

Abstract
Lingual thyroid is a rare clinical entity due to failure of the embryonic gland to descend to its normal pretracheal location. We report a case of 29 years old male patient who presented with the complaints of difficulty in swallowing and phonation. The clinical and radiology features were diagnostic of ectopic lingual thyroid. Our case report focuses on an unusual presentation of huge ectopic lingual thyroid in a male with disproportionate pressure symptoms, successfully managed surgically via suprahyoid approach.
Keywords: Ectopic Lingual Thyroid, Supra Hyoid Approach, Surgical Excision
Introduction
Lingual thyroid is rare developmental anomaly where the ectopic thyroid tissue is located at the base of the tongue in the midline. Lingual thyroid occurs as a result of failure of the embryonic gland to descend from its position posterior to the tuberculum impar to its normal pretracheal location between weeks 3 and 7 of embryologic development. Most of the ectopic thyroid are hypofunctioning, hence individuals remain in a state of hypothyroidism. An ectopic thyroid can be present over various sites such as lingual, thyroglossal, laryngotracheal and rarely at sub-mandibular, retroperitoneal and very rarely at oesophagus and mediastinum. Predominant in females. Lingual thyroid may manifest with obstructive symptoms such as dysphagia, dysphonia or upper respiratory tract obstruction. Investigations such as USG neck and CT neck can be done to diagnose lingual thyroid though the Technetium (Tc-99) scintigraphy is most important diagnostic tool used in the identification of ectopic thyroid and its functionality.
Case Report
A 29 years old male patient presented to our ENT department with chief complaints of difficulty in swallowing and a growth in the posterior aspect of the tongue, which was gradual in onset, progressive in nature since 1 year. He also complained of voice change since 6 months. Patient was known case of hypothyroidism since childhood, for which he was under irregular medication Tab thyroxine.
On examination (Fig. 1), a well-defined huge globular mass measuring 6 × 6 cm at base of tongue posterior to circumvallate papillae seen. Posterior extent of the swelling not visualised, no visible pulsation and firm in consistency. Tongue movements normal.
Fig. 1.

Picture showing Lingual Thyroid
On video-laryngoscopy (Fig. 2) a globular mass with dilated blood vessels over the surface seen arising from the base of tongue posterior to circumvallate papillae occupying the oropharynx, vallecula and laryngeal inlet could not be visualised. USG neck revealed absence of thyroid gland in its normal anatomical location and confirmed by CT Neck.
Fig. 2.
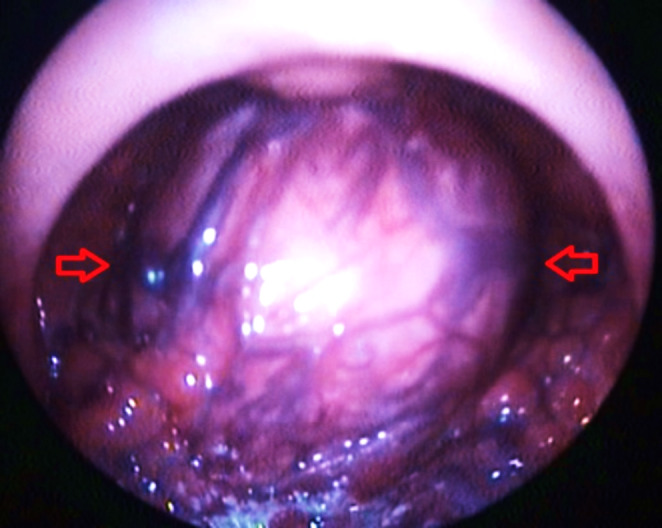
Videolaryngoscopic picture describing Lingual Thyroid
On CT Neck (Fig. 3) Correlation – No evidence of calcification in the oropharyngeal lesion predominantly hypodense.
Fig. 3.

CT Neck demonstrating Lingual thyroid A.Axial B.Coronal C.Sagittal
On MRI Neck (Fig. 4) revealed a well circumscribed lesion 5 × 5 × 4.5 cm at base of tongue, narrowing the oropharyngeal lumen to 4 mm in dimension. The lesion was indenting the base of the tongue splaying the genioglossus muscle. Inferiorly displacing the epiglottis more posteriorly, on the right side. Feature suggested ectopic lingual thyroid with cystic changes.
Fig. 4.

MRI Neck showing the extent of the lingual thyroid
Tc99 uptake scan (Fig. 5) revealed possibility of Ectopic lingual thyroid with very poor trapping function corresponding to the clinical swelling in the anatomical location. Thyroid function tests showed increased thyroid-stimulating hormone(TSH) with decreased T3 and T4 level. With the provisional diagnosis of lingual thyroid the patient was planned for excision under general anaesthesia via supra hyoid approach.
Fig. 5.

Tc99 uptake scan revealed possibility of Ectopic lingual thyroid
Under general anaesthesia preliminary Tracheostomy was done anticipating difficult intubation considering the size of the mass. Transverse skin crease incision was made at the level of hyoid bone for the suprahyoid approach. Skin, subcutaneous tissue and cervical fascia were elevated in the subplatysmal plane.
The flap was raised above the level of hyoid bone (Fig. 6) and dissection continued medial to greater horn of hyoid in layers.
Fig. 6.

Supra hyoid flap elevation
The supra hyoid muscles were split, and the oral cavity is entered (Fig. 7). From the oral cavity the mass is pushed downwards using a finger by an assistant and was delivered via the suprahyoid neck incision. Mass excised completely in pieces and sent for HPE. On histopathological examination an adenomatous hyperplasia of thyroid with cystic changes, areas of hyalinization and hemorrhage were seen. Focal areas showed skeletal muscle bundles and mucous glands.
Fig. 7.

Suprahyoid muscles split
During the post-operative period, Tracheostomy tube care was given. On Post-operative day-2 Ryle’s tube feed was started according to dietician advice. On Post operative day 7, Tracheostomy tube was removed. Suture removal was done on day 10 & wound was healthy.
On examination oral cavity and oropharynx appeared normal (Fig. 8).
Fig. 8.

Examination of Oropharynx
On postoperative video-laryngoscopy (Fig. 9) Oropharynx and post 1/3rd of tongue normal. Vallecula, laryngeal inlet visualized, appeared normal.
Fig. 9.

Post-operative video laryngoscopy
Discussion
Lingual thyroid being a rare developmental anomaly occurs due Failure of descend of embryonic thyroid gland, which usually occurs between 3rd and 7th weeks of embryonic development. [1].
Hickmann recorded the first case of Lingual thyroid in 1869. [2] Lingual thyroid with clinical incidence of 1:100000 has a significant female predominance of 8:1. [3] The differential diagnosis of a lingual thyroid includes vascular tumours, submandibular tumors, telangiectatic granuloma, teratomas, and benign or malignant tumours at posterior aspect of the tongue. [4, 5] Lingual thyroid should be suspected based on thyroid function tests and scintigraphy. [6] An elevated TSH value with decreased T3 and T4 level are commonly seen in thyroid function test in a case of lingual thyroid. [7] Most of the patients though asymptomatic, few may present with symptoms of upper airway obstruction, dysphagia, snoring, dysphonia, and sore throat. [8].
The ectopic thyroid is more prone for conditions such as hyperplasia, thyroid adenoma, thyroiditis, and carcinoma when compared to thyroid gland in its normal position. [9] The most common type of tumor occurring in ectopic thyroid is papillary carcinoma though follicular, mixed follicular and medullary carcinomas have also been demonstrated. [10].
Our case report mainly focuses on an unusual presentation of a huge ectopic lingual thyroid in a male with disproportionate pressure symptoms. In our patient, investigations showed a undescended thyroid tissue at the base of the tongue. Radionucleotide Tc-99 scintigraphy is a used to diagnose the presence of any functional thyroid tissue other than lingual thyroid in the body.
Treatment options for a case lingual thyroid depends on factors such as a general condition of patient, size of the mass, and the pressure symptoms. [11] Euthyroid patients and asymptomatic patients can be followed-up regularly without any treatment. TSH suppression therapy/Thyroxine supplementation is given in mild symptomatic hypothyroid patients. [12] There are various surgical approaches for lingual thyroid excision namely lip split mandibulotomy, suprahyoid approach, cervical/lateral neck approach & transoral approach. We chose suprahyoid approach considering the size of the mass and which would provide a better exposure.
The thyroxine therapy has to be initiated after surgical excision since the lingual thyroid is the only functioning thyroid organ in 70% of ectopic thyroids. [13, 14] We continued the thyroxine supplementation in our patient after excision of the lingual thyroid.
Conclusion
Ectopic thyroid is a rare developmental anomaly. Treatment could be conservative with substitutive thyroxine treatment in patients with small size with mild symptoms, while surgery is recommended in cases with large size with obstructive symptoms. The suprahyoid approach to the lingual thyroid gives better exposure with lesser morbidity.
Declarations
Conflict of Interest
This case report has been done with clear adherence to the ethical standards set by the institutional ethical committee and is in compliance with the ethical standard. This case report does not have any conflict of interest and doesn’t have any funding.
Ethical approval
Obtained.
Informed consent
Obtained.
Footnotes
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
References
- 1.Ce ´rulus G, Hacourt A, Selvais P. Unusual cause of hypothyroidism: about three cases. Louvain Med. 2003;122:82–89. [Google Scholar]
- 2.Hickman W: Congenital tumor of the base of the tongue; causing death by suffoca- tion. Trans Path Soc Lond 20:160–163, 1869
- 3.Klubo-Gwiezdzinska J, Manes RP, Chia SH, Burman KD, Sta- thatos NA, Deeb ZE, et al. Clinical review: ectopic cervical thyroid carcinoma—review of the literature with illustrative case series. J Clin Endocrinol Metab. 2011;96:2684–2691. doi: 10.1210/jc.2011-0611. [DOI] [PubMed] [Google Scholar]
- 4.Jain A, Pathak S. Rare developmental abnormalities of thyroid gland, especially multiple ectopia: a review and our experience. Indian J Nucl Med. 2010;25(4):143–6. doi: 10.4103/0972-3919.78248. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Kumar R, Sharma S, Marwah A, et al. Ectopic goiter masquerading as submandibular gland swelling: a case report and review of the literature. Clinical Nuclear Medicine. 2001 Apr;26(4):306–309. 10.1097/00003072-200104000-00005. PMID: 11290889. [DOI] [PubMed]
- 6.Douglas PS, Baker AW. Lingual thyroid. Br J Oral Maxillofac Surg. 1994;32:123–4. doi: 10.1016/0266-4356(94)90144-9. [DOI] [PubMed] [Google Scholar]
- 7.Farrell ML, Forer M. Lingual thyroid. Aust N Z J Surg. 1994;64:135–8. doi: 10.1111/j.1445-2197.1994.tb02163.x. [DOI] [PubMed] [Google Scholar]
- 8.Thomas G, Hoilat R, Daniels JS, Kalagie W. Ectopic lingual thyroid: a case report. Int J Oral Maxillofac Surg. 2003;32:219–21. doi: 10.1054/ijom.2002.0311. [DOI] [PubMed] [Google Scholar]
- 9.Akyol MU, Ozcan M. Lingual thyroid. Otolaryngol Head Neck Surg. 1996;115:483–4. doi: 10.1177/019459989611500522. [DOI] [PubMed] [Google Scholar]
- 10.Shah BC, Ravichand CS, Juluri S, Agarwal A, Pramesh CS, Mistry RC. Ectopic thyroid cancer. Ann Thorac Cardiovasc Surg. 2000;13(2):122–124. [PubMed] [Google Scholar]
- 11.Gallo A, Leonetti F, Torri E, Manciocco V, Simonelli M. DeVincentiis M.Ectopic lingual thyroid as unusual cause of severe dysphagia. Dysphagia. 2001;16:220–3. doi: 10.1007/s00455-001-0067-7. [DOI] [PubMed] [Google Scholar]
- 12.Rahbar R, Yoon MJ, Connolly LP, et al. Lingual thyroid in children: a rare clinical entity. Laryngoscope 2008 July;118(7): 1174–1179. [DOI] [PubMed]
- 13.Alt B, Elsalini OA, Schrumpf P, et al. Arteries define the posi- tion of the thyroid gland during developmental relocaliza- tion. Development. 2006;133(14):3797–3804. doi: 10.1242/dev.02550. [DOI] [PubMed] [Google Scholar]
- 14.Hazarika P, Siddiqui SA, Pujary K, Shah P, Nayak DR, Balakrishnan R. Dual ectopic thyroid: a report of two cases. J Laryngol Otol. 1998 Apr;112(4):393-5. 10.1017/s0022215100140563. PMID: 9659508. [DOI] [PubMed]