586-015-4254-x. Doi:10.1007/s00586-015-4254-x. [DOI] [PubMed] [Google Scholar]
- Abbasi AH, Aslam M, Ashraf T, Malik AN. Evaluation of the forward head posture, its association with neck pain & quality of life of female DPT students. J Riphah Coll Rehabil Sci. 2016;4(2):59–64. [Google Scholar]
- Lamba D, Upadhyay RK. Accumulative repetitive strain injury among business process outsourcing employees: A survey study. Asian J Pharm Clin Res. 2017;10(11):118–21. Doi:10.22159/ajpcr.2017.v10i11.19423. [Google Scholar]
- Aegerter AM, Deforth M, Johnston V, Sj⊘gaard G, Volken T. No evidence for an effect of working from home on neck pain and neck disability among Swiss office workers: Short-term impact of COVID-19. Eur Spin J. 2021:1699–1707. doi: 10.1007/s00586-021-06829-w. Published online. Doi:10.1007/s00586-021-06829-w. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kim EK, Kim JS. Correlation between rounded shoulder posture, neck disability indices, and degree of forward head posture. J Phys Ther Sci. 2016;28(10):2929–2932. doi: 10.1589/jpts.28.2929. Doi:10.1589/jpts.28.2929. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Elwardany SH, El-Sayed WH, Ali MF. Reliability of Kinovea Computer Program in Measuring Cervical Range of Motion in Sagittal Plane. OALib. 2015;02(09):1–10. Doi:10.4236/oalib.1101916. [Google Scholar]
- Latif SHA, Kamel RM, Draz AH. Effect of Smartphone Extensive Usage and Gender on Cervical angle. Curr Sci Int. 2018;7(4):762–767. [Google Scholar]
- Sun A, Yeo HG, Kim TU, Hyun JK, Kim JY. Radiologic assessment of forward head posture and its relation to myofascial pain syndrome. Ann Rehabil Med. 2014;38(6):821–826. doi: 10.5535/arm.2014.38.6.821. Doi:10.5535/arm.2014.38.6.821. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hansraj KK. Assessment of stresses in the cervical spine caused by posture and position of the head. Surg Technol Int. 2014;25:277–279. http://www.ncbi.nlm.nih.gov/pubmed/25393825. [PubMed] [Google Scholar]
- Nejati P, Lotfian S, Moezy A, Nejati M. The study of correlation between forward head posture and neck pain in Iranian office workers. Int J Occup Med Environ Health. 2015;28(2):295–303. doi: 10.13075/ijomeh.1896.00352. Doi:10.13075/ijomeh.1896.00352. [DOI] [PubMed] [Google Scholar]
- Pontes A, Mariana S, Avila A, et al. The Short - Form Neck Disability index has adequate measurement properties in chronic neck pain patients. Eur Spine J. 2021;30(12):3593–3599. doi: 10.1007/s00586-021-07019-4. Doi:10.1007/s00586-021-07019-4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Bobos P, Macdermid JC, Walton DM, Gross A, Santaguida PL. Patient-reported outcome measures used for neck disorders: An overview of systematic reviews. J Orthop Sports Phys Ther. 2018;48(10):775–788. doi: 10.2519/jospt.2018.8131. Doi:10.2519/jospt.2018.8131. [DOI] [PubMed] [Google Scholar]
- Lindegård A, Wahlström J, Hagberg M, Vilhelmsson R, Toomingas A, Wigaeus Tornqvist E. Perceived exertion, comfort and working technique in professional computer users and associations with the incidence of neck and upper extremity symptoms. BMC Musculoskelet Disord. 2012;13:1–8. doi: 10.1186/1471-2474-13-38. Doi:10.1186/1471-2474-13-38. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Jun D, Johnston V, McPhail SM, O’Leary S. A Longitudinal Evaluation of Risk Factors and Interactions for the Development of Nonspecific Neck Pain in Office Workers in Two Cultures. Hum Factors. 2020;(1):1–21. doi: 10.1177/0018720820904231. Doi:10.1177/0018720820904231. [DOI] [PubMed] [Google Scholar]
- Sonne M, Villalta DL, Andrews DM. Development and evaluation of an office ergonomic risk checklist: ROSA - Rapid office strain assessment. Appl Ergon. 2012;43(1):98–108. doi: 10.1016/j.apergo.2011.03.008. Doi:10.1016/j.apergo.2011.03.008. [DOI] [PubMed] [Google Scholar]
- Barkhordarzadeh S, Choobineh A, Razeghi M, Cousins R, Mokarami H. Effects of an ergonomic intervention program based on the PRECEDE – PROCEED model for reducing work - related health problems and exposure risks among emergency medical dispatchers. Int Arch Occup Environ Health. 2022 Aug;95(6):1389–1399. doi: 10.1007/s00420-022-01846-8. Published online 2022 Doi:10.1007/s00420-022-01846-8. [DOI] [PubMed] [Google Scholar]