

Abstract
BACKGROUND:
Perioperative anemia has been associated with increased risk of red blood cell transfusion and increased morbidity and mortality following surgery. The optimal approach to the diagnosis and management of perioperative anemia is not fully established.
OBJECTIVE:
To develop consensus recommendations for anemia management in surgical patients.
METHODS:
An international expert panel reviewed the current evidence and developed recommendations using modified RAND Delphi methodology.
RESULTS:
The panel recommends that all patients, except those undergoing minor procedures, be screened for anemia prior to surgery. Appropriate therapy for anemia should be guided by an accurate diagnosis of the etiology. The need to proceed with surgery in some patients with anemia is expected to persist. However, early identification and effective treatment of anemia has the potential to reduce the risks associated with surgery and improve clinical outcomes. As with preoperative anemia, postoperative anemia should be treated in the perioperative period.
CONCLUSIONS:
Early identification and effective treatment of anemia has the potential to improve clinical outcomes in surgical patients.
Graphical Abstract
Mini-abstract
An international expert panel developed recommendations for anemia management in surgical patients. The panel recommends that all patients except those undergoing minor procedures be screened for anemia prior to surgery. Appropriate therapy should be guided by an accurate diagnosis. Early identification and effective treatment of anemia has the potential to improve clinical outcomes.
Introduction
As many as one-third of patients undergoing elective surgery are anemic preoperatively.1 The presence of preoperative anemia, even if mild, has been associated with increased risk of red blood cell (RBC) transfusion and increased morbidity and mortality following surgery.2, 3 In addition, transfusion of RBCs has been consistently associated with worsened clinical outcomes.4
Timely identification and appropriate management of anemia in the surgical population is necessary to optimize patient outcomes. Moreover, it has been suggested that clinicians should prioritize management of anemia as a disease independent of RBC transfusion thresholds.5 The etiology of preoperative anemia can be multifactorial, but almost two-thirds of anemic elective surgical patients have iron-deficiency anemia (IDA). At the same time, as many as one-third of non-anemic elective surgical patients are also iron deficient. The approach to the diagnosis and management of anemia in surgery has been evolving as more data have become available, both on pathophysiology and on how the underlying mechanism should influence therapy.
In recent years, heterogeneity has been observed in clinical trials of iron therapy for anemia management in surgical patients. Some randomized controlled trials (RCTs) have shown that iron therapy is beneficial,6–9 while others have reported a lack of benefit.10, 11 There is a need for clinical guidelines on anemia to be based on all the available data, including the most recent studies. An expert panel was convened by the Society for the Advancement of Patient Blood Management (SABM). Current evidence was reviewed to determine the prevalence, etiology, diagnosis and management of anemia in surgical patients, including outcome measures. The objective of the panel was to develop clinical recommendations for treatment of anemia in surgical populations, using modified RAND Delphi methodology.
Methods
ICCAMS panel
A group of experts in patient blood management (PBM) selected a multidisciplinary panel to participate in the International Consensus Conference on Anemia Management in Surgical Patients (ICCAMS). Fourteen individuals with expertise in anemia management and/or PBM and surgery were selected based on academic qualifications, subject matter expertise, and relevant clinical experience. All panel members reviewed the literature and established consensus recommendations on the diagnosis and management of anemia in patients undergoing surgery. Eight additional individuals reviewed the manuscript and contributed to its development. The roles of each individual are shown in the Supplemental Digital Content (Part 3; Supplementary table 1).
Literature review
Searches were performed using PubMed on 11 January 2021. The following search string was used: (anemia [tiab] OR anaemia [tiab]) AND (surgery [tiab] OR surgical [tiab]). The results were restricted to articles published in the preceding 10 years. ‘Publication type’ filters were applied in three different ways: clinical trial or randomized controlled trial (200 hits), systematic review (103 hits) and consensus development conference or guideline or practice guideline (19 hits). Thus, all types of clinical trials, systematic reviews and guidelines were considered. To include additional relevant literature (including observational or retrospective studies and articles published before 2011), reference lists of review and guideline publications were reviewed, and panel members provided input.
Initial screening, based on titles and abstracts, was performed to select relevant articles. Inclusion criteria for clinical trials were: clinical study performed in patients undergoing surgery, and presentation of data on the prevalence, impact or management of pre- or perioperative anemia. Preclinical studies (those conducted in vitro or in animals), and those focused on cancer treatment (except surgery for colorectal cancer) were excluded. For reviews and guidelines, the principal inclusion criterion was sufficient focus on the prevalence, impact or management of anemia around the time of surgery.
Panel survey
Statements were developed by selected members of the panel (AS, JM, AH, SO, MM). A multiple-choice format was chosen for collecting responses to each statement, and a 5-point Likert scale was applied where appropriate. All panel members completed the survey before attending a virtual meeting.
Achievement of consensus
In March 2021, the panel members attended the virtual ICCAMS meeting. The survey responses were discussed, and the RAND Delphi (modified) process was used to establish consensus. Consensus was defined according to the survey results, with a minimum agreement threshold of 75% of respondents agreeing (strongly agree/agree) or disagreeing (strongly disagree/disagree) with a survey statement.
During the meeting, discussions were focused on the survey questions with discordant responses. Statements for which there was consensus agreement or disagreement were not discussed unless specific questions were raised. Panel members were given an opportunity to change their responses and, where required, adjustments were made to the statements. All changes were agreed by vote. Where further clarification was needed, minor revisions to the consensus statements were made during manuscript development.
Role of the funding source
ICCAMS was a virtual meeting with no venue or travel costs. Literature search and manuscript development costs, and project development and management fees were funded by SABM via grants received from American Regent, Pharmacosmos, Vifor and Zuellig Pharma. Consulting fees/honoraria were offered to the authors.
Consensus statements
Prevalence and outcomes
Consensus statements: prevalence
Anemia is common in surgical populations.
Prevalence of anemia varies across surgical populations.
Supporting evidence: prevalence
In the general surgical population, anemia prevalence rates vary according to age and gender.12 The prevalence of anemia is markedly higher among females than males between the ages of 18 and 49 years, while the highest prevalence rate in both sexes is observed in the oldest age group (≥70 years). In a large meta-analysis that included 949,455 surgical patients from 24 studies, preoperative anemia had a prevalence rate of 39.1%.3 In 13 studies where preoperative anemia was defined according to World Health Organization (WHO) criteria (hemoglobin [Hb] <13 g/dL for males or Hb <12 g/dL for females), the prevalence rate was 29.9%.3 Similarly, in an analysis of 18 studies including >650,000 surgical patients, the mean prevalence of preoperative anemia was approximately 35%.13
The prevalence of anemia may be influenced by underlying illness and therefore differs between populations undergoing particular types of surgery.14 Muñoz et al. compared prevalence rates between surgical settings; as shown in Figure 1, the highest prevalence rates were observed in gynecologic and vascular surgery while the lowest rates were observed in orthopedic and urologic surgery.13 Prevalence of anemia in specific types of surgery has been reported in numerous clinical studies; further details on these studies can be found in the Supplemental Digital Content (Part 4; Evidence spreadsheet).
Figure 1.

Prevalence of preoperative anemia: variations across surgical settings. This figure has been adapted from Muñoz et al. 201513 (publisher: SIMTI Servizi Srl) in accordance with the terms and conditions of the Creative Commons Attribution license.
Consensus statements: outcomes
Low preoperative hemoglobin concentration is a risk for increased transfusion of blood components and/or poor clinical outcomes.
The relationship between anemia and outcomes is important in all types of surgery (elective, urgent and emergency).
Patients should be educated about the impact of anemia.
Patients should be educated about the relationship between anemia and RBC transfusion and the impact of increased RBC transfusion.
Supporting evidence: outcomes
Preoperative anemia
Data from large observational studies, including over 600,000 surgical patients, have shown that preoperative anemia is an independent risk factor for postoperative morbidity and mortality, as well as prolonged length of hospital stay.13 Preoperative anemia was also identified as an independent predictor of perioperative allogeneic blood transfusion (ABT). Similar results were reported in a separate meta-analysis that included 24 studies: preoperative anemia was associated with increased short-term mortality and increased rates of stroke, acute kidney injury (AKI) and infection postoperatively.3 Subsequently published systematic review articles have shown that anemia is associated with increased risk of surgical site infection, and that it is an independent risk factor for unplanned critical care admission after major surgery.15, 16
In a large retrospective study including over 300,000 non-cardiac surgery patients aged ≥65 years, each percentage-point decrease in the hematocrit value from the normal range was associated with a 1.6% (95% confidence interval, 1.1%–2.2%) increase in 30-day postoperative mortality.17 Mortality increased similarly with increases in hematocrit levels above the normal range. A subsequent retrospective analysis of 7,679 patients undergoing non-emergency, non-cardiac surgery showed that preoperative anemia is independently associated with increased mortality.18 The authors also observed that anemia increases the risk of transfusion. Two Austrian benchmark studies, conducted in cardiac, orthopedic and abdominal surgery, showed that the preoperative Hb level was one of the main predictors of RBC transfusion.19, 20 In a study of nonagenarians undergoing non-elective, non-trauma-related surgery, preoperative anemia was shown to be an independent risk factor for RBC transfusion.21 However, anemia had no significant impact on morbidity or mortality.21
Overall, there is strong evidence of correlations between anemia and a range of clinical outcomes. However, the panel acknowledged that anemia is not a confirmed cause of these outcomes; it is possible that anemia is a marker of other underlying morbidities that impair outcomes.
The importance of educating patients preoperatively about anemia and its correlation with post-surgical outcomes was recognized by the panel. Improved education is associated with increased adherence to treatment for anemia and may encourage dietary improvements, potentially leading to higher hemoglobin levels at the time of surgery.22–25
Results of clinical studies investigating outcomes associated with preoperative anemia in specific types of surgery are presented in the Supplemental Digital Content (Parts 1 and 4).
Perioperative and postoperative anemia
Blood loss is an important cause of perioperative anemia, and surgical bleeding increases the risks of morbidity and mortality because of the need for RBC transfusion and the occurrence of hemorrhagic shock or ischemia.26–29 In addition, if perioperative anemia remains undiagnosed and untreated, the patient may be placed at risk of negative outcomes including those described below for postoperative anemia.26
Postoperative anemia has been associated with worsened clinical outcomes. A recent study of patients with colorectal cancer reported that postoperative anemia was associated with increased RBC transfusion, longer length of hospital stay, impaired quality of life scores and lower overall survival at 5 years.30 In a retrospective analysis of 300 surgical patients who had declined RBC transfusions, the odds of death increased by a factor of 2.5 for each 1 g/dL decrease in postoperative Hb below 8 g/dL.31 A study of coronary artery bypass graft (CABG) patients showed that decreased postoperative Hb levels were associated with increased all-cause mortality.32 Postoperative anemia was also associated with an increased incidence of cardiovascular events. In orthopedic surgery, hospital stay has been shown to be prolonged when the severity of postoperative anemia is increased.33 As with preoperative anemia, the panel acknowledged that postoperative anemia is not a confirmed cause of worsened clinical outcomes and that it could instead be a marker of other underlying morbidities.
Screening and diagnosis
Consensus statements: screening
The prevalence of preoperative anemia and its association with worse clinical outcomes justify screening all patients for anemia before surgery, except those undergoing minor procedures.
Screening for preoperative anemia should not be restricted to patients undergoing elective surgery.
It is never too late to start anemia evaluation in patients undergoing elective or urgent surgery.
Supporting evidence: screening
The most commonly used criteria for defining anemia are the WHO definitions (Hb <12.0 g/dL for women or <13.0 g/dL for men). However, it has been suggested that these should be updated.34 A range of Hb cut-off levels for anemia have been used in studies. In an observational study of >4,000 adults undergoing elective cardiac surgery, a preoperative Hb concentration <13.0 g/dL was reported as the optimal threshold in women.35 Similarly, in a review by Muñoz et al., a Hb level <13.0 g/dL for both men and women was advocated for preoperative anemia, while the WHO criteria were considered acceptable for postoperative anemia.13 This approach was echoed in international consensus guidelines on the management of surgery-related anemia.1 Adoption of the 13.0 g/dL threshold in both genders has also been suggested in recent reviews of perioperative anemia and PBM.36, 37 Therefore, the panel supports defining anemia by a Hb level <13.0 g/dL in both men and women. To allow time for a response to therapy, at least 4 weeks prior to surgery has been suggested as the optimal time frame for evaluation.37, 38 However, treatment as little as 1 day before surgery (intravenous [IV] iron, subcutaneous erythropoietin alpha, vitamin B12, and oral folic acid) has been shown to be effective in reducing transfusion of allogeneic blood products in cardiac surgery patients with preoperative anemia.39
Opinions of the panel: screening
The panel agreed that the optimal time before surgery to screen for anemia is at least 4 weeks. However, shorter time frames such as in the case of urgent or emergent surgery should not preclude evaluation. The results of tests performed shortly before surgery may enable treatments with a rapid onset of action (e.g., IV iron) to be administered preoperatively, and they may also help define the need for anemia treatment postoperatively.
Minor procedures such as cataract surgery or other surgeries where testing requirements are waived because of no blood loss can be undertaken in patients with anemia, therefore there is no requirement for this population to be screened. However, due to the high frequency of anemia in the general population, patients undergoing all other types of surgery should be screened preoperatively. Screening may be beneficial by providing an opportunity to treat previously undiagnosed anemia, regardless of the setting. The importance of screening is heightened in those undergoing major surgery with at least moderate risk of clinically significant blood loss, those with risk factors for anemia or poor tolerance of anemia, and those unable to receive blood products.
Consensus statements: diagnosis
All patients with anemia should be evaluated for the cause of anemia – wherever possible, early enough preoperatively to enable sufficient time for treatment to be successful.
It is important to identify iron deficiency, including in patients with anemia of inflammation (or anemia of chronic disease).
Patients with iron deficiency anemia should be evaluated for the cause of the iron deficiency while patients with anemia and normal iron studies should be evaluated for coexisting causes of anemia (i.e., renal disease, primary hematologic disease, nutrition deficiency).
Evaluation for iron deficiency should include iron studies (serum iron, total iron binding capacity (TIBC), transferrin saturation (TSAT), serum ferritin); if available, reticulocyte hemoglobin content and/or serum hepcidin should be considered in inflammatory states.
The most important criteria for defining absolute iron deficiency were ferritin <30 ng/mL and/or TSAT <20%; ferritin <100 ng/mL may define iron deficiency in inflammatory states. If available, either a reticulocyte hemoglobin <29 pg or a serum hepcidin level <20 µg/L also suggest the presence of iron deficiency in inflammatory states.
Supporting evidence: diagnosis
In a study of 3,342 patients undergoing major elective surgery, the overall prevalence of anemia was 36%.40 Of the patients with anemia, 62% had absolute iron deficiency and another 5% had low iron stores.40 Therefore, all patients with anemia should be screened for iron deficiency. In some circumstances (e.g., planned surgery associated with large blood loss), it may also be appropriate to evaluate non-anemic surgical patients for iron deficiency.41 Patients with anemia who are not iron deficient should be evaluated for other causes of anemia (e.g., renal disease, primary hematologic disease, nutritional deficiencies). Determination of whether anemia is microcytic, normocytic, or macrocytic (in patients with reticulocyte production index <2) may help identify likely causes.42 Wherever possible, evaluations should be performed early enough preoperatively to enable sufficient time for treatment to be successful. In patients undergoing urgent/emergency procedures, blood samples for evaluation and classification of anemia should be drawn preoperatively, with the aim of testing promptly (preoperatively if possible).
Iron deficiency is considered to be present if ferritin <30 ng/mL and/or TSAT <20%. It has been considered uncommon in patients with anemia of inflammation (or anemia of chronic disease), but this may be attributable to difficulties using the usual iron parameters in this setting. Because ferritin is an acute-phase reactant in inflammatory states, ferritin levels are often elevated independent of iron status therefore a higher cut-off (<100 µg/L) is needed to define IDA in these settings.43 Also in inflammatory states, serum iron and total iron-binding capacity are generally low, limiting the utility of TSAT for diagnosing IDA.44 This may be explained by the potential for inflammation to dysregulate iron homeostasis.45, 46 The key regulator of iron homeostasis is hepcidin, a peptide that is produced primarily by hepatocytes. Increased hepcidin levels decrease iron absorption from the gut and iron release from macrophages and hepatocytes. In inflammatory states, hepcidin levels generally increase as a response to inflammatory cytokines and the net effect is decreased iron availability for erythropoiesis.45, 47, 48 Patients with inflammatory disorders and iron deficiency exhibit lower levels of hepcidin than those with ‘pure’ anemia of inflammation and, consequently, hepcidin levels can help distinguish between IDA and other anemias where there is no iron deficiency.49 The serum hepcidin level may be more reliable than ferritin or TSAT for identifying iron deficiency. For example, in patients discharged from the intensive care unit (ICU), a low hepcidin level (<20 µg/L) identified iron deficiency in 37% of patients in contrast to 6% identified by iron tests alone.50
Other laboratory parameters have also been suggested as candidates for identifying iron deficiency in inflammatory states. Reticulocyte Hb content is an early marker of iron deficiency that can identify patients who may respond to iron supplementation and is unaffected by inflammation.43, 51–53 A reticulocyte Hb content below 29 pg per cell is suggestive of IDA. The soluble transferrin receptor (sTfR) may also be useful because it is elevated in IDA and not by inflammation.53, 54 The ratio of sTfR and log of ferritin (ferritin index) has been used to identify IDA.53–55 At this point, hepcidin, reticulocyte Hb and sTfR testing are not readily available in many hospitals. However, as these tests become more generally available, they may become useful in clinical practice.
Several algorithms for the evaluation of anemia have been published, all of which have different strengths and weaknesses.1, 37, 56, 57 We suggest using the algorithm published in 2017 by Muñoz et al. as it has the benefit of simplicity and highlights the wide range of factors that can cause or contribute to anemia.1 Also, it is focused only on diagnosis and classification, meaning that it is not complicated by recommendations on treatment.
Management
Consensus statements: treatment of preoperative anemia
The aim of treating preoperative anemia is to improve hemoglobin concentration and this may decrease RBC transfusion.
Therapy should be tailored to the etiology of anemia.
Supporting evidence: treatment of preoperative anemia
As described above, preoperative anemia is associated with worsened clinical outcomes. Existing evidence also shows that treating this condition with iron therapy and/or erythropoiesis-stimulating agents (ESAs) may increase Hb levels and decrease RBC transfusion rates (see sections below). The data suggest that treatment of anemia should be initiated some time (e.g., several weeks) before surgery to enable the full effects to be attained.58, 59 However, there are differences between treatment modalities in their speed of onset, and combination therapy with IV iron, subcutaneous erythropoietin alpha, vitamin B12 and oral folic acid has been shown to be effective in the immediate perioperative period.39
Opinions of the panel: treatment of preoperative anemia
The treatment target in patients with preoperative anemia is usually to restore the Hb level to the normal range. The exact target Hb level may be affected by the clinical setting (e.g., lower in patients with renal disease) or by demographic characteristics. Additional data are needed to assess the impact of anemia treatment on clinical outcomes. The optimal timeframe to begin treating preoperative anemia prior to surgery is as soon as possible after surgery is scheduled, ideally at least 3–4 weeks in advance. However, a short time-frame prior to surgery should not preclude treatment.
Consensus statements: preoperative iron therapy
Iron therapy should be administered as treatment for preoperative iron-deficiency anemia, except when it is contraindicated.
IV iron is preferable to oral iron in preoperative iron-deficiency anemia.
Preoperative oral iron therapy should be started as early as possible.
Preoperative IV iron therapy should be started as early as possible.
Administration of IV iron is generally well tolerated and does not increase the patient’s risk of infection.
Supporting evidence: preoperative iron therapy
A systematic review and meta-analysis of preoperative IV iron in patients undergoing major surgery concluded that this intervention significantly decreases the blood transfusion rate and provides a significant but modest increase in Hb concentration preoperatively and >4 weeks postoperatively when compared with placebo or oral iron (Figure 2).58 Positive results were also reported in a systematic review and meta-analysis of perioperative iron therapy in acute major non-cardiac surgery.60 Patients receiving IV iron had lower 30-day mortality, reduced ABT and a lower risk of postoperative infection. However, most of the evidence was from small observational studies, meaning that the analysis was not sufficiently powered to formally recommend iron therapy. According to the authors of a comprehensive, narrative review, meta-analyses have demonstrated that preoperative treatment with IV iron increases Hb levels, reduces transfusion of RBCs, and improves patient outcomes.61
Figure 2.

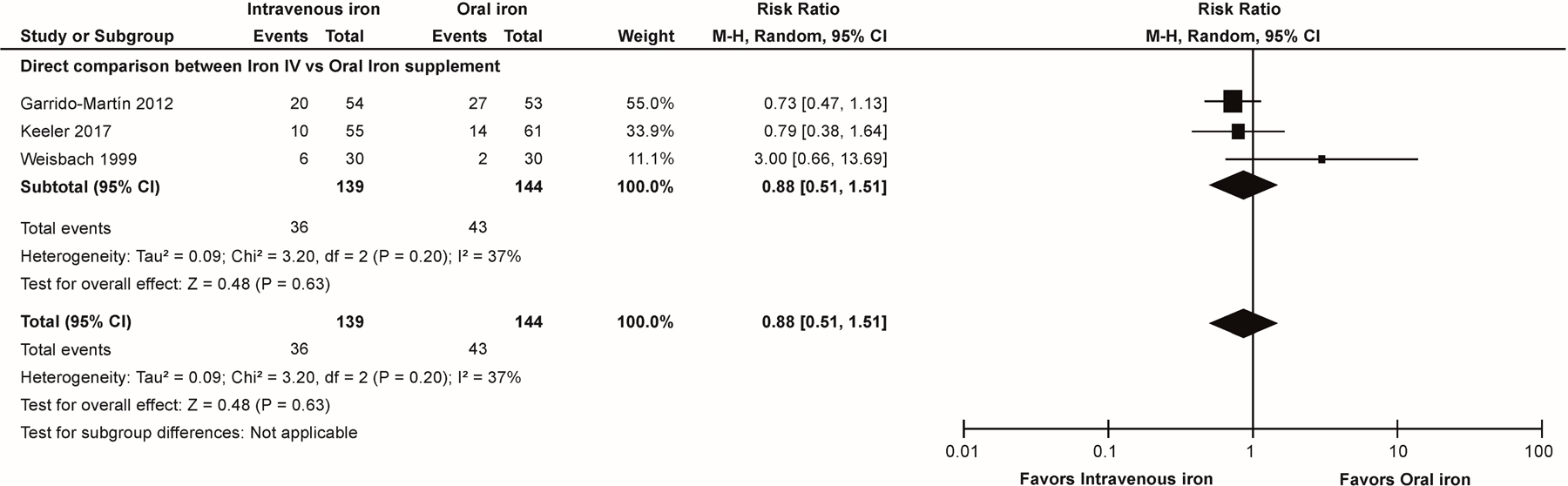



Meta-analysis of preoperative IV iron for preoperative correction of anemia in patients undergoing major surgery: comparisons of the effects of IV iron therapy versus placebo/standard care or oral iron on: proportion of participants receiving allogeneic blood transfusion (A, B); preoperative hemoglobin levels (g/dL; C, D); and hemoglobin levels >4 weeks postoperatively (g/dL; E). This figure has been adapted from Elhenawy et al. 202158 (publisher: BioMed Central Ltd, part of Springer Nature) in accordance with the terms and conditions of the Creative Commons Attribution license.
(A – comparison with placebo/standard care)
(B – comparison with oral iron)
(C – comparison with placebo/standard care)
(D – comparison with oral iron)
(E – comparison with placebo/standard care)
Other analyses have reported uncertainty regarding the effectiveness of iron therapy while citing a need for improved evidence. For example, in a systematic review and meta-analysis, Shah et al. reported no conclusive evidence that IV iron improves clinically important outcomes in non-elective surgery.62 A Cochrane review of iron therapy for preoperative anemia concluded that iron therapy did not produce a clinically significant reduction in the proportion of patients receiving an ABT compared to no iron therapy.63 Compared with oral iron, IV iron was associated with greater increases in Hb and ferritin, but the evidence for this was not considered reliable.
Data from 2006 show that the rates of adverse reactions to IV iron are low, at around 40 per million doses of low molecular weight iron dextran and 130 per million doses of high molecular weight iron dextran administered in the USA.64 The reported reactions included dyspnea, chest pain and hypotension. Some reactions (e.g., anaphylaxis) are potentially life-threatening, but these are rare (the incidence of anaphylaxis has been reported to be <4 per million doses).65 A recent meta-analysis reported an increased risk of infection with IV iron versus ‘no iron or oral iron’, but the extent of this increase was modest (relative risk, 1.16 [95% confidence interval 1.03–1.29]) and statistical significance was not observed when comparing IV iron with ‘no iron’ alone or ‘oral iron’ alone.66
Use of iron therapy in patients undergoing specific types of surgery has been investigated in numerous clinical studies and reviews. The placebo-controlled PREVENTT trial (whose design has been called into question) reported that preoperative IV iron before major abdominal surgery was not superior to placebo in reducing perioperative RBC transfusions or mortality, but hemoglobin levels 8 weeks and 6 months after surgery were increased (in line with meta-analyses) and the hospital readmission rate was lower.10, 67 Details of the publications can be found in the Supplemental Digital Content (Parts 1 and 4).
Opinions of the panel: preoperative iron therapy
The available data suggest that iron therapy as a treatment for preoperative anemia should be limited to patients with IDA. Iron therapy is contraindicated only in patients with an allergy to iron, and septic patients should have their infection controlled before iron therapy is commenced. Both oral and IV iron have been used to treat preoperative anemia. However, in general, IV iron may be preferable to oral iron due to high frequency of adverse effects, non-compliance, poor intestinal absorption in patients with inflammation, and the need for prolonged treatment (to ensure sufficient iron stores) associated with oral therapy.1, 58 Recent data suggest that IV iron therapy is typically well tolerated and effective.58, 60, 61 Treatment with IV iron (or oral iron) would ideally be started at least 3 weeks in advance of surgery to allow sufficient time for restoration of iron stores and for other treatment(s) in case of inadequate response.
The panel members perceived the risk of oxidative stress observations with IV iron to be low and of minimal clinical relevance. The potential for IV iron to increase the risk of infection appears to be relatively modest, and the available data may be confounded by factors such as variability in transfusion practices.66 Panel members believed that the possibility of hypophosphatemia in patients receiving IV iron is a question requiring more study.68
Consensus statements: preoperative treatment with ESAs
ESAs have a role in the preoperative treatment of anemia in surgery.
If ESAs are used, supplemental iron should also be given.
If ESAs are used, postoperative prophylactic treatment for thromboembolism should be considered.
Supporting evidence: preoperative treatment with ESAs
Anemia of inflammation (or anemia of chronic disease) is characterized by the failure of circulating erythropoietin concentrations to increase appropriately in response to a reduction in Hb.45 Inflammatory mediators inhibit erythropoietin production by the kidney and limit the responsiveness of erythropoietin receptors, leading to a reduction in erythropoiesis.45 The original rationale for ESA therapy was that increased erythropoiesis would result in higher Hb concentrations, reducing the need for RBC transfusions. Almost three decades ago, ESAs were approved for treating preoperative anemia in patients undergoing orthopedic surgery and other surgical procedures. However, in 2007, the FDA issued a Black Box Warning for ESAs based on data from clinical trials suggesting increased risk of death and other adverse events in patients with renal failure or cancer.69, 70 As a result, the perioperative use of ESAs to treat anemia has declined.
A number of RCTs of ESAs in surgical patients have been published, and the results have been summarized in four recent meta-analyses.59, 71–73 One of these, published by Van Remoortel et al., included 20 RCTs comparing preoperative ESA treatment (administered with oral or IV iron) versus placebo, usual care or no treatment in surgical patients.73 ESAs reduced the percentage of patients receiving transfusion and increased Hb concentrations, but safety data were not reported. The meta-analysis of Cho et al. included 32 RCTs (4750 patients) and showed that preoperative treatment of surgical patients with ESAs alone or in combination with iron were associated with reduced RBC transfusions and increased pre- and post-operative Hb levels in comparison with placebo.71 No increase in thromboembolic events was noted in this analysis. Analysis of data from 4,719 patients in 25 RCTs comparing ESAs plus iron with iron therapy alone showed that ESAs reduced the likelihood of RBC transfusion without increasing the risk of thromboembolic events.72 Finally, in a Cochrane review, Kaufner et al. identified 12 RCTs (1880 participants) comparing preoperative ESAs plus iron with either placebo, no treatment, or standard care with or without iron in non-cardiac surgery.59 Treatment with ESAs plus iron reduced the use of RBC transfusion and, at higher ESA doses (500–600 IU/kg), increased Hb concentration. There were no differences between the treatments in adverse events or mortality at 30 days.
Details of clinical studies and reviews of ESA therapy in patients undergoing specific types of surgery identified by our literature search can be found in the Supplemental Digital Content (Parts 1 and 4). The use of iron therapy and ESAs, according to clinical indications, is supported by several international guidelines (Supplemental Digital Content [Part 2]).1, 37, 56, 74–76
Opinions of the panel: preoperative treatment with ESAs
The available data suggest that ESAs are effective in treating perioperative anemia in surgery patients, including cardiac surgery. ESAs are particularly suitable for types of anemia that are not related to iron deficiency (e.g., anemia of inflammation). Case-by-case consideration of the risks and benefits of ESA utilization is important because the time available to treat anemia before surgery may vary. In addition, there is no standard ESA treatment protocol; the dose and duration of ESA treatment as well as the route and dose of supplemental iron have varied across studies. If ESAs are used, the treatment duration should be limited to the minimum clinically required, and concomitant IV iron should be given (partly as a means of reducing the risk of thrombocytosis). Concern regarding thromboembolic events remains, although the increase in risk appears to be small,77 and an RCT of ESA in critically ill patients showed that the incidence of thromboembolic events was not increased in those receiving prophylactic anticoagulation.78 Therefore, postoperative prophylactic anticoagulation therapy (a combination of pharmacologic therapy and intermittent pneumatic compression) should be considered for individuals receiving ESAs perioperatively. The importance of such therapy may be increased in cardiac surgery patients, due to the need for aspirin treatment to be discontinued before the surgical procedure. Future studies should help to refine the optimal ESA treatment protocol.
Consensus statements: perioperative transfusion of RBCs
RBC transfusion for the treatment of anemia adds risk.
The interaction of anemia and RBC transfusion contributes to poor outcomes.
Transfusion and anemia represent safety concerns.
RBC transfusion may be considered for severe, symptomatic postoperative anemia where clinical need cannot be met by volume replacement or hematinic medication alone.
Supporting evidence: perioperative transfusion of RBCs
RBC transfusion is the principal treatment for rapidly increasing the Hb concentration in hemodynamically unstable patients with severe anemia. This intervention can be an effective, potentially life-saving, intervention in critical bleeding.79 However, clinical data also show that RBC transfusions are associated with adverse outcomes. A multivariate, retrospective analysis compared 11,855 surgical patients who received one unit of RBCs intraoperatively with propensity-matched individuals who received no transfusion.4 This minimal dose of RBCs was associated with significant increases in mortality rates and a range of morbidity outcomes such as pulmonary complications, renal dysfunction, sepsis and length of postoperative hospital stay. Broader analysis including patients receiving larger quantities of RBCs showed that the risks of adverse outcomes were dose-dependent. A subsequent retrospective study, involving >1.5 million patients undergoing non-cardiac, non-intracranial, non-vascular surgery, assessed whether transfusion of 1 U RBCs affects the likelihood of perioperative ischemic stroke or myocardial infarction.80 Among patients receiving 1 U RBCs, compared with those receiving no RBCs, the adjusted odds ratio for perioperative stroke/myocardial infarction was 2.33 (95% CI 1.90 to 2.86). The odds ratio increased with increasing dose, to a maximum of 4.87 (95% CI 3.86 to 6.14) in patients receiving ≥4 U RBCs. These data suggest that reducing or limiting RBC transfusion would be beneficial.
PBM programs have been associated with reduced RBC transfusion, lower complication rates and reduced mortality.81 Preoperative treatment of anemia is an essential component of PBM in all types of surgery, and there is evidence that implementing multiple PBM measures provides benefits including reductions in transfusion, major complications, length of hospital stay and mortality.36
Details of further studies and reviews of RBC transfusion, including those focused on specific types of surgery, can be found in the Supplemental Digital Content (Parts 1 and 4). Guidelines on RBC transfusion thresholds identified by our literature search are also presented in the Supplemental Digital Content (Part 2).
Opinions of the panel: perioperative transfusion of RBCs
The panel recognizes the possible benefits of RBC therapy, particularly in patients with life-threatening bleeding. However, considering the associated risks, the panel recommends RBC transfusion only as temporary therapy for severe anemia (Hb levels below 7 g/dL), symptomatic anemia or active bleeding. RBCs should not be used to treat anemia that can be corrected with hematinic medications.
Consensus statement: postoperative anemia
The treatment of postoperative anemia should begin before discharge.
Supporting evidence: postoperative anemia
In a review of short-term perioperative iron therapy in major orthopedic surgery, postoperative oral iron was not found to increase Hb levels or reduce transfusion, but a risk of significant gastrointestinal adverse effects was demonstrated.82 Conversely, there was evidence that IV iron (with or without ESAs) may reduce the use of transfusion and/or accelerate recovery from postoperative anemia, with few clinically relevant adverse effects.82 In a previous systematic review and meta-analysis of postoperative oral and IV iron therapy following elective surgery, insufficient evidence was found to support the routine use of postoperative iron therapy in all elective surgery.83 IV iron was associated with a statistically significant increase in Hb, but it was questioned whether the extent of increase would be clinically meaningful. Oral iron had no significant impact on Hb versus control. The authors noted that much of the available evidence was from patients without preoperative iron deficiency.
Two hundred and one patients undergoing elective surgery with functional IDA on the first postoperative day were included in a randomized, placebo-controlled trial of IV iron.84 Active treatment produced a significantly greater increase in the Hb level, significant improvements in serum iron, iron saturation and serum ferritin, and a significant reduction in the incidence of blood transfusion.
Results of clinical studies investigating the management of postoperative anemia in specific types of surgery are presented in the Supplemental Digital Content (Parts 1 and 4). Published guidelines are also summarized in the Supplemental Digital Content (Part 2).
Conclusions
Anemia is common in surgical patients and the need to proceed with surgery in some patients with this condition is expected to persist in the near future. However, anemia is associated with worsened clinical outcomes and it may be a modifiable risk factor. We report consensus recommendations from an international group of experts. The panel recommended that patients should be screened for anemia before surgery, with accurate diagnosis of the etiology enabling initiation of the most appropriate preoperative therapy. In patients with IDA, IV iron is generally preferable to oral iron in the preoperative setting. As with preoperative anemia, postoperative anemia should be treated early (i.e., initiated before discharge from hospital). Given the high prevalence of anemia, early identification and effective treatment of this condition has the potential to improve clinical outcomes.
Supplementary Material
Acknowledgments
The authors thank Meridian HealthComms, Plumley, UK for providing support with the literature search and manuscript development, which was funded by SABM in accordance with Good Publication Practice (GPP3).
Funding
ICCAMS was a virtual meeting that did not require funding. The literature search and manuscript development were funded by SABM via grants received from American Regent, Pharmacosmos, Vifor and Zuellig Pharma. Dr Warner’s contribution to this project was supported by the US National Center for Advancing Translational Science (NCATS; CTSA grant number KL2 TR002379) and the US National Heart Lung and Blood Institute (NHLBI; grant number K23HL153310). The manuscript contents are solely the responsibility of the authors and do not necessarily represent the official views of the US National Institutes of Health (NIH).
Footnotes
Conflict of interest
MA has received research funding for data management from Covis Pharmaceuticals (formerly AMAG) and has participated in educational, non-promotional programs for Pfizer and Pharmacosmos. EB has received honoraria from Vifor Pharma and Sysmex for giving lectures. HLC has received honoraria from American Regent. JE has received payment from Vifor Pharma for giving lectures. SF has received honoraria from Ethicon Biosurgery for giving lectures, and funding from National Blood Authority (Australia) for traveling to and attending meetings. SMF has received honoraria from Haemonetics for scientific advisory board participation. DG has received honoraria from Vifor Pharma, for advisory board participation. AH received fees, honoraria or travel costs for consultancy or lecturing from: Celgene, G1 Therapeutics, International Foundation for Patient Blood Management, PBMe Solutions, South African National Blood Service, Takeda, TEM and Vifor. JFH has received honoraria from Pharmacosmos for consultancy and scientific presentations, and from Nordic Pharma for consultancy. JM received a project-linked scientific grant from Vifor Pharma. MM has received honoraria for lectures and/or consultancy from Pharmacosmos, Vifor Pharma and PharmaNutra. SO has received honoraria from Baxter Healthcare for consultancy. AS has received honoraria for consultancy and/or serving as a speaker for Merck, AMAG, Masimo Corp, CSL Behring, Vifor Pharma, Pharmacosmos, Pharmaniaga, Accumen and I-SEP, and has received research grants from Masimo Corp, CSL Behring, HbO2 Therapeutics and Werfen. DRS has received honoraria/travel support for consulting or lecturing from: Danube University of Krems (Austria), US Department of Defense, European Society of Anaesthesiology, Korean Society for Patient Blood Management, Korean Society of Anesthesiologists, Network for the Advancement of Patient Blood Management, Alexion Pharmaceuticals, Baxalta Switzerland, Bayer, B. Braun Melsungen, Boehringer Ingelheim, Bristol-Myers-Squibb, CSL Behring, Celgene International, Daiichi Sankyo, Haemonetics, Instrumentation Laboratory (Werfen), LFB Biomédicaments, Merck Sharp & Dohme, Novo Nordisk Health Care, PAION Deutschland, Pharmacosmos, Pfizer, Pierre Fabre Pharma, Portola Schweiz, Roche Diagnostics International, Sarstedt, Shire, Tem International, Vifor Pharma, Vifor International and Zuellig Pharma. RT has received honoraria from Zuellig Pharma for giving lectures. MAW receives research support through the National Heart, Lung, and Blood Institute of the National Institutes of Health (K23HL153310). JB, DF, TH, CKL, TWL and JS have no interests to declare.
Supplemental digital content
• Part 1: Clinical studies and reviews in specific types of surgery
• Part 2: Guidelines on clinical management
• Part 3: Supplementary tables
• Part 4: Evidence spreadsheet
References
- 1.Muñoz M, Acheson AG, Auerbach M, et al. International consensus statement on the peri-operative management of anaemia and iron deficiency. Anaesthesia 2017;72:233–247. [DOI] [PubMed] [Google Scholar]
- 2.Baron DM, Hochrieser H, Posch M, et al. Preoperative anaemia is associated with poor clinical outcome in non-cardiac surgery patients. Br J Anaesth 2014;113:416–423. [DOI] [PubMed] [Google Scholar]
- 3.Fowler AJ, Ahmad T, Phull MK, et al. Meta-analysis of the association between preoperative anaemia and mortality after surgery. Br J Surg 2015;102:1314–1324. [DOI] [PubMed] [Google Scholar]
- 4.Ferraris VA, Davenport DL, Saha SP, et al. Surgical outcomes and transfusion of minimal amounts of blood in the operating room. Arch Surg 2012;147:49–55. [DOI] [PubMed] [Google Scholar]
- 5.Shander A, Goodnough LT. Management of anemia in patients who decline blood transfusion. Am J Hematol 2018;93:1183–1191. [DOI] [PubMed] [Google Scholar]
- 6.Froessler B, Palm P, Weber I, et al. The Important Role for Intravenous Iron in Perioperative Patient Blood Management in Major Abdominal Surgery: A Randomized Controlled Trial. Ann Surg 2016;264:41–46. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Johansson PI, Rasmussen AS, Thomsen LL. Intravenous iron isomaltoside 1000 (Monofer®) reduces postoperative anaemia in preoperatively non-anaemic patients undergoing elective or subacute coronary artery bypass graft, valve replacement or a combination thereof: a randomized double-blind placebo-controlled clinical trial (the PROTECT trial). Vox Sang 2015;109:257–266. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Lidder PG, Sanders G, Whitehead E, et al. Pre-operative oral iron supplementation reduces blood transfusion in colorectal surgery - a prospective, randomised, controlled trial. Ann R Coll Surg Engl 2007;89:418–421. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Yoo YC, Shim JK, Kim JC, et al. Effect of single recombinant human erythropoietin injection on transfusion requirements in preoperatively anemic patients undergoing valvular heart surgery. Anesthesiology 2011;115:929–937. [DOI] [PubMed] [Google Scholar]
- 10.Richards T, Baikady RR, Clevenger B, et al. Preoperative intravenous iron to treat anaemia before major abdominal surgery (PREVENTT): a randomised, double-blind, controlled trial. Lancet 2020;396:1353–1361. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Urena M, Del Trigo M, Altisent OA, et al. Combined erythropoietin and iron therapy for anaemic patients undergoing transcatheter aortic valve implantation: the EPICURE randomised clinical trial. EuroIntervention 2017;13:44–52. [DOI] [PubMed] [Google Scholar]
- 12.Sim YE, Wee HE, Ang AL, et al. Prevalence of preoperative anemia, abnormal mean corpuscular volume and red cell distribution width among surgical patients in Singapore, and their influence on one year mortality. PLoS One 2017;12:e0182543. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Muñoz M, Gómez-Ramírez S, Campos A, et al. Pre-operative anaemia: prevalence, consequences and approaches to management. Blood Transfus 2015;13:370–379. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Clevenger B, Richards T. Pre-operative anaemia. Anaesthesia 2015;70 Suppl 1:20–28. [DOI] [PubMed] [Google Scholar]
- 15.McLaren AC, Lundy DW. AAOS Systematic Literature Review: Summary on the Management of Surgical Site Infections. J Am Acad Orthop Surg 2019;27:e717–e720. [DOI] [PubMed] [Google Scholar]
- 16.Onwochei DN, Fabes J, Walker D, et al. Critical care after major surgery: a systematic review of risk factors for unplanned admission. Anaesthesia 2020;75 Suppl 1:e62–e74. [DOI] [PubMed] [Google Scholar]
- 17.Wu WC, Schifftner TL, Henderson WG, et al. Preoperative hematocrit levels and postoperative outcomes in older patients undergoing noncardiac surgery. JAMA 2007;297:2481–2488. [DOI] [PubMed] [Google Scholar]
- 18.Beattie WS, Karkouti K, Wijeysundera DN, et al. Risk associated with preoperative anemia in noncardiac surgery: a single-center cohort study. Anesthesiology 2009;110:574–581. [DOI] [PubMed] [Google Scholar]
- 19.Gombotz H, Rehak PH, Shander A, et al. Blood use in elective surgery: the Austrian benchmark study. Transfusion 2007;47:1468–1480. [DOI] [PubMed] [Google Scholar]
- 20.Gombotz H, Rehak PH, Shander A, et al. The second Austrian benchmark study for blood use in elective surgery: results and practice change. Transfusion 2014;54:2646–2657. [DOI] [PubMed] [Google Scholar]
- 21.Pelavski AD, de Miguel M, Lacasta A, et al. Anaemia and transfusion in nonagenarians undergoing emergency, non-traumatic surgery: a prospective observational study. Transfus Med 2013;23:238–244. [DOI] [PubMed] [Google Scholar]
- 22.da Silva Lopes K, Yamaji N, Rahman MO, et al. Nutrition-specific interventions for preventing and controlling anaemia throughout the life cycle: an overview of systematic reviews. Cochrane Database Syst Rev 2021;9:CD013092. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Nahrisah P, Somrongthong R, Viriyautsahakul N, et al. Effect of Integrated Pictorial Handbook Education and Counseling on Improving Anemia Status, Knowledge, Food Intake, and Iron Tablet Compliance Among Anemic Pregnant Women in Indonesia: A Quasi-Experimental Study. J Multidiscip Healthc 2020;13:43–52. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Sharifirad G, Golshiri P, Shahnazi H, et al. PRECEDE educational model for controlling iron-deficiency anaemia in Talesh, Iran. J Pak Med Assoc 2011;61:862–865. [PubMed] [Google Scholar]
- 25.Yusoff H, Daud WN, Ahmad Z. Nutrition education and knowledge, attitude and hemoglobin status of Malaysian adolescents. Southeast Asian J Trop Med Public Health 2012;43:192–200. [PubMed] [Google Scholar]
- 26.Gómez-Ramírez S, Jericó C, Muñoz M. Perioperative anemia: Prevalence, consequences and pathophysiology. Transfus Apher Sci 2019;58:369–374. [DOI] [PubMed] [Google Scholar]
- 27.Shander A, Javidroozi M, Ozawa S, et al. What is really dangerous: anaemia or transfusion? Br J Anaesth 2011;107 Suppl 1:i41–59. [DOI] [PubMed] [Google Scholar]
- 28.Wu WC, Smith TS, Henderson WG, et al. Operative blood loss, blood transfusion, and 30-day mortality in older patients after major noncardiac surgery. Ann Surg 2010;252:11–17. [DOI] [PubMed] [Google Scholar]
- 29.Smilowitz NR, Oberweis BS, Nukala S, et al. Association Between Anemia, Bleeding, and Transfusion with Long-term Mortality Following Noncardiac Surgery. Am J Med 2016;129:315–323. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Moncur A, Chowdhary M, Chu Y, et al. Impact and outcomes of postoperative anaemia in colorectal cancer patients: a systematic review. Colorectal Dis 2021;23:776–786. [DOI] [PubMed] [Google Scholar]
- 31.Carson JL, Noveck H, Berlin JA, et al. Mortality and morbidity in patients with very low postoperative Hb levels who decline blood transfusion. Transfusion 2002;42:812–818. [DOI] [PubMed] [Google Scholar]
- 32.Westenbrink BD, Kleijn L, de Boer RA, et al. Sustained postoperative anaemia is associated with an impaired outcome after coronary artery bypass graft surgery: insights from the IMAGINE trial. Heart 2011;97:1590–1596. [DOI] [PubMed] [Google Scholar]
- 33.Sanoufa M, Smisson W, Floyd H, et al. The effect of anaemia on hospital length of stay in lumbar decompression and fusion procedures. J Perioper Pract 2015;25:267–271. [DOI] [PubMed] [Google Scholar]
- 34.Pasricha SR, Colman K, Centeno-Tablante E, et al. Revisiting WHO haemoglobin thresholds to define anaemia in clinical medicine and public health. Lancet Haematol 2018;5:e60–e62. [DOI] [PubMed] [Google Scholar]
- 35.Ripoll JG, Smith MM, Hanson AC, et al. Sex-Specific Associations Between Preoperative Anemia and Postoperative Clinical Outcomes in Patients Undergoing Cardiac Surgery. Anesth Analg 2021;132:1101–1111. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36.Spahn DR, Muñoz M, Klein AA, et al. Patient Blood Management: Effectiveness and Future Potential. Anesthesiology 2020;133:212–222. [DOI] [PubMed] [Google Scholar]
- 37.Warner MA, Shore-Lesserson L, Shander A, et al. Perioperative Anemia: Prevention, Diagnosis, and Management Throughout the Spectrum of Perioperative Care. Anesth Analg 2020;130:1364–1380. [DOI] [PubMed] [Google Scholar]
- 38.Geisser P, Burckhardt S. The pharmacokinetics and pharmacodynamics of iron preparations. Pharmaceutics 2011;3:12–33. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 39.Spahn DR, Schoenrath F, Spahn GH, et al. Effect of ultra-short-term treatment of patients with iron deficiency or anaemia undergoing cardiac surgery: a prospective randomised trial. Lancet 2019;393:2201–2212. [DOI] [PubMed] [Google Scholar]
- 40.Muñoz M, Laso-Morales MJ, Gómez-Ramírez S, et al. Pre-operative haemoglobin levels and iron status in a large multicentre cohort of patients undergoing major elective surgery. Anaesthesia 2017;72:826–834. [DOI] [PubMed] [Google Scholar]
- 41.Al-Naseem A, Sallam A, Choudhury S, et al. Iron deficiency without anaemia: a diagnosis that matters. Clin Med (Lond) 2021;21:107–113. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 42.Patel MS, Carson JL. Anemia in the preoperative patient. Med Clin North Am 2009;93:1095–1104. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 43.Camaschella C Iron-deficiency anemia. N Engl J Med 2015;372:1832–1843. [DOI] [PubMed] [Google Scholar]
- 44.Corwin HL, Gettinger A, Pearl RG, et al. The CRIT Study: Anemia and blood transfusion in the critically ill--current clinical practice in the United States. Crit Care Med 2004;32:39–52. [DOI] [PubMed] [Google Scholar]
- 45.Weiss G, Ganz T, Goodnough LT. Anemia of inflammation. Blood 2019;133:40–50. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 46.Sihler KC, Napolitano LM. Anemia of inflammation in critically ill patients. J Intensive Care Med 2008;23:295–302. [DOI] [PubMed] [Google Scholar]
- 47.Young B, Zaritsky J. Hepcidin for clinicians. Clin J Am Soc Nephrol 2009;4:1384–1387. [DOI] [PubMed] [Google Scholar]
- 48.Camaschella C, Girelli D. The changing landscape of iron deficiency. Mol Aspects Med 2020;75:100861. [DOI] [PubMed] [Google Scholar]
- 49.Girelli D, Nemeth E, Swinkels DW. Hepcidin in the diagnosis of iron disorders. Blood 2016;127:2809–2813. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 50.Lasocki S, Lefebvre T, Mayeur C, et al. Iron deficiency diagnosed using hepcidin on critical care discharge is an independent risk factor for death and poor quality of life at one year: an observational prospective study on 1161 patients. Crit Care 2018;22:314. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 51.Camaschella C New insights into iron deficiency and iron deficiency anemia. Blood Rev 2017;31:225–233. [DOI] [PubMed] [Google Scholar]
- 52.Abdul Gafor AH, Subramaniam R, Hadi F, et al. The role of reticulocyte hemoglobin content in the management of iron deficiency anemia in patients on hemodialysis. Nephro-Urol Mon 2018;10:e65629. [Google Scholar]
- 53.Thomas DW, Hinchliffe RF, Briggs C, et al. Guideline for the laboratory diagnosis of functional iron deficiency. Br J Haematol 2013;161:639–648. [DOI] [PubMed] [Google Scholar]
- 54.Shin DH, Kim HS, Park MJ, et al. Utility of Access Soluble Transferrin Receptor (sTfR) and sTfR/log Ferritin Index in Diagnosing Iron Deficiency Anemia. Ann Clin Lab Sci 2015;45:396–402. [PubMed] [Google Scholar]
- 55.Infusino I, Braga F, Dolci A, et al. Soluble transferrin receptor (sTfR) and sTfR/log ferritin index for the diagnosis of iron-deficiency anemia. A meta-analysis. Am J Clin Pathol 2012;138:642–649. [DOI] [PubMed] [Google Scholar]
- 56.National Blood Authority (NBA) [Australia] 2012;Pages https://www.blood.gov.au/pbm-module-2 on April 2021.
- 57.Society for the Advancement of Blood Management (SABM) 2014;Pages https://sabm.org/ on June 2021.
- 58.Elhenawy AM, Meyer SR, Bagshaw SM, et al. Role of preoperative intravenous iron therapy to correct anemia before major surgery: a systematic review and meta-analysis. Syst Rev 2021;10:36. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 59.Kaufner L, von Heymann C, Henkelmann A, et al. Erythropoietin plus iron versus control treatment including placebo or iron for preoperative anaemic adults undergoing non-cardiac surgery. Cochrane Database Syst Rev 2020;8:Cd012451. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 60.Schack A, Berkfors AA, Ekeloef S, et al. The Effect of Perioperative Iron Therapy in Acute Major Non-cardiac Surgery on Allogenic Blood Transfusion and Postoperative Haemoglobin Levels: A Systematic Review and Meta-analysis. World J Surg 2019;43:1677–1691. [DOI] [PubMed] [Google Scholar]
- 61.Peters F, Ellermann I, Steinbicker AU. Intravenous Iron for Treatment of Anemia in the 3 Perisurgical Phases: A Review and Analysis of the Current Literature. Anesth Analg 2018;126:1268–1282. [DOI] [PubMed] [Google Scholar]
- 62.Shah A, Palmer AJR, Fisher SA, et al. What is the effect of perioperative intravenous iron therapy in patients undergoing non-elective surgery? A systematic review with meta-analysis and trial sequential analysis. Perioper Med (Lond) 2018;7:30. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 63.Ng O, Keeler BD, Mishra A, et al. Iron therapy for preoperative anaemia. Cochrane Database Syst Rev 2019;12:Cd011588. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 64.Chertow GM, Mason PD, Vaage-Nilsen O, et al. Update on adverse drug events associated with parenteral iron. Nephrol Dial Transplant 2006;21:378–382. [DOI] [PubMed] [Google Scholar]
- 65.Gomez-Ramirez S, Shander A, Spahn DR, et al. Prevention and management of acute reactions to intravenous iron in surgical patients. Blood Transfus 2019;17:137–145. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 66.Shah AA, Donovan K, Seeley C, et al. Risk of Infection Associated With Administration of Intravenous Iron: A Systematic Review and Meta-analysis. JAMA Netw Open 2021;4:e2133935. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 67.Hofmann A, Gross I, Girelli D, et al. Iron deficiency in PREVENTT. Lancet 2021;397:668–669. [DOI] [PubMed] [Google Scholar]
- 68.Wolf M, Rubin J, Achebe M, et al. Effects of Iron Isomaltoside vs Ferric Carboxymaltose on Hypophosphatemia in Iron-Deficiency Anemia: Two Randomized Clinical Trials. JAMA 2020;323:432–443. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 69.Gilreath JA, Rodgers GM. How I treat cancer-associated anemia. Blood 2020;136:801–813. [DOI] [PubMed] [Google Scholar]
- 70.Aapro M, Gascon P, Patel K, et al. Erythropoiesis-Stimulating Agents in the Management of Anemia in Chronic Kidney Disease or Cancer: A Historical Perspective. Front Pharmacol 2018;9:1498. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 71.Cho BC, Serini J, Zorrilla-Vaca A, et al. Impact of Preoperative Erythropoietin on Allogeneic Blood Transfusions in Surgical Patients: Results From a Systematic Review and Meta-analysis. Anesth Analg 2019;128:981–992. [DOI] [PubMed] [Google Scholar]
- 72.Kei T, Mistry N, Curley G, et al. Efficacy and safety of erythropoietin and iron therapy to reduce red blood cell transfusion in surgical patients: a systematic review and meta-analysis. Can J Anaesth 2019;66:716–731. [DOI] [PubMed] [Google Scholar]
- 73.Van Remoortel H, Laermans J, Avau B, et al. Effectiveness of Iron Supplementation With or Without Erythropoiesis-Stimulating Agents on Red Blood Cell Utilization in Patients With Preoperative Anaemia Undergoing Elective Surgery: A Systematic Review and Meta-Analysis. Transfus Med Rev 2021;35:103–124. [DOI] [PubMed] [Google Scholar]
- 74.Cinnella G, Pavesi M, De Gasperi A, et al. Clinical standards for patient blood management and perioperative hemostasis and coagulation management. Position Paper of the Italian Society of Anesthesia, Analgesia, Resuscitation and Intensive Care (SIAARTI). Minerva Anestesiol 2019;85:635–664. [DOI] [PubMed] [Google Scholar]
- 75.National Clinical Guideline Centre. National Institute for Health and Care Excellence: Clinical Guidelines. Blood Transfusion London: National Institute for Health and Care Excellence (UK); 2015. [Google Scholar]
- 76.Kaufner L, von Heymann C 2018;Pages. Accessed at AWMF online at https://www.awmf.org/uploads/tx_szleitlinien/001-024l_S3_Praeoperative-Anaemie_2018-04-verlaengert.pdf on October 2021.
- 77.Litton E, Latham P, Inman J, et al. Safety and efficacy of erythropoiesis-stimulating agents in critically ill patients admitted to the intensive care unit: a systematic review and meta-analysis. Intensive Care Med 2019;45:1190–1199. [DOI] [PubMed] [Google Scholar]
- 78.Corwin HL, Gettinger A, Fabian TC, et al. Efficacy and safety of epoetin alfa in critically ill patients. N Engl J Med 2007;357:965–976. [DOI] [PubMed] [Google Scholar]
- 79.National Blood Authority (NBA) [Australia] 2011;Pages https://www.blood.gov.au/pbm-module-1 on April 2022.
- 80.Whitlock EL, Kim H, Auerbach AD. Harms associated with single unit perioperative transfusion: retrospective population based analysis. BMJ 2015;350:h3037. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 81.Althoff FC, Neb H, Herrmann E, et al. Multimodal Patient Blood Management Program Based on a Three-pillar Strategy: A Systematic Review and Meta-analysis. Ann Surg 2019;269:794–804. [DOI] [PubMed] [Google Scholar]
- 82.Gómez-Ramírez S, Maldonado-Ruiz M, Campos-Garrigues A, et al. Short-term perioperative iron in major orthopedic surgery: state of the art. Vox Sang 2019;114:3–16. [DOI] [PubMed] [Google Scholar]
- 83.Perelman I, Winter R, Sikora L, et al. The Efficacy of Postoperative Iron Therapy in Improving Clinical and Patient-Centered Outcomes Following Surgery: A Systematic Review and Meta-Analysis. Transfus Med Rev 2018;32:89–101. [DOI] [PubMed] [Google Scholar]
- 84.Khalafallah AA, Yan C, Al-Badri R, et al. Intravenous ferric carboxymaltose versus standard care in the management of postoperative anaemia: a prospective, open-label, randomised controlled trial. Lancet Haematol 2016;3:e415–425. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.