

Abstract
Purpose: to review recent literature concerning long-term health issues and transitional care in esophageal atresia (EA) patients. PubMed, Scopus, Embase and Web of Science databases were screened for studies regarding EA patients aged more than or equal to 11 years, published between August 2014 and June 2022. Sixteen studies involving 830 patients were analyzed. Mean age was 27.4 years (range 11–63). EA subtype distribution was: type C (48.8%), A (9.5%), D (1.9%), E (0.5%) and B (0.2%). 55% underwent primary repair, 34.3% delayed repair, 10.5% esophageal substitution. Mean follow-up was 27.2 years (range 11–63). Long-term sequelae were: gastro-esophageal reflux (41.4%), dysphagia (27.6%), esophagitis (12.4%), Barrett esophagus (8.1%), anastomotic stricture (4.8%); persistent cough (8.7%), recurrent infections (4.3%) and chronic respiratory diseases (5.5%). Musculo-skeletal deformities were present in 36 out of 74 reported cases. Reduced weight and height were detected in 13.3% and 6% cases, respectively. Impaired quality of life was reported in 9% of patients; 9.6% had diagnosis or raised risk of mental disorders. 10.3% of adult patients had no care provider. Meta-analysis was conducted on 816 patients. Estimated prevalences are: GERD 42.4%, dysphagia 57.8%, Barrett esophagus 12.4%, respiratory diseases 33.3%, neurological sequelae 11.7%, underweight 19.6%. Heterogeneity was substantial (> 50%).
Conclusion: EA patients must continue follow-up beyond childhood, with a defined transitional-care path by a highly specialized multidisciplinary team due to the multiple long-term sequelae.
|
What is Known: • Survival rates of esophageal atresia patients is now more than 90% thanks to the improvements in surgical techniques and intensive care, therefore patients’ needs throughout adolescence and adulthood must be taken into account. | |
|
What is New: • This review, by summarizing recent literature concerning long term sequelae of esophageal atresia, may contribute to raise awareness on the importance of defining standardized protocols of transitional and adulthood care for esophageal atresia patients. |
Supplementary Information
The online version contains supplementary material available at 10.1007/s00431-023-04893-6.
Keyword: Esophageal atresia, Transitional care, Systematic review, Long term follow-up
Introduction
Esophageal atresia (EA) is a rare congenital disorder consisting of the disruption of the esophageal continuity, with or without the persistence of a tracheoesophageal fistula (TEF). The estimated birth incidence is 1:2500–3000 live births with a slight male preponderance [1]. Thanks to the improvement of surgical techniques and intensive care, postnatal survival nowadays is more than 90% [1], meaning that most patients reach adolescence and adulthood. While follow-up throughout childhood is well standardized, the interest in transitional care and its impact on patients’ health is relatively recent and constantly rising. A 2014 meta-analysis [2] quantified the prevalence of long-term issues referable to EA in order to lay the foundations for standardized transitional care protocols. Furthermore, a qualitative study [3] reported physical and mental health problems identified by the patients themselves as relevant and therefore worthy of being addressed in follow-up programs. Nonetheless, shared guidelines for the management of adolescent and adult EA patients are still lacking.
The aim of this study was to review the recent literature concerning long term follow-up and transitional care in adolescent and adult EA patients, in particular to determine whether structured transitional care programs are being followed and their impact on patients’ health.
Methods
This review was performed according to the PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) [4] and SWiM (Synthesis Without Meta-analysis) [5] reporting guidelines.
Search strategy
PubMed, Embase, Scopus and Web of Science were screened electronically until July 2022, using the key words “transitional care AND esophageal atresia OR long term follow-up AND esophageal atresia”. The search and selection criteria were restricted to the English language. Reference lists of relevant articles and reviews were hand searched for additional reports. The publication span included the period August 2014–June 2022.
Inclusion criteria
Inclusion criteria were: (1) original studies and (2) sufficient data concerning EA patients aged equal or more than 11 years. The age limit of 11 years old was defined in order to have enough long-term follow-up for outcome evaluation and to avoid including in the analysis younger children. Two authors (GB and MG) reviewed all abstracts independently. Agreement about potential relevance was reached by consensus, and full-text copies of those articles were obtained. Quality assessment was performed by two authors (GB and MG) using the Newcastle–Ottawa Scale [6].
Exclusion criteria
For the descriptive analysis we excluded: (1) articles published before August 2014 to avoid overlap with the results of another exhaustive meta-analysis that summarized the literature from 1993 to July 2014 [2]; (2) systematic reviews in order to analyze original data; (3) studies that did not report the analyzed outcomes (detailed in the next paragraph) referred to EA patients ≥ 11 years; (4) articles written in languages other than English. For the meta-analysis, we excluded studies with less than 5 patients.
Data extraction and synthesis
Studies were assessed according to the following variables: population (age at follow-up, years; sex; follow-up, years), clinical characteristics (EA type; associated congenital anomalies), surgical features (type of repair; other surgeries in the first years of life) and outcomes grouped by systems (gastrointestinal, respiratory, musculoskeletal, neurodevelopment, mental health and quality of life, other). The same reviewers mentioned above independently extracted relevant data regarding study characteristics, patients’ features, and outcomes. Inconsistencies were discussed by the reviewers and consensus reached. If more than one study was published for the same cohort with identical end points, the report containing the most comprehensive information on the population was included to avoid overlapping populations. Results are presented with descriptive statistics. Quantitative variables were summarized as mean and ranges, while qualitative variables were summarized as frequency rates. Results for each outcome were calculated considering the subtotal of patients obtained by the studies that reported the outcome. Statistical analysis was performed using Microsoft Office Excel.
Additionally, pooled estimates for the occurrence of main findings were calculated through a meta-analysis that, in order to cope with the presumptive heterogeneity in study design, was designed through a random effect model. I2 statistic was then applied in order to estimate the amount of inconsistency between included studies (i.e. the percentage of total variation across studies that could be associated with underlying heterogeneity rather than chance), and the following categorization was taken in account: I2 ranging between 0 to 25% = low heterogeneity; I2 ranging between 26 and 50% = moderate heterogeneity; I2 ≥ 50% = substantial heterogeneity. Publication bias was then investigated through calculation of the contour-enhanced funnel plots, and Egger test for quantitative publication bias analysis (at a 5% of significance level). Radial plots were then calculated and visually inspected to rule out small study bias. All analyses were performed by means of “meta”, “metafor”, and “robvis” packages with R (version 4.0.3) and RStudio (version 1.1.463) software. The aforementioned packages are an open-source add-ons for conducting meta-analyses.
Results
Study search and selection
1025 articles were screened. Excluding duplicates, 16 articles met the inclusion criteria and were considered for descriptive analysis, including 830 patients, while 11 articles met the inclusion criteria for the meta-analysis, with a total of 816 patients (Fig. 1).
Fig. 1.
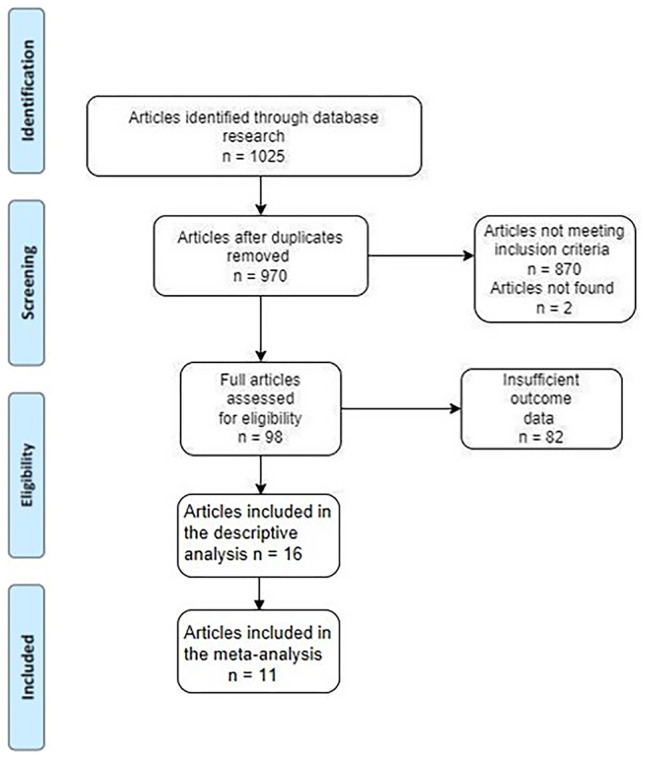
Diagram summarizing the results of the systematic analysis
Descriptive analysis
A total of 830 patients were considered in the review. Table 1 [7–22] summarizes the patients’ most important characteristics, as obtained from the analyzed articles.
Table 1.
Key details of the papers included in the descriptive analysis
| Author | n° patients | EA type | Age at follow-up mean (range) | GI outcomes | Respiratory outcomes | Musculoskeletal outcomes | Design | Year |
|---|---|---|---|---|---|---|---|---|
| Arneitz et al. [7] | 19 | A (1); B (1); C (16); D (1) | 24.7 y (14–40) | dysphagia (5); GERD (6); other (9) | cough (4); 13 chronic disorder | mean low muscle mass | prospective | 2020 |
| Curci and Dibbins [8] | 1 | C | 23 y | GERD | N | scoliosis | case report | 2015 |
| Dessanti et al. [9] | 2 | A (2) | 36 y (29–43) | N (2) | n.s. | n.s. | case report | 2021 |
| Di Natale et al. [10] | 4 | A (1); C (3) | 23.2 y (n.s.) | dysphagia (3); GERD (1) | n.s. | asymmetric thorax (1); scoliosis (1); rib fusions (1); winged scapula (1) | retrospective | 2021 |
| Gatzinsky et al. [11] | 29 | n.s. | 31 y (25–40) | dysphagia (22); GERD (11); esophagitis (14); Barrett (2); other (17) | n.s. | n.s. | retrospective | 2016 |
| Gibreel et al. [12] | 46 | A (4); C (40); D (1); E (1) | 40 y (18–63) | dysphagia (38); GERD (12); anastomotic stenosis (18) | n.s. | n.s. | retrospective | 2017 |
| Hannon et al. [13] | 64 | A (14); B (1); C (45); D (4) | 29 y (n.s.) | dysphagia (28); GERD (32); anastomotic stenosis (15); Barrett (1); other (20) | chronic disorder (9) | n.s. | retrospective | 2019 |
| Hsieh et al. [14] | 3 | C (3) | 15.6 y (13.6–17) | dysphagia (1); Barrett (3); other (1) | n.s. | n.s. | retrospective | 2017 |
| Huynh-Trudeau et al. [15] | 41 | C (35); n.s. (6) | 25 y (18–44) | dysphagia (30); GERD (12); esophagitis (8); Barrett (10); other (71) | n.s. | n.s. | prospective | 2015 |
| Leibovitch et al. [16] | 26 | n.s. | n.s. (12–21 y) | GERD (5); anastomotic stenosis (1) | chronic disorder (9); recurrent infections (5); other (2) | n.s. | retrospective | 2018 |
| Mikkelsen et al. [17] | 68 | A (3); C (58); D (4); E (3) | 16 y (13–20) | dysphagia (58); GERD (44) | n.s. | n.s.. | cross-sectional | 2020 |
| Okuyama et al. [18] | 69 | A (6); C (63) | 19 y (15–33) | dysphagia (5); other (3) | oxygen dependence (1); other (2) | scoliosis (25); asymmetric thorax (8); elevated scapula (18) | retrospective | 2017 |
| Presse et al. [19] | 37 | A (6); C (31) | 25.3 y (18–44) | dysphagia (24); other (16) | n.s. | n.s | prospective | 2016 |
| Schneider et al. [20] | 120 | A (6); C (108); D (6) | 16.5 y (n.s.) | dysphagia (70); GERD (49); esophagitis (80); Barrett (51); anastomotic stenosis (4); other (12) | cough (48) | n.s. | prospective | 2016 |
| Svoboda et al. [21] | 297 | A (34); n.s. (263) | n.s. (≥ 11y) | GERD (169) | recurrent infections (21) | n.s. | retrospective | 2018 |
| Vergouwe et al. [22] | 4 | A (2); C (2) | 48.25 y (36–47) | dysphagia (3); GERD (1); esophagitis (1); anastomotic stenosis (2); cancer (5); other (1) | chronic disorder (2) | n.s. | case-series | 2018 |
Esophagitis was defined endoscopically. N° patients per endpoint reported in brackets. EA type as in Gross classification
y years, Y yes, N none, n.s. not specified, GERD gastro-esophageal reflux disease
Patients’ mean age was 27.4 years (range 11–63 years). Sex was specified in 507 patients: 259 (51%) were male, 248 (49%) female. The most common subtype (according to Gross classification) was type C (405 patients, 48.8%), followed by: type A (79, 9.5%), type D (16, 1.9%), type E (4, 0.5%) and type B (2, 0.2%). In 324 (39%) cases the subtype was not described. The reported associated congenital anomalies were: cardiac in 53 patients (6.4%); gastrointestinal in 28 (3.4%); vertebral in 27 (3.2%); renal in 23 (2.8%); musculoskeletal in 8 (1%); VACTERL/VACTER association in 17 (2%); other than the previously cited in 19 (2.3%). In 472 (57%) cases the presence or absence of other congenital anomalies was not reported. The type of repair was reported in 496 patients: the most common was primary repair (275 patients, 55.4%), followed by delayed repair (170 cases, 34.3%), and esophageal substitution (52 patients, 10.5%). In the latter subgroup, the transposition performed was gastric in 37 cases, colonic in 5 and jejunal in 2; the transposed organ was not specified in 8 cases. Concerning other surgeries during childhood, esophageal dilatations are reported in 142 patients (17%), with a range of 1–108 dilatations per patient [17]; fundoplication in 105 (12.6%); aortopexy in 10 (1.2%); repair of recurrent TEF in 5 (0.6%); other not specified surgeries in 5 (0.6%). Mean age at follow-up was 27.4 years (range 11–63 years).
All studies reported data concerning gastrointestinal outcomes. One hundred sixty one patients [15, 20] were evaluated for the study purposes (either through endoscopy, barium swallow and manometry), while in the remaining 669 cases data was obtained retrospectively. The most frequently reported signs were GERD symptoms (gastro-esophageal reflux disease, 344 patients, 41.4% of total) and dysphagia (229 cases, 27.6%). A hiatal hernia was identified in 33 cases (4%), while esophagitis was histologically documented in 103 patients (12.4%) and Barrett esophagus in 67 (8.1%). Anastomotic stricture was present in 40 patients (4.4%) and food blockage was observed in 22 (2.6%) cases. Esophageal hypomotility was documented in 55 patients (6.6%). 10 patients (1.2%) necessitated nutritional support. 5 (0.6%) cases of esophageal cancer were reported. Other symptoms were signaled in 30 patients (3.6%), such as upper gastrointestinal bleeding, dumping syndrome and the necessity of revision surgery [13].
Respiratory outcomes were reported in 600 out of 830 patients. Nineteen patients underwent prospective clinical examination, spirometry and spiroergometry [7]. Persistent cough was described in 52 cases (8.7%); chronic respiratory disease (not specified whether obstructive or restrictive) in 33 (5.5%); recurrent respiratory infections in 26 (4.3%); asthma in 10 (1.7%); restrictive respiratory disorder in 9 (1.5%); other morbidities like oxygen-dependence and recurrent TEF [18] in 8 (1.3%). A study found that EA patients present minor alterations in respiratory microbiome as compared to healthy peers, associated with decreased performance capacity and peak VO2 (volume of oxygen consumed) [7].
Musculoskeletal outcomes were described in 74 patients. Recent X-ray examinations were reviewed in 4 cases [10]. Scoliosis was observed in 27 patients (36.5%); winged or elevated scapula in 19 (25.7%); chest wall deformity in 9 (12%); rib fusion in 1 (1.3%). A study pointed out a lower mean muscle mass compared to controls [7].
Neurological sequelae were delineated in 135 patients: there are 12 reported cases of mental retardation (8.9%) and 1 of cerebral palsy (0.7%).
Mental health and quality of life (QoL) were evaluated in 5 studies, totaling 208 patients; a reduced QoL compared to healthy peers was identified using validated questionnaires in 19 cases (9%). Mental disorders were present in 20 patients (9.6%): depression in 9, PTSD (post-traumatic stress disorder) in 6 and a raised risk to develop an overt mental illness in 5 [17].
Among other long term outcomes observed (700 patients), 93 patients (13.3%) were underweight and 42 (6%) had a reduced height compared to general population, while only 13 patients were obese (1.8%). 3 patients (0.4%) underwent a renal transplant in adulthood. Chronic anemia was reported in 18 cases (2.6%), 15 of whom were corrected through gastric transposition. Allergy or food intolerance were described in 9 patients (1.3%). Interestingly, 72 patients (10.3%) had no care provider [21].
Meta-analysis
Eleven studies with more than 5 patients were considered for meta-analysis after quality assessment with New-Ottawa scale (Table 2). A total of 816 patients were considered. Figure 2 shows the forest and funnel plots for GERD, dysphagia, Barrett esophagus, respiratory sequelae, neurological sequelae and underweight.
Table 2.
Quality Assessment [6]
| Author | Year | Country | Quality Score | Ottawa Score |
|---|---|---|---|---|
| Arneitz et al. [7] | 2020 | Austria | high quality | 7 |
| Gatzinsky et al. [11] | 2016 | Sweden | high quality | 7 |
| Gibreel et al. [12] | 2017 | USA | high quality | 7 |
| Hannon et al. [13] | 2019 | UK | high quality | 7 |
| Huynh-Trudeau et al. [15] | 2015 | Canada | high quality | 7 |
| Leibovitch et al. [16] | 2018 | Israel | high risk | 6 |
| Mikkelsen et al. [17] | 2020 | Norway | high quality | 7 |
| Okuyama et al. [18] | 2017 | Japan | high quality | 7 |
| Presse et al. [19] | 2016 | Canada | high quality | 7 |
| Schneider et al. [20] | 2016 | France, Canada, Belgium | high quality | 7 |
| Svoboda et al. [21] | 2018 | Germany, UK | high risk | 6 |
Fig. 2.

Forest plots of pooled estimated prevalence alongside with the related funnel plots and standard error
Ten studies reported data on GERD (340 patients). The estimated prevalence is 42.4%, with a 95% CI (confidence interval) of 33.2% to 52.1% and heterogeneity of 80%.
Dysphagia was reported in 9 studies (280 patients), with an estimated prevalence of 57.8% (95% CI 37.1% to 76.1%) and heterogeneity of 90%.
Barrett esophagus was described in 4 studies (64 patients). The estimated prevalence is 12.4% (95% CI 3.1% to 38.3%) and heterogeneity of 88%.
Overall, respiratory sequelae (cough, recurrent respiratory infections, chronic respiratory disorders) were reported in 6 studies (115 patients), with an estimated prevalence of 33.3% (95% CI 10.1% to 69%) and heterogeneity of 92%.
Neurological sequelae were described in 3 studies (18 patients). Estimated prevalence is 11.7% (95% CI 6.7% to 19.8%), with a heterogeneity of 58%.
Lastly, 6 studies reported 93 underweight patients, with an estimated prevalence of 19.6% (95% CI 11.6% to 31.1%) and heterogeneity of 86%.
Details of the meta-analysis can be found in the Supplementary file online.
Discussion
Advances in surgical techniques and intensive care have resulted in a radical improvement in the survival of patients with congenital anomalies as EA. At the same time, these advances present new challenges for the pediatric surgeon, by creating a subset of adult patients with characteristic long-term outcomes and specific needs. Transitional care has been defined as a planned movement of adolescents and young adults with chronic physical and medical conditions from child-centered to adult-oriented health-care systems [23]. It is gaining more and more importance in the management of EA patients; efforts must be put in creating standardized follow-up protocols throughout adolescence and adulthood to avoid and promptly treat detrimental consequences on patients’ health [24]. Positive impact of transitional care has been reported in a 2017 study [25], in which a two-day educational program for EA adolescents and their parents met a high satisfaction, but at the same time highlighted a low pre-existing transition-specific knowledge. The aim of this systematic review is to underline the long-term health problems in EA patients in order to establish proper follow-up and transitional care protocols to be shared with adult specialists: gastroenterologists, surgeons, pneumologists, orthopedics, neurologists and psychologists.
The analyzed sample includes 830 adolescent and adult EA patients’, aging from 11 to 63 years. Findings concerning long term outcomes were consistent with other reports in literature, in particular with a recent meta-analysis by Connor et al. [2], as gastrointestinal symptoms are the most reported complaint, the most frequent being GERD (41.4%) and dysphagia (27.6%). These and other symptoms, such as food blockage due to anastomotic stenosis or esophageal hypomotility, have a detrimental impact on quality of life. Moreover, the reported prevalence of esophagitis (12.4%), Barrett esophagus (8.1%) and esophageal cancer (0.6%) renders standardized endoscopic follow-up mandatory. A consensus conference conducted by ERNICA (European Reference Network for Rare Inherited Congenital Anomalies) [26] aimed to define surgical follow-up guidelines for EA patients, reviewing simultaneously the ESPGHAN (European Society for Pediatric Gastroenterology Hepatology and Nutrition) 2016 guidelines [27]. General consensus was reached regarding the necessity of a scheduled endoscopic and 24-ph or ph-impedance monitoring in EA children and adolescents, although the frequency of such exams was not defined; on the other hand, an agreement concerning the role of routine contrast upper gastrointestinal studies was not reached. Concerning adult patients, the ESPGHAN surveillance guidelines were considered adequate: routine endoscopy (with biopsies in four quadrants at gastroesophageal junction and anastomotic site) at time of transition into adulthood and every 5–10 years; on-demand adjunctive endoscopies according to the presence of new or worsening symptoms or of Barrett esophagus. Another recent study [28] also suggested following the ESPGHAN guidelines to tackle adequately gastrointestinal issues in EA adult patients.
Respiratory symptoms have been underreported compared to digestive ones, being specified in 600 out of 830 patients. The most common were persistent cough (8.7%); chronic respiratory diseases (8.7%) and recurrent respiratory infections (4.3%); our data were not sufficient to determine the correlation with GERD. Respiratory symptoms reported in EA children can persist in adulthood, as already highlighted in previous studies [29]. The etiopathogenesis appears to be multifactorial [30]: the malformation itself, particularly if a TEF was present; persistent GERD; an acquired damage after surgery and repeated respiratory infections in childhood. Nonetheless, respiratory symptoms are often overlooked by general practitioners and patients’ themselves compared to digestive ones [18]. Therefore, EA patients’ pulmonary function should be regularly assessed, particularly in patients who underwent esophageal substitution as they may present, additionally, a reduced lung capacity due to compression by the transposed organ [13]. During the ERNICA conference [26], general consensus was reached regarding the necessity of scheduled lung function tests in EA children and adolescents, while routine bronchoscopies are not deemed necessary. A recent paper endorsed by INoEA (International Network of Esophageal Atresia) also suggests the use of pulmonary function tests in the follow-up of adolescent EA patients, along with chest CT scan for detection of bronchiectasis [31]. We did not find specific protocols for a pneumological follow-up in EA adult patients in literature.
The musculoskeletal morbidities described appear consistent with those thoroughly reported in literature [32]. Although our data do not allow us to correlate these outcomes with the presence of vertebral congenital anomalies nor with the surgical technique, they seem more common in patients who underwent a thoracotomy [18]. In the cohort reported by Di Natale et al. [10], rib fusions and winged scapula were reported more frequently in subjects aged above 18 years old than in other age groups; probably in this group thoracoscopy or muscle-sparing thoracotomy were performed less often. In a recent systematic review [33], secondary scoliosis after thoracotomy repair in EA children is reported in 13% of cases; according to a meta-analysis by Drevin et al. [34], musculoskeletal complications are less common with the thoracoscopic approach. Considering only adult patients, a study by Sistonen et al. [35] reported a 13-fold risk of scoliosis compared to the general population, with rib fusions post-thoracotomy being the strongest predictive factor; however, spinal surgery was never needed. As further studies are needed to define technique-related differences in musculoskeletal outcomes, efforts must be put also in defining the orthopedic follow-up in adult EA patients.
Considering neurological outcomes, 8.9% of patients were diagnosed with mental retardation; it was not possible to define the correlation with prematurity, associated congenital anomalies or other perinatal factors. Impairment in motor and cognitive function in EA children are well described in literature [36]. Early identification is essential in these patients to limit detrimental effects through supportive services such as occupational therapy, speech and language therapy, dietetics and physiotherapy teams [37]. Nonetheless, we did not find studies reporting details concerning neurological follow-up in adolescence and adulthood.
According to our data, 9% of patients reported a reduced QoL and 9.6% presented a mental disorder or a raised risk to develop one. An adequate transitional care program, including psychiatric and psychological support, can prevent development and worsening of such conditions, whereas the absence of such programs cause patients to feel “thrown into the unknown” [38], negatively influencing QoL and mental health.
Interestingly, a reduced weight (13.3%) and height (6%) can persist in adult EA patients. A recent study [39], highlighted risk factors for poor nutrition in EA children and the importance of having an early personalized nutritional program to prevent undergrowth. Our data suggest including nutritional consultations when planning a transitional care program.
Lastly, 10.3% adult EA patients reported to have no care provider [21]; this data underlines that current efforts in improving transitional care must be continued and implemented. In particular, as promoted by ERNICA [26], centralization of rare congenital diseases can improve patient care in every life phase, from birth and throughout adulthood, by registering cases and offering standardized and up-to-date healthcare.
The meta-analysis allowed us to define estimated prevalence for major outcomes (GERD, dysphagia, Barrett esophagus, respiratory sequelae, neurological sequelae and underweight), confirming that a significant proportion of EA patients is affected by long term health problems with a potentially high impact on quality of life. The most significant outcome appears to be dysphagia, with an estimated prevalence of 57.8%. However, due to the substantial heterogeneity of the included studies, no conclusions concerning the effective impact of these conditions can be drawn. Prospective transitional care programs can be useful to define the prevalence of long-term outcomes and how they can be reduced with adequate follow-up.
Conclusions
Limitations
Limitations and bias derive from the features of the studies included in this review: most studies are retrospective studies lacking some of the target data, therefore a complete evaluation of all long-term outcomes was not possible and a more extensive meta-analysis could not be performed. Furthermore, no study reported transitional care programs and a long-term evaluation of their impact on patients’ health.
Implications for clinical practice and research
It is well known that numerous long-term outcomes can persist in EA patients throughout adolescence and adulthood. Patients with congenital malformations seek for information concerning transfer to adult care and require a regular follow-up by specialized centers [40]. Although both EA long term outcomes and patient-driven proposals for follow-up programs are well described in literature, further studies reporting transitional-care programs and their effects on patients’ health are needed in order to help to improve current care practices for adolescent and adult EA patients. As a matter of fact, in clinical practice adult EA patients (as well as patients with other congenital malformations) often can rely only on pediatric specialists for regular follow-up, as knowledge regarding these patients is still limited among general surgeons and practitioners. This issue derives from the fact that congenital malformations are rare diseases and therefore uncommonly encountered in adult care practice. We hope that this review, which summarizes recent literature concerning adolescent and adult EA patients, can raise awareness about these patients’ needs among not only pediatricians and pediatric surgeons but also adult care providers. The ultimate goal is to improve transitional care by standardizing protocols in specialized centers as well as keeping general practitioners, adult specialists and general surgeons updated on this subset of patients that will be more and more encountered in everyday practice. The adoption of prospective standardized protocols in the early treatment, follow-up and transitional care of EA patients is an important and attractive field of clinical research, with positive effects on clinical practice and on the outcomes of this complex malformation.
Supplementary Information
Below is the link to the electronic supplementary material.
Authors' contributions
G.B. and M.G. performed the research and statistical analysis. A.R. performed the meta-analysis. G.B. wrote the main manuscript text. M.B., G.R. and A.R. reviewed the manuscript.
Funding
Open access funding provided by Università degli Studi di Pavia within the CRUI-CARE Agreement.
Data availability
The datasets generated during and/or analysed during the current study are available from the corresponding author on reasonable request.
Declarations
Ethical approval
According to the current legislation, anonymized data may be analyzed and used in aggregate form for scientific purposes without further authorization, meaning that no formal ethical committee approval was needed.
Competing interests
The authors declare no competing interests.
Footnotes
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Contributor Information
G. Brooks, Email: giulia.brooks90@gmail.com
M. Gazzaneo, Email: marta.gazzaneo@gmail.com
M. Bertozzi, Email: mirko.bertozzi@unipv.it
G. Riccipetitoni, Email: giovanna.riccipetitoni@unipv.it
A. Raffaele, Email: a.raffaele@smatteo.pv.it
References
- 1.Holcomb GJ, Murphy P, Peter S. Ashcraft's Pediatric Surgery. 7. Amsterdam: Elsevier; 2019. [Google Scholar]
- 2.Connor MJ, Springford LR, Kapetanakis VV, Giuliani S. Esophageal atresia and transitional care - step 1: a systematic review and meta-analysis of the literature to define the prevalence of chronic long-term problems. The American Journal of Surgery. 2015;209:747–759. doi: 10.1016/j.amjsurg.2014.09.019. [DOI] [PubMed] [Google Scholar]
- 3.ten Kate CA, Rietman AB, Kamphuis LS, Gischler S, Lee D, Fruithof J, Wijnen RMH, Spaander MCM. Patient-driven healthcare recommendations for adults with esophageal atresia and their families. J Ped Surg. 2021;56:1932–1939. doi: 10.1016/j.jpedsurg.2020.12.024. [DOI] [PubMed] [Google Scholar]
- 4.Moher D, Liberati A, Tetzlaff J, Altman DG (2009) Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. PLoS Med 6:e1000097. 10.1371/journal.pmed.1000097 [DOI] [PMC free article] [PubMed]
- 5.Campbell M, McKenzie JE, Sowden A et al (2020) Synthesis without meta-analysis (SWiM) in systematic reviews: reporting guideline. BMJ 16(368):l6890. 10.1136/bmj.l6890 [DOI] [PMC free article] [PubMed]
- 6.Wells GA, Shea B, O’Connell D et al (2000) The Newcastle-Ottawa Scale (NOS) for assessing the quality of nonrandomised studies in meta-analyses. Available at: http://www.ohri.ca/programs/clinical_epidemiology/oxford.asp
- 7.Arneitz C, Windhaber J, Castellani C, Kienesberger B, Klymiuk I, Fasching G, Till H, Singer G. Cardiorespiratory performance capacity and airway microbiome in patients following primary repair of esophageal atresia. Pediatr Res. 2021;90:66–73. doi: 10.1038/s41390-020-01222-7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Curci M, Dibbins A (2015) Unilateral pulmonary agenesis and esophageal atresia with a tracheoesphageal fistula-23 year followup. J Ped Surg Case Rep 3:141–142 10.1016/j.epsc.2015.02.001
- 9.Dessanti A, Falchetti D, Di Benedetto V, Scuderi MG (2021) Pedicled jejunal interposition as esophageal substitute in pediatric patients. Technical considerations and long - term results. J Ped Surg Case Reports 64:101744. 10.1016/j.epsc.2020.101744
- 10.Di Natale A, Brestel J, Mauracher AA, Tharakan SJ, Meuli M, Möhrlen U, Subotic U (2022) Long-term outcomes and health-related quality of life in a swiss patient group with esophageal atresia. Eur J Pediatr Surg Aug 32(4):334–345. 10.1055/s-0041-1731391 [DOI] [PubMed]
- 11.Gatzinsky V, Andersson O, Eriksson A, Jönsson L, Abrahamsson K, Sillén U. Added Value of pH Multichannel Intraluminal Impedance in Adults Operated for Esophageal Atresia. Eur J Pediatr Surg. 2016;26:172–179. doi: 10.1055/s-0034-1544049. [DOI] [PubMed] [Google Scholar]
- 12.Gibreel W, Zendejas B, Antiel RM, Fasen G, Moir CR, Zarroug AE (2017) Swallowing dysfunction and quality of life in adults with surgically corrected esophageal Atresia/Tracheoesophageal Fistula as infants. Ann Surg Aug 266(2):305–310. 10.1097/SLA.0000000000001978 [DOI] [PubMed]
- 13.Hannon E, Eaton S, Curry JI, Kiely EM, Spitz L, De Coppi P. Outcomes in adulthood of gastric transposition for complex and long gap esophageal atresia. J Ped Surg. 2020;55:639–645. doi: 10.1016/j.jpedsurg.2019.08.012. [DOI] [PubMed] [Google Scholar]
- 14.Hsieh H, Frenette A, Michaud L, Krishnan U, Dal-Soglio DB, Gottrand F, Faure C. Intestinal Metaplasia of the Esophagus in Children With Esophageal Atresia. JPGN. 2017;65:e1–e4. doi: 10.1097/MPG.0000000000001558. [DOI] [PubMed] [Google Scholar]
- 15.Huynh-Trudeau V, Maynard S, Terzic T, Soucy G, Bouin M. Dysphagia among adult patients who underwent surgery for esophageal atresia at birth. Can J Gastroenterol Hepatol. 2015;29(5):91–94. doi: 10.1155/2015/787069. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Leibovitch L, Zohar I, Maayan-Mazger A, Mazkereth R, Strauss T, Bilik R (2018) Infants born with esophageal atresia with or without tracheo-esophageal fistula: short- and long-term outcomes. Isr Med Assoc J. Mar 20(3):161–166 [PubMed]
- 17.Mikkelsen A, Boye B, Diseth TH, Malt U, Mørkridd L, Ijsselstijn H, Emblem R (2022) Traumatic stress, mental health and quality of life in adolescents with esophageal atresia. J Pediatr Surg Jul 57(7):1423–1431. 10.1016/j.jpedsurg.2020.10.029 [DOI] [PubMed]
- 18.Okuyama H, Tazuke Y, Uenoa T, Yamanaka H, Takama Y, Saka R, Nara K, Usui N. Long-term morbidity in adolescents and young adults with surgically treated esophageal atresia. Surg Today. 2017;47:872–876. doi: 10.1007/s00595-016-1462-x. [DOI] [PubMed] [Google Scholar]
- 19.Presse N, Taillefer J, Maynard S, Bouin M. Insufficient Body Weight of Adults Born With Esophageal Atresia. JPGN. 2016;62:469–473. doi: 10.1097/MPG.0000000000000961. [DOI] [PubMed] [Google Scholar]
- 20.Schneider A, Gottrand F, Bellaiche M, Becmeur F, Lachaux A, Bridoux-Henno L, Michel J, Faure C, Philippe P, Vandenplas Y, Dupont C, Breton A, Gaudin J, Lamireau T, Muyshont L, Podevin G, Viola S, Bertrand V, Caldari D, Colinet S, Wanty C, Sauleau E, Leteurtre E, Michaud L. Prevalence of Barrett Esophagus in Adolescents and Young Adults With Esophageal Atresia. Ann Surg. 2016;264:1004–1008. doi: 10.1097/SLA.0000000000001540. [DOI] [PubMed] [Google Scholar]
- 21.Svoboda E, Fruithof J, Widenmann-Grolig A, Slater G, Armand F, Warner B, Eaton S, De Coppi P, Hannon E. A patient led, international study of long term outcomes of esophageal atresia: EAT 1. J Ped Surg. 2018;53:610–615. doi: 10.1016/j.jpedsurg.2017.05.033. [DOI] [PubMed] [Google Scholar]
- 22.Vergouwe FWT, Gottrand M, Wijnhoven BPL, IJsselstijn H, Piessen G, Bruno MJ, Wijnen RMH, Spaander MCW (2018) Four cancer cases after esophageal atresia repair: Time to start screening the upper gastrointestinal tract. World J Gastroenterol 24(9):1056–1062. 10.3748/wjg.v24.i9.1056 [DOI] [PMC free article] [PubMed]
- 23.Blum RW, Garell D, Hodgman CH, Jorissen TW, Okinow NA, Orr DP, Slap G (1993) Transition from child-centered to adult health-care systems for adolescents with chronic conditions. A position paper of the Society for Adolescent Medicine. J Adolesc Health 14(7):570–6. 10.1016/1054-139x(93)90143-d [DOI] [PubMed]
- 24.Sampat K, Losty PD. Transitional care and paediatric surgery BJS. 2016;103:163–164. doi: 10.1002/bjs.10118. [DOI] [PubMed] [Google Scholar]
- 25.Dingemann J, Szczepanski R, Ernst G, Thyen U, Ure B, Goll M, Menrath I. Transition of Patients with Esophageal Atresia to Adult Care: Results of a Transition-Specific Education Program. Eur J Pediatr Surg. 2017;27:61–67. doi: 10.1055/s-0036-1587334. [DOI] [PubMed] [Google Scholar]
- 26.Dingemann C, Eaton S, Aksnes G, Bagolan P, Cross KM, De Coppi P, Fruithof J, Gamba P, Husby S, Koivusalo A, Rasmussen L, Sfeir R, Slater G, Svensson JF, Van der Zee DC, Wessel LM, Widenmann-Grolig A, Wijnen R, Ure BM (2020) ERNICA Consensus Conference on the Management of Patients with Esophageal Atresia and Tracheoesophageal Fistula: Follow-up and framework. Eur J Pediatr Surg 30:475–482. 10.1055/s-0039-3400284 [DOI] [PubMed]
- 27.Krishnan U, Mousa H, Dall’Oglio L, Homaira N, Rosen R, Faure C, Gottrand F, ESPGHAN-NASPGHAN Guidelines for the Evaluation and Treatment of Gastrointestinal and Nutritional Complications in Children With Esophageal Atresia-Tracheoesophageal Fistula. JPGN. 2016;63:550–570. doi: 10.1097/MPG.0000000000001401. [DOI] [PubMed] [Google Scholar]
- 28.Aumar M, Nicolas A, Sfeir R, Seguy D, Gottrand F (2022) Long term digestive outcome of œsophageal atresia. Best Pract Res Clin Gastroenterol 56–57 101771 10.1016/j.bpg.2021.101771 [DOI] [PubMed]
- 29.Gatzinsky V, Wennergren G, Jönsson L, Ekerljung L, Houltz B, Redfors S, Sillén U, Gustafsson P. Impaired peripheral airway function in adults following repair of esophageal atresia. J Ped Surg. 2014;49:1347–1352. doi: 10.1016/j.jpedsurg.2013.12.027. [DOI] [PubMed] [Google Scholar]
- 30.Patria MF, Ghislanzoni S, Macchini F, Lelii M, Mori A, Leva E, Principi N, Esposito S. Respiratory Morbidity in Children with Repaired Congenital Esophageal Atresia with or without Tracheoesophageal Fistula. Int J Environ Res Public Health. 2017;14:1136. doi: 10.3390/ijerph14101136. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Koumbourlis AC, Belessis Y, Cataletto M, Cutrera R, DeBoer E, Kazachkov M, Leberge S, Popler J, Porcaro F, Kovesi T (2020) Care recommendations for the respiratory complications of esophageal atresia-tracheoesophageal fistula. The International Network of Esophageal Atresia, Respiratory Complications Working Group. Pediatr Pulmonol. 10.1002/ppul.24982 [DOI] [PubMed]
- 32.Wei S, Saran N, Emil S. Musculoskeletal deformities following neonatal thoracotomy: long-term follow-up of an esophageal atresia cohort. J Ped Surg. 2017;52:1898–1903. doi: 10.1016/j.jpedsurg.2017.08.062. [DOI] [PubMed] [Google Scholar]
- 33.Mishra PR, Tinawi GK, Stringer MD. Scoliosis after thoracotomy repair of esophageal atresia: a systematic review. Pediatr Surg Int. 2020;36:755–761. doi: 10.1007/s00383-020-04683-3. [DOI] [PubMed] [Google Scholar]
- 34.Drevin G, Andersson B, Svensson JF. Thoracoscopy or Thoracotomy for Esophageal Atresia. A Systematic Review and Meta-analysis. Ann Surg. 2021;274:945–953. doi: 10.1097/SLA.0000000000004239. [DOI] [PubMed] [Google Scholar]
- 35.Sistonen SJ, Helenius I, Peltonen J, Sarna S, Rintala RJ, Pakarinen MP (2009) Natural history of spinal anomalies and scoliosis associated with esophageal atresia. Pediatrics 124(6):e1198–204. 10.1542/peds.2008-3704 [DOI] [PubMed]
- 36.van Hoorn CE, en Kate CA, Rietman AB, Toussaint-Duyster LCC, Stolker RJ, Wijnen RMH, de Graaff JC (2021) Long-term neurodevelopment in children born with esophageal atresia: a systematic review. Dis Esophagus 34(11):doab054. 10.1093/dote/doab054 [DOI] [PMC free article] [PubMed]
- 37.Mawlana W, Zamiara P, Lane H, Marcon M, Lapidus-Krol E, Chiu PPL, Moore AM. Neurodevelopmental outcomes of infants with esophageal atresia and tracheoesophageal fistula. J Ped Surg. 2018;53:1651–1654. doi: 10.1016/j.jpedsurg.2017.12.024. [DOI] [PubMed] [Google Scholar]
- 38.Haig-Ferguson A, Wallace V, Davis C. The lived experience of adults and parents: Transitioning from paediatric to adult health care with oesophageal atresia and tracheo-oesophageal fistula. J Clin Nurs. 2022;00:1–10. doi: 10.1111/jocn.16333. [DOI] [PubMed] [Google Scholar]
- 39.Pelizzo G, Destro F, Selvaggio GGO, Maestri L, Roveri M, Bosetti A, Borsani B, Pendezza E, Meroni M, Pansini A, La Pergola E, Riccipetitoni G, De Silvestri A, Cena H, Calcaterra V. Esophageal Atresia: Nutritional Status and Energy Metabolism to Maximize Growth Outcome. Children. 2020;7:228. doi: 10.3390/children7110228. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 40.Kassa AM, Engvall G, Dellenmark Blom M, Engstrand Lilja H (2022) Understanding of the transition to adult healthcare services among individuals with VACTERL association in Sweden: A qualitative study. PLoS ONE 17(5):e0269163. 10.1371/journal.pone.0269163 [DOI] [PMC free article] [PubMed]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Data Availability Statement
The datasets generated during and/or analysed during the current study are available from the corresponding author on reasonable request.