

Abstract
Background and Purpose
Cortical dysfunction, quantifiable by cerebral perfusion techniques, is prevalent in MS patients contributing to cognitive impairment. We sought to localize perfusion distribution differences in relapsing-remitting MS patients with and without cognitive impairment, and healthy controls.
Materials and Methods
39 relapsing-remitting MS patients (20 cognitively impaired, 19 non-impaired) and 19 age and gender-matched healthy controls underwent a neurocognitive battery and MRI scanning. Voxel-based analysis compared regional deep and cortical GM perfusion and volume among the cohorts.
Results
Adjusting for localized volumetric differences in the right frontal, temporal and occipital lobes, progressive CBF and CBV deficits were present in the left middle frontal cortex for all cohorts and in the left superior frontal gyrus for cognitively impaired patients compared to unimpaired patients and controls. Compared to healthy controls, reduced CBF was present in the limbic regions of cognitively impaired patients and reduced CBV in the right middle frontal gyrus of cognitively impaired and temporal gyrus of non-impaired relapsing-remitting MS patients.
Conclusions
Consistent regional frontal cortical perfusion deficits are present in relapsing-remitting MS patients, with more widespread hypoperfusion in cognitively impaired patients, independent of structural differences indicating that cortical perfusion may be a useful biomarker of cortical dysfunction and cognitive impairment in MS.
INTRODUCTION
MS is traditionally considered a demyelinating-inflammatory WM disorder, however, GM involvement is recognized in 50–93% of patients1,2 contributing to cognitive impairment which is present in 40–68% of cases.3,4 MS patients may display deficits in several cognitive domains including working memory, learning and memory retrieval, executive function and especially information processing speed.2,5
Multiple studies have quantified the relative contributions of WM T2 hyperintense, and to a lesser extent, GM cortical lesions to cognition in MS. The relationship between WM T2 hyperintense lesion burden and cognitive impairment is modest,6 and GM and WM damage may occur interdependently1 with cortical abnormalities reported in the absence of WM disease.7 Both atrophy and cortical lesion load are important predictors of cognitive deficits in MS patients, 5 nevertheless, cortical lesion burden is increasingly reported as a stronger and an independent predictor of cognitive performance in comparison to cortical volume.8
Current clinical imaging techniques utilized for cortical lesion detection such as double inversion recovery detect few lesions (around 18%) compared to histopathological studies.9 Several studies have proposed new strategies to detect cortical abnormality including cortical lesion volume or more subtle ultrastructural (MTR,10,11 DTI12,13) or perfusion abnormality in the clinical setting. GM is inherently sensitive to perfusion changes caused by both physiological and pathologic alterations, due to its high vascularity and metabolic activity. Cortical perfusion can be evaluated with multiple imaging techniques including fMRI, arterial spin-labelling (ASL) and gadolinium-based MRI techniques, such as DSC which is the most widely performed clinical perfusion technique. By using pre- and post-gadolinium scans to calibrate DSC, the bookend technique offers accurate cerebral perfusion quantification with high PET correlation and inter-observer reliability.14,15
Previous perfusion studies show that, regardless of MS clinical subtype, cerebral hypoperfusion is an early and integral occurrence16,17 including in early relapsing-remitting MS (RRMS) where reduction may be seen in the absence of structural differences compared to healthy controls (HC).18 Studies explicitly exploring cognitive impairment in both RRMS and secondary progressive MS (SPMS) describe significant and focal frontal cortical correlations between CBV and CBF reductions and cognitive deficits.16,19–21
In the present study, we sought to localize CBF and CBV in HC and cognitively impaired and intact RRMS patients to determine whether a similar pattern of involvement is present compared to that previously reported for SPMS. We hypothesized that RRMS patients with cognitive impairment similarly exhibit localized frontal cerebral CBF and CBV reduction in functionally consistent brain regions, compared with non-impaired RRMS patients and HC. We further evaluated the consistency of the localized findings before and after accounting for any structural group differences.
METHODS
Patient cohort
Thirty-nine patients with RRMS (modified McDonald criteria 201022) were prospectively recruited over a 1 year period from 2 tertiary referral MS clinics. Initially 20 cognitively impaired patients were recruited followed by the remaining unimpaired and 19 HC (with no previous history of neurological disorders) who were selected to reflect the overall distribution of gender and age of the impaired cohort. Charts of potential patients were reviewed by a senior neurologist (20 years’ experience) prior to recruitment. Exclusion criteria included relapse or corticosteroid use within the past 3 months; history of drug/alcohol abuse; premorbid (pre-MS) psychiatric history; head injury including loss of consciousness; concurrent morbidity and MR imaging/gadolinium contraindications. All study participants were purposely recruited for this study. At the time of consent, the small potential risks associated with gadolinium injection were discussed referencing American College of Radiology and FDA communications. Consent was obtained following confirmation of MRI (and gadolinium) eligibility on the basis of a standardized MRI contraindication questionnaire and GFR (glomerular filtration rate) determination. The study was approved by the research ethic board of both Sunnybrook and St. Michael's hospitals, and informed consent was obtained from all participants.
Neurocognitive testing
All patients underwent clinical assessments within 1 week of image acquisition documenting demographic data and medical history including relapse history. Disability was assessed using the Expanded Disability Status Score.23 All participants were tested using the Minimal Assessment of Cognitive Function in Multiple Sclerosis battery covering 5 cognitive domains: working memory and processing speed (Paced Auditory Serial Addition Test; Symbol Digit Modalities Test); learning and memory (Brief Visual Memory Test-revised; California Verbal Learning Test-II); executive function (Delis-Kaplan Executive Function System); verbal fluency (Controlled Word Association Test); and visuospatial perception (Judgement of Line Orientations).24 Raw scores of each individual test were converted to Z scores using widely available normative data which corrects for age and gender. Norms for three of the key components of the neurocognitive battery (Paced Auditory Serial Addition Test; Symbol Digit Modalities Test; Controlled Word Association Test) also correct for education. Patients scoring 1.5 standard deviations below normative data on ≥2 cognitive tests were considered cognitively impaired.25 The Hospital Anxiety and Depression Scale was also administered.
MR imaging acquisition
All scans were acquired on a 3T MRI system (Achieva, Philips Healthcare, Best NL) with an 8-channel phased array head coil receiver. Conventional MRI sequences were acquired for structural and lesion characterization including: axial volumetric TSE T1 (TR/TE/flip angle= 9.5ms/2.3ms/12°; FOV= 24 cm; acquisition matrix= 256×219; slice thickness= 1.2 mm); axial proton density/T2 (TR/TE/flip angle= 2500ms/10.7ms/90°; FOV= 23 cm; acquisition matrix= 256×263; slice thickness= 3 mm); axial phase-sensitive inversion recovery (TR/TE= 3374ms/15ms; FOV= 23 cm; acquisition matrix= 400×255; slice thickness= 3 mm); axial field-echo echo-planar DSC (TR/TE/flip angle= 1633ms/30ms/60°; FOV= 22 cm; acquisition matrix= 96×93; slice thickness= 4 mm; no gap; signal bandwidth= 1260 Hz/pixel; sections= 24). A segmented inversion recovery Look-Locker EPI sequence was performed immediately pre- and post-axial DSC sequence (TR/TE/flip angle= 29ms/14ms/20°; inversion time= 15.8ms; FOV= 22 cm; acquisition matrix= 128×126; 15 lines in k-space per acquisition; slice thickness= 4 mm; 60 time points). 10cc of 1 mmol/mL concentration Gadobutrol (Gadovist; Bayer, Toronto, Canada) was administered by power injector at a rate of 5 mL/s, followed by a 25 mL bolus of saline at 5 mL/s. A total of 60 images were acquired at 1.6-second intervals with the injection occurring at the 5th volume. A 3 second delay was placed after the last imaging time point to facilitate longitudinal magnetization recovery.
Image processing
Perfusion maps
quantitative CBF (qCBF) and CBV (qCBV) maps were generated from the DSC and Look-Locker EPI images (T1-weighted pre and postgadolinium reference scans) by using the bookend technique.15 Briefly, these Look-Locker EPI scans allow for DSC calibration, independent of an arterial input function, by quantifying WM T1 signal changes relative to blood pool to calculate the steady state CBV in WM using a water-correction factor to correct for intra- to extravascular water exchange. Deconvolution of tissue concentration-time curves by the arterial input function using singular value decomposition yields the rCBF while rCBV is determined by calculating the ratio of the area under the tissue-concentration-time curve and the arterial input function. Final perfusion quantification of qCBV and qCBF is then performed as previously described.26
Lesion load
Structural T1- and proton density/T2-weighted images were co-registered using linear registration (SPM 8.0; Wellcome Department of Imaging Neuroscience, London, UK). Lesions were manually traced with Analyze 8.0 (Mayo Clinic, Rochester, Minnesota) by an experienced clinician (10 years’ experience) using phase-sensitive inversion recovery for cortical lesion tracing, and proton density/T2 and T1 scans for WM T2 hyperintense lesion and T1 black hole tracing respectively.
Voxel-based morphometry (VBM) analysis
VBM analysis was performed in SPM8 by using DARTEL and the unified segmentation model for structural and perfusion images respectively.27,28
Structural VBM
T1 structural images were segmented using both unified segmentation model and DARTEL functions in SPM8, and then checked for accuracy. A group-specific template was created using the DARTEL space segmentations. Each participant’s native space segmentations were registered to this template employing a non-linear transformation, and then affine transformed into MNI (Montreal Neurological Institute, McGill University) space, before being smoothed with an 8 mm full width half maximum isotropic Gaussian kernel. The segmentations were aligned to MNI152 space via the DARTEL template using the same transformations in a single step.
Perfusion VBM
A mean DSC series was constructed for each patient by averaging the 60 EPI DSC acquisitions and then normalizing them to MNI152 space using SPM8. A group-specific perfusion template was then created in MNI space. The DSC sequence was linearly registered to the group template using FSL-FLIRT followed by non-linear intensity modulation and multi-resolution non-linear registration with 4 subsampling levels (FSL-FNIRT).29 These sequences were smoothed at each respective resolution level during the registration using full width half maximum Gaussian kernel of 6, 4, 2, and 2 mm. This transformation matrix was then applied to the intrinsically co-registered bookend perfusion maps of qCBF and qCBV.
Statistical analysis
Clinical and demographic measures
Demographic, neurological and neuropsychological data were summarized in HC, cognitively impaired and non-impaired RRMS patients using mean and standard deviation for continuous variables, and counts for categorical variables. Statistical Analysis Software (SAS version 9.4) was used to compare each clinical, demographic and volumetric measure among the 3 groups; general linear regression or logistic regression analysis were applied for continuous or for categorical variables. Any variables demonstrating significant group differences (p<0.017, p<0.05 corrected for multiple comparisons between the 3 cohorts) were included as covariates for the respective mass univariate analysis.
VBM analysis
Perfusion maps and structural images were compared using the mass univariate technique employed by SPM. Based on previous research16,19 we hypothesized cortical perfusion changes in the frontal cortex. With this a priori hypothesis VBM analysis was restricted to GM and clusters with ≥20 contiguous voxels with voxel-wise p-value threshold of p < 0.001 were considered significant. VBM analysis was repeated for perfusion measures with structural findings as covariates. Brain regions identified by SPM as statistically significant were identified using Xjview software 8.12 (http://www.alivelearn.net/xjview).
RESULTS
Demographic, clinical and volumetric data
Demographic, clinical, and volumetric data are summarized in Table 1. Similar group characteristics were present with the exception of lower education in cognitively impaired RRMS patients compared to HC (p=0.004). Both cognitively impaired and non-impaired RRMS patients scored higher on the anxiety measure than HC (p=0.0004 and p=0.012 respectively), and cognitively impaired patients also showed higher depression scores compared to non-impaired RRMS and HC (p<0.0001, p=0.0001). Furthermore, cognitively impaired patients were more functionally disabled compared to non-impaired patients (p=0.014) as measured by the Expanded Disability Status Scale. With respect to structural/volumetric differences, cognitively impaired RRMS patients had a reduction in WM (p=0.008) and thalamic volume (p=0.014).
Table 1.
Demographic, neurological and neuropsychological data of healthy controls and RRMS patients.
| Healthy Controls n = 19 | Non-Impaired RRMS n = 19 | Cognitively Impaired RRMS n = 20 | |
|---|---|---|---|
|
Demographic and Clinical Data
| |||
| Age (yrs) | 49.0 ± 7.1 | 46.4 ± 7.2 | 48.1 ± 4.7 |
| Gender (F/M) | 14 / 5 | 15 / 4 | 12 / 8 |
| Education (yrs) | 16.9 ± 2.9╪ | 16.1 ± 1.3 | 14.6 ± 1.9╪ |
| Disease duration (yrs) | NA | 11.8 ± 5.4 | 11.6 ± 4.9 |
| EDSS | NA | 1.8 ± 0.7* | 2.6 ± 0.7* |
| HADS-A | 4.4 ± 4.3╪⋄ | 6.37 ± 3.1⋄ | 8.5 ± 3.7╪ |
| HADS-D | 2.3 ± 2.3╪ | 3.5 ± 3.2* | 7.6 ± 2.9╪* |
| Treatment | N/A | ||
| β-Interferon | 4 (21%) | 3 (15%) | |
| Other Immune Suppressors | 11 (58%) | 12 (60%) | |
| None | 4 (21%) | 5 (25%) | |
| Presence of Enhancing Lesions | N/A | 1 (5%) | 5 (25%) |
|
| |||
|
Volumetric Data (cm3)
| |||
| GM | 653.37 ± 81.51 | 618.83 ± 53.94 | 605.09 ± 60.90 |
| WM | 458.22 ± 65.02 ╪ | 421.84 ± 39.29 | 414.53 ± 71.56 ╪ |
| BG | 19.41 ± 2.75 | 18.68 ± 2.52 | 18.04 ± 2.93 |
| Th | 9.83 ± 1.92 ╪ | 9.14 ± 1.98 | 7.91 ± 1.88 ╪ |
| CL | 0.00 ± 0.00 ╪ | 0.12 ± 0.11 | 0.22 ± 0.36 ╪ |
| T2H | 0.00 ± 0.00 ╪ | 9.37 ± 10.02 | 13.47 ± 13.30 ╪ |
| T1bh | 0.00 ± 0.00 ╪ | 3.21 ± 2.98 | 5.85 ± 6.77 ╪ |
| CSF | 320.89 ± 210.43 ╪ | 353.22 ± 131.71 | 400.29 ± 173.78 ╪ |
|
| |||
|
Neurocognitive Tests (z-score)
| |||
| COWAT-FAS | −0.67 ± 0.83 | −0.26 ± 1.06* | −1.16 ± 0.89 * |
| COWAT-Animals | −0.13 ± 1.14 | 0.41 ± 0.95* | −0.59 ± 1.18* |
| BVMT-IR | 0.37 ± 1.15 ╪ | −0.07 ± 1.04* | −1.68 ± 1.34 ╪* |
| BVMT-DR | 0.40 ± 1.14 ╪ | 0.42 ± 0.77* | −1.62 ± 1.48 ╪* |
| PASAT-3 | −0.39 ± 0.94 ╪ | 0.05 ± 0.61* | −1.71 ±0.82 ╪* |
| PASAT-2 | −0.21 ± 0.89 ╪ | −0.26 ± 0.66* | −1.80 ± 0.57 ╪* |
| JLO | 0.98 ± 0.20 | 0.83 ± 0.56 | 0.40 ± 0.67 |
| SDMT | −0.14 ± 0.92 ╪ | 0.02 ± 0.75* | −1.80 ± 1.17 ╪* |
| CVLT II-IR | −0.25 ± 1.05 ╪ | −0.23 ± 1.04* | −1.94 ± 1.36 ╪* |
| CVLT II-DR | −0.11 ± 0.66 ╪ | 0.21 ± 0.92* | −2.20 ± 1.61 ╪* |
| DKEFS-ST | 0.51 ± 0.73 | 0.26 ± 0.61 | −0.20 ± 1.25 |
Note: Significance p<0.017, corrected for multiple comparisons;
Healthy Controls vs. Non-Impaired RRMS,
Healthy Controls vs. Cognitively Impaired RRMS,
Non-Impaired RRMS vs. Cognitively Impaired RRMS.
All values are mean ± SD unless specified.
EDSS, Expanded Disability Status Score; HADS, Hospital Anxiety and Depression Scale; COWAT, Controlled Oral Work Association Test; BVMT, Brief Visuospatial Test – revised; PASAT, Paced Auditory Serial Addition Test; JLO, Judgment of Line Orientation Test; SDMT, Symbol Digit Modalities Test; CVLT II, California Verbal Learning Test – II; IR, Immediate Recall; DR, Delayed Recall; DKEFS-ST, Delis-Kaplan Executive Function System Sorting Test; GM, Grey Matter; WM, White Matter; BG, Basal Ganglia; Th, Thalamus; CL, Cortical Lesions; T2H, T2 Hyperintensities; T1bh, T1 Black Holes; Cerebrospinal Fluid (CSF).
Neurocognitive performance
There was no difference in cognitive performance between HC and non-impaired RRMS. Cognitively impaired RRMS patients performed significantly worse on all cognitive tests compared to both HC and non-impaired patients (Table 1), except for the Delis-Kaplan Executive Function System and the Judgement of Line Orientations test.
VBM data (perfusion and structural)
Mass univariate SPM analysis detected significantly reduced qCBF and qCBV in the left middle frontal gyrus (encompassing Brodmann area, BA 10, 11, 46) for all group comparisons (puncorr<0.001). Cognitively impaired patients showed qCBF and qCBV reduction compared to non-impaired RRMS and HC in the bilateral superior frontal gyrus (BA 6, 8, 10), left fusiform gyrus (BA 20) and right limbic lobe including cingulate gyrus (BA 24).
Compared to unimpaired RRMS, cognitively impaired RRMS patients showed lower qCBF in the left thalamus (including the medial dorsal nuclei); and lower qCBV in the right anterior cingulate (BA 25), left posterior cingulate (BA 31), right inferior parietal lobule (BA 40), right lingual gyrus and left caudate. Furthermore, cognitively impaired RRMS showed qCBF reductions compared to HC in the right middle frontal gyrus (BA 6, 10), and qCBV deficits in the right precentral (BA 4) and right parahippocampal gyri (BA 28).
Regional volume of the right superior frontal gyrus (BA 6, 10) was decreased in cognitively impaired RRMS compared to non-impaired patients, and in non-impaired patients compared to healthy controls. Additionally, cognitively impaired RRMS showed focal atrophy in the right precentral (BA 6) and trans-temporal gyri (BA 42) compared to non-impaired RRMS, and in the right inferior occipital gyrus (BA 18) compared to HC.
VBM analysis conducted with regional volumes of focal atrophy included as covariates, found that cortical hypoperfusion (qCBF and qCBV) was maintained in the left middle frontal gyrus (BA 10, 11, 46) for all group comparisons, and in the left superior frontal gyrus (BA 6, 10) for cognitively impaired RRMS patients compared to both unimpaired patients and HC (Figure 1, Table 2). Cognitively impaired patients continued showing qCBV deficits in the right lingual gyrus (with additional qCBF reduction in left BA 18), right inferior parietal lobule (BA 40), left fusiform gyrus (BA 20), and qCBF reductions in caudate head and thalamic medial dorsal nuclei in comparison to non-impaired RRMS patients; and decreased qCBF in the right middle frontal gyrus (BA 6) and qCBV in left parahippocampal gyrus (BA 28) in comparison to HC. Reduced qCBV in cognitively impaired compared to non-impaired RRMS was present in the left inferior frontal gyrus (BA 46), and diminished qCBF in the right caudate body. Compared to HC, non-impaired patients showed reduced qCBF in the superior temporal lobe (BA 38).
Figure 1. Areas of significantly (puncorr<0.001) reduced cortical perfusion in RRMS subgroups and healthy controls, with volumes for atrophied regions added as covariates.
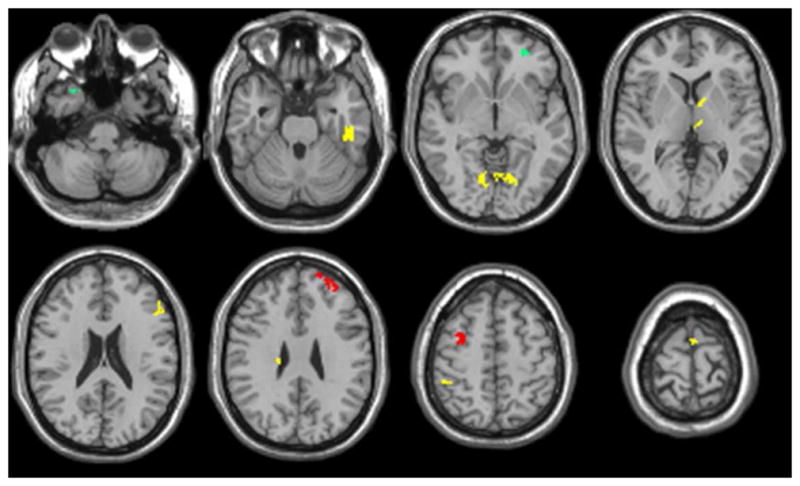
Green, healthy controls vs. non-impaired RRMS; Red, healthy controls vs. cognitively impaired RRMS; Yellow, non-impaired RRMS vs cognitively impaired RRMS.
Table 2.
Areas of significantly (puncorr<0.001) reduced cortical perfusion in RRMS subgroups and healthy controls, with volumes for atrophied regions added as covariates.
| qCBF | qCBV | Anatomical Regions | Cluster Size | MNI Coordinates | t Values | ||||
|---|---|---|---|---|---|---|---|---|---|
| x | y | z | HC vs CI | HC vs NI | NI vs CI | ||||
|
| |||||||||
| ✓ | ✓ | Left Superior Frontal Gyrus (BA6, 10)* | 78 | −32 | 50 | 28 | 3.52 | 3.62 | |
| ✓ | Right Middle Frontal Gyrus (BA 6)* | 26 | 34 | 0 | 64 | 3.31 | |||
| ✓ | ✓ | Left Middle Frontal Gyrus (BA 10, 11, 46)* | 100 | −22 | 56 | 26 | 4.79 | 4.56 | 3.21 |
| ✓ | Left Inferior Frontal Gyrus (BA 46) | 21 | −48 | 30 | 20 | 3.29 | |||
| ✓ | Right Parahippocampal Gyrus (BA 28)* | 27 | 24 | −22 | −12 | 4.15 | |||
| ✓ | ✓ | Right Lingual Gyrus* | 101 | 12 | −72 | −2 | 5.11 | ||
| ✓ | Left Lingual Gyrus (BA 18) | 72 | −6 | −68 | 2 | 3.99 | |||
| ✓ | Right Inferior Parietal Lobule (BA 40)* | 22 | 48 | −40 | 56 | 3.98 | |||
| ✓ | Right Superior Temporal Gyrus (BA 38) | 38 | 28 | 10 | −46 | 3.64 | |||
| ✓ | Left Temporal Fusiform Gyrus (BA 20)* | 134 | −44 | −22 | −30 | 3.74 | |||
| ✓ | Left Caudate Head* | 36 | −10 | 6 | 4 | 3.64 | |||
| ✓ | Right Caudate Body | 24 | 18 | −20 | 26 | 3.68 | |||
| ✓ | Left Thalamic Medial Dorsal Nuclei* | 31 | −6 | −18 | 6 | 3.63 | |||
Note: Starred anatomical regions remained significant from previous VBM analysis without atrophy areas added as covariates.
qCBF, quantitative cerebral blood flow; qCBV, quantitative cerebral blood volume; BA, Brodmann area; HC, healthy controls; CI, cognitively impaired RRMS patients; NI, non-impaired RRMS patients.
DISCUSSION
Consistent perfusion deficits in the frontal cortex are present in RRMS patients independent of global or regional atrophy. Significantly different and progressive qCBF and qCBV reduction between all groups was demonstrated in the middle frontal cortex and in the left superior frontal gyrus in impaired RRMS compared to the other two cohorts, after considering confounding variables of disability, anxiety, depression and education. RRMS patients and HC were further distinguished by qCBV reductions in right limbic and qCBF reductions in the right frontal regions (for impaired) and right temporal region (for non-impaired patients). Finally, qCBV deficits were found in cognitively impaired compared to non-impaired RRMS in the left frontal (inferior frontal gyrus), right parietal (inferior parietal lobule), left temporal (fusiform gyrus), and bilateral occipital (lingual gyrus) lobes; and qCBF deficits in deep GM structures including the bilateral caudate and the left thalamus (medial dorsal nuclei).
Distribution of qCBF and qCBV reduction in the superior frontal, middle frontal and parahippocampal gyri are similar to that reported in a recent pseudocontinous ASL study comparing HC and very early RRMS patients.18 That study also showed additional qCBF reduction in multiple other areas not demonstrated in the present study; however, the discrepancies could be explained by different MRI techniques (pseudocontinous ASL vs bookend perfusion) and patient populations. Unlike our non-impaired RRMS patients which are cognitively indistinguishable from healthy controls, Debernard et al.18 reported a borderline significant BVMT reduction and demonstrated a lower white matter volume in his early RRMS cohort suggesting a greater level of disease burden in the patient sample (supported by a higher upper EDSS range of 4.5 compared to 3.5 in our sample). In contrast to that study, we demonstrated regional cortical GM volume reduction within the right frontal, temporal and occipital lobes consistent with that observed by Riccitelli et al.30 Reduced superior frontal gyrus, thalamic and caudate nuclei perfusion was similarly reported in a SPMS patient cohort with cognitive impairment, suggesting that the frontal reduction may be a marker of impairment in both RRMS and SPMS patients even after controlling for structural differences.19
The frontal areas, BA6, 10 and 46 affected in our RRMS patients are responsible for memory processing, particularly working memory, memory encoding and retrieval.31,32 Several studies relate BA 10 with prospective memory and “intentional forgetting,” suggesting involvement of BA 10 in controlling and manipulating memory.32,33 BA 46 activation is associated with working memory processes, as well as memory manipulation.31,33 It has been assumed that working memory is involved in a diversity of cognitive processes, including planning,34 reasoning,35 and problem solving.36 On the other hand, involvement of BA 6 in memory and attention may be due to the activation of an extended brain network where the middle frontal gyrus has a fundamental task in memory strategy organization and memory control.37 Hypoperfusion (qCBF and qCBV) in the left middle frontal and right superior temporal gyri with preservation of perfusion within the remaining medial prefrontal cortex in non-impaired compared to cognitively impaired RRMS patients likely reflects increased cortical plasticity as the medial prefrontal cortex is previously shown to adaptively compensate for functional impairment in MS patients.38 RRMS and SPMS performing a processing speed and attention task (counting Stroop task) were found to have activation predominantly in the left medial frontal region (left middle frontal gyrus/superior frontal sulcus and bilateral superior frontal gyri corresponding to BA 8, 9, 10) while HC had greater right frontal activation (inferior frontal gyrus, BA 45; and right basal ganglia).38 Lastly, BA 28 and 38 are also implicated in memory, particularly non-verbal memory (right parahippocampal gyrus)39 and multimodal memory retrieval (superior temporal gyrus).40
Supporting the validity of the structural and progressive perfusion differences in cognitively impaired RRMS patients described above, significant impairment in working memory (Paced Auditory Serial Addition Test and Symbol Digit Modalities Test), visual and verbal learning and memory retrieval ((Brief Visual Memory Test-revised and California Verbal Learning Test-II) were present compared to non-impaired patients and HC.
Our VBM analysis by necessity controlled for a number of important potential confounding covariates for example, the effect of depression was accounted for by the inclusion of Hamilton Anxiety and Depression scores. Differing educational level between cohorts was accounted for by the “normalization” of raw neurocognitive battery scores against representative population datasets. Cortical lesions and, to a lesser extent, T2 hyperintense lesion burden are also both implicated in cognitive impairment of MS patients. Comparisons between patient groups and HC included lesion volumes as covariates in our VBM analysis. However, no significant difference in lesion burden was present between MS groups precluding this for that comparison.
Cerebral blood volume (amount of blood in 100 grams of brain tissue) and blood flow (amount of blood flowing through 100 grams of brain tissue per minute) abnormalities are found in a number of neurological conditions such as stroke, characterized by ischemia. The physiopathology leading to cerebral hypoperfusion is unknown and may be multi-factorial. While evidence does not support a primary neuronal loss mechanism given multiple findings of reduced cortical perfusion in the absence of GM volume loss,16,18,19 mitochondrial disturbances and vascular abnormalities have been implicated in cerebral hypoperfusion in MS. Mitochondrial dysfunction can contribute to cerebral hypoperfusion in the form of diminished mitochondrial capacity resulting from reductions in gene products specific for the mitochondrial electron transport chain41 or due to intra-axonal mitochondrial pathology triggered by macrophage-derived reactive oxygen and nitrogen species which may precede axonal damage.42 Cerebral hypoperfusion can also be secondary to vascular abnormalities. Increased levels of endothelin-1, a potent vasoconstrictive peptide, are found in MS patients suggesting that cerebral blood flow reductions are mediated by elevated levels of this peptide.43 Astrocytes of MS patients are deficient in the β2-adrenergic receptor resulting in cellular metabolic dysfunction affecting potassium uptake after synaptic activity, and its subsequent release to the perivascular space thus reducing arteriolar vasodilation.44
Venous changes are also well described in MS and given that venous capacitance accounts for approximately 70% of CBV, pathologies that decrease venous capacitance should greatly impact qCBV. For example, Ge et al.45 demonstrated reduced visibility of periventricular venous vasculature in MS patients using susceptibility-weighted imaging. The authors suggested this reduction could be attributable to decreased vein number or size secondary to venous occlusion and perivenular inflammation. Such pathology could also be driven by obliterative vasculitis that preferentially disrupts venous changes.46,47 Additionally, intrastriatal injections of proinflammatory cytokine tumour necrosis factor alpha (TNF-α) – found elevated in MS brains48 – in rat models resulted in significant reductions of cerebral blood flow.49 Cerebral hypoperfusion is characterized by both blood flow and volume changes and may be that these perfusion metrics are differentially affected by the physiopathological methods proposed. Additional studies should be conducted to explore the differences in cerebral blood flow and volume and its relation to physiopathology.
Limitations include the need for contrast agent injection required for DSC perfusion precluding its use in patients with contra-indications such as renal impairment. DSC is a relatively low resolution technique in comparison to structural imaging but comparable to other functional techniques such as diffusion tensor and ASL techniques which were previously applied to MS. DSC enables whole brain scanning in approximately 2 minutes, therefore, minimally prolonging scan time with higher signal to noise than ASL. Since the classes of disease modifying drugs were evenly represented in both cognitively impaired and non-impaired groups, we did not adjust for this factor. However, given that the effects of such treatments on cortical perfusion abnormalities are unclear, it would be prudent to adjust for disease modifying drugs in future studies if difference occurs. Similarly, fatigue, experienced by 78–90% of MS patients,50 may be associated with impaired cognitive function and should be accounted for in future studies.51 Despite the relatively small sample size, consistent frontal perfusion deficits were demonstrated in our RRMS sample. According to our a priori hypothesis this comparison was uncorrected but included several confounders. These results should be validated in a larger patient cohort. Longitudinal studies would also be helpful in determining whether perfusion measurements are sensitive to disease progression.
In conclusion, consistent regional frontal cortical perfusion deficits are found in RRMS patients, with more widespread hypoperfusion in cognitively impaired RRMS, independent of structural differences. Our findings suggest a potential role for cortical perfusion as a useful biomarker of cortical dysfunction and cognitive impairment in MS.
Acknowledgments
Grant Funding:
Dr Aviv was supported by Canadian Institutes of Health Research (CIHR) operating grant (130366). Dr. Aviv and Dr. Hojjat are supported by a Biogen fellowship funding award. Charles Cantrell is supported by the American Heart Association (14PRE20380310). Dr. Carroll is supported by the US NIH (1R21EB017928-01A1).
Abbreviations
- ASL
arterial spin labelling
- BA
Brodmann area
- HC
healthy control
- MNI
Montreal Neurological Institute
- qCBF
quantitative cerebral blood flow
- qCBF
quantitative cerebral blood volume
- RRMS
relapsing-remitting multiple sclerosis
- SPMS
secondary-progressive multiple sclerosis
- VBM
voxel-based morphometry
Footnotes
money paid to institution
DISCLOSURES: Charles Cantrell—RELATED: Grant: American Heart Association (14PRE20380810).* Liesly Lee—UNRELATED: Consultancy: Biogen Canada, Novartis Canada, Genyzme Canada, Teva Neurosciences, Serono Canada, Comments: Advisory board member; Payment for Manuscript Preparation: Biogen Canada, Comments: Publication of review article; Travel/Accommodations/Meeting Expenses Unrelated to Activities Listed: Biogen Canada, Novartis Canada, Comments: Travel to Conferences and Advisory Boards; OTHER: Biogen Canada,* Novartis Canada,* Teva Neurosciences,* Comments: Clinical trial funding. Timothy Carroll—RELATED: Grant: NIH,* Comments: I hold an NIH research grant related to cerebral perfusion; UNRELATED: Grants/Grants Pending: NIH,* AHA,* Comments: In addition to the NIH and AHA grants that support this work, I have research grants that are independent to the work presented in this paper. Richard Aviv—RELATED: Grant: CIHR,* Biogen.*
References
- 1.Calabrese M, De Stefano N, Atzori M, et al. Detection of cortical inflammatory lesions by double inversion recovery magnetic resonance imaging in patients with multiple sclerosis. Arch Neurol. 2007;64(10):1416–1422. doi: 10.1001/archneur.64.10.1416. [DOI] [PubMed] [Google Scholar]
- 2.Calabrese M, Rocca MA, Atzori M, et al. A 3-year magnetic resonance imaging study of cortical lesions in relapse-onset multiple sclerosis. Ann Neurol. 2010;67(3):376–383. doi: 10.1002/ana.21906. [DOI] [PubMed] [Google Scholar]
- 3.Deloire MS, Salort E, Bonnet M, et al. Cognitive impairment as marker of diffuse brain abnormalities in early relapsing remitting multiple sclerosis. J Neurol Neurosurg Psychiatry. 2005;76(4):519–526. doi: 10.1136/jnnp.2004.045872. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Heaton RK, Nelson LM, Thompson DS, Burks JS, Franklin GM. Neuropsychological findings in relapsing-remitting and chronic-progressive multiple sclerosis. J Consult Clin Psychol. 1985;53(1):103–110. doi: 10.1037//0022-006x.53.1.103. [DOI] [PubMed] [Google Scholar]
- 5.Calabrese M, Agosta F, Rinaldi F, et al. Cortical lesions and atrophy associated with cognitive impairment in relapsing-remitting multiple sclerosis. Arch Neurol. 2009;66(9):1144–1150. doi: 10.1001/archneurol.2009.174. [DOI] [PubMed] [Google Scholar]
- 6.Rao SM, Leo GJ, Bernardin L, Unverzagt F. Cognitive dysfunction in multiple sclerosis. I. Frequency, patterns, and prediction. Neurology. 1991;41(5):685–691. doi: 10.1212/wnl.41.5.685. [DOI] [PubMed] [Google Scholar]
- 7.Calabrese M, Gallo P. Magnetic resonance evidence of cortical onset of multiple sclerosis. Mult Scler. 2009;15(8):933–941. doi: 10.1177/1352458509106510. [DOI] [PubMed] [Google Scholar]
- 8.Calabrese M, Poretto V, Favaretto A, et al. Cortical lesion load associates with progression of disability in multiple sclerosis. Brain. 2012;135(Pt 10):2952–2961. doi: 10.1093/brain/aws246. [DOI] [PubMed] [Google Scholar]
- 9.Seewann A, Enzinger C, Filippi M, et al. MRI characteristics of atypical idiopathic inflammatory demyelinating lesions of the brain : A review of reported findings. J Neurol. 2008;255(1):1–10. doi: 10.1007/s00415-007-0754-x. [DOI] [PubMed] [Google Scholar]
- 10.Tardif CL, Bedell BJ, Eskildsen SF, Collins DL, Pike GB. Quantitative magnetic resonance imaging of cortical multiple sclerosis pathology. Mult Scler Int. 2012;2012:742018. doi: 10.1155/2012/742018. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Chen JT, Easley K, Schneider C, et al. Clinically feasible MTR is sensitive to cortical demyelination in MS. Neurology. 2013;80(3):246–252. doi: 10.1212/WNL.0b013e31827deb99. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Poonawalla AH, Hasan KM, Gupta RK, et al. Diffusion-tensor MR imaging of cortical lesions in multiple sclerosis: initial findings. Radiology. 2008;246(3):880–886. doi: 10.1148/radiol.2463070486. [DOI] [PubMed] [Google Scholar]
- 13.Calabrese M, Rinaldi F, Seppi D, et al. Cortical diffusion-tensor imaging abnormalities in multiple sclerosis: a 3-year longitudinal study. Radiology. 2011;261(3):891–898. doi: 10.1148/radiol.11110195. [DOI] [PubMed] [Google Scholar]
- 14.Shin W, Horowitz S, Ragin A, Chen Y, Walker M, Carroll TJ. Quantitative cerebral perfusion using dynamic susceptibility contrast MRI: evaluation of reproducibility and age- and gender-dependence with fully automatic image postprocessing algorithm. Magn Reson Med. 2007;58(6):1232–1241. doi: 10.1002/mrm.21420. [DOI] [PubMed] [Google Scholar]
- 15.Vakil P, Lee JJ, Mouannes-Srour JJ, Derdeyn CP, Carroll TJ. Cerebrovascular occlusive disease: quantitative cerebral blood flow using dynamic susceptibility contrast mr imaging correlates with quantitative H2[15O] PET. Radiology. 2013;266(3):879–886. doi: 10.1148/radiol.12120756. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Aviv RI, Francis PL, Tenenbein R, et al. Decreased frontal lobe gray matter perfusion in cognitively impaired patients with secondary-progressive multiple sclerosis detected by the bookend technique. AJNR Am J Neuroradiol. 2012;33(9):1779–1785. doi: 10.3174/ajnr.A3060. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Rashid W, Parkes LM, Ingle GT, et al. Abnormalities of cerebral perfusion in multiple sclerosis. J Neurol Neurosurg Psychiatry. 2004;75(9):1288–1293. doi: 10.1136/jnnp.2003.026021. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Debernard L, Melzer TR, Van Stockum S, et al. Reduced grey matter perfusion without volume loss in early relapsing-remitting multiple sclerosis. J Neurol Neurosurg Psychiatry. 2014;85(5):544–551. doi: 10.1136/jnnp-2013-305612. [DOI] [PubMed] [Google Scholar]
- 19.Francis PL, Jakubovic R, O’Connor P, et al. Robust perfusion deficits in cognitively impaired patients with secondary-progressive multiple sclerosis. AJNR Am J Neuroradiol. 2013;34(1):62–67. doi: 10.3174/ajnr.A3148. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Hojjat SPCC, Vitorino R, Feinstein A, Shirzadi Z, MacIntosh BJ, Crane DE, Zhang L, Morrow SA, Lee L, O’Connor P, Carroll TJ, Aviv RI. Regional reduction in cortical blood flow among cognitively impaired adults with relapsing-remitting multiple sclerosis patients. Multiple Sclerosis. doi: 10.1177/1352458515622696. In Press. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Hojjat SPCC, Carroll TJ, Vitorino R, Feinstein A, Zhang L, Symons SP, Morrow SA, Lee L, O’Connor P, Aviv RI. Perfusion reduction in the absence of structural differences in cognitively impaired versus unimpaired RRMS patients. Multiple Sclerosis. doi: 10.1177/1352458516628656. Submitted. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Polman CH, Reingold SC, Banwell B, et al. Diagnostic criteria for multiple sclerosis: 2010 revisions to the McDonald criteria. Annals of neurology. 2011;69(2):292–302. doi: 10.1002/ana.22366. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Kurtzke JF. Rating neurologic impairment in multiple sclerosis: an expanded disability status scale (EDSS) Neurology. 1983;33(11):1444–1452. doi: 10.1212/wnl.33.11.1444. [DOI] [PubMed] [Google Scholar]
- 24.Benedict RH, Fischer JS, Archibald CJ, et al. Minimal neuropsychological assessment of MS patients: a consensus approach. Clin Neuropsychol. 2002;16(3):381–397. doi: 10.1076/clin.16.3.381.13859. [DOI] [PubMed] [Google Scholar]
- 25.Benedict RH, Bruce JM, Dwyer MG, et al. Neocortical atrophy, third ventricular width, and cognitive dysfunction in multiple sclerosis. Arch Neurol. 2006;63(9):1301–1306. doi: 10.1001/archneur.63.9.1301. [DOI] [PubMed] [Google Scholar]
- 26.Shah MK, Shin W, Parikh VS, et al. Quantitative cerebral MR perfusion imaging: preliminary results in stroke. J Magn Reson Imaging. 2010;32(4):796–802. doi: 10.1002/jmri.22302. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Ashburner J, Friston KJ. Unified segmentation. Neuroimage. 2005;26(3):839–851. doi: 10.1016/j.neuroimage.2005.02.018. [DOI] [PubMed] [Google Scholar]
- 28.Ashburner J. A fast diffeomorphic image registration algorithm. Neuroimage. 2007;38(1):95–113. doi: 10.1016/j.neuroimage.2007.07.007. [DOI] [PubMed] [Google Scholar]
- 29.Jenkinson M, Beckmann CF, Behrens TE, Woolrich MW, Smith SM. Fsl. Neuroimage. 2012;62(2):782–790. doi: 10.1016/j.neuroimage.2011.09.015. [DOI] [PubMed] [Google Scholar]
- 30.Riccitelli G, Rocca MA, Pagani E, et al. Mapping regional grey and white matter atrophy in relapsing-remitting multiple sclerosis. Mult Scler. 2012;18(7):1027–1037. doi: 10.1177/1352458512439239. [DOI] [PubMed] [Google Scholar]
- 31.Ranganath C, Johnson MK, D’Esposito M. Prefrontal activity associated with working memory and episodic long-term memory. Neuropsychologia. 2003;41(3):378–389. doi: 10.1016/s0028-3932(02)00169-0. [DOI] [PubMed] [Google Scholar]
- 32.Leung HC, Gore JC, Goldman-Rakic PS. Sustained mnemonic response in the human middle frontal gyrus during on-line storage of spatial memoranda. J Cogn Neurosci. 2002;14(4):659–671. doi: 10.1162/08989290260045882. [DOI] [PubMed] [Google Scholar]
- 33.Zhang JX, Leung HC, Johnson MK. Frontal activations associated with accessing and evaluating information in working memory: an fMRI study. Neuroimage. 2003;20(3):1531–1539. doi: 10.1016/j.neuroimage.2003.07.016. [DOI] [PubMed] [Google Scholar]
- 34.Law AS, Trawley SL, Brown LA, Stephens AN, Logie RH. The impact of working memory load on task execution and online plan adjustment during multitasking in a virtual environment. Q J Exp Psychol (Hove) 2013;66(6):1241–1258. doi: 10.1080/17470218.2012.748813. [DOI] [PubMed] [Google Scholar]
- 35.Suss HM, Oberauer K, Wittmann WW, Wilhelm O, Schulze R. Working-memory capacity explains reasoning ability - and a little bit more. Intelligence. 2002;30(3):161–288. [Google Scholar]
- 36.Wiley J, Jarosz AF. Working Memory Capacity, Attentional Focus, and Problem Solving. Current Directions in Psychological Science. 2012;21(4):258–262. [Google Scholar]
- 37.Haxby JV, Petit L, Ungerleider LG, Courtney SM. Distinguishing the functional roles of multiple regions in distributed neural systems for visual working memory. Neuroimage. 2000;11(5 Pt 1):380–391. doi: 10.1006/nimg.2000.0592. [DOI] [PubMed] [Google Scholar]
- 38.Parry AM, Scott RB, Palace J, Smith S, Matthews PM. Potentially adaptive functional changes in cognitive processing for patients with multiple sclerosis and their acute modulation by rivastigmine. Brain. 2003;126(Pt 12):2750–2760. doi: 10.1093/brain/awg284. [DOI] [PubMed] [Google Scholar]
- 39.Kohler S, Black SE, Sinden M, et al. Memory impairments associated with hippocampal versus parahippocampal-gyrus atrophy: an MR volumetry study in Alzheimer’s disease. Neuropsychologia. 1998;36(9):901–914. doi: 10.1016/s0028-3932(98)00017-7. [DOI] [PubMed] [Google Scholar]
- 40.Takashima A, Nieuwenhuis IL, Rijpkema M, Petersson KM, Jensen O, Fernandez G. Memory trace stabilization leads to large-scale changes in the retrieval network: a functional MRI study on associative memory. Learn Mem. 2007;14(7):472–479. doi: 10.1101/lm.605607. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 41.Dutta R, McDonough J, Yin X, et al. Mitochondrial dysfunction as a cause of axonal degeneration in multiple sclerosis patients. Ann Neurol. 2006;59(3):478–489. doi: 10.1002/ana.20736. [DOI] [PubMed] [Google Scholar]
- 42.Nikic I, Merkler D, Sorbara C, et al. A reversible form of axon damage in experimental autoimmune encephalomyelitis and multiple sclerosis. Nat Med. 2011;17(4):495–499. doi: 10.1038/nm.2324. [DOI] [PubMed] [Google Scholar]
- 43.D’Haeseleer M, Hostenbach S, Peeters I, et al. Cerebral hypoperfusion: a new pathophysiologic concept in multiple sclerosis? J Cereb Blood Flow Metab. 2015;35(9):1406–1410. doi: 10.1038/jcbfm.2015.131. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 44.De Keyser J, Steen C, Mostert JP, Koch MW. Hypoperfusion of the cerebral white matter in multiple sclerosis: possible mechanisms and pathophysiological significance. J Cereb Blood Flow Metab. 2008;28(10):1645–1651. doi: 10.1038/jcbfm.2008.72. [DOI] [PubMed] [Google Scholar]
- 45.Ge Y, Zohrabian VM, Osa EO, et al. Diminished visibility of cerebral venous vasculature in multiple sclerosis by susceptibility-weighted imaging at 3.0 Tesla. J Magn Reson Imaging. 2009;29(5):1190–1194. doi: 10.1002/jmri.21758. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 46.Tanaka R, Iwasaki Y, Koprowski H. Ultrastructural studies of perivascular cuffing cells in multiple sclerosis brain. Am J Pathol. 1975;81(3):467–478. [PMC free article] [PubMed] [Google Scholar]
- 47.Adams CW, Poston RN, Buk SJ, Sidhu YS, Vipond H. Inflammatory vasculitis in multiple sclerosis. J Neurol Sci. 1985;69(3):269–283. doi: 10.1016/0022-510x(85)90139-x. [DOI] [PubMed] [Google Scholar]
- 48.Woodroofe MN, Cuzner ML. Cytokine mRNA expression in inflammatory multiple sclerosis lesions: detection by non–radioactive in situ hybridization. Cytokine. 1993;5(6):583–588. doi: 10.1016/s1043-4666(05)80008-0. [DOI] [PubMed] [Google Scholar]
- 49.Sibson NR, Blamire AM, Perry VH, Gauldie J, Styles P, Anthony DC. TNF-alpha reduces cerebral blood volume and disrupts tissue homeostasis via an endothelin- and TNFR2-dependent pathway. Brain. 2002;125(Pt 11):2446–2459. doi: 10.1093/brain/awf256. [DOI] [PubMed] [Google Scholar]
- 50.Fisk JD, Pontefract A, Ritvo PG, Archibald CJ, Murray TJ. The impact of fatigue on patients with multiple sclerosis. Can J Neurol Sci. 1994;21(1):9–14. [PubMed] [Google Scholar]
- 51.Krupp LB, Elkins LE. Fatigue and declines in cognitive functioning in multiple sclerosis. Neurology. 2000;55(7):934–939. doi: 10.1212/wnl.55.7.934. [DOI] [PubMed] [Google Scholar]