

Abstract
Importance:
Goals-of-care discussions are important for high-quality palliative care yet are often lacking for hospitalized older patients with serious illness.
Objective:
To evaluate a communication-priming intervention to promote goals-of-care discussions for hospitalized older patients with serious illness.
Design/Setting/Participants:
We conducted a pragmatic, parallel, 1:1 randomized trial of a communication-priming intervention compared to usual care in three US hospitals in one healthcare system, including a university, county, and community hospital. Eligible hospitalized patients were over age 55 with any of the chronic illnesses used by the Dartmouth Atlas project to study end-of-life care, or over age 80. We excluded patients with a documented goals-of-care discussion or palliative care consult during the current hospitalization prior to randomization.
Intervention:
Physicians and advance practice providers of patients randomized to the intervention received a one-page, patient-specific Jumpstart Guide to prompt and guide a goals-of-care discussion.
Main Outcomes:
The primary outcome was the proportion of patients with a natural language processing (NLP)-identified goals-of-care discussion within 30 days of randomization, based on data from the electronic health record. We also evaluated whether the intervention effect varied by age, sex, minoritized race or ethnicity, or history of dementia.
Results:
Of 3918 patients screened, 2512 were enrolled (mean age 71.7 years; 42% women; 12% Asian, 13% Black, 2% Native American or Pacific Islander, 70% White; 93% non-Hispanic, 6% Hispanic) and randomized (1255 to intervention, 1257 to usual care). The proportion of patients with goals-of-care discussions was 34.5% with intervention and 30.4% with usual care, for a hospital- and dementia-adjusted difference of 4.1% (95%CI 0.4%, 7.8%). Analyses of treatment effect modifiers suggested that the intervention had a larger effect size among patients of minoritized race or ethnicity. Among 803 patients of minoritized race or ethnicity, the hospital- and dementia-adjusted proportion with goals-of-care discussions was 10.2% (4.0%, 16.5%) higher in the intervention group than in the control group; whereas, among 1641 white non-Hispanic patients, the adjusted proportion with goals-of-care discussions was 1.6% (−3.0%, 6.2%) higher in the intervention group than in the control group. Differential effects of the intervention on the primary outcome by other characteristics were not detected.
Conclusions:
Among hospitalized older adults with serious illness, a clinician-facing Jumpstart intervention significantly improved documentation of goals-of-care discussions in the electronic health record, with a greater effect size in racially or ethnically minoritized patients.
Introduction
Goals-of-care communication for patients with serious illness has been associated with improved patient and family outcomes as well as reduced intensity of care at the end of life.1,2 However, conducting and documenting high-quality goals-of-care discussions with seriously ill patients remains a shortcoming in many health systems.2–7 Electronic health records (EHR) provide a key opportunity to identify patients who might benefit from goals-of-care discussions and to promote these discussions, yet prior interventions have not used the EHR to accomplish these objectives.8,9
Our previous randomized trials have examined a bi-directional “Jumpstart” Guide delivered to both patients and clinicians to promote goals-of-care discussions. The bi-directional Jumpstart Guide used pre-encounter patient surveys to populate one-page guides summarizing patient-specific communication and care preferences, as well as communication prompts including example language.7,10 In a randomized trial of outpatients with serious illness, this intervention increased the incidence of goals-of-care discussions at the targeted clinic visit from 31% to 74% (p<0.001), and increased patient-assessed quality of communication.7 A second pilot randomized trial of hospitalized patients with serious illness also showed that this bi-directional intervention increased the incidence of documented goals-of-care discussions from 8% to 21% (p=0.04) during the hospitalization.11 However, surveying patients or family members for preferences prior to the intervention made the bi-directional Jumpstart challenging to implement, owing to the resources required. Additionally, these two trials involved manual EHR review to assess documentation of goals-of-care discussions which is time intensive.11,12 These limitations highlight the need to evaluate the effectiveness of a more scalable implementation of the Jumpstart Guide, as well as more efficient methods to measure documented goals-of-care discussions for patients with serious illness.
This large pragmatic trial compared usual care with a clinician-facing-only, EHR-populated patient-specific Jumpstart Guide prompting clinicians to initiate goals-of-care discussions with hospitalized older patients with serious illness. Differential effects of the Jumpstart Guide were examined by patient age, sex, minoritized race or ethnicity, and whether they had dementia.
Methods
Overview:
This was a pragmatic, parallel, 1:1 randomized trial of intervention versus usual care. We used a waiver of informed consent, and all eligible patients were randomized. The waiver of informed consent was approved based on the rationale that the intervention was designed to promote standard of care. The protocol was published previously (Supplement 1).13 This study was approved by the University of Washington Human Subjects Committee (STUDY00007031) and registered at ClinicalTrials.gov (NCT04281784). A Data Safety Monitoring Committee acted in an advisory capacity, monitoring participant safety, evaluating the progress of the study, and reviewing procedures for maintaining the confidentiality of data and the quality of data collection, management, and analyses.
Setting:
The trial was conducted at three UW Medicine hospitals: two teaching hospitals, including a university hospital and a safety-net county hospital, and a community hospital. The university hospital is a quaternary-care academic medical center that provides subspecialty care to the region; it has 529 acute care beds and 86 ICU beds. The county hospital is a university-operated tertiary care hospital and regional referral center, and the sole Level 1 Trauma Center for a five-state region; it has 413 acute care beds and 89 ICU beds. The community hospital is academically affiliated and serves a large geriatric and nursing home resident population; it has 218 acute care beds and 15 ICU beds.
Patient population:
Eligible patients were hospitalized, 55 years of age or older, and identified using ICD-10 codes documented in the EHR during the 2 years prior to the hospitalization that indicated one or more of the nine chronic conditions used by the Dartmouth Atlas to study end-of-life care:14–16 dementia, cancers of poor prognosis, chronic pulmonary disease, coronary artery disease, heart failure, chronic liver disease, chronic renal disease, diabetes with end-organ damage, and peripheral vascular disease. These nine conditions account for 90% of deaths among Medicare beneficiaries in the US.17,18 To increase inclusivity of important and under-studied populations at high risk of hospital morbidity and mortality, we also included all hospitalized patients over age 80.19,20 To be eligible for randomization, patients had to be in the hospital for at least 12 hours and not more than 96 hours. Among patients meeting eligibility criteria, we enrolled those with no identified documentation of goals-of-care discussions or palliative care consultations during the current admission prior to the day of randomization as determined through manual daily screening of hospitalized patients.12,21–25 The following groups were considered ineligible: patients receiving a transplant in the prior year, patients currently on hospice or comfort care, admission for suicide attempt or psychiatric diagnosis, and prisoners or victims of violence. Clinicians were allowed to opt out of the study or ask that an individual patient not be included.
Sample size calculations:
With a target total sample size of 2000 (1000 per group) and two-sided significance level (α) of 0.05, we estimated 80% power to detect a difference in the proportion of patients with documented goals-of-care discussions of at least 6% between those randomized to Jumpstart and usual care. In our sample size calculation, we used the Normal approximation to the Binomial and assumed an average proportion with goals-of-care discussions of 0.54 based on the proportion among all participants in a prior trial of the Jumpstart Guide.
Randomization:
Patients were randomized in a 1:1 ratio, using variable size blocks ranging from 2 to 6, and stratified for dementia based on ICD-10 codes and hospital, using Visual Basic (Microsoft Access v16.0, Redmond, WA). Randomization occurred between April 2020 and March 2021. Enrollment was extended beyond the target sample size of 2000 to increase the number of patients with dementia; enrollment was concluded immediately prior to a change in the study sites’ health system’s EHR vendor to avoid anticipated stress associated with that change. Randomization occurred within the first 5 days of hospitalization.
Intervention:
We use automated methods to examine structured data elements in the EHR prior to randomization, identifying current code status as well as prior Physician Orders for Life-Sustaining Treatment (POLST) forms and advance directives; this information was included on a one-page Jumpstart Guide to inform goals-of-care discussions along with example language for conducting such discussions (Figure 1). We delivered the Jumpstart Guide to the primary hospital team (the attending physician as well as all resident physicians and advanced practice providers on the care team) via secure email. The email was sent once. We also sent one pager message to clinicians to alert them to the presence of the Jumpstart Guide in their email. Jumpstart Guides were delivered on the day of randomization.
Figure 1: Example Jumpstart Guide.
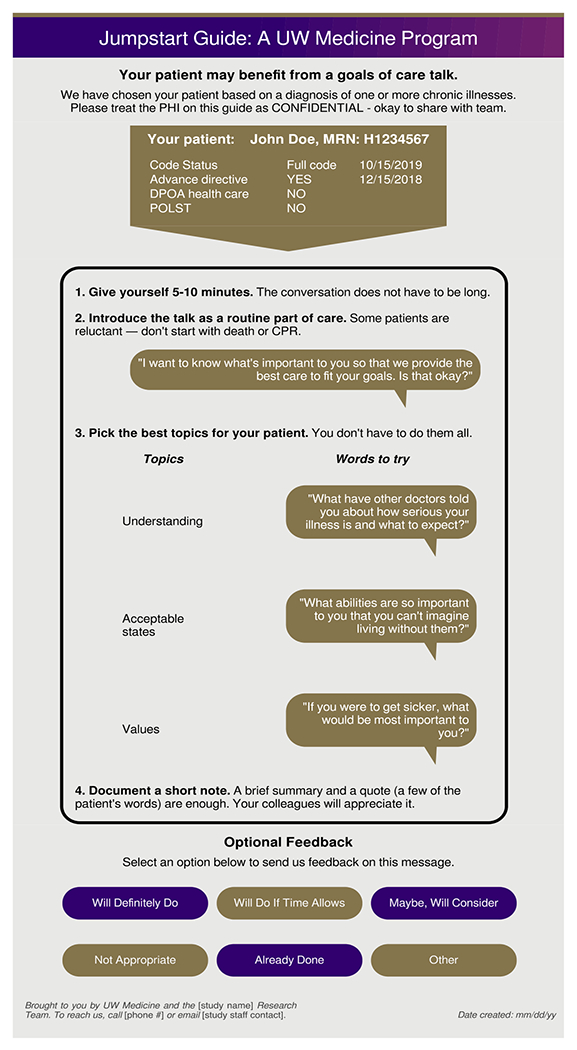
Jumpstart Guides were emailed to clinicians on the day of patient randomization. A message was sent to clinicians via their pager to alert them to the presence of the Jumpstart Guide in their email.
Outcomes and covariates:
The primary outcome was the cumulative incidence of EHR-documented goals-of-care discussions within 30 days of randomization, as identified by NLP-screened human abstraction26 which is described in a separate publication.27 Goals-of-care discussions were defined as discussions about a patient’s overarching goals for medical care;28 we did not consider discussions solely focused on code status to be goals-of-care discussions. To measure this outcome, we trained a deep-learning NLP model to screen EHR text for passages likely to contain documented goals-of-care discussions. Passages that screened positive by NLP were then reviewed by research coordinators to determine the presence or absence of documented goals-of-care discussions. We set the screening threshold to achieve 92.6% patient-level sensitivity of NLP-screened human abstraction in a 159-patient internal validation sample; this discrimination threshold corresponded with patient-level sensitivity of 99.2% and specificity of 33.2% of the NLP model functioning as a standalone classifier within the same validation sample.27 Randomization was concealed from abstractors, and instances of disagreement resolved by consensus.
Prespecified secondary outcomes obtained from the EHR were: utilization metrics associated with intensity of care (any ICU admissions, any ED visits, any palliative care consultations, and ICU- and hospital-free days) assessed at 30 days after randomization; hospital readmission within 7 days of discharge from the index hospitalization; and, mortality at 30 days after randomization using the EHR.
Race, ethnicity, and sex were collected from the EHR, and minoritized race or ethnicity was defined as either race other than White (i.e., Asian, Black, Native American, Pacific Islander) or Hispanic ethnicity. To identify participants with a history of dementia not captured by ICD-10 codes at randomization, research coordinators also performed a manual adjudication of EHR notes for dementia diagnoses.
Analysis:
Statistical analyses included five steps: 1) descriptive analyses of patient characteristics within the two randomization groups, 2) evaluation of the treatment effect of Jumpstart on the primary outcome, 3) evaluation of the treatment effect of Jumpstart on secondary outcomes, 4) evaluation of modifiers of treatment effect on the primary outcome, and 5) a sensitivity analysis. We followed the intention-to-treat principle for the primary analysis. The effect of the intervention on the primary outcome was quantified by the difference in proportions and evaluated with a linear regression model with robust standard errors. The primary analysis adjusted for hospital site and history of dementia as defined by ICD-10 code, since randomization was stratified on these factors. The effect of the intervention on secondary outcomes was quantified by the difference in proportions or means using similar regression models. For the primary outcome, we also evaluated whether the effect of the intervention varied by age, sex, minoritized race or ethnicity, and history of dementia. We combined minoritized race or ethnicity as our primary approach, and also explored differences in intervention effect among individual races and ethnicities. We conducted a sensitivity analysis evaluating differences in intervention effect by history of dementia as determined by the two methods of identifying dementia.
Analyses were completed with SPSS version 27 (IBM, Armonk, NY) and Stata IC Version 16.1 (StataCorp, College Station, TX).
Results
Study staff screened 3918 patients and enrolled 2512 patients; 1255 were randomized to intervention, and 1257 to usual care (Figure 2). The mean age was 71.7 (SD, 10.8) years; 1056 (42.0%) were female. For race, 12% were Asian, 13% were Black, 2% were Native American or Pacific Islander, 70% were White, and 3% were unknown. For ethnicity, 6% were Hispanic, 93% were non-Hispanic, and 1% were unknown. Of 2444 patients with reported race or ethnicity, 803 (33%) patients were of minoritized race or ethnicity. We identified 280 patients with dementia by ICD-10 codes (known at the time of randomization) “and an additional 75 with a history of dementia not captured by ICD-10 code that were identified after randomization by manual EHR review. Patient characteristics were similar between randomization groups (Table 1).
Figure 2: Eligibility assessment, randomization, and flow of patients through a trial of communication-priming for goals-of-care discussions.
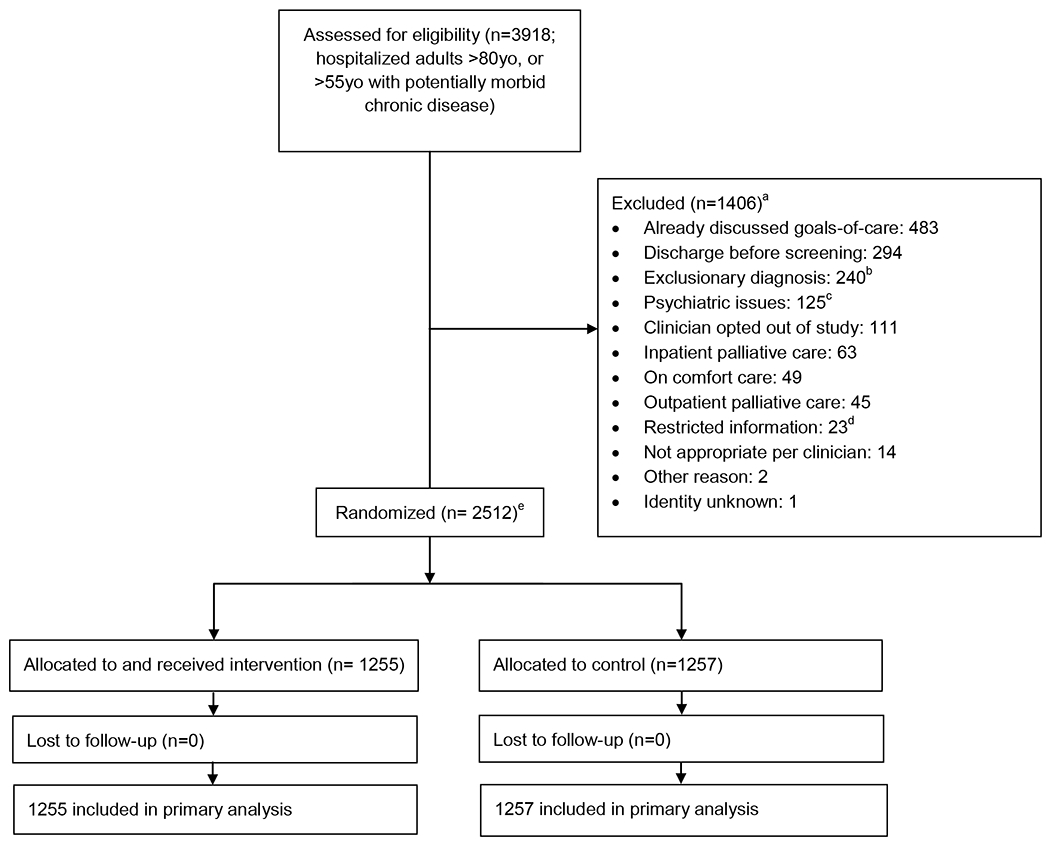
a The exclusions sum to more than the number of excluded patients because some patients were ineligible for >1 reason.
b Transplant within 1 year; CAR-T cell therapy; history of bone marrow transplant
c Suicidal ideation during current hospitalization; resident at inpatient psychiatric facility; transferring to or from psychiatric service
d Prisoner or other confidential record.
e Randomization stratified by site and Alzheimer Disease and related dementias (ADRD).
Table 1.
Sample Characteristics. Number (percentage) or median (IQR)
| Characteristic | Jumpstart Group | Usual Care |
|---|---|---|
| Group Size | 1,255 | 1,257 |
| Sex, n (%) | ||
| Female | 543 (43.3) | 513 (40.8) |
| Male | 712 (56.7) | 744 (59.2) |
| Race, n/N (%)a | ||
| Asian | 143/1218 (11.7) | 149/1216 (12.3) |
| Black | 168/1218 (13.8) | 148/1216 (12.2) |
| Native American | 21/1218 (1.7) | 24/1216 (2.0) |
| Pacific Islander | 4/1218 (0.3) | 9/1216 (0.7) |
| White | 882/1218 (72.4) | 886/1216 (72.9) |
| Ethnicity, n/N (%)a | ||
| Hispanic | 77/1248 (6.2) | 73/1249 (5.8) |
| Non-Hispanic | 1171/1248 (93.8) | 1176/1249 (94.2) |
| Minoritized Race and Ethnicity, n/N (%) | 409/1224 (33.4) | 394/1220 (32.3) |
| Age in years, median (IQR) | 70 (63, 80) | 70 (62, 80) |
| Marital Status, n/N (%) | ||
| Married | 502/1238 (40.5) | 515/1242 (41.5) |
| Single | 346/1238 (27.9) | 349/1242 (28.1) |
| Widowed | 199/1238 (16.1) | 187/1242 (15.1) |
| Divorced/separated | 191/1238 (15.4) | 191/1242 (15.4) |
| Limited (Spoken) English Proficiency, n (%) | ||
| No; preferred spoken English | 1,061 (84.5) | 1,078 (85.8) |
| Yes, preferred another spoken language: | 186 (14.8) | 171 (13.6) |
| Inapplicableb | 3 (0.3) | 0 (0.0) |
| Preferred language not documented | 5 (0.4) | 8 (0.6) |
| Chronic Illness (not mutually exclusive)c | ||
| Coronary artery disease | 424 (33.8) | 442 (35.2) |
| Heart failure | 356 (28.4) | 342 (27.2) |
| Lung disease | 339 (27.0) | 341 (27.1) |
| Kidney failure | 301 (24.0) | 326 (25.9) |
| Cancer | 300 (23.9) | 296 (23.5) |
| Peripheral vascular disease | 269 (21.4) | 269 (21.4) |
| Diabetes | 190 (15.1) | 196 (15.6) |
| Dementia (expanded definition)d | 172 (13.7) | 183 (14.6) |
| Liver disease | 163 (13.0) | 152 (12.1) |
| Dementia (definition used at randomization)d | 140 (11.2) | 140 (11.1) |
| Deyo-Charlson Comorbidity Index, median (IQR)e | 4 (2,6) | 5 (3,6) |
| Advance Directive in EHR prior to admission, n (%) | 97 (7.7) | 134 (10.7) |
| Designated Power of Attorney prior to enrollment, n (%) | 154 (12.3) | 167 (13.3) |
| Physician Orders for Life-Sustaining Treatment (POLST) prior to enrollment, n (%) | 94 (7.5) | 90 (7.2) |
| Hospital, n (%) | ||
| County hospital | 485 (38.6) | 487 (38.7) |
| University hospital | 442 (35.2) | 443 (35.2) |
| Community hospital | 328 (26.1) | 327 (26.0) |
Race and ethnicity were determined through EHR extraction of fixed categories.
Inapplicable indicates American Sign Language or need for interpreter to interpreter services
Chronic disease diagnoses were determined through EHR extraction of ICD codes relevant to each disease for the 24 months prior to the patient’s hospital admission.
History of dementia at the point of randomization was based on ICD diagnosis codes in the EHR any time during the 24 months prior to the patient’s hospital admission.
Deyo-Charlson Comorbidity Index was based on the sum of weighted scores assigned to 17 comorbidities (range, 0-26) identified using ICD9/ICD10 codes. Higher scores are prognostic of higher mortality.
Primary outcome
The number of patients with NLP-identified EHR documentation of a goals-of-care discussion within 30 days of randomization was 433 (34.5%) in the intervention group and 382 (30.4%) in the usual care group, with a difference in proportions of 4.1% (95%CI 0.4-7.8%; p=0.027; Table 2).
Table 2.
Effect of Clinician-Facing Jumpstart Guide on Primary and Secondary Outcomes
| Outcome | Jumpstart Group (n=1255) | Usual Care (n=1257) | Difference, % (95%CI)* | p |
|---|---|---|---|---|
| Primary Outcome | ||||
| NLP-identified documentation of a goals-of-care discussion, n (%) | 433 (34.5) | 382 (30.4) | 4.1 (0.4, 7.8) | 0.03 |
| Secondary outcomes: | ||||
| ICU care in 30 days after randomization, n (%) | 343 (27.3) | 356 (28.3) | −1.0 (−4.4, 2.5) | 0.58 |
| ED care in 30 days after randomization, n (%) | 217 (17.3) | 234 (18.6) | −1.3 (−4.3, 1.7) | 0.39 |
| Hospital readmission in 7 days after discharge, n (%) | 81 (6.5) | 90 (7.2) | −0.7 (−2.7, 1.3) | 0.48 |
| Death within 30 days after randomization, n (%) | 70 (5.6) | 64 (5.1) | 0.5 (−1.3, 2.2) | 0.59 |
| Palliative care consultation in 30 days after randomization, n (%) | 63 (5.0) | 62 (4.9) | 0.001 (−1.6, 1.8) | 0.91 |
| Days out of ICU and alive in 30 days after randomization, mean (SD) | 27.8 (6.2) | 27.9 (6.1) | −0.08 (−0.6, 0.4) | 0.75 |
| Days out of hospital and alive in 30 days after randomization, mean (SD) | 21.6 (9.1) | 22.0 (8.7) | −0.4 (−1.1 0.3) | 0.31 |
| Days in hospital after randomization, mean (SD) | 8.4 (11.9) | 8.1 (12.1) | 0.3 (−0.6, 1.3) | 0.48 |
Difference, 95% confidence interval, and p-value from linear regression models adjusted for history of dementia (as measured at the time of randomization) and hospital site.
Secondary outcomes
We did not observe significant differences in the secondary outcomes between treatment groups (Table 2). In the intervention group, 27.3% were admitted to an ICU within 30 days after randomization compared to 28.3% in the usual care group (risk difference −1.0%; 95%CI −4.4%, +2.5%). For emergency department use within 30 days of randomization, 17.3% of the intervention group had visits compared to 18.6% in the usual care group (risk difference −1.3%; 95%CI −4.3%, +1.7%). In each group, the mean number of days within 30 days after randomization that were spent alive and out of the hospital was about 22, and number of days alive and out of the ICU was about 28; 95% confidence intervals for the differences in mean days between groups ranged from about a day less to a half-day more. In each group, the mean duration of the index hospitalization from randomization was about 8 days. The vast majority of patients were discharged within 30 days (95.5% in intervention and 96.1% in usual care). Mortality at 30 days post randomization was 5.6% in the intervention and 5.1% in the usual care group (difference 0.5%; 95%CI −1.3%, +2.2%).
Modifiers of treatment effect on the primary outcome
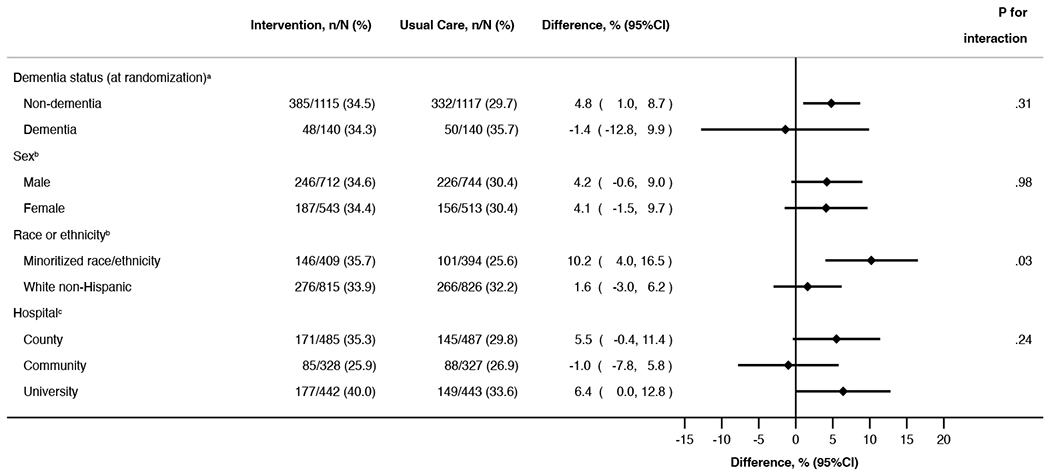
There was a statistically significant interaction between intervention and minoritized race or ethnicity (p=0.03). Among 803 patients of minoritized race or ethnicity, after adjustment for hospital and history of dementia, the proportion with goals-of-care discussions was 10.2% (95% CI 4.0%, 16.5%) higher in the intervention group than in the control group; among non-Hispanic white patients, the adjusted proportion with goals-of-care discussions was 1.6% (95% CI −3.0%, 6.2%) higher in the intervention group (Table 3). Analyses by individual races and ethnicities were generally consistent with these findings, although limited by sample sizes (Supplement 2, eTable 1). We did not see evidence of differential treatment effect by sex, diagnosis of dementia, or hospital as defined by the test for an interaction effect (Table 3). There was also no evidence of differential treatment effect by patient age.
Table 3.
Comparison of Subgroups with Regard to Associations between the Intervention Effect and the Occurrence of Goals-of-Care Discussions
|
Differences and 95% confidence interval are adjusted for hospital.
Differences and 95% confidence interval are adjusted for history of dementia at randomization and hospital.
Differences and 95% confidence interval are adjusted for history of dementia at randomization.
Sensitivity Analysis:
In our sensitivity analysis where we defined dementia by ICD-10 or manual abstraction, results were similar.
Discussion
Among hospitalized older adults with serious illness, a clinician-facing communication-priming “Jumpstart” intervention significantly improved documentation of goals-of-care discussions in the electronic health record, with a greater effect size in racially or ethnically minoritized patients. These findings suggest that clinician-facing prompting interventions may promote goals-of-care discussions, particularly among racially or ethnically minoritized patients.
These findings are consistent with studies of other clinician-facing communication priming interventions that have been tested in the outpatient setting with patients with serious illness. In one study of a clinician-facing intervention for patient with cancer, goals-of-care discussions in the treatment group increased from 1.3% to 4.6%;29 and, studies of a cancer clinician-directed communication training intervention with patient-specific communication prompts demonstrated reductions in patient-reported anxiety and depression.30,31 Similarly, our prior trial of a bilateral, patient- and clinician-facing Jumpstart Guide for outpatients with chronic life-limiting illness also found that the Jumpstart Guide was associated with an increase in patient-reported goals-of-care discussions.7 Notably, the proportion of control-arm patients with documented goals-of-care discussions was much lower in this current trial than in the previous outpatient trial. This may be due to differences in Jumpstart implementation (clinician-facing-only in this study vs. patient- and clinician-facing in the outpatient trial), control arm (usual care vs. usual care with consent for enrollment and participant surveys), differences in serious illness communication between outpatient and inpatient clinical settings, or differences in the definition of the primary outcome.
Given the importance of goals-of-care discussions to patients, families and clinicians,32–35 as well as research suggesting that communication priming interventions may be effective in the hospital setting,36 we previously conducted a pilot study7 for the current trial using a bi-directional Jumpstart Guide for hospitalized patients.11 This pilot study found a very small number of goals-of-care discussions in the EHR overall (2% of 4642 notes for 150 patients), and a larger effect size than the current study (8% control vs. 21% intervention). The differences in findings between the pilot trial and this study may be explained by a number of factors. The current study: 1) is pragmatic and does not require participant consent; 2) is based on EHR data only, with no survey data collected or used; 3) tests a clinician-facing Jumpstart Guide populated solely by EHR data, whereas the pilot trial tested a bi-directional Jumpstart that required patient surveys to populate; 4) was conducted at 3 hospitals, including a community site, whereas the pilot was conducted at 2; 5) has a larger proportion of patients with history of dementia; and 6) measured the primary outcome over a different time period using NLP rather than whole-chart manual abstraction. We hypothesize that the “higher touch” design of the pilot trial (e.g., survey-based “tips”, bi-directional distribution) may account for much of the difference in effect, as the bi-directional Jumpstart is designed to activate both clinicians and patients towards having a goals-of-care discussion. Additionally, we observed a much lower control-group proportion of patients with goals-of-care discussions in the pilot trial compared to this study. Although the exact reason for this is unclear, we hypothesize that the two studies’ substantial differences in screening, eligibility, and consent procedures may have led to systematic differences in the characteristics of patients enrolled.
An appealing feature of the pragmatic design of the current study is the ability to disseminate the intervention on a much wider scale than what can be achieved when requiring patient informed consent and completion of surveys. The size of the treatment effect found in this study is of unclear clinical significance, although the study suggests that such a nudge intervention can change clinician behavior. To have a more robust effect on goals-of-care discussions and change healthcare utilization, it seems likely that a stronger intervention is needed or that a clinician-facing Jumpstart Guide should be one component of a multi-faceted intervention.
Although the aim of promoting goals-of-care discussions during hospitalization for acute illness is to promote “in-the-moment” decision-making for patients with serious illness,37 it is noteworthy that we did not detect a statistically significant difference in secondary utilization outcomes between randomization groups. This failure to influence utilization may be attributable to both substantive and methodological factors. For example, goals-of-care discussions and their documentation may be of poor quality, failing to appropriately and adequately assess and describe patients’ goals or values and how they relate to patients’ treatment preferences.3–6 Even if goals-of-care discussions are conducted and well-documented, they may not be optimally timed for or optimally designed to meet patients’ needs; as such, utilization outcomes may only be tenuously linked to the types of discussions promoted by the Jumpstart intervention. Furthermore, goals-of-care documentation may be difficult for other clinicians to find and access; such documentation, even when present in the EHR, may not allow treating clinicians to shape care plans based on these prior discussions.38–40 There remains much to be understood about the timeliness, content, quality, and documentation of goals-of-care discussions, and the relationship of these quality metrics and process measures with patient-centered, clinical, and utilization outcomes.
An important finding of this study is that the Jumpstart Guide appeared to be more beneficial among racially or ethnically minoritized patients in increasing NLP-identified goals-of-care discussions. Racially and ethnically minoritized patients were one of several subgroup analyses that must be interpreted with caution. However, there are important racial and ethnic disparities in palliative and end-of-life care: minoritized patient populations are less likely to receive hospice services,41 more likely to receive higher intensity care near the end of life,42,43 and more likely to report concerns regarding quality of care and provider communication.44 Importantly, racially and ethnically minoritized patients with serious illness are also less likely to have EHR-documented goals-of-care discussions during an acute care hospitalization.45 These disparities highlight a need for race-conscious research efforts in palliative care,46 and provide a strong rationale for developing interventions that can address these inequities. A prior non-randomized controlled trial of an advance care planning video and communication intervention also showed increased benefit among Black and Hispanic patients.47 Our findings suggest that interventions to promote goals-of-care discussions may offer a useful approach to improve equity in serious illness communication.
Limitations
This study has many limitations. First, it was conducted in one region and one healthcare system, which may limit generalizability. Second, because data were extracted from electronic health records from a single healthcare system, findings are susceptible to measurement error in exposures and outcome misclassification, including outcomes occurring in other health systems.48 We mitigated this risk by focusing outcomes within 30 days rather than longer time periods and by assessing variables that are reliably documented in the EHR (demographic information, comorbidities).49 Third, our findings may be biased by differential performance of NLP over randomization group, or minoritized race or ethnicity. We believe this to be unlikely because the Jumpstart intervention does not modify existing documentation workflows, and the NLP model was trained on data that contained no textual documentation of Jumpstart or study-related activities. We also did not observe differential performance over these variables in our internal validation sample (Supplement 3, eFigures 1a and 1b). Fourth, the construct of a goals-of-care discussion represents a spectrum of important discussions that are multifaceted and vary over dimensions of context, timing, depth, content, and execution, all of which influence its quality.50 We are continuing to refine the criteria by which goals-of-care discussions are defined and measured.27,45 Fifth, we combined multiple racial and ethnic groups into a single category for analyses. When racial subgroups and Hispanic ethnicity were examined separately in a prior study, the finding of decreased occurrence of goals-of-care discussions was maintained for patients who identify as Black or Asian.45 However, future studies should strive to achieve power to examine groups separately.
Conclusions
Among hospitalized older adults with serious illness, a clinician-facing Jumpstart intervention significantly improved documentation of goals-of-care discussions in the electronic health record, with a greater effect size in racially or ethnically-minoritized individuals.
Supplementary Material
KEY POINTS.
Question:
Can a patient-specific, clinician-facing communication priming intervention with discussion prompts (Jumpstart) effectively promote goals-of-care discussions between clinicians and hospitalized, older patients with serious illness?
Findings:
In this pragmatic, randomized clinical trial of 2,512 hospitalized patients, the clinician-facing Jumpstart intervention resulted in a significant increase in the proportion of patients with a documented goals-of-care discussion within 30 days (34.0% of patients in Jumpstart group vs. 29.9% in usual care). The effect of the intervention was greater among racially or ethnically minoritized patients.
Meaning:
These findings suggest that clinician-facing prompting interventions promote goals-of-care discussions, particularly among racially or ethnically minoritized patients.
Funding support:
Funding support was provided by the National Institute on Aging (R01 AG062441) and a grant from the Cambia Health Foundation The funders had no role in the design and conduct of the study; collection, management, analysis, and interpretation of the data; preparation, review, or approval of the manuscript; or decision to submit the manuscript for publication.
Footnotes
Clinical Trials Registration: NCT04281784
Data Access, Responsibility and Analysis
Dr. Engelberg had full access to all the data in the study and takes responsibility for the integrity of the data and the accuracy of the data analysis. The following individuals conducted the data analyses: Lyndia C. Brumback, PhD1, Robert Y. Lee MD MS2, Lois Downey MA2,
1 Department of Biostatistics, University of Washington, Seattle;
2 Cambia Palliative Care Center of Excellence, University of Washington, Seattle, WA; Division of Pulmonary, Critical Care and Sleep Medicine, Department of Medicine, University of Washington, Seattle, WA;
Additional information
Who can access the data: Researchers with interest in improving communication around goals-of-care for older adults with serious illness.
Mechanisms of data availability: The de-identified EHR data will be made available in the form of a database with no personally-identifying characteristics retained in order to protect the identity of participants.
Data Sharing Statement
Data
Data Available: Yes
Data Types: Participants’ de-identified health record data
How to access data: Participants’ de-identified EHR data may be requested from study investigators; use of data will require completion of a Data Use Agreement.
REFERENCES
- 1.Detering KM, Hancock AD, Reade MC, Silvester W. The impact of advance care planning on end of life care in elderly patients: randomised controlled trial. BMJ. 2010;340:c1345. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Wright AA, Zhang B, Ray A, et al. Associations between end-of-life discussions, patient mental health, medical care near death, and caregiver bereavement adjustment. JAMA. 2008;300(14):1665–1673. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Fakhri S, Engelberg RA, Downey L, et al. Factors Affecting Patients’ Preferences for and Actual Discussions About End-of-Life Care. J Pain Symptom Manage. 2016;52(3):386–394. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Heyland DK, Dodek P, You JJ, et al. Validation of quality indicators for end-of-life communication: results of a multicentre survey. CMAJ. 2017;189(30):E980–E989. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Silveira MJ, Kim SY, Langa KM. Advance directives and outcomes of surrogate decision making before death. N Engl J Med. 2010;362(13):1211–1218. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Teno JM, Gruneir A, Schwartz Z, Nanda A, Wetle T. Association between advance directives and quality of end-of-life care: a national study. J Am Geriatr Soc. 2007;55(2):189–194. [DOI] [PubMed] [Google Scholar]
- 7.Curtis JR, Downey L, Back AL, et al. Effect of a Patient and Clinician Communication-Priming Intervention on Patient-Reported Goals-of-Care Discussions Between Patients With Serious Illness and Clinicians: A Randomized Clinical Trial. JAMA Intern Med. 2018;178(7):930–940. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Aslakson RA, Reinke LF, Cox C, Kross EK, Benzo RP, Curtis JR. Developing a Research Agenda for Integrating Palliative Care into Critical Care and Pulmonary Practice To Improve Patient and Family Outcomes. J Palliat Med. 2017;20(4):329–343. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Tulsky JA, Beach MC, Butow PN, et al. A Research Agenda for Communication Between Health Care Professionals and Patients Living With Serious Illness. JAMA Intern Med. 2017;177(9):1361–1366. [DOI] [PubMed] [Google Scholar]
- 10.Au DH, Udris EM, Engelberg RA, et al. A randomized trial to improve communication about end-of-life care among patients with COPD. Chest. 2012;141(3):726–735. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Lee RY, Kross EK, Downey L, et al. Efficacy of a Communication-Priming Intervention on Documented Goals-of-Care Discussions in Hospitalized Patients With Serious Illness: A Randomized Clinical Trial. JAMA Netw Open. 2022;5(4):e225088. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Curtis JR, Sathitratanacheewin S, Starks H, et al. Using Electronic Health Records for Quality Measurement and Accountability in Care of the Seriously Ill: Opportunities and Challenges. J Palliat Med. 2018;21(S2):S52–S60. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Curtis JR, Lee RY, Brumback LC, et al. Improving communication about goals of care for hospitalized patients with serious illness: Study protocol for two complementary randomized trials. Contemp Clin Trials. 2022;120:106879. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Goodman DC, Fisher ES, Wennberg JE, Skinner JS, Chasan-Taber S, Bronner KK. In: Tracking Improvement in the Care of Chronically Ill Patients: A Dartmouth Atlas Brief on Medicare Beneficiaries Near the End of Life. Lebanon (NH)2013. [PubMed] [Google Scholar]
- 15.Wennberg JE, Fisher ES, Goodman DC, Skinner JS. In: Tracking the Care of Patients with Severe Chronic Illness: The Dartmouth Atlas of Health Care 2008. Lebanon (NH)2008. [PubMed] [Google Scholar]
- 16.Iezzoni LI, Heeren T, Foley SM, Daley J, Hughes J, Coffman GA. Chronic conditions and risk of in-hospital death. Health Serv Res. 1994;29(4):435–460. [PMC free article] [PubMed] [Google Scholar]
- 17.Wennberg JE, Bronner K, Skinner JS, Fisher ES, Goodman DC. Inpatient care intensity and patients’ ratings of their hospital experiences. Health Aff (Millwood). 2009;28(1):103–112. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Wennberg JE, Fisher ES, Stukel TA, Skinner JS, Sharp SM, Bronner KK. Use of hospitals, physician visits, and hospice care during last six months of life among cohorts loyal to highly respected hospitals in the United States. BMJ. 2004;328(7440):607. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Zaslavsky O, Zelber-Sagi S, LaCroix AZ, et al. Comparison of the Simplified sWHI and the Standard CHS Frailty Phenotypes for Prediction of Mortality, Incident Falls, and Hip Fractures in Older Women. J Gerontol A Biol Sci Med Sci. 2017;72(10):1394–1400. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Fried LP, Tangen CM, Walston J, et al. Frailty in older adults: evidence for a phenotype. J Gerontol A Biol Sci Med Sci. 2001;56(3):M146–156. [DOI] [PubMed] [Google Scholar]
- 21.Hicks K, Downey L, Engelberg RA, et al. Predictors of Death in the Hospital for Patients with Chronic Serious Illness. J Palliat Med. 2017. [DOI] [PubMed] [Google Scholar]
- 22.Lavin K, Davydow DS, Downey L, et al. Effect of Psychiatric Illness on Acute Care Utilization at End of Life From Serious Medical Illness. J Pain Symptom Manage. 2017;54(2):176–185 e171. [DOI] [PubMed] [Google Scholar]
- 23.Sathitratanacheewin S, Engelberg RA, Downey L, et al. Temporal trends between 2010 and 2015 in intensity of care at end-of-life for patients with chronic illness: Influence of age under versus over 65 years. J Pain Symptom Manage. 2017;55(1):75–81. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Brown CE, Engelberg RA, Sharma R, et al. Race/ethnicity, socioeconomic status, and healthcare intensity at the end of life. J Palliat Med. 2018;21(9):1308–1316. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Steiner JM, Kirkpatrick JN, Heckbert SR, et al. Identification of adults with congenital heart disease of moderate or great complexity from administrative data. Congenit Heart Dis. 2018;13(1):65–71. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Lindvall C, Deng CY, Moseley E, et al. Natural Language Processing to Identify Advance Care Planning Documentation in a Multisite Pragmatic Clinical Trial. J Pain Symptom Manage. 2022;63(1):e29–e36. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Lee RY, Kross EK, Torrence J, et al. Assessment of Natural Language Processing of Electronic Health Records to Measure Goals-of-Care Discussions as a Clinical Trial Outcome. JAMA Netw Open. 2023;6(3):e231204. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Secunda K, Wirpsa MJ, Neely KJ, et al. Use and Meaning of “Goals of Care” in the Healthcare Literature: a Systematic Review and Qualitative Discourse Analysis. J Gen Intern Med. 2020;35(5):1559–1566. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Manz CR, Parikh RB, Small DS, et al. Effect of Integrating Machine Learning Mortality Estimates With Behavioral Nudges to Clinicians on Serious Illness Conversations Among Patients With Cancer: A Stepped-Wedge Cluster Randomized Clinical Trial. JAMA Oncol. 2020;6(12):e204759. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Bernacki R, Paladino J, Neville BA, et al. Effect of the Serious Illness Care Program in Outpatient Oncology: A Cluster Randomized Clinical Trial. JAMA Intern Med. 2019;179(6):751–759. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Paladino J, Koritsanszky L, Nisotel L, et al. Patient and clinician experience of a serious illness conversation guide in oncology: A descriptive analysis. Cancer Med. 2020;9(13):4550–4560. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.Walker E, McMahan R, Barnes D, Katen M, Lamas D, Sudore R. Advance Care Planning Documentation Practices and Accessibility in the Electronic Health Record: Implications for Patient Safety. J Pain Symptom Manage. 2018;55(2):256–264. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.Sudore RL, Lum HD, You JJ, et al. Defining Advance Care Planning for Adults: A Consensus Definition From a Multidisciplinary Delphi Panel. J Pain Symptom Manage. 2017;53(5):821–832 e821. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34.Sudore RL, Heyland DK, Lum HD, et al. Outcomes That Define Successful Advance Care Planning: A Delphi Panel Consensus. J Pain Symptom Manage. 2018;55(2):245–255 e248. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.Bischoff KE, Sudore R, Miao Y, Boscardin WJ, Smith AK. Advance care planning and the quality of end-of-life care in older adults. J Am Geriatr Soc. 2013;61(2):209–214. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36.Ma C, Riehm LE, Bernacki R, Paladino J, You JJ. Quality of clinicians’ conversations with patients and families before and after implementation of the Serious Illness Care Program in a hospital setting: a retrospective chart review study. CMAJ Open. 2020;8(2):E448–E454. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37.Sudore RL, Fried TR. Redefining the “planning” in advance care planning: preparing for end-of-life decision making. Ann Intern Med. 2010;153(4):256–261. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 38.Sinuff T, Dodek P, You JJ, et al. Improving End-of-Life Communication and Decision Making: The Development of a Conceptual Framework and Quality Indicators. J Pain Symptom Manage. 2015;49(6):1070–1080. [DOI] [PubMed] [Google Scholar]
- 39.Bernacki RE, Block SD, American College of Physicians High Value Care Task F. Communication about serious illness care goals: a review and synthesis of best practices. JAMA Intern Med. 2014;174(12):1994–2003. [DOI] [PubMed] [Google Scholar]
- 40.You JJ, Fowler RA, Heyland DK, Canadian Researchers at the End of Life N. Just ask: discussing goals of care with patients in hospital with serious illness. CMAJ. 2014;186(6):425–432. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 41.Cohen LL. Racial/ethnic disparities in hospice care: a systematic review. J Palliat Med. 2008;11(5):763–768. [DOI] [PubMed] [Google Scholar]
- 42.Barnato AE, Herndon MB, Anthony DL, et al. Are regional variations in end-of-life care intensity explained by patient preferences?: A Study of the US Medicare Population. Med Care. 2007;45(5):386–393. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 43.Muni S, Engelberg RA, Treece PD, Dotolo D, Curtis JR. The influence of race/ethnicity and socioeconomic status on end-of-life care in the ICU. Chest. 2011;139(5):1025–1033. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 44.Welch LC, Teno JM, Mor V. End-of-life care in black and white: race matters for medical care of dying patients and their families. J Am Geriatr Soc. 2005;53(7):1145–1153. [DOI] [PubMed] [Google Scholar]
- 45.Uyeda AM, Lee RY, Pollack LR, et al. Predictors of Documented Goals-of-Care Discussion for Hospitalized Patients With Chronic Illness. J Pain Symptom Manage. 2023;65(3):233–241. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 46.Brown CE, Curtis JR, Doll KM. A Race-Conscious Approach Toward Research on Racial Inequities in Palliative Care. J Pain Symptom Manage. 2022;63(5):e465–e471. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 47.Volandes AE, Zupanc SN, Paasche-Orlow MK, et al. Association of an Advance Care Planning Video and Communication Intervention With Documentation of Advance Care Planning Among Older Adults: A Nonrandomized Controlled Trial. JAMA Netw Open. 2022;5(2):e220354. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 48.Dziadkowiec O, Callahan T, Ozkaynak M, Reeder B, Welton J. Using a Data Quality Framework to Clean Data Extracted from the Electronic Health Record: A Case Study. EGEMS (Wash DC). 2016;4(1):1201. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 49.Wells BJ, Chagin KM, Nowacki AS, Kattan MW. Strategies for handling missing data in electronic health record derived data. EGEMS (Wash DC). 2013;1(3):1035. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 50.Uyeda AM, Curtis JR, Engelberg RA, et al. Mixed-methods evaluation of three natural language processing modeling approaches for measuring documented goals-of-care discussions in the electronic health record. J Pain Symptom Manage. 2022;63(6):e713–e723. [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Data Availability Statement
Data
Data Available: Yes
Data Types: Participants’ de-identified health record data
How to access data: Participants’ de-identified EHR data may be requested from study investigators; use of data will require completion of a Data Use Agreement.