

Abstract
We report a 48‐year‐old female patient with various stress fractures of extremities, musculoskeletal pain, and tooth loss. Hypophosphatasia was diagnosed based on clinical and laboratory findings and ALPL genetic results. This case highlights the importance of early diagnosis of hypophosphatasia in adults and appropriate treatment to prevent further complications.
Keywords: dental loss, low alkaline phosphatase, stress fracture
Adult hypophosphatasia may present with recurrent fractures, chronic musculoskeletal pain, tooth loss, and low alkaline phosphatase level. Asfotase alfa therapy can be used to improve respiratory function, motor function, and reduce tooth loss.
1. CASE PRESENTATION
A 48‐year‐old female patient presented with a history of vitamin D deficiency, stress fractures of various extremities, and dental issues with loose teeth. Past medical/surgical history also included perimenopause, nasal cartilage collapse, breast reduction, and 4 bone grafts. She was from European descent, and family history was notable for a mother with early adulthood hip fracture and osteoporosis. She denied any use of tobacco, alcohol, and did not exercise regularly due to pain and limited range of motion. On physical examination, vital signs, heart, and lungs were normal. Dental examination demonstrated loosen teeth of both upper and lower jaws confirmed on X‐rays (Figure 1) and diffuse muscle/joint pain throughout the body. Laboratory findings showed serum alkaline phosphatase level 21 U/L (normal 35–113), normal renal, parathyroid hormone (PTH), and thyroid function tests. Cone beam CT scan showed edentulous maxilla, thin cortical contours, sclerotic cancellous bone surrounding the teeth, and bone loss of mandibular teeth (Figure 2). Genetic testing revealed a single heterozygous pathogenic variant in the ALPL gene. Baseline dual‐energy X‐ray absorptiometry (DXA) was normal (Figure 3).
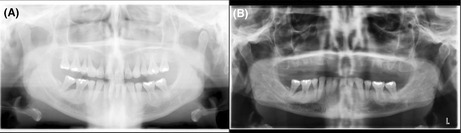
FIGURE 1.
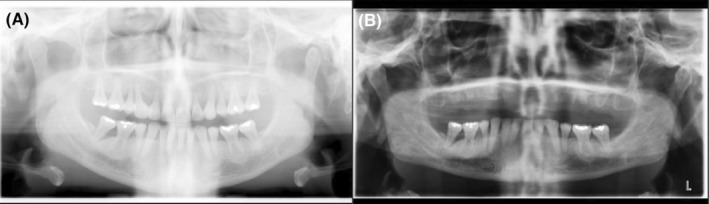
(A and B) Pano pre‐op and post‐op X‐rays of extraction of all upper teeth
FIGURE 2.
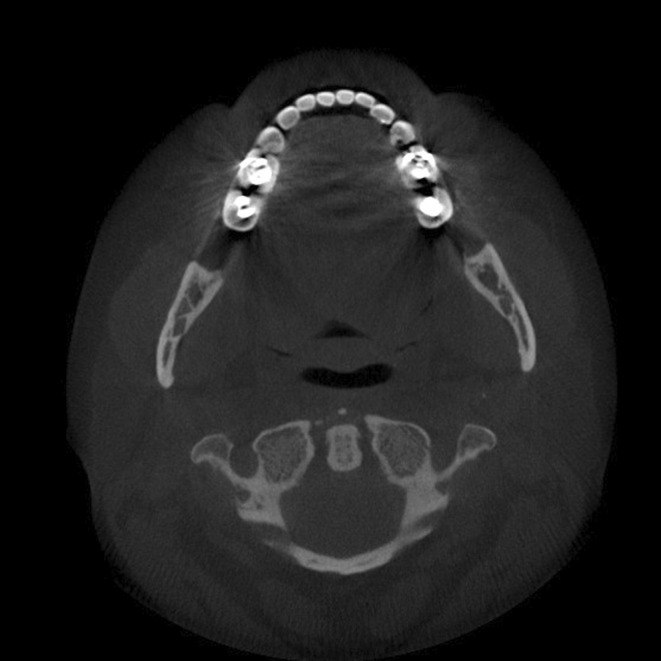
Cone beam CT scan showed edentulous maxilla, thin cortical contours, sclerotic cancellous bone surrounding the teeth and bone loss of mandibular teeth
FIGURE 3.
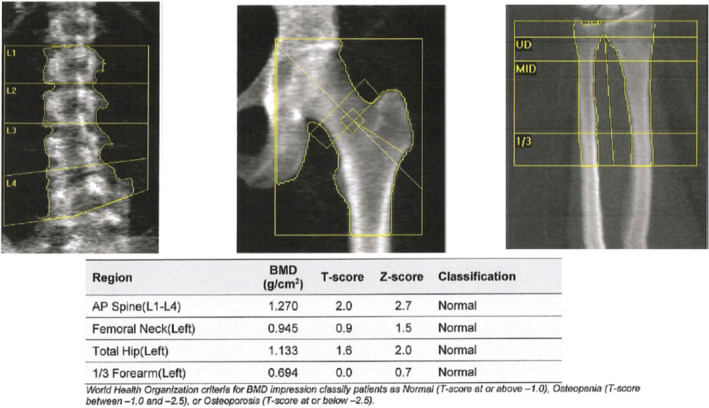
Dual‐energy X‐ray absorptiometry showing normal bone mineral density in the lumbar spine, hip, and forearm
2. WHAT IS THE DIAGNOSIS?
Answer: Hypophosphatasia.
Dental findings and medical history are all consistent with the diagnosis of juvenile onset hypophosphatasia. Hypophosphatasia is characterized by defective mineralization of bone and/or teeth and low serum and bone alkaline phosphatase. 1 , 2 , 3 Severe cases include stillbirth without mineralized bone while milder cases include recurrent fractures of the lower extremities or premature tooth loss in adulthood. Perinatal and infantile hypophosphatasia are inherited in an autosomal recessive manner in which both parents contribute one copy of the mutated gene while adult/milder forms can be inherited in an autosomal dominant or recessive manner where only one copy of the mutated gene is needed for the person to show symptoms. Affected infants may present with short limbs, soft skull bones, and unusual chest shape. Other complications include hypercalcemia, respiratory problems, and difficulty gaining weight. Early primary tooth loss is one of the first signs of this condition in children, whereas adult forms may include recurring fractures, chronic pain, and premature tooth loss of the secondary set of teeth, as in our patient despite normal DXA scan. A characteristic dental finding of hypophosphatasia is early exfoliation of primary teeth, most commonly affecting the anterior teeth, starting between the ages of 1 and 4 years. In hypophosphatasia, early exfoliation of primary teeth is caused by poor mineralization of cementum due to low alkaline phosphatase activity. Disturbed formation of cementum is also recognized in permanent teeth, which may result in permanent teeth being exfoliated. The disturbed formation of cementum increases the susceptibility for early exfoliation of anterior teeth and also ankylosis involving posterior teeth. The occlusal force damages weak periodontal tissue and subsequently interferes with root adhesion to alveolar bone. Thus, early diagnosis is important for patients to receive early intervention in dental fields. In these patients with early exfoliation of primary teeth, dentures are generally recommended so as to ensure that important oral functions are acquired. Studies have shown that treatment with asfotase alfa injection therapy improves dental mineralization, resulting in the stabilization of periodontal tissues and ultimately resulting in better growth of tooth roots. 4 , 5 , 6 , 7 Treatment with asfotase alfa injection is FDA approved for patients with perinatal/infantile and juvenile‐onset hypophosphatasia and proven to improve respiratory function, motor function, and bone mineralization. 3 This case highlights the importance of early diagnosis of hypophosphatasia in adults and appropriate treatment to prevent further complications.
AUTHOR CONTRIBUTIONS
Lindsay Thi Hoang: Conceptualization; data curation; formal analysis; investigation; writing – original draft. Jennifer S Hatfield: Conceptualization; formal analysis; investigation; writing – review and editing. Quan Nguyen: Conceptualization; investigation; writing – review and editing. Mohamed KM Shakir: Conceptualization; formal analysis; investigation; resources; supervision; writing – review and editing. Thanh D Hoang: Conceptualization; formal analysis; investigation; methodology; resources; supervision; validation; writing – review and editing.
CONFLICT OF INTEREST STATEMENT
None to declare.
ETHICS STATEMENT
The manuscript has been reviewed and approved by the IRB and Public Affairs Office.
INFORMED CONSENT
Written informed consent was obtained from the patient to publish this report in accordance with the journal's patient consent policy.
ACKNOWLEDGMENTS
The views expressed in this article are those of the authors and do not reflect the official policy of the Department of Army/Navy/Air Force, Department of Defense, or the U.S. Government.
Hoang LT, Hatfield JS, Nguyen Q, Shakir MKM, Hoang TD. Dental loss, stress fractures, and musculoskeletal pain in a 48‐year‐old woman. Clin Case Rep. 2023;11:e7002. doi: 10.1002/ccr3.7002
DATA AVAILABILITY STATEMENT
Not applicable.
REFERENCES
- 1. Mornet E, Nunes ME. Hypophosphatasia. In: Adam MP, Ardinger HH, Pagon RA, et al., eds. GeneReviews® [Internet]. University of Washington, Seattle; 2007:1993‐2021. [PubMed] [Google Scholar]
- 2. Reis FS, Gomes DC, Arantes HP, Lazaretti‐Castro M. A two‐year follow‐up of asfotase alfa replacement in a patient with hypophosphatasia: clinical, biochemical, and radiological evaluation. Arch Endocrinol Metab. 2021;64(5):623‐629. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3. Scott LJ. Asfotase alfa: a review in paediatric‐onset hypophosphatasia. Drugs. 2016;76(2):255‐262. [DOI] [PubMed] [Google Scholar]
- 4. Shetty S, Zargar NM, Shenoy K, Rekha V. Occlusal plane location in edentulous patients: a review. J Indian Prosthodont Soc. 2013;13(3):142‐148. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5. Okawa R, Nakano K. Dental manifestation and management of hypophosphatasia. Jpn Dent Sci Rev. 2022;58:208‐216. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6. Villa‐Suárez JM, García‐Fontana C, Andújar‐Vera F, et al. Hypophosphatasia: a unique disorder of bone mineralization. Int J Mol Sci. 2021;22(9):4303. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7. D'Orto B, Polizzi E, Nagni M, Tetè G, Capparè P. Full arch implant‐prosthetic rehabilitation in patients with type I diabetes mellitus: retrospective clinical study with 10 year follow‐up. Int J Environ Res Public Health. 2022;19(18):11735. [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Data Availability Statement
Not applicable.