

Abstract
Background:
Survival outcomes of children on extracorporeal membrane oxygenation (ECMO) at time of lung transplant (LTx) remain unclear.
Methods:
Pediatric first-time LTx recipients transplanted between January 2000 and December 2020 were identified in the United Network for Organ Sharing Registry to compare post-transplant survival according to ECMO support at time of transplant. For a comprehensive analysis of the data, univariate analysis, multivariable Cox regression, and propensity score matching were performed.
Results:
During the study period, 954 children under 18 years of age underwent LTx with 40 patients on ECMO. We did not identify a post-LTx survival difference between patients receiving ECMO when compared to those that did not. A multivariable Cox regression model (Hazard ratio = 0.83; 95% confidence interval: 0.47, 1.45; p=0.51) did not demonstrate an increased risk for death post-LTx. Lastly, a propensity score matching analysis, retaining 33 ECMO and 33 non-ECMO patients, further confirmed no post-LTx survival difference comparing ECMO to no ECMO cohorts (Hazard ratio = 0.98; 95% confidence interval: 0.48, 2.00; p=0.96).
Conclusions:
In this contemporary cohort of children, the use of ECMO at the time of LTx did not negatively impact post-transplant survival.
Keywords: lung transplant, extracorporeal membrane oxygenation (ECMO) support, post-lung transplant survival, pediatrics
Graphical Abstract

The use of ECMO at the time of pediatric LTx did not negatively impact post-transplant survival.
Introduction
There have been remarkable surgical and medical advancements in pediatric lung transplant (LTx) since the first successful LTx in a pediatric patient in 1987 at the University of Toronto.1–4 As LTx emerges as a life-saving therapy for those with advanced lung diseases, more than 2000 pediatric LTx cases have been reported to the International Society for Heart and Lung Transplantation (ISHLT) Registry according to recent reports.5,6 Despite improved survival for pediatric LTx, a scarcity of donor organs continues to be a problem.1,4–6 Mechanical circulatory support, such as extracorporeal membrane oxygenation (ECMO), is a therapeutic option for patients declining rapidly on the LTx waitlist.7–10 Following initial skepticism, the use of ECMO as a bridge to LTx has been widely accepted in the adult population for worsening respiratory failure as patients await for a suitable donor.7,9,11,12 Major adult LTx centers have implemented ambulatory ECMO protocols that have shown to improve the recipient’s pre-transplant conditioning, thereby improving post-transplant outcomes.7,9,12,13 Studies have shown that use of ECMO as a bridge to LTx does not have any negative effect on short- and mid-term survival among adult recipients.10,12–16
Investigating the use of ECMO as a bridge to LTx in pediatric recipients has been limited by the smaller patient population when compared to adult recipients.17–23 Between 2000 and 2013, only 17 pediatric patients were identified in the United States (US) to be on ECMO as a bridge to LTx.17 Using multi-center data, this study found that ECMO support at time of LTx did not adversely impact post-LTx survival in children receiving ECMO when compared to all other children who underwent LTx in the US. Since then, additional studies have investigated the impact of ECMO use on LTx survival in pediatric recipients.18,19,22 However, in these studies, the patient selection was either limited to teenagers or expanded to include patients over the age of 18 years, who were primarily transplanted at adult hospitals in the US. As overall use of ECMO has increased among pediatric patients, our study aims to investigate the impact of ECMO at the time of a primary LTx among children under 18 years of age in the modern era. We hypothesized that ECMO at the time of LTx does not negatively impact short-term post-LTx survival.
Patients and Methods
Data Collection
This was a retrospective study using registered data from The United Network for Organ Sharing (UNOS) Organ Procurement and Transplantation Network Standard Transplant Analysis and Research (OPTN STAR) database. The study was approved by the Cincinnati Children’s Hospital Medical Center Institutional Review Board. The OPTN STAR database was queried for the first-time pediatric patients younger than 18 who underwent LTx between January 2000 and December 2020. Patients with re-transplantation or multi-organ transplantation, or without transplantation date were excluded. Presence of ECMO support was identified for those who were bridged to LTx. Extracted data variables included demographic characteristics of recipients and donors, creatinine level, total bilirubin level, presence of diabetes on the recipient, underlying diagnosis for transplant listing, ischemic time, length of total hospital stay, and post-transplant survival status.
Statistical Analysis
Descriptive statistics for continuous variables were described using medians with interquartile ranges (IQR) and frequencies with percentages for categorical variables. Chi-square tests and Wilcoxon rank-sum tests were used to test for differences in demographic and clinical characteristics according to ECMO status.
Kaplan–Meier survival curves were generated to compare differences in the time to death or re-transplantation according to patient ECMO status. Follow-up time was calculated from the date of the lung transplant until the date of death, second transplant, or censoring. Patients alive and not undergoing a second transplant were censored at the last date of follow-up. Cox proportional hazards regression with ECMO status was also employed to estimate the hazard ratio (HR) for ECMO at the time of LTx on transplant free survival, as implemented in survival::coxph function in R (version 3.6.1).24 Gender and race of the recipient and donor, diabetes, diagnosis (primary pulmonary hypertension (PPH), cystic fibrosis (CF), interstitial lung disease (ILD), acute respiratory distress syndrome (ARDS)/pneumonia, and other), age at transplant, year of transplant, creatinine, and ischemic time were included as model covariates. Model covariates were derived from the ISHLT reports and relevant patient characteristics with significance to the outcome of our interest. Model assumptions were verified using Schoenfeld residuals.
A propensity score matching method was also used to confirm the estimates obtained from the multivariable Cox model in the sub-sample of patients matched on the propensity to be on ECMO at the time of transplant. The propensity of ECMO at the time of LTx was calculated as a logit function of the covariates included in the multivariable Cox analysis. We matched each ECMO patient with one non-ECMO patient through one-to-one matching without replacement via the nearest neighbor algorithm with the caliper set as 20% of the propensity score standard deviation, as implemented in “MatchIt” R package.25 Cox proportional hazards regression stratified on the matched pairs was then used to estimate the HR for death or second transplant according to ECMO status at the time of LTx. P-values < 0.05 were considered statistically significant. All statistical analyses were performed using the R statistical program (version 3.6.1, https://www.r-project.org/).
Results
Patient Characteristics
There were a total 954 first-time pediatric lung transplant recipients (age <18 years old) between 2000 and 2020 (Table 1). Forty patients (4.2%) required ECMO support as a bridge to LTx. The most common indication for the first-time transplant was CF followed by PPH. ECMO bridge to LTx was most common among children with CF, PPH, and ARDS. Recipient gender (male), presence of diabetes, and body mass index (BMI) were associated with requiring ECMO support. Patients on ECMO support had higher bilirubin levels and a longer hospital stay. The patients above age 12 years old on ECMO support also had the higher lung allocation scores (LAS). Two patients was bridged to LTx on ECMO between 2000 and 2010 (one each in 2000–2008 and 2009–2010) while the remaining thirty-eight patients were bridged to LTx on ECMO since 2011.
Table 1.
Patient characteristics, comparing ECMO to non-ECMO cohorts.
| Variable | Overall, N = 954 | ECMO | p-value | |
|---|---|---|---|---|
| ECMO, N = 40 | Non-ECMO, N = 914 | |||
| Male recipient | 395 (41%) | 8 (20%) | 387 (42%) | 0.01 |
| Male donor | 492 (52%) | 17 (42%) | 475 (52%) | 0.30 |
| Race of recipient | 0.20 | |||
| White | 697 (73%) | 24 (60%) | 673 (74%) | |
| Black | 62 (6.5%) | 4 (10%) | 58 (6.3%) | |
| Others | 195 (20%) | 12 (30%) | 183 (20%) | |
| Race of donor | 0.30 | |||
| White | 545 (57%) | 20 (50%) | 525 (57%) | |
| Black | 195 (20%) | 12 (30%) | 183 (20%) | |
| Others | 214 (22%) | 8 (20%) | 206 (23%) | |
| Diabetes | 187 (20%) | 2 (5.0%) | 185 (20%) | 0.03 |
| Diagnosis | ||||
| PPH | 102 (11%) | 9 (22%) | 93 (10%) | 0.03 |
| CF | 534 (56%) | 9 (22%) | 525 (57%) | <0.01 |
| ILD | 26 (2.7%) | 2 (5.0%) | 24 (2.6%) | 0.70 |
| ARDS/pneumonia | 7 (0.7%) | 6 (15%) | 1 (0.1%) | <0.01 |
| Others | 285 (30%) | 14 (35%) | 271 (30%) | 0.60 |
| Age (year) | 13.0 (8.0, 16.0) | 13.5 (7.0, 16.2) | 13.0 (8.0, 16.0) | 0.50 |
| Body mass index a | 16.7 (14.8, 18.8) | 19.2 (15.7, 22.3) | 16.7 (14.8, 18.8) | <0.01 |
| Creatinine (mg/dL) b | 0.4 (0.3, 0.5) | 0.3 (0.2, 0.5) | 0.4 (0.3, 0.6) | 0.20 |
| Ischemic time (hour) c | 5.5 (4.6, 6.4) | 5.5 (5.1, 6.8) | 5.5 (4.6, 6.4) | 0.20 |
| Bilirubin (mg/dL) d | 0.3 (0.2, 0.6) | 0.6 (0.4, 1.3) | 0.3 (0.2, 0.6) | <0.01 |
| Hospital stay (day) e | 19.0 (13.0, 31.0) | 36.0 (26.0, 47.0) | 19.0 (13.0, 30.0) | <0.01 |
| Transplant year | <0.01 | |||
| 2000–2008 | 432 (45%) | 1 (2.5%) | 431 (47%) | |
| 2009–2010 | 112(12%) | 1 (2.5%) | 111 (12%) | |
| 2011–2020 | 410 (43%) | 38 (95%) | 372 (41%) | |
| LAS scores for age >=12 f | 37.5 (34.9, 46.0) | 88.4 (82.8, 90.4) | 37.1 (34.8, 44.0) | <0.01 |
Categorical variables as n (%) and Continuous variable as median (IQR). Total patients included for analysis;
n=949,
n=875,
n=909,
n=842,
n=939,
n= 441
Kaplan-Meier and multivariable survival analysis
All 954 patients were included in the Kaplan-Meier survival analysis. There was no statistically significant difference in transplant-free survival according to ECMO status (90.0% vs. 84.8%, 76.2% vs. 59.0%, 57.2% vs. 46.0% at 1, 3, and 5 years respectively representing ECMO vs. non-ECMO group, p = 0.25; Figure 1). The numbers of patients at risk on both groups decreased by about 50% between the second and the third post-transplant year. There was a rather sharp decline in the survival curve between the eighth and ninth post-transplant years among ECMO group patients.
Figure 1.
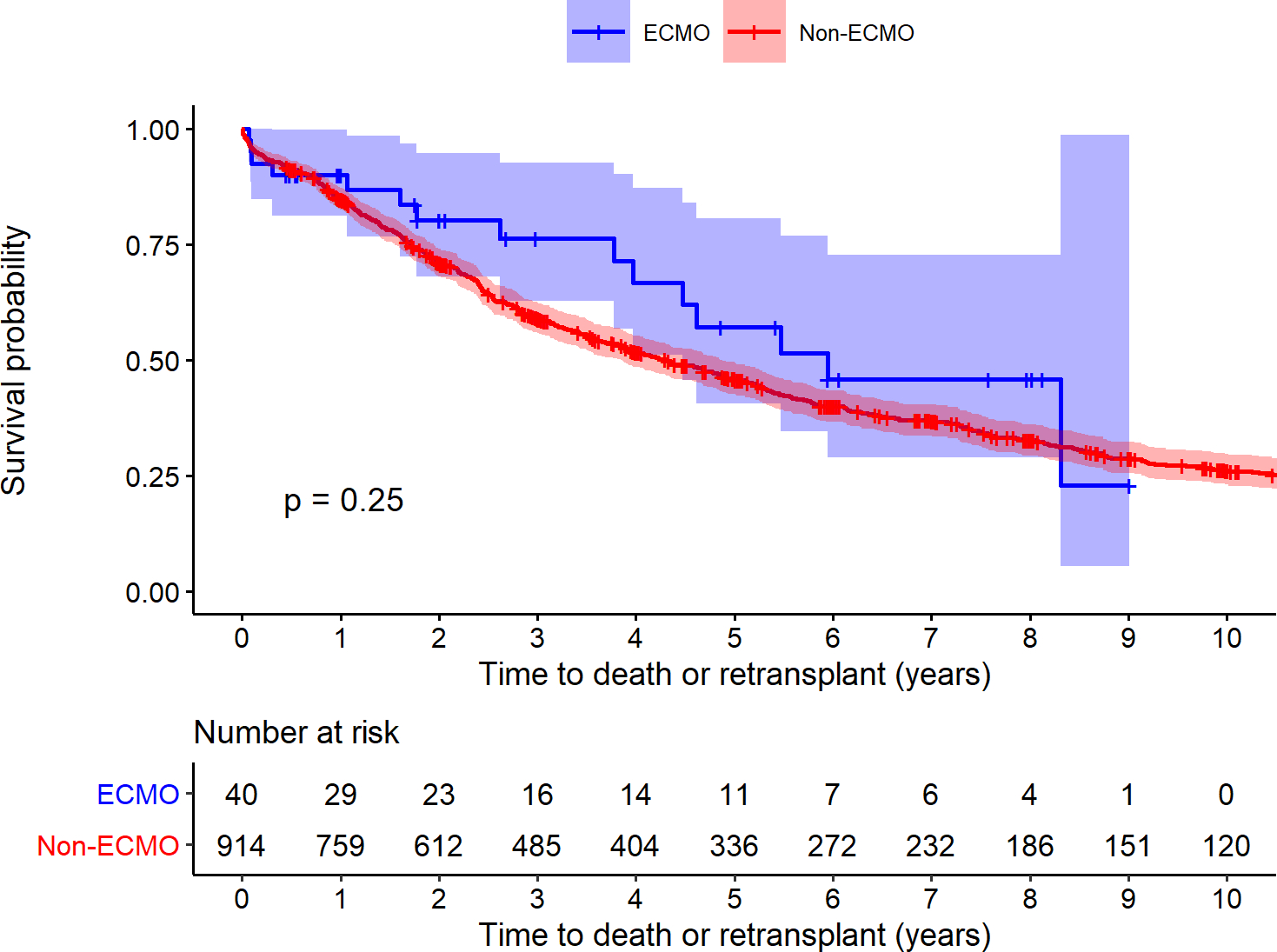
Transplant Free Survival: Kaplan-Meier estimates of survival probability for patients with ECMO (red), and without ECMO (blue). Shaded areas are 95% confidence intervals and log rank p-value= 0.25.
Multi-variable survival analysis using Cox proportional hazards regression showed that being on ECMO as a bridge to LTx was not associated with increased risk of post-transplant mortality or re-transplant (HR=0.83; 95% confidence interval (CI): 0.47, 1.45; p=0.51, Table 2). Risk factors for increased mortality or re-transplant regardless of ECMO support included the recipient’s race (African American vs. White), older age (> 12 years), and the recipient’s creatinine level at the time of listing. Being a male recipient was associated with decreased mortality or re-transplant.
Table 2.
Hazard Ratios (HR) and 95% Confidence Intervals (CI) for death or re-transplant according to risk factors (N = 838*).
| Variable | HR | 95% CI | p-value |
|---|---|---|---|
| ECMO status | |||
| Non-ECMO | Reference | ||
| ECMO | 0.83 | 0.47, 1.45 | 0.51 |
| Male recipient | 0.78 | 0.65, 0.93 | 0.006 |
| Male donor | 0.95 | 0.80, 1.13 | 0.60 |
| Race of recipient | |||
| White | Reference | ||
| Black | 1.81 | 1.28, 2.57 | <0.001 |
| Others | 1.03 | 0.82, 1.28 | 0.80 |
| Diabetes | 0.74 | 0.58, 0.93 | 0.01 |
| Diagnosis | |||
| PPH | Reference | ||
| CF | 1.33 | 0.96, 1.85 | 0.08 |
| ILD | 0.88 | 0.47, 1.63 | 0.70 |
| ARDS/pneumonia | 0.56 | 0.12, 2.55 | 0.50 |
| Others | 1.16 | 0.83, 1.61 | 0.40 |
| Age (year) | |||
| < 1 yr | Reference | ||
| 1 to 5 yrs | 1.52 | 0.96, 2.41 | 0.08 |
| 5 to 12 yrs | 1.06 | 0.71, 1.58 | 0.80 |
| >= 12 yrs | 1.57 | 1.07, 2.32 | 0.02 |
| Transplant year | |||
| 2000–2008 | Reference | ||
| 2009–2020 | 0.83 | 0.69, 0.99 | 0.04 |
| Creatinine (mg/dL) | 1.15 | 1.01, 1.31 | 0.04 |
| Ischemic time (hour) | 1.00 | 0.94, 1.06 | >0.9 |
116 patients were not included in the analysis due to missing covariate data.
Propensity score matching
A total of 66 patients (33 ECMO matched to 33 non-ECMO) were included in the propensity score (PS) matching analysis. All covariates in the multivariable Cox analysis were included in the model for the propensity of receiving ECMO. The PS-matched analysis confirmed that ECMO prior to LTx was not associated with increased risk of death or re-transplant (HR=0.98; 95% CI: 0.48, 2.00; p = 0.96).
Discussion
There has been a steady rise in the number of pediatric LTx in the past twenty years with improved post-transplant survival.1,4–6,8 While organ demand persists, the supply remains scarce, thus leading to a long waiting period in children which is associated with higher waitlist mortality.5,6, 26 The number of LTx recipients under the age of 12 has risen in the past decade, especially for children with ILD or PPH.1,5,6,8 Another patient population often on ECMO who may ultimately require LTx are children with refractory ARDS who have lung injury unamenable to survival without LTx.27 However, donor availability for younger children is even scarcer leading to much longer waitlist times, and each LTx center is confronted with the increasing need to support them to the LTx. ECMO has emerged as a key strategy to manage waitlist mortality, raising awareness to understand the latest trend and impact of ECMO use among pediatric LTx recipients.7,17,21–23
Our current analysis of the UNOS Registry identified 40 children on ECMO between January 2000 and December 2020 who underwent first-time or primary LTx (4.2% of first-time pediatric LTx recipients). This is more than a two-fold increase in the number of ECMO bridge to LTx since 2013 when a previous study reported 17 patients bridged to LTx on ECMO between 2000 and 2013, indicating that more pediatric centers are using ECMO as a bridge therapy to LTx.17 With the findings of the current study, the frequency of ECMO as a bridge to LTx in children is now approaching the reported frequency of 5–7% ECMO bridge among adult LTx recipients.9,10,12,28 Our analysis shows that a majority of ECMO use in children occurred after 2009, the year of the H1N1 pandemic (1 ECMO vs 39 ECMO before and after 2009) (Table 1). The number of children with ARDS was comparable to the number of patients with CF or PPH requiring ECMO as a bridge to LTx although ARDS diagnosis itself represents a small portion of LTx indication in our cohort.
The current study demonstrates that ECMO at the time of LTx did not negatively impact children. Patients bridged on ECMO to LTx had higher bilirubin levels and longer hospital stay compared to those who were not. We hypothesize that hemolysis which often occurs with ECMO support may be a contributing factor to this finding. A bilirubin level greater than 3 mg/dL, while on ECMO, was shown to have negative impact on post-transplant survival among adult patients although exact underlying etiology unclear.9 The median level in our cohort was 1.6 mg/dL, which was mildly elevated compared to the upper normal bilirubin level (1 mg/dL for those under 18 years of age), thereby not significantly affecting post-LTx survival. The total hospital stay for patients on ECMO was longer as expected given their critical illness leading to ECMO support, but this difference of length of stay did not impact post-transplant survival, which is similar to findings among adult recipients.9,10,13 There has been mixed reports on the duration of ECMO support with a few studies using a small cohort of adult recipients in early 2010’s indicating that the total duration of ECMO support, rather than total duration of hospital stay, has significant negative impact on post-transplant survival.9,10,13 The total duration of ECMO support prior to LTx is not available in the registry, thereby limiting more detailed analysis. Risk factors for post-transplant mortality and re-transplantation included older age and renal dysfunction at the time of listing regardless of ECMO status, which has been reported in other studies examining all pediatric LTx recipients.5,6 Older age and renal dysfunction are well-known risk factors associated increased morality among adult LTx recipients.29 The recipient’s race (African-American) was associated with a higher risk of mortality and re-transplantation in our analysis. Racial disparities in solid-organ transplant outcomes continue to exist; although, recent studies suggest some improvement in modern era.30–33 African-American recipients have been shown to have worse outcome following heart transplant in both pediatric and adult population.34,35 Further investigation is needed to explore the underlying causes (i.e., socioeconomic) manifesting the observed relationship between race and post-transplant survival in pediatric LTx recipients. Being a male recipient was associated with decreased mortality risk, which was similar to previous studies assessing all pediatric LTx recipients.5
ECMO has emerged as a key strategy to manage long wait-time, especially to LTx candidates who are severely or critically ill, and has been widely accepted as a bridge to LTx in adult population. Based on the results of the current study, ECMO as a means of support at LTx is expanding into pediatric population. Notably, there has also been remarkable technological and medical advances in ECMO circuit design, protocols, and management that have improved the efficacy and outcome associated with ECMO utilization, especially in the setting of prolonged use.7,9,36 Risk factors related to ECMO support remain with children having and include higher risk of bleeding, neurological accident, infection, and multi-organ dysfunction.7
Veno-venous (VV) ECMO has emerged as the preferred mode of support as a bridge to LTx given fewer associated complications compared to veno-arterial (VA) ECMO. Previous studies support VV ECMO as a bridge to LTx with comparable short- and mid-term post-transplant survival in adult patients. However, VV ECMO is applicable to those with respiratory failure only.7,9,10,13,15 Patients with cardiac dysfunction or severe pulmonary hypertension and associated right ventricular dysfunction often require VA ECMO as VV ECMO lacks sufficient support. VA ECMO can be cannulated peripherally or centrally. Central VA ECMO (cannulation of the right atrium and aorta) can provide higher flow but has a higher risk of bleeding.7,13 Peripheral VA cannulation mostly is done via neck (the right internal jugular vein and carotid artery).7, 13 There is emerging evidence that VA ECMO bridge to LTx can lead to a similar short-term survival outcome compared to the VV ECMO or no-ECMO group among adult population.10,16 An important limitation to our analysis as we cannot discern differences between VA ECMO and VV ECMO bridge to LTx among our study cohorts as the UNOS database does not provide ECMO modality information. Future research needs to assess how the ECMO configuration influences outcomes in pediatric LTx.
VV ECMO via right internal jugular vein with a bicaval dual-lumen catheter is the typically preferred approach that allows for maximal rehabilitation and ambulation as an awake ECMO modality.9,12,36 Impaired functional status or increased length of immobilization even on ECMO has clearly shown to lead to poorer post-transplant outcomes.1,8,37 A strategy for awake ECMO is to enable liberation from mechanical ventilation and to facilitate weaning from sedation leading to early mobilization and rehabilitation.37–39 If patients cannot be liberated from mechanical ventilation while on VV ECMO, early tracheostomy should be performed to maximize the benefits of awake EMCO.38–40 Evidence for benefits of awake ECMO on post-transplant survival and outcomes has been mounting in both adult and pediatric patients.12,20,21,23,37 In our center alone, awake VV ECMO has been utilized in 4 patients under the age of 12 years in the past 2 years. Two patients with progression of underlying ILD were successfully bridged with VV ECMO (10 month-old requiring a 4-month run and 16 year-old requiring a 1-month run). The other two patients were bridged to native lung recovery with liberation from paralytics and sedation and optimization of rehabilitation nutrition after 2 months of VV ECMO. ECMO use in this type of setting involves extensive collaboration among multi-disciplinary teams to optimize its success while also meticulously selecting patients suitable for ECMO bridge to LTx or recovery for that matter. During the study period, we identified that 49 children on ECMO in the UNOS registry did not undergo LTx while 40 children on ECMO had LTx (45% of children on ECMO). More than half of those patients who did not receive LTx died or were removed from the waitlist due to worsening status while about 10% achieved lung recovery.
The current study has several limitations including the retrospective nature of data collection and the available small sample size of pediatric patients on ECMO at time of LTx. Additional challenges are incomplete data entry, potential data entry errors, and confounders that were not collected in the dataset. We cannot determine center-specific factors that may influence outcomes for this high risk pediatric population. Moreover, the database does not provide some key information such as ECMO configuration (VA vs VV) or duration of ECMO support. Additionally, propensity score matching resulted in the exclusion of >90% of the non-ECMO cohort, resulting in inference specific to the patients comprising the matched cohort and potentially limiting generalizability. However, despite the reduction in precision, the results were generally indistinguishable from those obtained using our outcome regression analysis. Our study was multi-institutional, drawing from the largest registry of pediatric LTx recipients currently available, reducing potential biases observed in single-institution observational studies. Long-term survival is an important outcome measure that also needs to be followed.
Our study highlights that the pediatric patients on ECMO at the time of LTx have similar post-transplant survival compared to those children not on ECMO. As the demand for pediatric LTx continues to increase, these findings shed further insights on how we can effectively utilize ECMO for patients on the LTx waitlist to achieve maximal chance for survival during the waiting period as well as post-transplant period. With these results and from our own experience, we believe any child with single-organ lung failure on ECMO regardless of the underlying cause should be at least considered for LTx and be excluded as a candidate accordingly. Our future work is to investigate longer-term effects of ECMO so that enhancements in technology and clinical experiences provide better support for children requiring LTx.
Financial or funding support:
NIH National Heart, Lung, and Blood Institute R01HL142210 (AZ) and R01HL151588 (AZ)
Abbreviations List:
- ARDS
acute respiratory distress syndrome
- BMI
body mass index
- CF
cystic fibrosis
- CI
confidence interval
- ECMO
extracorporeal membrane oxygenation
- HR
hazard ratio
- ILD
interstitial lung disease
- ISHLT
International Society for Heart and Lung Transplantation
- LAS
lung allocation scores
- LTx
lung transplantation
- OPTN STAR
Organ Procurement and Transplantation Network Standard Transplant Analysis and Research
- PPH
primary pulmonary hypertension
- UNOS
United Network for Organ Sharing
- VA
venous-arterial
- VV
veno-venous
Footnotes
Conflicts of interest:
The authors report no conflicts of interest and have no relevant disclosures regarding this manuscript.
Data statement:
The data that support the findings of this study are available from the corresponding author upon reasonable request.
References
- 1.Benden C Pediatric lung transplantation. J Thorac Dis. 2017;9(8):2675–2683. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Grossman RF, Frost A, Zamel N, et al. Results of single-lung transplantation for bilateral pulmonary fibrosis. The Toronto Lung Transplant Group. N Engl J Med. 1990;322(11):727–733. [DOI] [PubMed] [Google Scholar]
- 3.Lancaster TS, Eghtesady P. State of the Art in Pediatric Lung Transplantation. Semin Thorac Cardiovasc Surg. 2018;30(2):166–174. [DOI] [PubMed] [Google Scholar]
- 4.Sweet SC. Pediatric lung transplantation. Proc Am Thorac Soc. 2009;6(1):122–127. [DOI] [PubMed] [Google Scholar]
- 5.Hayes D Jr., Cherikh WS, Chambers DC, et al. The International Thoracic Organ Transplant Registry of the International Society for Heart and Lung Transplantation: 22nd pediatric lung and heart-lung transplantation report-2019; Focus theme: Donor and recipient size match. J Heart Lung Transplant. 2019;38(10):1015–1027. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Hayes D Jr., Harhay MO, Cherikh WS, et al. The International Thoracic Organ Transplant Registry of the International Society for Heart and Lung Transplantation: 24th pediatric lung transplantation report - 2021; Focus on recipient characteristics. J Heart Lung Transplant. 2021;40(10):1023–1034. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Faccioli E, Terzi S, Pangoni A, et al. Extracorporeal membrane oxygenation in lung transplantation: Indications, techniques and results. World J Transplant. 2021;11(7):290–302. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Kirkby S, Hayes D, Jr. Pediatric lung transplantation: indications and outcomes. J Thorac Dis. 2014;6(8):1024–1031. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Loor G, Simpson L, Parulekar A. Bridging to lung transplantation with extracorporeal circulatory support: when or when not? J Thorac Dis. 2017;9(9):3352–3361. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Nasir BS, Klapper J, Hartwig M. Lung Transplant from ECMO: Current Results and Predictors of Post-transplant Mortality. Curr Transplant Rep. 2021;8(2):140–150. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Mason DP, Thuita L, Nowicki ER, Murthy SC, Pettersson GB, Blackstone EH. Should lung transplantation be performed for patients on mechanical respiratory support? The US experience. J Thorac Cardiovasc Surg. 2010;139(3):765–773 e761. [DOI] [PubMed] [Google Scholar]
- 12.Fuehner T, Kuehn C, Hadem J, et al. Extracorporeal membrane oxygenation in awake patients as bridge to lung transplantation. Am J Respir Crit Care Med. 2012;185(7):763–768. [DOI] [PubMed] [Google Scholar]
- 13.Rajagopal K, Hoeper MM. State of the Art: Bridging to lung transplantation using artificial organ support technologies. J Heart Lung Transplant. 2016;35(12):1385–1398. [DOI] [PubMed] [Google Scholar]
- 14.Sef D, Verzelloni Sef A, Trkulja V, et al. Midterm outcomes of venovenous extracorporeal membrane oxygenation as a bridge to lung transplantation: Comparison with nonbridged recipients. J Card Surg. 2022;37(4):747–759. [DOI] [PubMed] [Google Scholar]
- 15.Toyoda Y, Bhama JK, Shigemura N, et al. Efficacy of extracorporeal membrane oxygenation as a bridge to lung transplantation. J Thorac Cardiovasc Surg. 2013;145(4):1065–1071. [DOI] [PubMed] [Google Scholar]
- 16.Xia Y, Ragalie W, Yang EH, et al. Venoarterial Versus Venovenous Extracorporeal Membrane Oxygenation As Bridge to Lung Transplantation. Ann Thorac Surg. 2021. [DOI] [PubMed] [Google Scholar]
- 17.Hayes D Jr., McConnell PI, Tobias JD, et al. Survival in children on extracorporeal membrane oxygenation at the time of lung transplantation. Pediatr Transplant. 2015;19(1):87–93. [DOI] [PubMed] [Google Scholar]
- 18.Sainathan S, Ryan J, Sharma M, Harano T, Morell V, Sanchez P. Outcome of Bridge to Lung Transplantation With Extracorporeal Membrane Oxygenation in Pediatric Patients 12 Years and Older. Ann Thorac Surg. 2021;112(4):1083–1088. [DOI] [PubMed] [Google Scholar]
- 19.Thompson K, Staffa SJ, Nasr VG, et al. Mortality after Lung Transplantation for Children Bridged with Extracorporeal Membrane Oxygenation. Ann Am Thorac Soc. 2022;19(3):415–423. [DOI] [PubMed] [Google Scholar]
- 20.Casswell GK, Pilcher DV, Martin RS, et al. Buying time: The use of extracorporeal membrane oxygenation as a bridge to lung transplantation in pediatric patients. Pediatr Transplant. 2013;17(8):E182–188. [DOI] [PubMed] [Google Scholar]
- 21.Schmidt F, Sasse M, Boehne M, et al. Concept of “awake venovenous extracorporeal membrane oxygenation” in pediatric patients awaiting lung transplantation. Pediatr Transplant. 2013;17(3):224–230. [DOI] [PubMed] [Google Scholar]
- 22.Toprak D, Midyat L, Freiberger D, Boyer D, Fynn-Thompson F, Visner G. Outcomes of mechanical support in a pediatric lung transplant center. Pediatr Pulmonol. 2017;52(3):360–366. [DOI] [PubMed] [Google Scholar]
- 23.Turner DA, Rehder KJ, Bonadonna D, et al. Ambulatory ECMO as a bridge to lung transplant in a previously well pediatric patient with ARDS. Pediatrics. 2014;134(2):e583–585. [DOI] [PubMed] [Google Scholar]
- 24.Therneau T A Package for Survival Analysis in R. R package version 3.3–1, https://CRAN.R-project.org/package=survival. 2022. [Google Scholar]
- 25.Ho D IK, King G, Stuart E, Whitworth A. Package ‘MatchIt’. 2018. [Google Scholar]
- 26.Lancaster TS, Miller JR, Epstein DJ, DuPont NC, Sweet SC, Eghtesady P. Improved waitlist and transplant outcomes for pediatric lung transplantation after implementation of the lung allocation score. J Heart Lung Transplant. 2017;36(5):520–528. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Hayes D Jr., Tumin D, Frazier WJ. Children with refractory ARDS. Pediatr Pulmonol. 2017;52(10):1249. [DOI] [PubMed] [Google Scholar]
- 28.Kukreja J, Tsou S, Chen J, et al. Risk Factors and Outcomes of Extracorporeal Membrane Oxygenation as a Bridge to Lung Transplantation. Semin Thorac Cardiovasc Surg. 2020;32(4):772–785. [DOI] [PubMed] [Google Scholar]
- 29.Chambers DC, Perch M, Zuckermann A, et al. The International Thoracic Organ Transplant Registry of the International Society for Heart and Lung Transplantation: Thirty-eighth adult lung transplantation report - 2021; Focus on recipient characteristics. J Heart Lung Transplant. 2021;40(10):1060–1072. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Isaacs RB, Nock SL, Spencer CE, et al. Racial disparities in renal transplant outcomes. Am J Kidney Dis. 1999;34(4):706–712. [DOI] [PubMed] [Google Scholar]
- 31.Liu A, Woodside KJ, Augustine JJ, Sarabu N. Racial disparity in kidney transplant survival relates to late rejection and is independent of steroid withdrawal. Clin Transplant. 2018;32(9):e13381. [DOI] [PubMed] [Google Scholar]
- 32.Liu V, Bhattacharya J, Weill D, Hlatky MA. Persistent racial disparities in survival after heart transplantation. Circulation. 2011;123(15):1642–1649. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.Liu V, Weill D, Bhattacharya J. Racial disparities in survival after lung transplantation. Arch Surg. 2011;146(3):286–293. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34.Mahle WT, Kanter KR, Vincent RN. Disparities in outcome for black patients after pediatric heart transplantation. J Pediatr. 2005;147(6):739–743. [DOI] [PubMed] [Google Scholar]
- 35.Maredia H, Bowring MG, Massie AB, et al. Better Understanding the Disparity Associated With Black Race in Heart Transplant Outcomes: A National Registry Analysis. Circ Heart Fail. 2021;14(2):e006107. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36.Barbaro RP, Paden ML, Guner YS, et al. Pediatric Extracorporeal Life Support Organization Registry International Report 2016. ASAIO J. 2017;63(4):456–463. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37.Rehder KJ, Turner DA, Hartwig MG, et al. Active rehabilitation during extracorporeal membrane oxygenation as a bridge to lung transplantation. Respir Care. 2013;58(8):1291–1298. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 38.Biscotti M, Sonett J, Bacchetta M. ECMO as bridge to lung transplant. Thorac Surg Clin. 2015;25(1):17–25. [DOI] [PubMed] [Google Scholar]
- 39.Haji JY, Mehra S, Doraiswamy P. Awake ECMO and mobilizing patients on ECMO. Indian J Thorac Cardiovasc Surg. 2021;37(Suppl 2):309–318. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 40.DiChiacchio L, Boulos FM, Brigante F, et al. Early tracheostomy after initiation of venovenous ECMO is associated with decreased duration of extracorporeal membrane oxygenation support. Perfusion. 2020;35(6):509–514. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Data Availability Statement
The data that support the findings of this study are available from the corresponding author upon reasonable request.