

An asymptomatic well-circumscribed tumor approximately 10 cm in diameter was excised from the back of a 31-year-old male patient [Figure 1]. Physical examination and laboratory investigations were otherwise unremarkable. Histopathological examination of the lesion showed a neoplasm composed of well-differentiated fat divided by collagenous septae [Figure 2]. There was some variation in the size of adipocytes and focal nuclear atypia was noted in areas adjacent to the septae [Figure 3]. The septae themselves contained numerous atypical hyperchromatic cells, some of which were multinucleated. No hypercellular areas or mitotic figures were noted [Figure 4].
Figure 1.

Well-circumscribed yellowish tumor approximately 10 cm in diameter
Figure 2.

Neoplasm composed of adipose tissue divided by collagenous septae (H and E, ×40)
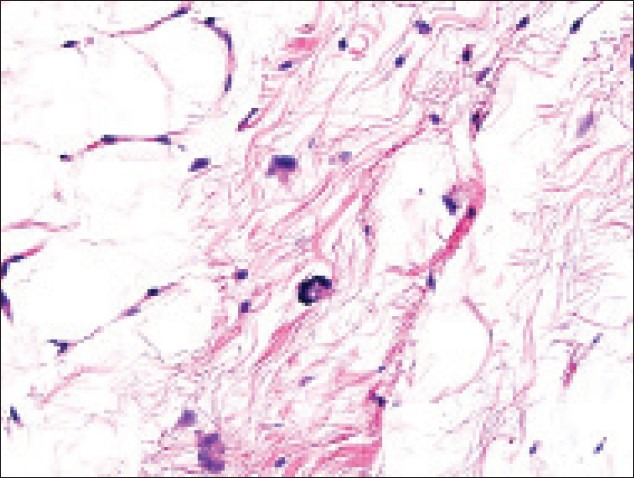
Figure 3.

Moderate atypia of nuclei of adipocytes (H and E, ×400)
Figure 4.
The septae themselves contained numerous atypical hyperchromatic cells, some of which were multinucleated. No hypercellular areas or mitotic figures were noted
The lesion most likely represents?
-
A)
Dedifferentiated liposarcoma
-
B)
Hibernoma
-
C)
Atypical lipomatous tumor (well-differentiated sarcoma)
-
D)
Spindle cell lipoma
-
E)
Pleomorphic lipoma
ANSWER: C. Atypical lipomatous tumor (well-differentiated sarcoma)
DISCUSSION
Atypical lipomatous tumor (ALT) or well-differentiated liposarcoma is the most common type of liposarcoma encountered in skin. It usually affects elderly patients and tends to localize to the retroperitomeum, subcutaneous tissue, or within muscle. It may also affect oral cavity, esophagus, orbit, stomach, and parotid gland. The neoplasm is usually asymptomatic.
On gross examination, the tumor is usually misdiagnosed as a lipoma, although it tends to be larger, characterized by presence of more fibrous septae, superficial hemorrhages, and myxoid zones. Symptoms of internal organs and tissue compression may be seen in large retroperitoneal tumors.
Histopathological examination usually reveals mature adipocytes alternating with sclerotic or myxoid zones which may be scant or predominant. Atypical cells are seen in the septae. Lipoblasts may be scattered randomly in the adipose tissue, but their absence is not necessary for definitive diagnosis. Four types of atypical lipomatous tumor are described: Lipoma-like, sclerosing, inflammatory, and spindle-cell; but precise distinction between them is not always possible.[1] Mitotic rate in ALT is low. Hypercellular areas are rare and, if present, are not mitotically active. Cases of coexistence of ALT with ordinary lipoma have been reported and suggest that fat tissue neoplasms may actually represent a continuum of histopathological changes.[2]
The differential diagnosis includes a variety of adipose tissue neoplasms. Hibernoma is a neoplasm differentiating towards brown fat, composed of monomorphic vacuolated adipocytes with round nuclei. It usually occurs in young adults. Pleomorphic and spindle cell lipomas may be more difficult to differentiate from ALT, both present as well-circumscribed lesions of upper back of older patients. Spindle cell lipoma demonstrates an admixture of spindle cells, ropey collagen, and adipocytes. Mucin and mast cells are common, but the mitotic rate in spindle cell lipoma is low. Floret-type multinucleated cells with myxoid septae are characteristic of pleomorphic lipoma.
Foci of dedifferentiation may occur in ALT, and are characterized by highly atypical hypercellular areas with a high mitotic rate (at least five mitotic figures per ten high power fields).[1] Ki67 staining has shown some benefit in aiding to access the proliferation rate in dedifferentiating foci.
Although histopathology is still the main diagnostic modality for atypical ALT, the distinction between atypical lipomatous tumor and unusual variants of benign lipomas is sometimes challenging. Modern cytogenetic methods may be of great help. Cytogenetically, atypical lipomatous tumor is characterized by the presence of supernumerary ring and/or giant marker chromosomes mainly of sequences from 12q13-15 region (MDM2, CDK4, HMGA2, and SAS genes). Fluorescence in situ hybridization (FISH) and comparative genomic hybridization (CGH) of MDM2 (murine double minute 2) gene are used to diagnose challenging cases. It was shown to correlate with p53 expression. Commercially available MDM2 FISH kit is 95% sensitive.[3]
Immunohistochemistry based on the genetic background is now more widely used. MDM2, CDK4, and p16 immunohistochemistry can be helpful to differentiate ALT and dedifferentiated liposarcoma from benign adipose tissue tumors. Three markers were shown to be expressed in about 70% of ALT and DDL.[4]
Complete excision with wide margins is usually curative for ALT, but recurrences may occur.[1,2,3,4,5] They are more frequent if the tumor is located retroperitoneally. Metastases develop only if dedifferentiation occurs.
Footnotes
Source of Support: Nil
Conflict of Interest: Nil.
REFERENCES
- 1.Evans HL. Atypical lipomatous tumor, its variants, and its combined forms: A study of 61 cases, with a minimum follow-up of 10 years. Am J Surg Pathol. 2007;31:1–14. doi: 10.1097/01.pas.0000213406.95440.7a. [DOI] [PubMed] [Google Scholar]
- 2.Kuhnen C, Mentzel T, Lehnhardt M, Homann HH, Sciot R, Debiec-Rychter M. Lipoma and atypical lipomatous tumor within the same neoplasia: Evidence for a continuous transition. Pathologe. 2010;31:129–34. doi: 10.1007/s00292-009-1257-6. [DOI] [PubMed] [Google Scholar]
- 3.Kashima T, Halai D, Ye H, Hing SN, Delaney D, Pollock R, et al. Sensitivity of MDM2 amplification and unexpected multiple faint alphoid 12 (alpha 12 satellite sequences) signals in atypical lipomatous tumor. Mod Pathol. 2012;25:1384–96. doi: 10.1038/modpathol.2012.90. [DOI] [PubMed] [Google Scholar]
- 4.Thway K, Flora R, Shah C, Olmos D, Fisher C. Diagnostic utility of p16, CDK4, and MDM2 as an immunohistochemical panel in distinguishing well-differentiated and dedifferentiated liposarcomas from other adipocytic tumors. Am J Surg Pathol. 2012;36:462–9. doi: 10.1097/PAS.0b013e3182417330. [DOI] [PubMed] [Google Scholar]
- 5.Mavrogenis AF, Lesensky J, Romagnoli C, Alberghini M, Letson GD, Ruggieri P. Atypical lipomatous tumors/well-differentiated liposarcomas: Clinical outcome of 67 patients. Orthopedics. 2011;34:e893–8. doi: 10.3928/01477447-20111021-11. [DOI] [PubMed] [Google Scholar]