

Abstract
Clinical trials frequently include multiple end points that mature at different times. The initial report, typically based on the primary end point, may be published when key planned co-primary or secondary analyses are not yet available. Clinical trial updates provide an opportunity to disseminate additional results from studies, published in JCO or elsewhere, for which the primary end point has already been reported.
Two years of adjuvant abemaciclib combined with endocrine therapy (ET) resulted in a significant improvement in invasive disease-free survival (IDFS) and distant relapse-free survival (DRFS) that persisted beyond the 2-year treatment period in patients with hormone receptor–positive, human epidermal growth factor receptor 2–negative, node-positive, high-risk early breast cancer (EBC). Here, we report 5-year efficacy results from a prespecified overall survival (OS) interim analysis. In the intent-to-treat population, with a median follow-up of 54 months, the benefit of abemaciclib was sustained with hazard ratios of 0.680 (95% CI, 0.599 to 0.772) for IDFS and 0.675 (95% CI, 0.588 to 0.774) for DRFS. This persistence of abemaciclib benefit translated to continuous separation of the curves with a deepening in 5-year absolute improvement in IDFS and DRFS rates of 7.6% and 6.7%, respectively, compared with rates of 6% and 5.3% at 4 years and 4.8% and 4.1% at 3 years. With fewer deaths in the abemaciclib plus ET arm compared with the ET-alone arm (208 v 234), statistical significance was not reached for OS. No new safety signals were observed. In conclusion, abemaciclib plus ET continued to reduce the risk of developing invasive and distant disease recurrence beyond the completion of treatment. The increasing absolute improvement at 5 years is consistent with a carryover effect and further supports the use of abemaciclib in patients with high-risk EBC.
INTRODUCTION
Patients with hormone receptor–positive (HR+), human epidermal growth factor receptor 2–negative (HER2–), node-positive early breast cancer (EBC) are at high risk of recurrence (up to 30% at 5 years1) and need intensification of treatment. Two years of adjuvant abemaciclib in combination with endocrine therapy (ET) is an internationally approved standard of care with National Comprehensive Cancer Network category 12 and European Society for Medical Oncology–Magnitude of Clinical Benefit Scale score A3 recommendation for patients with HR+, HER2–, node-positive EBC at high risk of recurrence. With a median follow-up of 42 months, abemaciclib demonstrated a persistent benefit in invasive disease-free survival (IDFS) and distant relapse-free survival (DRFS) beyond the 2-year treatment period, with all patients off treatment. While overall survival (OS) remained immature, the lower number of deaths in the abemaciclib arm compared with the ET arm suggested that a survival signal favoring abemaciclib was emerging.4 Here, we present efficacy results from a prespecified OS interim analysis that provides 5-year estimates of IDFS and DRFS and updated OS evaluation.
METHODS
A total of 5,637 patients in the monarchE phase III global trial were assigned to one of two cohorts. Cohort 1 (n = 5,120 [91%]) included patients with either at least four positive pathologic axillary lymph nodes (pALNs) or one to three pALNs with additional high-risk features of either grade 3 disease or tumor ≥5 cm. Cohort 2 (n = 517 [9%]) included patients with one to three positive pALNs and central Ki-67 ≥ 20%. The intent-to-treat (ITT) population consisted of cohort 1 and cohort 2. Patients were randomly assigned (1:1) to receive at least 5 years of ET with or without abemaciclib for 2 years (treatment period). OS in the ITT population was planned to be tested for statistical significance per the gated strategy. The detailed study design and statistical analyses have been previously reported.4,5 Hazard ratios (HRs) were estimated using the Cox proportional hazard model, and IDFS, DRFS, and OS rates up to 5 years were based on Kaplan-Meier (KM) methods. For subgroups, landmark yearly rates were estimated up to 4 years to ensure the sufficient number of events within subgroups. The study Protocol (online only) and amendments were approved by each ethical and institutional review board in compliance with the Declaration of Helsinki. All patients provided written informed consent.
RESULTS
Patients
Baseline demographics, clinical characteristics, and patient disposition are shown in Appendix Table A1 and Figure A1 (online only). At data cutoff (July 3, 2023), the median follow-up time was 54 months (IQR, 49-59).
Efficacy
Efficacy in the ITT Population
With approximately 80% of patients having been followed for at least 4 years (2 years after completion of the treatment period), there is a sustained benefit of adjuvant abemaciclib in reducing the risk of developing an IDFS event (HR, 0.680 [95% CI, 0.599 to 0.772]; nominal P < .001). The IDFS KM curves continue to separate, and the absolute improvement in IDFS rates further deepened at 5 years (7.6%) compared with 6%, 4.8%, and 2.8% at 4, 3, and 2 years, respectively (Fig 1A). The addition of abemaciclib to ET also resulted in an improvement in DRFS compared with ET alone (HR, 0.675 [95% CI, 0.588 to 0.774]; nominal P < .001; Fig 1B). At 5 years, the absolute benefit in DRFS rates increased to 6.7% compared with 5.3%, 4.1%, and 2.5% at 4, 3, and 2 years, respectively. The IDFS and DRFS benefit was consistent across all subgroups (Fig 2 and Appendix Fig A2).
FIG 1.
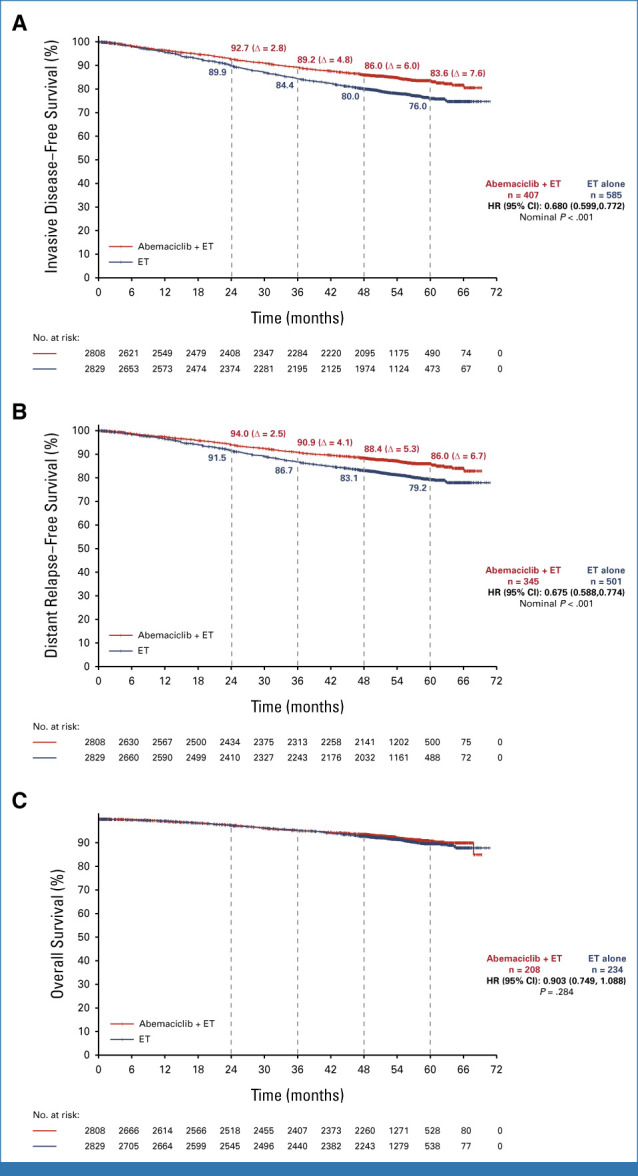
Kaplan-Meier survival curves of (A) IDFS, (B) DRFS, and (C) OS in the intent-to-treat population. The absolute difference might slightly differ from the subtraction between estimated rates because of rounding. DRFS, distant relapse-free survival; ET, endocrine therapy; HR, hazard ratio; IDFS, invasive disease-free survival; OS, overall survival.
FIG 2.

Forest plot of subgroup analyses. Invasive disease-free survival in the ITT prespecified subgroups. ECOG PS, Eastern Cooperative Oncology Group performance status; ET, endocrine therapy; IDFS, invasive disease-free survival; ITT, intention-to-treat; IWRS, Interactive-voice Web Response System.
At the time of the interim analysis, 208 deaths (7.4%) had occurred in the abemaciclib plus ET arm versus 234 deaths (8.3%) in the ET-alone arm. The large majority of patients were alive in the study follow-up (84% in the abemaciclib plus ET arm compared with 81.4% in the ET-alone arm), and a similar proportion of patients withdrew from the study or were lost to follow-up (8.6% in the abemaciclib plus ET arm compared with 10.3% in the ET-alone arm). While fewer deaths were noted in the abemaciclib plus ET arm compared with the ET-alone arm, the difference in OS did not reach statistical significance (HR, 0.903 [95% CI, 0.749 to 1.088]; P = .284; Fig 1C). In addition to patients who had already died of metastatic disease, 269 patients in the ET-alone arm were living with metastatic disease compared with 138 in the abemaciclib plus ET arm (Appendix Fig A3).
Efficacy in Subpopulations
In cohort 1, IDFS, DRFS, and OS were consistent with the ITT population (Appendix Fig A4). Higher IDFS and DRFS event rates were observed in patients with Ki-67 ≥ 20% tumors, but treatment benefit was consistent across Ki-67 subgroups (Table 1 and Appendix Fig A5). Although OS data in ITT are still immature, patients with Ki-67 ≥ 20% tumors have the highest OS event rates and fewer deaths were noted in the abemaciclib plus ET arm compared with the ET-alone arm. Efficacy data in cohort 2 data remain immature at the time of the analysis (Table 1).
TABLE 1.
Summary of Efficacy Results
| Efficacy Result | ITT | Cohort 1 | Cohort 1 Ki-67–High | Cohort 1 Ki-67–Low | Cohort 2 | ||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Abemaciclib + ET (n = 2,808) | ET (n = 2,829) | Abemaciclib + ET (n = 2,555) | ET (n = 2,565) | Abemaciclib + ET (n = 1,017) | ET (n = 986) | Abemaciclib + ET (n = 946) | ET (n = 968) | Abemaciclib + ET (n = 253) | ET (n = 264) | ||
| IDFS | |||||||||||
| No. of events, No. | 407 | 585 | 382 | 553 | 176 | 251 | 116 | 171 | 25 | 32 | |
| Five-year event rate, % (95% CI) | 83.6 (82 to 85.1) | 76 (74.1 to 77.8) | 83.2 (81.5 to 84.7) | 75.3 (73.4 to 77.2) | 81 (78.1 to 83.4) | 72 (68.7 to 75) | 86.3 (83.6 to 88.6) | 80.2 (77.2 to 82.9) | — | — | |
| HR (95% CI) | 0.680 (0.599 to 0.772) | 0.670 (0.588 to 0.764) | 0.643 (0.530 to 0.781) | 0.662 (0.522 to 0.839) | 0.827 (0.484 to 1.414) | ||||||
| Nominal P | <.001 | <.001 | <.001 | <.001 | .488 | ||||||
| DRFS | |||||||||||
| No. of events, No. | 345 | 501 | 325 | 477 | 152 | 221 | 96 | 143 | 20 | 24 | |
| Five-year event rate, % (95% CI) | 86 (84.5 to 87.4) | 79.2 (77.4 to 80.9) | 85.6 (84 to 87.1) | 78.5 (76.6 to 80.3) | 83.4 (80.7 to 85.8) | 75.2 (72.1 to 78) | 88.6 (86.1 to 90.7) | 83.5 (80.7 to 86) | — | — | |
| HR (95% CI) | 0.675 (0.588 to 0.774) | 0.665 (0.577 to 0.765) | 0.634 (0.515 to 0.781) | 0.664 (0.512 to 0.861) | 0.892 (0.485 to 1.643) | ||||||
| Nominal P | <.001 | <.001 | <.001 | .002 | .714 | ||||||
| OS (immature) | |||||||||||
| No. of events, No. | 208 | 234 | 197 | 223 | 92 | 121 | 56 | 62 | 11 | 11 | |
| HR (95% CI) | 0.903 (0.749 to 1.088) | 0.894 (0.738 to 1.084) | 0.717 (0.546 to 0.941) | 0.911 (0.633 to 1.309) | 1.078 (0.465 to 2.501) | ||||||
| Nominal P | .284 | .254 | .016 | .613 | .861 | ||||||
NOTE. Bold numbers highlight key findings.
Abbreviations: DRFS, distant relapse-free survival; ET, endocrine therapy; HR, hazard ratio; IDFS, invasive disease-free survival; ITT, intention-to-treat; OS, overall survival.
Safety
No new safety concerns were identified. Serious adverse events regardless of causality continue to be reported for all patients who entered the long-term follow-up period, with higher rates observed in the ET-alone arm (7.3%) compared with abemaciclib plus ET (6.5%) in the long-term follow-up, predominantly because of more infections and GI disorders in the ET-alone arm.
DISCUSSION
The addition of abemaciclib to standard-of-care ET in the adjuvant treatment of HR+, HER2–, high-risk EBC provided a persistent IDFS and DRFS benefit, with deepening of the absolute benefit in IDFS and DRFS rates at 5 years compared with that at previous years. These observations are consistent with a carryover effect of adjuvant abemaciclib beyond the 2-year treatment duration, which has been previously observed in EBC with adjuvant ET alone.6 Overall, these 5-year data indicate that adjuvant abemaciclib substantially affects patient outcomes as the addition of abemaciclib prevents one recurrence event for every 13 patients treated, mostly incurable metastatic recurrences.
Five-year data are an important landmark for the assessment of efficacy outcomes in HR+, HER2– EBC adjuvant trials (ATAC, 20057; BIG 1-98, 20058) and are especially relevant for a high-risk patient population. Several meta-analyses have shown that approximately one in six women with HR+, HER2– EBC experience recurrence within the first 5 years of starting ET, peaking at 1-3 years.9,10 With nearly one in four patients having recurred at 5 years in the ET-alone arm, the current results from monarchE further demonstrate that the enrolled patients are at very high risk of recurrence, highlighting the need for improved adjuvant endocrine-based therapy. In addition, the outcomes for the control arm of monarchE are consistent with those recently published by the GEICAM group for a cohort of 2,552 patients meeting monarchE eligibility criteria where 25% experienced an IDFS event at 5 years.10 Notably, this number increased to 43% at 10 years, demonstrating the prolonged risk of recurrence in this high-risk population.
Previous studies in adjuvant treatment of HR+ breast cancer have shown that a survival signal could emerge after 10 or more years of follow-up (SOFT/TEXT,11 EBCTCG meta-analysis6). In this analysis of monarchE, statistical significance was not reached for OS; however, a numerical difference in favor of abemaciclib was observed. The study continues until final OS with the majority of patients in active follow-up. With low and well-balanced permanent dropout rates across arms indicating no informative censoring, the assessment of OS is robust and reliable. Of note, in the cohort 1 Ki-67–high subgroup, a population with a worse prognosis and the highest OS event rate, the difference in OS is most pronounced. These data, along with the DRFS results in the ITT population and the substantially lower number of patients living with metastatic disease in the abemaciclib plus ET arm, provide potential insights into how OS data in the ITT population are likely to mature with additional follow-up.
Efficacy analyses by subgroups have confirmed consistent abemaciclib benefit regardless of demographics, disease characteristics, and choice of adjuvant ET (tamoxifen or aromatase inhibitors). Of note, consistent with the data previously reported, patients with one to three lymph nodes and additional risk features like poor grade or tumor size were at a high risk of recurrence, comparable with those of patients with four to nine positive nodes.10 Importantly, the benefit of abemaciclib was consistent regardless of the number of nodes involved.
These 5-year outcomes demonstrate strength in the maturity of the monarchE data and provide further assurance of benefit beyond the 2-year treatment period, which is important given two negative trials for the CDK4/6 inhibitor, palbociclib, in HR+, HER2– EBC.12,13 Interim data from a study exploring the addition of 3 years of ribociclib to ET in the adjuvant setting have reported a statistically significant improvement in IDFS14; however, at the time of the interim analysis, most patients (78%)14 remained on study treatment and additional follow-up is needed to determine if this benefit persists beyond the 3-year treatment duration.
There were no new safety findings in the long-term follow-up with no cumulative or persistent symptoms observed after treatment completion. Overall, patient-reported outcome findings confirm that adjuvant abemaciclib has a tolerable safety profile15 with symptoms that are reversible and can be managed by dose reductions without compromising efficacy.16
In conclusion, at the pivotal 5-year mark for adjuvant EBC trials, adjuvant abemaciclib plus ET continued to reduce the risk of developing invasive and distant disease recurrence well beyond the completion of treatment. The deepened absolute improvement at 5 years is consistent with a carryover effect and further supports the use of abemaciclib in patients with high-risk EBC. OS did not reach statistical significance; however, the lower number of deaths in the abemaciclib arm compared with the ET arm suggests that a survival signal favoring abemaciclib may be emerging.
ACKNOWLEDGMENT
The authors thank patients and their families as well as the investigators and their support staff for participating in this trial. Finally, the authors are grateful for the time and efforts of the monarchE Executive and Steering Committees. All writing, editorial assistance, and statistical analysis were funded by Eli Lilly and Company. Medical writing and editorial support were provided by Monique Mendonca, an employee of Eli Lilly.
APPENDIX
TABLE A1.
Patient Demographics and Baseline Characteristics in the Intention-to-Treat Population
| Demographic and Characteristic | Abemaciclib + ET (n = 2,808)a | ET Alone (n = 2,829)a |
|---|---|---|
| Sex, No. (%) | ||
| Female | 2,787 (99) | 2,814 (99) |
| Male | 21 (1) | 15 (1) |
| Age, years, median (IQR) | 51 (44-60) | 51 (44-60) |
| Race, No. (%) | ||
| White | 1,947 (69) | 1,978 (70) |
| Asian | 675 (24) | 669 (24) |
| All others | 146 (5) | 140 (5) |
| Menopausal status, No. (%)b,c | ||
| Premenopausal | 1,221 (43) | 1,232 (44) |
| Postmenopausal | 1,587 (57) | 1,597 (56) |
| Hormone receptor status, No. (%) | ||
| Estrogen receptor–positive | 2,786 (99) | 2,810 (99) |
| Progesterone receptor–positive | 2,426 (86) | 2,456 (87) |
| Previous adjuvant ET, No. (%) | ||
| Yes | 1,764 (63) | 1,795 (63) |
| No | 1,044 (37) | 1,034 (37) |
| Previous (neo) adjuvant chemotherapies, No. (%) | ||
| Yes | 2,656 (95) | 2,664 (94) |
| No | 152 (5) | 165 (6) |
| Tumor, node, metastasis stages, No. (%)d | ||
| IIA | 324 (12) | 353 (12) |
| IIB | 392 (14) | 387 (14) |
| IIIA | 1,029 (37) | 1,026 (36) |
| IIIC | 950 (34) | 963 (34) |
| Positive axillary lymph nodes, No. (%) | ||
| 1-3 | 1,118 (40) | 1,142 (40) |
| 4-9 | 1,107 (39) | 1,126 (40) |
| ≥10 | 575 (20) | 554 (20) |
| Pathologic tumor size, cm, No. (%) | ||
| <2 | 781 (28) | 767 (27) |
| 2-4 | 1,372 (49) | 1,419 (50) |
| ≥5 | 607 (22) | 610 (22) |
| Histopathologic grade at diagnosis, No. (%) | ||
| Grade 1 | 209 (7) | 216 (8) |
| Grade 2 | 1,377 (49) | 1,395 (49) |
| Grade 3 | 1,086 (39) | 1,064 (38) |
| Ki-67 index, No. (%) | ||
| <20% | 953 (34) | 974 (34) |
| ≥20% | 1,262 (45) | 1,233 (44) |
Abbreviation: ET, endocrine therapy.
Where values do not add up to 100%, remaining data are missing, are unavailable, or could not be assessed.
Per the interactive web response system.
cMenopausal status is at the time of diagnosis, and all male patients are considered postmenopausal.
Derived on the basis of the pathologic tumor size and number of positive lymph nodes after primary surgery.
FIG A1.
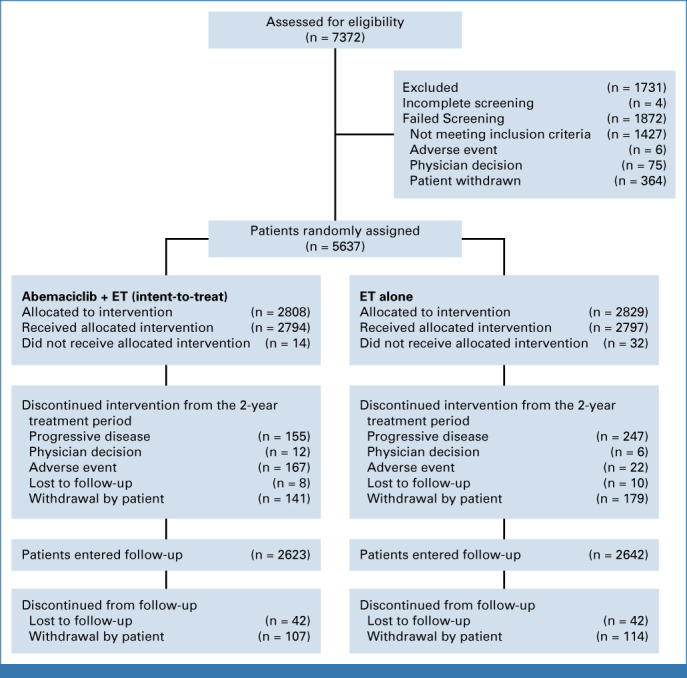
CONSORT diagram. ET, endocrine therapy.
FIG A2.

Forest plot of subgroup analyses. Distant relapse-free survival in the ITT prespecified subgroups. DRFS, distant relapse-free survival; ECOG PS, Eastern Cooperative Oncology Group performance status; ET, endocrine therapy; ITT, intention-to-treat; IWRS, Interactive-voice Web Response System.
FIG A3.

Bar plot of survival status over time. Patients in the ITT population who died or had distant metastases. ET, endocrine therapy; IA, interim analysis; ITT, intention-to-treat; OS, overall survival.
FIG A4.
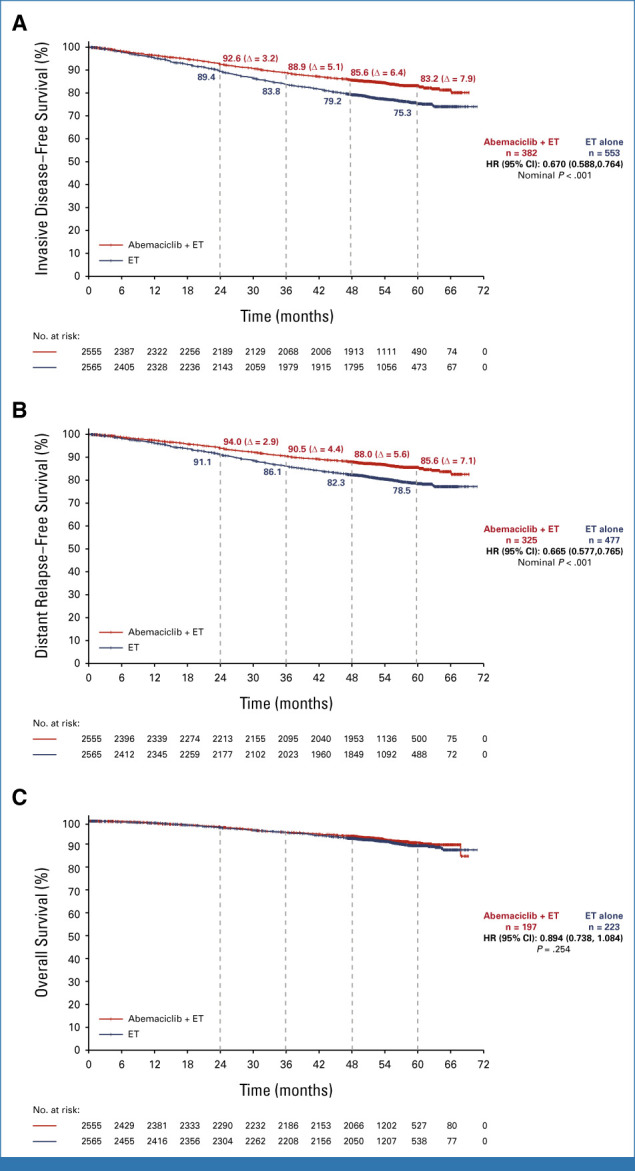
Kaplan-Meier survival curves of (A) IDFS, (B) DRFS, and (C) OS in cohort 1. The absolute difference might slightly differ from the subtraction between estimated rates because of rounding. DRFS, distant relapse-free survival; HR, hazard ratio; IDFS, invasive disease-free survival; OS, overall survival.
FIG A5.
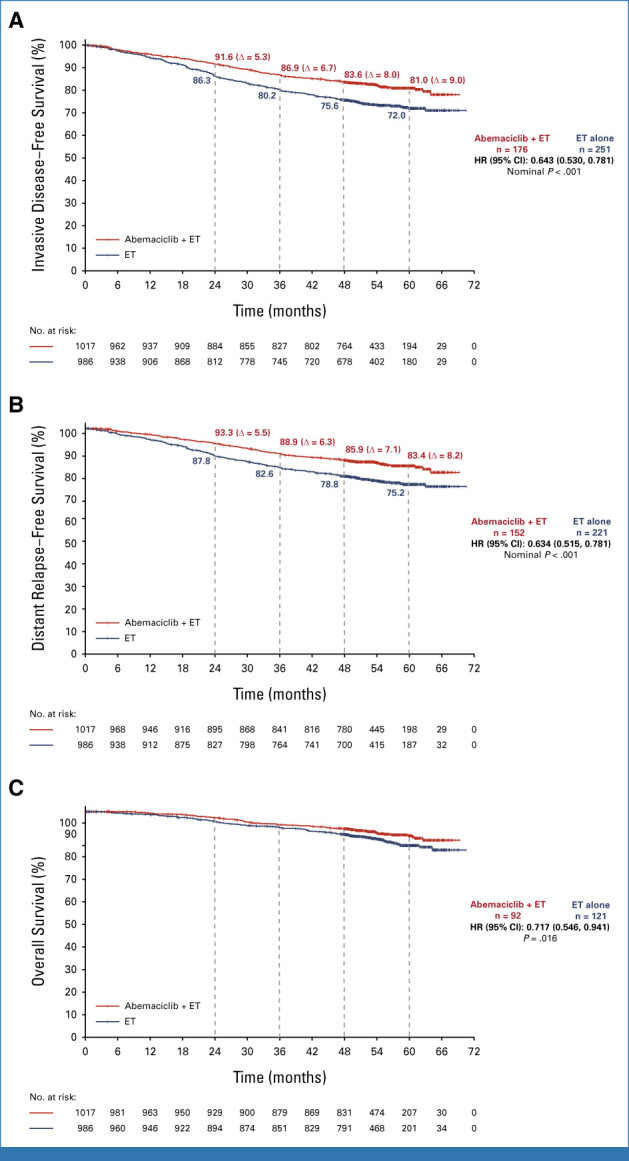
Kaplan-Meier survival curves of (A) IDFS, (B) DRFS, and (C) OS in cohort 1 Ki-67–high subpopulation. The absolute difference might slightly differ from the subtraction between estimated rates because of rounding. DRFS, distant relapse-free survival; HR, hazard ratio; IDFS, invasive disease-free survival; OS, overall survival.
Priya Rastogi
Travel, Accommodations, Expenses: Genentech/Roche, Lilly, AstraZeneca
Joyce O'Shaughnessy
Honoraria: AstraZeneca, Lilly, AbbVie, Celgene, Eisai, Novartis, Pfizer, Agendia, Amgen, Bristol Myers Squibb, Genentech, GRAIL, Immunomedics, HERON, Ipsen, Merck, Myriad Pharmaceuticals, Puma Biotechnology, Roche, Syndax, Sanofi, Samsung, Daiichi Sankyo, Aptitude Health, Bayer, G1 Therapeutics, Gilead Sciences, Halozyme, Nektar, Pharmacyclics, Pierre Fabre, Prime Oncology, Seagen, Taiho Oncology, Takeda, Synthon, Ontada/McKesson
Consulting or Advisory Role: Novartis, Pfizer, Lilly, AbbVie, AstraZeneca, Celgene, Eisai, Agendia, Amgen, Bristol Myers Squibb, Genentech, GRAIL, Immunomedics, HERON, Ipsen, Merck, Myriad Pharmaceuticals, Puma Biotechnology, Roche, Syndax, Sanofi, Samsung, Daiichi Sankyo, Aptitude Health, Bayer, G1 Therapeutics, Gilead Sciences, Halozyme, Nektar, Pharmacyclics, Pierre Fabre, Prime Oncology, Seagen, Taiho Oncology, Takeda, Synthon, Ontada/McKesson
Speakers' Bureau: AstraZeneca, Novartis, Lilly, Pfizer, Seagen
Research Funding: Seagen (Inst)
Travel, Accommodations, Expenses: Celgene, Lilly, Novartis, Pfizer, AbbVie, Agendia, Amgen, Eisai, GRAIL, Ipsen, Myriad Pharmaceuticals, Puma Biotechnology, Seagen, AstraZeneca, Sanofi, Roche
Miguel Martin
Honoraria: Roche/Genentech, Lilly, Pfizer, Novartis, Pierre Fabre, Seagen
Consulting or Advisory Role: Roche/Genentech, Novartis, Pfizer, Lilly, AstraZeneca, Daiichi-Sankyo
Speakers' Bureau: Lilly/ImClone, Roche/Genentech, Pierre Fabre
Research Funding: Novartis (Inst), Roche (Inst), Puma Biotechnology (Inst)
Travel, Accommodations, Expenses: Daichii-Sankyo
Other Relationship: Roche, Novartis
Frances Boyle
Honoraria: Lilly, Eisai, Roche, Gilead Sciences, AstraZeneca
Consulting or Advisory Role: Roche, Lilly, Novartis, Pfizer, Gilead Sciences
Expert Testimony: Lilly, Gilead Sciences
Travel, Accommodations, Expenses: Novartis
Other Relationship: Paxman, Pamgene
Uncompensated Relationships: Paxman
Javier Cortes
Stock and Other Ownership Interests: Leuko, MAJ3 Capital
Honoraria: Novartis, Eisai, Celgene, Pfizer, Roche, Samsung, Lilly, Merck Sharp & Dohme, Daiichi Sankyo, AstraZeneca, Gilead Sciences, Steamline Therapeutics
Consulting or Advisory Role: Celgene, Cellestia Biotech, AstraZeneca, Roche, Seagen, Daiichi Sankyo, Erytech Pharma, Polyphor, Athenex, Lilly, Servier, Merck Sharp & Dohme, GlaxoSmithKline, Leuko, Clovis Oncology, Bioasis, Boehringer Ingelheim, Ellipses Pharma, HiberCell, Bioinvent, GEMoaB, Gilead Sciences, Menarini, Zymeworks, Reveal Genomics, Expres2ion Biotechnologies, Jazz Pharmaceuticals, AbbVie, Bridgebio
Research Funding: ARIAD (Inst), AstraZeneca (Inst), Baxalta (Inst), Bayer (Inst), Eisai (Inst), Guardant Health (Inst), Merck Sharp & Dohme (Inst), Pfizer (Inst), Puma Biotechnology (Inst), Queen Mary University of London (Inst), Roche (Inst), Piqur (Inst)
Patents, Royalties, Other Intellectual Property: Pharmaceutical Combinations of a Pi3k Inhibitor and a Microtubule Destabilizing Agent. Javier Cortés Castán, Alejandro Piris Giménez, Violeta Serra Elizalde. WO 2014/199294 A. HER2 as a predictor of response to dual HER2 blockade in the absence of cytotoxic therapy. Aleix Prat, Antonio Llombart, Javier Cortés. US 2019/0338368 A1
Travel, Accommodations, Expenses: Roche, Pfizer, Eisai, Novartis, Daiichi Sankyo, Gilead Sciences, AstraZeneca, Merck Sharp & Dohme, Steamline Therapeutics
Hope S. Rugo
Consulting or Advisory Role: Napo Pharmaceuticals, Puma Biotechnology, Mylan, Eisai, Daiichi Sankyo
Research Funding: OBI Pharma (Inst), Pfizer (Inst), Novartis (Inst), Lilly (Inst), Merck (Inst), Daiichi Sankyo (Inst), Sermonix Pharmaceuticals (Inst), AstraZeneca (Inst), Gilead Sciences (Inst), Astellas Pharma (Inst), Pionyr (Inst), Taiho Oncology (Inst), Veru (Inst), GlaxoSmithKline (Inst), Hoffmann-La Roche AG/Genentech, Inc (Inst), Stemline Therapeutics (Inst)
Travel, Accommodations, Expenses: Merck, AstraZeneca, Gilead Sciences, Pfizer
Open Payments Link: https://openpaymentsdata.cms.gov/physician/183398
Matthew P. Goetz
Consulting or Advisory Role: Lilly (Inst), AstraZeneca (Inst), Blueprint Medicines (Inst), Genzyme (Inst), ARC Therapeutics (Inst), BioTheranostics (Inst), RNA Diagnostics (Inst), Seagen (Inst), Engage Health Media (Inst), Novartis (Inst), Sermonix Pharmaceuticals (Inst)
Research Funding: Lilly (Inst), Pfizer (Inst), Sermonix Pharmaceuticals (Inst), Atossa Genetics (Inst), AstraZeneca (Inst), Loxo (Inst)
Patents, Royalties, Other Intellectual Property: Methods and Materials for Assessing Chemotherapy Responsiveness and Treating Cancer, Methods and Materials for Using Butyrylcholinesterase to Treat Cancer, Development of Human Tumor Xenografts From Women With Breast Cancer Treated With Neoadjuvant Chemotherapy (Inst)
Travel, Accommodations, Expenses: Lilly (Inst)
Erika P. Hamilton
Consulting or Advisory Role: Pfizer (Inst), Genentech/Roche (Inst), Lilly (Inst), Daiichi Sankyo (Inst), Mersana (Inst), AstraZeneca (Inst), Novartis (Inst), Seagen (Inst), ITeos Therapeutics (Inst), Janssen (Inst), Loxo (Inst), Relay Therapeutics (Inst), Greenwich LifeSciences (Inst), Orum Therapeutics (Inst), Ellipses Pharma (Inst), Olema Pharmaceuticals (Inst), Stemline Therapeutics (Inst), Tubulis GmbH (Inst), Verascity Science (Inst), Theratechnologies (Inst)
Research Funding: AstraZeneca (Inst), Hutchison MediPharma (Inst), OncoMed (Inst), MedImmune (Inst), Stem CentRx (Inst), Genentech/Roche (Inst), Curis (Inst), Verastem (Inst), Zymeworks (Inst), Syndax (Inst), Lycera (Inst), Rgenix (Inst), Novartis (Inst), Mersana (Inst), Millennium (Inst), TapImmune Inc (Inst), Lilly (Inst), Pfizer (Inst), Tesaro (Inst), Boehringer Ingelheim (Inst), H3 Biomedicine (Inst), Radius Health (Inst), Acerta Pharma (Inst), MacroGenics (Inst), AbbVie (Inst), Immunomedics (Inst), Fujifilm (Inst), eFFECTOR Therapeutics (Inst), Merus (Inst), Nucana (Inst), Regeneron (Inst), Leap Therapeutics (Inst), Taiho Pharmaceutical (Inst), EMD Serono (Inst), Daiichi Sankyo (Inst), ArQule (Inst), Syros Pharmaceuticals (Inst), Clovis Oncology (Inst), CytomX Therapeutics (Inst), InventisBio (Inst), Deciphera (Inst), Sermonix Pharmaceuticals (Inst), Sutro Biopharma (Inst), Zenith Epigenetics (Inst), Arvinas (Inst), Harpoon (Inst), Black Diamond Therapeutics (Inst), Orinove (Inst), Molecular Templates (Inst), Seagen (Inst), Compugen (Inst), G1 Therapeutics (Inst), Karyopharm Therapeutics (Inst), Dana Farber Cancer Hospital (Inst), Onconova Therapeutics (Inst), Shattuck Labs (Inst), PharmaMar (Inst), Olema Pharmaceuticals (Inst), Immunogen (Inst), Plexxikon (Inst), Amgen (Inst), Akeso Biopharma (Inst), ADC Therapeutics (Inst), AtlasMedx (Inst), Aravive (Inst), Ellipses Pharma (Inst), Incyte (Inst), MabSpace Biosciences (Inst), ORIC Pharmaceuticals (Inst), Pieris Pharmaceuticals (Inst), Pionyr (Inst), Repertoire Immune Medicines (Inst), Treadwell Therapeutics (Inst), Jacobio (Inst), Accutar Biotech (Inst), Artios (Inst), Bliss Biopharmaceutical (Inst), Cascadian Therapeutics (Inst), Dantari (Inst), Duality Biologics (Inst), Elucida Oncology (Inst), Infinity Pharmaceuticals (Inst), Relay Therapeutics (Inst), Tolmar (Inst), Torque (Inst), BeiGene (Inst), Context Therapeutics (Inst), K-Group Beta (Inst), Kind Pharmaceuticals (Inst), Loxo (Inst), Oncothyreon (Inst), Orum Therapeutics (Inst), Prelude Therapeutics (Inst), ProfoundBio (Inst), Cullinan Oncology (Inst)
Chiun-Sheng Huang
Honoraria: Roche, Pfizer, Novartis, AstraZeneca, Daiichi Sankyo, Lilly
Consulting or Advisory Role: Pfizer, Roche, Lilly, AstraZeneca, Novartis, Daiichi Sankyo
Speakers' Bureau: Roche, Daiichi Sankyo
Research Funding: AstraZeneca (Inst), Lilly (Inst), MSD (Inst), Novartis (Inst), Pfizer (Inst), Roche (Inst), OBI Pharma (Inst), EirGenix (Inst), Daiichi Sankyo (Inst), Gilead Sciences (Inst), Seagen (Inst)
Travel, Accommodations, Expenses: Pfizer (Inst), Gilead Sciences (Inst)
Elzbieta Senkus
Honoraria: AstraZeneca, Cancérodigest, Curio Science, Egis Pharmaceuticals, Lilly, Exact Sciences/Oecona, Gilead Sciences, High5md, MSD, Novartis, Pfizer, Roche
Consulting or Advisory Role: AstraZeneca, Lilly, Gilead Sciences, Novartis, Pfizer
Travel, Accommodations, Expenses: AstraZeneca, Egis Pharmaceuticals, Gilead Sciences, Novartis
Other Relationship: Amgen, AstraZeneca, Daiichi Sankyo, Lilly, Novartis, OBI Pharma, Pfizer, Roche, Astellas Pharma
Alexey Tryakin
Stock and Other Ownership Interests: Amgen, Lilly, Merck Serono, Merck, Bayer
Consulting or Advisory Role: BioCad, Roche/Genentech, Bristol Myers Squibb, Eisai, Merck Sharp & Dohme, AstraZeneca, Lilly, Amgen
Speakers' Bureau: Bayer Health, BioCad, Lilly, Merck Serono, Sanofi, Amgen, Bristol Myers Squibb, Eisai, Merck Sharp & Dohme, Pfizer, Bayer, AstraZeneca/Daiichi Sankyo, Novartis
Research Funding: Biocad (Inst)
Travel, Accommodations, Expenses: Novartis, BioCad, Bayer, Veropharm, Sanofi, AstraZeneca, Merck Serono
Irfan Cicin
Consulting or Advisory Role: Pfizer (Inst), MSD Oncology (Inst), Roche (Inst), Novartis/Ipsen (Inst), Lilly (Inst), Bristol Myers Squibb (Inst), Servier (Inst), Abdi Ibrahim (Inst), Nobelpharma (Inst), AbbVie (Inst), Teva, Janssen Oncology (Inst), Takeda (Inst), Gen (Inst), Astellas Pharma (Inst), Gilead Sciences (Inst)
Speakers' Bureau: Novartis (Inst), Roche (Inst), Bristol Myers Squibb (Inst), Pfizer (Inst), Abdi Ibrahim (Inst), Astellas Pharma, MSD (Inst), Gen (Inst), Teva (Inst)
Laura Testa
Consulting or Advisory Role: MSD Oncology, Lilly, Daiichi Sankyo/Astra Zeneca, MSD/AstraZeneca, AstraZeneca, Pfizer, Novartis
Speakers' Bureau: Novartis, Pfizer, MSD Oncology, Daiichi Sankyo/Astra Zeneca, Lilly
Research Funding: Novartis (Inst)
Travel, Accommodations, Expenses: Roche, Gilead Sciences, AstraZeneca
Patrick Neven
Consulting or Advisory Role: Lilly (Inst), Pfizer (Inst), Novartis (Inst), Roche (Inst), Radius Health (Inst)
Travel, Accommodations, Expenses: Lilly (Inst), Pfizer (Inst), Roche (Inst)
Jens Huober
Honoraria: Roche, Lilly, Pfizer, MSD Oncology, AstraZeneca, Novartis, Seagen, Daiichi Sankyo/Astra Zeneca, Gilead Sciences
Consulting or Advisory Role: Novartis, Roche, Pfizer, Lilly, AstraZeneca, Daiichi Sankyo/Astra Zeneca, Gilead Sciences
Travel, Accommodations, Expenses: Roche, Pfizer, Daiichi Sankyo, Gilead Sciences
Uncompensated Relationships: German Breast Group
Ran Wei
Employment: Lilly
Stock and Other Ownership Interests: Lilly
Valérie André
Employment: Lilly
Stock and Other Ownership Interests: Lilly
Maria Munoz
Employment: Lilly
Stock and Other Ownership Interests: Lilly
Honoraria: MSD Oncology, AstraZeneca, Debiopharm Group, Pfizer, Janssen, Sanofi, Takeda, BMS Norway, Lilly, Gilead Sciences
Consulting or Advisory Role: Janssen, MSD, AstraZeneca, Lilly, Pfizer, BMS Norway
Research Funding: Roche, AstraZeneca
Belen San Antonio
Employment: Lilly
Stock and Other Ownership Interests: Lilly
Ashwin Shahir
Employment: Lilly
Stock and Other Ownership Interests: Lilly
Nadia Harbeck
Stock and Other Ownership Interests: West German Study Group
Honoraria: Roche, Novartis, Pfizer, AstraZeneca, Pierre Fabre, Daiichi-Sankyo, MSD, Seagen, Lilly, Viatris, Sanofi, Zuelligpharma, Gilead Sciences, Amgen
Consulting or Advisory Role: Novartis, Sandoz, West German Study Group, Seagen, Gilead Sciences, Roche/Genentech
Speakers' Bureau: Medscape, Springer Healthcare, EPG Communication
Research Funding: Roche/Genentech (Inst), Lilly (Inst), MSD (Inst), AstraZeneca (Inst)
Stephen Johnston
Honoraria: Pfizer, AstraZeneca, Lilly
Consulting or Advisory Role: Lilly, Puma Biotechnology, Pfizer, Genzyme
Research Funding: Pfizer (Inst)
Expert Testimony: Novartis
No other potential conflicts of interest were reported.
PRIOR PRESENTATION
Presented in part at the European Society for Medical Oncology Congress, Madrid, Spain, October 20-24, 2023.
SUPPORT
Supported by Eli Lilly and Company.
CLINICAL TRIAL INFORMATION
DATA SHARING STATEMENT
Eli Lilly and Company provides access to all individual participant data collected during the trial, after anonymization, with the exception of pharmacokinetic or genetic data. Data are available to request 6 months after the indication studied has been approved in the United States and European Union and after primary publication acceptance, whichever is later. No expiration date of data requests is currently set once data are made available. Access is provided after a proposal has been approved by an independent review committee identified for this purpose and after receipt of a signed data sharing agreement. Data and documents, including the study protocol, statistical analysis plan, clinical study report, blank or annotated case report forms, will be provided in a secure data sharing environment. For details on submitting a request, see the instructions provided at www.vivli.org.
AUTHOR CONTRIBUTIONS
Conception and design: Priya Rastogi, Miguel Martin, Frances Boyle, Matthew P. Goetz, Valérie André, Ashwin Shahir, Nadia Harbeck, Stephen Johnston
Provision of study materials or patients: Miguel Martin, Frances Boyle, Javier Cortes, Hope S. Rugo, Matthew P. Goetz, Erika P. Hamilton, Chiun-Sheng Huang, Elzbieta Senkus, Alexey Tryakin, Jens Huober, Zhimin Shao, Nadia Harbeck, Stephen Johnston
Collection and assembly of data: Priya Rastogi, Miguel Martin, Frances Boyle, Erika P. Hamilton, Elzbieta Senkus, Alexey Tryakin, Laura Testa, Patrick Neven, Zhimin Shao, Valérie André, Maria Munoz, Nadia Harbeck
Data analysis and interpretation: Priya Rastogi, Miguel Martin, Javier Cortes, Hope S. Rugo, Matthew P. Goetz, Chiun-Sheng Huang, Irfan Cicin, Laura Testa, Patrick Neven, Jens Huober, Zhimin Shao, Ran Wei, Valérie André, Maria Munoz, Belen San Antonio, Ashwin Shahir, Nadia Harbeck, Stephen Johnston
Manuscript writing: All authors
Final approval of manuscript: All authors
Accountable for all aspects of the work: All authors
AUTHORS' DISCLOSURES OF POTENTIAL CONFLICTS OF INTEREST
Adjuvant Abemaciclib Plus Endocrine Therapy for Hormone Receptor–Positive, Human Epidermal Growth Factor Receptor 2–Negative, High-Risk Early Breast Cancer: Results From a Preplanned monarchE Overall Survival Interim Analysis, Including 5-Year Efficacy Outcomes
The following represents disclosure information provided by authors of this manuscript. All relationships are considered compensated unless otherwise noted. Relationships are self-held unless noted. I = Immediate Family Member, Inst = My Institution. Relationships may not relate to the subject matter of this manuscript. For more information about ASCO's conflict of interest policy, please refer to www.asco.org/rwc or ascopubs.org/jco/authors/author-center.
Open Payments is a public database containing information reported by companies about payments made to US-licensed physicians (Open Payments).
Priya Rastogi
Travel, Accommodations, Expenses: Genentech/Roche, Lilly, AstraZeneca
Joyce O'Shaughnessy
Honoraria: AstraZeneca, Lilly, AbbVie, Celgene, Eisai, Novartis, Pfizer, Agendia, Amgen, Bristol Myers Squibb, Genentech, GRAIL, Immunomedics, HERON, Ipsen, Merck, Myriad Pharmaceuticals, Puma Biotechnology, Roche, Syndax, Sanofi, Samsung, Daiichi Sankyo, Aptitude Health, Bayer, G1 Therapeutics, Gilead Sciences, Halozyme, Nektar, Pharmacyclics, Pierre Fabre, Prime Oncology, Seagen, Taiho Oncology, Takeda, Synthon, Ontada/McKesson
Consulting or Advisory Role: Novartis, Pfizer, Lilly, AbbVie, AstraZeneca, Celgene, Eisai, Agendia, Amgen, Bristol Myers Squibb, Genentech, GRAIL, Immunomedics, HERON, Ipsen, Merck, Myriad Pharmaceuticals, Puma Biotechnology, Roche, Syndax, Sanofi, Samsung, Daiichi Sankyo, Aptitude Health, Bayer, G1 Therapeutics, Gilead Sciences, Halozyme, Nektar, Pharmacyclics, Pierre Fabre, Prime Oncology, Seagen, Taiho Oncology, Takeda, Synthon, Ontada/McKesson
Speakers' Bureau: AstraZeneca, Novartis, Lilly, Pfizer, Seagen
Research Funding: Seagen (Inst)
Travel, Accommodations, Expenses: Celgene, Lilly, Novartis, Pfizer, AbbVie, Agendia, Amgen, Eisai, GRAIL, Ipsen, Myriad Pharmaceuticals, Puma Biotechnology, Seagen, AstraZeneca, Sanofi, Roche
Miguel Martin
Honoraria: Roche/Genentech, Lilly, Pfizer, Novartis, Pierre Fabre, Seagen
Consulting or Advisory Role: Roche/Genentech, Novartis, Pfizer, Lilly, AstraZeneca, Daiichi-Sankyo
Speakers' Bureau: Lilly/ImClone, Roche/Genentech, Pierre Fabre
Research Funding: Novartis (Inst), Roche (Inst), Puma Biotechnology (Inst)
Travel, Accommodations, Expenses: Daichii-Sankyo
Other Relationship: Roche, Novartis
Frances Boyle
Honoraria: Lilly, Eisai, Roche, Gilead Sciences, AstraZeneca
Consulting or Advisory Role: Roche, Lilly, Novartis, Pfizer, Gilead Sciences
Expert Testimony: Lilly, Gilead Sciences
Travel, Accommodations, Expenses: Novartis
Other Relationship: Paxman, Pamgene
Uncompensated Relationships: Paxman
Javier Cortes
Stock and Other Ownership Interests: Leuko, MAJ3 Capital
Honoraria: Novartis, Eisai, Celgene, Pfizer, Roche, Samsung, Lilly, Merck Sharp & Dohme, Daiichi Sankyo, AstraZeneca, Gilead Sciences, Steamline Therapeutics
Consulting or Advisory Role: Celgene, Cellestia Biotech, AstraZeneca, Roche, Seagen, Daiichi Sankyo, Erytech Pharma, Polyphor, Athenex, Lilly, Servier, Merck Sharp & Dohme, GlaxoSmithKline, Leuko, Clovis Oncology, Bioasis, Boehringer Ingelheim, Ellipses Pharma, HiberCell, Bioinvent, GEMoaB, Gilead Sciences, Menarini, Zymeworks, Reveal Genomics, Expres2ion Biotechnologies, Jazz Pharmaceuticals, AbbVie, Bridgebio
Research Funding: ARIAD (Inst), AstraZeneca (Inst), Baxalta (Inst), Bayer (Inst), Eisai (Inst), Guardant Health (Inst), Merck Sharp & Dohme (Inst), Pfizer (Inst), Puma Biotechnology (Inst), Queen Mary University of London (Inst), Roche (Inst), Piqur (Inst)
Patents, Royalties, Other Intellectual Property: Pharmaceutical Combinations of a Pi3k Inhibitor and a Microtubule Destabilizing Agent. Javier Cortés Castán, Alejandro Piris Giménez, Violeta Serra Elizalde. WO 2014/199294 A. HER2 as a predictor of response to dual HER2 blockade in the absence of cytotoxic therapy. Aleix Prat, Antonio Llombart, Javier Cortés. US 2019/0338368 A1
Travel, Accommodations, Expenses: Roche, Pfizer, Eisai, Novartis, Daiichi Sankyo, Gilead Sciences, AstraZeneca, Merck Sharp & Dohme, Steamline Therapeutics
Hope S. Rugo
Consulting or Advisory Role: Napo Pharmaceuticals, Puma Biotechnology, Mylan, Eisai, Daiichi Sankyo
Research Funding: OBI Pharma (Inst), Pfizer (Inst), Novartis (Inst), Lilly (Inst), Merck (Inst), Daiichi Sankyo (Inst), Sermonix Pharmaceuticals (Inst), AstraZeneca (Inst), Gilead Sciences (Inst), Astellas Pharma (Inst), Pionyr (Inst), Taiho Oncology (Inst), Veru (Inst), GlaxoSmithKline (Inst), Hoffmann-La Roche AG/Genentech, Inc (Inst), Stemline Therapeutics (Inst)
Travel, Accommodations, Expenses: Merck, AstraZeneca, Gilead Sciences, Pfizer
Open Payments Link: https://openpaymentsdata.cms.gov/physician/183398
Matthew P. Goetz
Consulting or Advisory Role: Lilly (Inst), AstraZeneca (Inst), Blueprint Medicines (Inst), Genzyme (Inst), ARC Therapeutics (Inst), BioTheranostics (Inst), RNA Diagnostics (Inst), Seagen (Inst), Engage Health Media (Inst), Novartis (Inst), Sermonix Pharmaceuticals (Inst)
Research Funding: Lilly (Inst), Pfizer (Inst), Sermonix Pharmaceuticals (Inst), Atossa Genetics (Inst), AstraZeneca (Inst), Loxo (Inst)
Patents, Royalties, Other Intellectual Property: Methods and Materials for Assessing Chemotherapy Responsiveness and Treating Cancer, Methods and Materials for Using Butyrylcholinesterase to Treat Cancer, Development of Human Tumor Xenografts From Women With Breast Cancer Treated With Neoadjuvant Chemotherapy (Inst)
Travel, Accommodations, Expenses: Lilly (Inst)
Erika P. Hamilton
Consulting or Advisory Role: Pfizer (Inst), Genentech/Roche (Inst), Lilly (Inst), Daiichi Sankyo (Inst), Mersana (Inst), AstraZeneca (Inst), Novartis (Inst), Seagen (Inst), ITeos Therapeutics (Inst), Janssen (Inst), Loxo (Inst), Relay Therapeutics (Inst), Greenwich LifeSciences (Inst), Orum Therapeutics (Inst), Ellipses Pharma (Inst), Olema Pharmaceuticals (Inst), Stemline Therapeutics (Inst), Tubulis GmbH (Inst), Verascity Science (Inst), Theratechnologies (Inst)
Research Funding: AstraZeneca (Inst), Hutchison MediPharma (Inst), OncoMed (Inst), MedImmune (Inst), Stem CentRx (Inst), Genentech/Roche (Inst), Curis (Inst), Verastem (Inst), Zymeworks (Inst), Syndax (Inst), Lycera (Inst), Rgenix (Inst), Novartis (Inst), Mersana (Inst), Millennium (Inst), TapImmune Inc (Inst), Lilly (Inst), Pfizer (Inst), Tesaro (Inst), Boehringer Ingelheim (Inst), H3 Biomedicine (Inst), Radius Health (Inst), Acerta Pharma (Inst), MacroGenics (Inst), AbbVie (Inst), Immunomedics (Inst), Fujifilm (Inst), eFFECTOR Therapeutics (Inst), Merus (Inst), Nucana (Inst), Regeneron (Inst), Leap Therapeutics (Inst), Taiho Pharmaceutical (Inst), EMD Serono (Inst), Daiichi Sankyo (Inst), ArQule (Inst), Syros Pharmaceuticals (Inst), Clovis Oncology (Inst), CytomX Therapeutics (Inst), InventisBio (Inst), Deciphera (Inst), Sermonix Pharmaceuticals (Inst), Sutro Biopharma (Inst), Zenith Epigenetics (Inst), Arvinas (Inst), Harpoon (Inst), Black Diamond Therapeutics (Inst), Orinove (Inst), Molecular Templates (Inst), Seagen (Inst), Compugen (Inst), G1 Therapeutics (Inst), Karyopharm Therapeutics (Inst), Dana Farber Cancer Hospital (Inst), Onconova Therapeutics (Inst), Shattuck Labs (Inst), PharmaMar (Inst), Olema Pharmaceuticals (Inst), Immunogen (Inst), Plexxikon (Inst), Amgen (Inst), Akeso Biopharma (Inst), ADC Therapeutics (Inst), AtlasMedx (Inst), Aravive (Inst), Ellipses Pharma (Inst), Incyte (Inst), MabSpace Biosciences (Inst), ORIC Pharmaceuticals (Inst), Pieris Pharmaceuticals (Inst), Pionyr (Inst), Repertoire Immune Medicines (Inst), Treadwell Therapeutics (Inst), Jacobio (Inst), Accutar Biotech (Inst), Artios (Inst), Bliss Biopharmaceutical (Inst), Cascadian Therapeutics (Inst), Dantari (Inst), Duality Biologics (Inst), Elucida Oncology (Inst), Infinity Pharmaceuticals (Inst), Relay Therapeutics (Inst), Tolmar (Inst), Torque (Inst), BeiGene (Inst), Context Therapeutics (Inst), K-Group Beta (Inst), Kind Pharmaceuticals (Inst), Loxo (Inst), Oncothyreon (Inst), Orum Therapeutics (Inst), Prelude Therapeutics (Inst), ProfoundBio (Inst), Cullinan Oncology (Inst)
Chiun-Sheng Huang
Honoraria: Roche, Pfizer, Novartis, AstraZeneca, Daiichi Sankyo, Lilly
Consulting or Advisory Role: Pfizer, Roche, Lilly, AstraZeneca, Novartis, Daiichi Sankyo
Speakers' Bureau: Roche, Daiichi Sankyo
Research Funding: AstraZeneca (Inst), Lilly (Inst), MSD (Inst), Novartis (Inst), Pfizer (Inst), Roche (Inst), OBI Pharma (Inst), EirGenix (Inst), Daiichi Sankyo (Inst), Gilead Sciences (Inst), Seagen (Inst)
Travel, Accommodations, Expenses: Pfizer (Inst), Gilead Sciences (Inst)
Elzbieta Senkus
Honoraria: AstraZeneca, Cancérodigest, Curio Science, Egis Pharmaceuticals, Lilly, Exact Sciences/Oecona, Gilead Sciences, High5md, MSD, Novartis, Pfizer, Roche
Consulting or Advisory Role: AstraZeneca, Lilly, Gilead Sciences, Novartis, Pfizer
Travel, Accommodations, Expenses: AstraZeneca, Egis Pharmaceuticals, Gilead Sciences, Novartis
Other Relationship: Amgen, AstraZeneca, Daiichi Sankyo, Lilly, Novartis, OBI Pharma, Pfizer, Roche, Astellas Pharma
Alexey Tryakin
Stock and Other Ownership Interests: Amgen, Lilly, Merck Serono, Merck, Bayer
Consulting or Advisory Role: BioCad, Roche/Genentech, Bristol Myers Squibb, Eisai, Merck Sharp & Dohme, AstraZeneca, Lilly, Amgen
Speakers' Bureau: Bayer Health, BioCad, Lilly, Merck Serono, Sanofi, Amgen, Bristol Myers Squibb, Eisai, Merck Sharp & Dohme, Pfizer, Bayer, AstraZeneca/Daiichi Sankyo, Novartis
Research Funding: Biocad (Inst)
Travel, Accommodations, Expenses: Novartis, BioCad, Bayer, Veropharm, Sanofi, AstraZeneca, Merck Serono
Irfan Cicin
Consulting or Advisory Role: Pfizer (Inst), MSD Oncology (Inst), Roche (Inst), Novartis/Ipsen (Inst), Lilly (Inst), Bristol Myers Squibb (Inst), Servier (Inst), Abdi Ibrahim (Inst), Nobelpharma (Inst), AbbVie (Inst), Teva, Janssen Oncology (Inst), Takeda (Inst), Gen (Inst), Astellas Pharma (Inst), Gilead Sciences (Inst)
Speakers' Bureau: Novartis (Inst), Roche (Inst), Bristol Myers Squibb (Inst), Pfizer (Inst), Abdi Ibrahim (Inst), Astellas Pharma, MSD (Inst), Gen (Inst), Teva (Inst)
Laura Testa
Consulting or Advisory Role: MSD Oncology, Lilly, Daiichi Sankyo/Astra Zeneca, MSD/AstraZeneca, AstraZeneca, Pfizer, Novartis
Speakers' Bureau: Novartis, Pfizer, MSD Oncology, Daiichi Sankyo/Astra Zeneca, Lilly
Research Funding: Novartis (Inst)
Travel, Accommodations, Expenses: Roche, Gilead Sciences, AstraZeneca
Patrick Neven
Consulting or Advisory Role: Lilly (Inst), Pfizer (Inst), Novartis (Inst), Roche (Inst), Radius Health (Inst)
Travel, Accommodations, Expenses: Lilly (Inst), Pfizer (Inst), Roche (Inst)
Jens Huober
Honoraria: Roche, Lilly, Pfizer, MSD Oncology, AstraZeneca, Novartis, Seagen, Daiichi Sankyo/Astra Zeneca, Gilead Sciences
Consulting or Advisory Role: Novartis, Roche, Pfizer, Lilly, AstraZeneca, Daiichi Sankyo/Astra Zeneca, Gilead Sciences
Travel, Accommodations, Expenses: Roche, Pfizer, Daiichi Sankyo, Gilead Sciences
Uncompensated Relationships: German Breast Group
Ran Wei
Employment: Lilly
Stock and Other Ownership Interests: Lilly
Valérie André
Employment: Lilly
Stock and Other Ownership Interests: Lilly
Maria Munoz
Employment: Lilly
Stock and Other Ownership Interests: Lilly
Honoraria: MSD Oncology, AstraZeneca, Debiopharm Group, Pfizer, Janssen, Sanofi, Takeda, BMS Norway, Lilly, Gilead Sciences
Consulting or Advisory Role: Janssen, MSD, AstraZeneca, Lilly, Pfizer, BMS Norway
Research Funding: Roche, AstraZeneca
Belen San Antonio
Employment: Lilly
Stock and Other Ownership Interests: Lilly
Ashwin Shahir
Employment: Lilly
Stock and Other Ownership Interests: Lilly
Nadia Harbeck
Stock and Other Ownership Interests: West German Study Group
Honoraria: Roche, Novartis, Pfizer, AstraZeneca, Pierre Fabre, Daiichi-Sankyo, MSD, Seagen, Lilly, Viatris, Sanofi, Zuelligpharma, Gilead Sciences, Amgen
Consulting or Advisory Role: Novartis, Sandoz, West German Study Group, Seagen, Gilead Sciences, Roche/Genentech
Speakers' Bureau: Medscape, Springer Healthcare, EPG Communication
Research Funding: Roche/Genentech (Inst), Lilly (Inst), MSD (Inst), AstraZeneca (Inst)
Stephen Johnston
Honoraria: Pfizer, AstraZeneca, Lilly
Consulting or Advisory Role: Lilly, Puma Biotechnology, Pfizer, Genzyme
Research Funding: Pfizer (Inst)
Expert Testimony: Novartis
No other potential conflicts of interest were reported.
REFERENCES
- 1.Sheffield KM, Peachey JR, Method M, et al. : A real-world US study of recurrence risks using combined clinicopathological features in HR-positive, HER2-negative early breast cancer. Future Oncol 18:2667-2682, 2022 [DOI] [PubMed] [Google Scholar]
- 2.NCCN : NCCN Clinical Practice Guidelines in Oncology (NCCN Guidelines) for Breast Cancer V.4.2023. 2023. https://www.nccn.org/ [Google Scholar]
- 3.ESMO-MCBS : ESMO-MCBS Scorecards. 2023. https://www.esmo.org/guidelines/esmo-mcbs/esmo-mcbs-for-solid-tumours/esmo-mcbs-scorecards/scorecard-371-1 [Google Scholar]
- 4.Johnston SRD, Toi M, O'Shaughnessy J, et al. : Abemaciclib plus endocrine therapy for hormone receptor-positive, HER2-negative, node-positive, high-risk early breast cancer (monarchE): Results from a preplanned interim analysis of a randomised, open-label, phase 3 trial. Lancet Oncol 24:77-90, 2023 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Johnston SRD, Harbeck N, Hegg R, et al. : Abemaciclib combined with endocrine therapy for the adjuvant treatment of HR+, HER2-node-positive, high-risk, early breast cancer (monarchE). J Clin Oncol 38:3987-3998, 2020 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Early Breast Cancer Trialists' Collaborative Group (EBCTCG) : Aromatase inhibitors versus tamoxifen in early breast cancer: Patient-level meta-analysis of the randomised trials. Lancet 386:1341-1352, 2015 [DOI] [PubMed] [Google Scholar]
- 7.Howell A, Cuzick J, Baum M, et al. : Results of the ATAC (Arimidex, Tamoxifen, Alone or in Combination) trial after completion of 5 years' adjuvant treatment for breast cancer. Lancet 365:60-62, 2005 [DOI] [PubMed] [Google Scholar]
- 8.Thürlimann B, Keshaviah A, Coates AS, et al. : A comparison of letrozole and tamoxifen in postmenopausal women with early breast cancer. N Engl J Med 353:2747-2757, 2005 [DOI] [PubMed] [Google Scholar]
- 9.Salvo EM, Ramirez AO, Cueto J, et al. : Risk of recurrence among patients with HR-positive, HER2-negative, early breast cancer receiving adjuvant endocrine therapy: A systematic review and meta-analysis. Breast 57:5-17, 2021 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Martín M, Carrasco E, Rodríguez-Lescure Á, et al. : Long-term outcomes of high-risk HR-positive and HER2-negative early breast cancer patients from GEICAM adjuvant studies and El Alamo IV registry. Breast Cancer Res Treat 201:151-159, 2023 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Pagani O, Walley BA, Fleming GF, et al. : Adjuvant exemestane with ovarian suppression in premenopausal breast cancer: Long-term follow-up of the combined TEXT and SOFT trials. J Clin Oncol 41:1376-1382, 2023 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Gnant M, Dueck AC, Frantal S, et al. : Adjuvant palbociclib for early breast cancer: The PALLAS trial results (ABCSG-42/AFT-05/BIG-14-03). J Clin Oncol 40:282-293, 2022 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Loibl S, Marmé F, Martin M, et al. : Palbociclib for residual high-risk invasive HR-positive and HER2-negative early breast cancer—The Penelope-B trial. J Clin Oncol 39:1518-1530, 2021 [DOI] [PubMed] [Google Scholar]
- 14.Slamon DJ, Stroyakovskiy D, Yardley DA, et al. : Ribociclib and endocrine therapy as adjuvant treatment in patients with HR+/HER2– early breast cancer: Primary results from the phase III NATALEE trial. J Clin Oncol 41:LBA500, 2023 [Google Scholar]
- 15.Harbeck N, Guarneri V, Seo JH, et al. : Long-term patient-reported outcomes from monarchE: Abemaciclib plus endocrine therapy for adjuvant HR+, HER2–, node-positive, high-risk, early breast cancer (EBC). Ann Oncol 8:101219, 2023 [DOI] [PubMed] [Google Scholar]
- 16.Hamilton EP, Kim JH, Eigeliene N, et al. : Efficacy and safety results by age in monarchE: Adjuvant abemaciclib combined with endocrine therapy (ET) in patients with HR+, HER2-node-positive, high-risk early breast cancer (EBC). J Clin Oncol 41:501, 2023 [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Data Availability Statement
Eli Lilly and Company provides access to all individual participant data collected during the trial, after anonymization, with the exception of pharmacokinetic or genetic data. Data are available to request 6 months after the indication studied has been approved in the United States and European Union and after primary publication acceptance, whichever is later. No expiration date of data requests is currently set once data are made available. Access is provided after a proposal has been approved by an independent review committee identified for this purpose and after receipt of a signed data sharing agreement. Data and documents, including the study protocol, statistical analysis plan, clinical study report, blank or annotated case report forms, will be provided in a secure data sharing environment. For details on submitting a request, see the instructions provided at www.vivli.org.