
Figure 13.
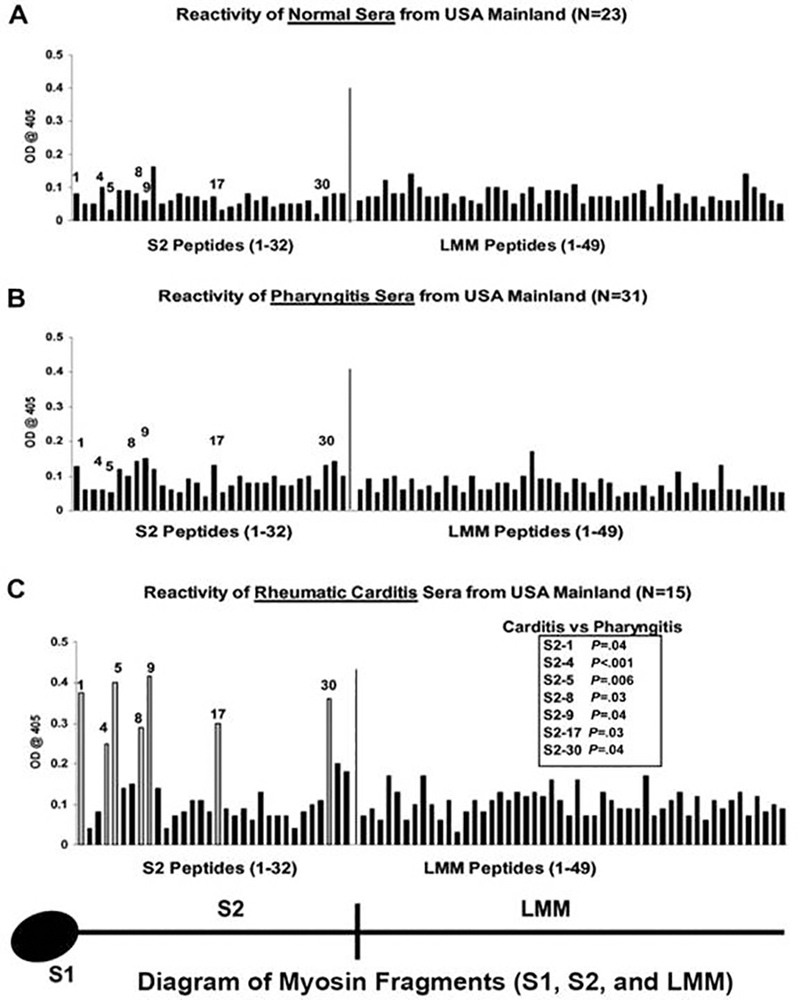
Reactivity of serum samples originating from the USA with human cardiac myosin peptides from the S2 and LMM regions in the enzyme-linked immunosorbent assay (1:100 serum dilution). A, Mean reactivity of normal serum samples from control donors with no evidence of streptococcal infection or heart disease on the US mainland against S2 and LMM peptides. These samples rarely reacted with any S2 or LMM peptide at an optical density (OD) of 0.2. B, Mean reactivity of serum samples from patients with streptococcal pharyngitis in the USA against S2 and LMM peptides. These samples rarely reacted with any S2 or LMM peptide at an OD of 0.2. C, Serum immunoglobulin G from patients with rheumatic carditis on the USA. Serum samples from patients with rheumatic carditis from the USA reacted predominantly with peptides S2–1, S2–4, S2–5, S2–8, S2–9, S2–17, and S2–30, compared with the reactivity of serum samples from patients with pharyngitis on the USA against those same peptides (B). Unadjusted Mann-Whitney P values for the comparison between carditis and pharyngitis on the US mainland are shown in panel C. The comparison for S2–4 is statistically significant on the basis of a 2-sided alpha level adjusted to preserve the false-discovery rate at 5%. Taken from Ellis et al in the Journal of Infectious Diseases with permission(24).