

ABSTRACT
Preparing fecal microbiota transplants immediately after donation is resource-intensive, and a proportion are destroyed following abnormal screening results. We retrospectively compared two processes, frozen fecal preparation (FFP) and fresh native frozen preparation (FNFP), for clinical efficacy in the treatment of recurrent Clostridioides difficile infection (rCDI). FFP and FNFP were similarly effective with clinical success rates of 76.7% and 86.7% (P = 0.32), respectively. FNFP is an efficient procedure that saves resources while maintaining clinical efficacy in rCDI.
KEYWORDS: fecal microbiota transplantation, FMT, Clostridium difficile
INTRODUCTION
In 2014, based on literature (1) and international recommendations, the French competent authority classified fecal microbiota transplants as drug (2) and authorized their use in recurrent Clostridioides difficile infection (rCDI). This led to the emergence of FMT centers staffed by pharmacists responsible for managing these preparations. Since then, the transplant production process has evolved. Adding a cryoprotectant allowed the storage at −80°C for up to 2 years, solving many practical and safety issues (3–8). However, the current process of preparing fecal transplants immediately after donation remains complex and time-consuming. In addition, a large proportion of it (approximately 50%) is destroyed due to non-compliant screening results. For these reasons, inspired by a published procedure (9), we started to store directly at −80°C aliquots of donor feces without any preparation. Once the FMT indication was validated, raw fecal samples were thawed the day before transplantation and prepared without cryopreservative solution. Here we report, retrospectively, the efficacy of FMT using this fresh frozen stool procedure compared to the classical frozen fecal preparation (FPP) regarding rCDI.
All patients were treated in the context of routine clinical care in the Assistance Publique-Hopitaux de Paris (AP-HP) FMT center with microbiota transplants prepared between October 2021 and September 2023 and analyzed retrospectively. All patients were enrolled in the COSMIC Cohort (Comité de Protection des Personnes TOURS – Région Centre – Ouest 1; IRB no. IORG0008143; registration number 2019-A02579-48). For all patients, rCDI was the FMT indication. The studied patients had at least two CDI recurrences, with a recurrence being defined as the presence of diarrhea and toxinogenic C. difficile occurring in the 8 weeks following a successful CDI treatment (defined as the resolution of diarrhea). The first 30 consecutive patients treated with fresh native frozen preparation (FNFP) were analyzed. The control group consisted of 30 consecutive patients treated with conventional FFP during the same period. The choice of using FFP or FNFP was made by the pharmacist, without the intervention of the clinician in charge of the patients, and based on the expiration date of the stored transplants. Donor screening was performed in accordance with the National Agency for the Safety of Medicines and Health Products (ANSM) and the French Fecal Transplantation Group (GFTF) guidelines (2, 10).
In FFP (Fig. 1A), the freshly emitted donation was homogenized in cryopreservation solution (NaCl 0.9%/glycerol 90/10 vol/vol), filtered and stored at −80°C within 6 h after donation. The sample was thawed at 4–8°C the day before the procedure, filtered and packaged into pharmaceutical form prior to the administration (11). FNFP (Fig. 1B) were made from aliquots of freshly donated stools frozen at −80°C within 6 h after donation, thawed at 4–8°C the day before the FMT procedure and homogenized with NaCl 0.9% only, filtered, and packaged into the pharmaceutical form prior to the administration.
Fig 1.
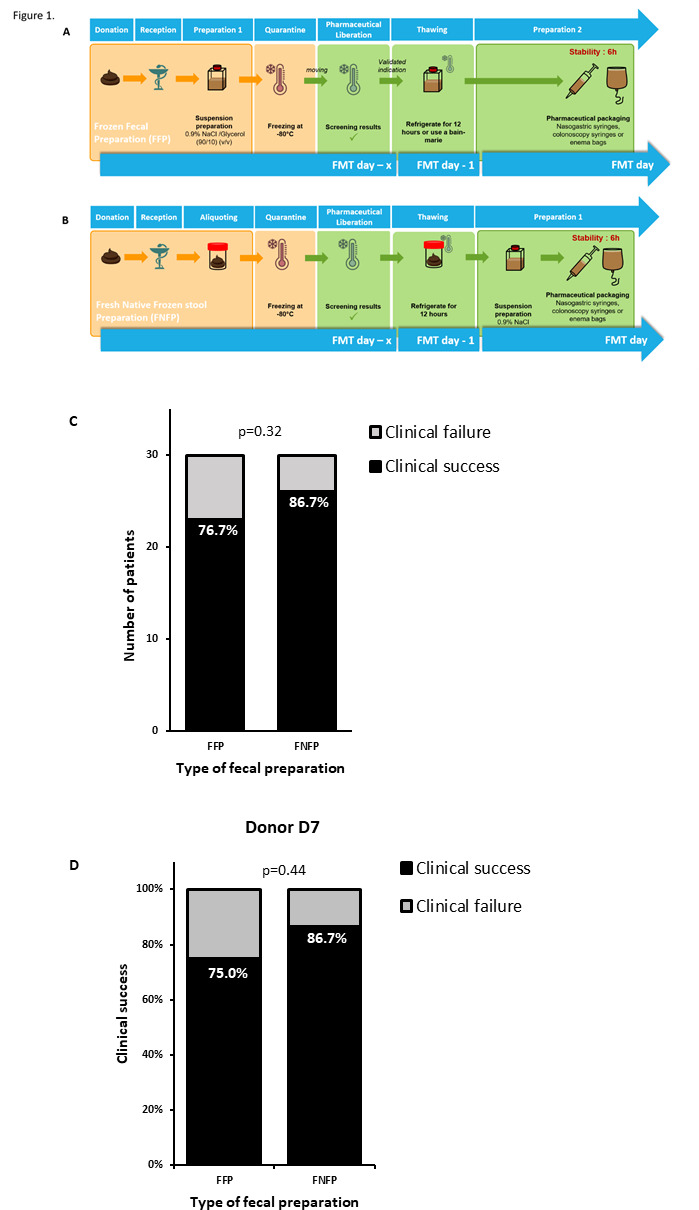
Clinical success of the two fecal preparation procedures. (A) Frozen fecal preparation (FFP), (B) fresh native frozen stool preparation (FNFP), (C) clinical success of FMT, and (D) clinical success of FMT restricted to donor D7.
The day before the FMT, the patient received the last dose of antibiotics (vancomycin or fidaxomicin) and a colon cleansing (4 L of polyethylene glycol). Transplant could be administered either by nasogastric tube (with proton pump inhibitor treatment the day before and the day of FMT) or by enema or colonoscopy.
Clinical success was defined as the absence of CDI recurrence within 10 weeks following FMT. The success rate was compared between the two groups using a χ2 test for independence, using R software (version 4.0.2). Beforehand, clinical parameters were tested to ensure that the two groups were comparable.
The two populations were comparable in terms of patient and FMT characteristics (Table 1). The overall clinical success rate was 86.7% [26/30—IC 95% (74.6–98.9)] and 76.7% [23/30 IC 95% (61.5–91.8)] in the FNFP and FFP groups, respectively, with no statistically significant difference (Fig. 1C). Among the 11 patients who failed FMT, 8 underwent a second FMT, 5 in the FFP group, and 3 in the FNFP group. In some patients, treatment was effective after several administrations, leading to an overall success rate of 91.7% [55/60—IC 95% (0.847–0.987)] (Table S1).
TABLE 1.
Clinical characteristics of the two groups of patientsa
| FFP (n = 30) | FNFP (n = 30) | P value | |
|---|---|---|---|
| Gender | |||
| Women: n (%) | 16 (53.3) | 18 (60.0) | 0.44 |
| Age: mean in years (range) | 62.3 (22–96) | 62.4 (24–101) | 0.69 |
| Administration route | |||
| Upper | 20 | 22 | 0.78 |
| Lower | 10 | 8 | |
| Stool quantity per FMT | |||
| 25 g | 18 | 20 | 0.79 |
| 50 g | 12 | 10 | |
| Donor | |||
| Donor 7 | 16 | 21 | 0.29 |
| Other donors | 14 | 9 | |
| Number of CDI recurrence before FMT: mean (range) | |||
| 2.8 (2–4) | 2.7 (2–5) | 0.19 | |
| Last antibiotics treatment before FMT | |||
| Vancomycin | 19 | 19 | 1 |
| Fidaxomicin | 11 | 11 | |
FMT, fecal microbiota transplantation; D + number = donor identity code; CDI, Clostridioides difficile infection.
Seven donors were used, but, as indicated in Table 1, stools from Donor 7 were used to prepare a majority of both FFP and FNFP. We prepared either FFP or FNFP from one stool donation. However, stool samples from each cycle of donation (consecutive donations for a maximum of 4 weeks) were used to prepare both FFP and FNFP. To rule out any “donor effect” that could have biased our results, we performed a sensitivity analysis by repeating the comparison in this subgroup. As shown in Fig. 1D, no statistically significant difference was observed.
This work demonstrates that FNFP leads to similar clinical efficacy in rCDI compared to conventional preparation with a success rate of the first FMT of 86.7%, which was not statistically different from the control group (76.7%) nor from the litterature (12, 13), even when restricting the analysis to the patients treated with material from the same donor. However, it is important to note that these results were obtained in a small cohort of patients and in a non-randomized way, without taking into account all potential confounding factors.
Although the effect of freezing on bacterial viability and the value of using a cryoprotectant to preserve it has been discussed in numerous studies, the usefulness of the cryoprotector is questioned by these results (14, 15). It seems that feces is not an inert material and probably have a protective effect on the micro-organisms, as shown by Biclot et al. (16). Moreover, the mechanism of action of FMT in the treatment of CDI has not been fully elucidated and may also involve the intervention of diffusible elements of human feces (17–19).
In a separate study, we showed that, in the frequent case of non-validation of the donor, FNFP is associated with much less waste of time as it requires an average of 4.6 min for aliquoting the fresh stools, compared to 24 min for the first part of the FFP preparation. With FNFP, only biologically validated feces are processed into pharmaceutical form, reducing the destruction of transplants and manipulations of uncharacterized fecal material. FNFP procedure is cost-effective as the budget required for the aliquoting of fresh stools is three times lower than the one required for the first step of the FFP procedure (20).
It is important to note that we cannot limit ourselves to the FNFP process, as capsules and ready-to-use preparations must be made from fresh stool.
Future studies are needed in larger cohorts, and to investigate the stability of FNP stool over time.
In conclusion, FNFP is a simple, practical cost-effective procedure while maintaining clinical efficacy in rCDI.
ACKNOWLEDGMENTS
The COSMIC cohort is funded by the Société Nationale Française de Gastro-Entérologie (SNFGE) and the Société de pathologie infectieuse de langue française (SPILF).
R.S., A.-C.J., and H.S. designed the study, performed the analyses, interpreted the results, and drafted the manuscript. S.T., P.M., C.L., A.B., N.B., and H.S. recruited the patients and donors. G.N., S.D., N.K., A.M.S., A.S., and C.E. provided technical help. All authors provided intellectual input, reviewed, and approved the manuscript.
Contributor Information
Anne-Christine Joly, Email: anne-christine.joly@aphp.fr.
Harry Sokol, Email: harry.sokol@gmail.com.
Jared A. Silverman, Bill & Melinda Gates Medical Research Institute, Cambridge, Massachusetts, USA
SUPPLEMENTAL MATERIAL
The following material is available online at https://doi.org/10.1128/aac.00734-24.
Follow-up after first fecal microbiota transplantation failure.
ASM does not own the copyrights to Supplemental Material that may be linked to, or accessed through, an article. The authors have granted ASM a non-exclusive, world-wide license to publish the Supplemental Material files. Please contact the corresponding author directly for reuse.
REFERENCES
- 1. van Nood E, Vrieze A, Nieuwdorp M, Fuentes S, Zoetendal EG, de Vos WM, Visser CE, Kuijper EJ, Bartelsman J, Tijssen JGP, Speelman P, Dijkgraaf MGW, Keller JJ. 2013. Duodenal infusion of donor feces for recurrent Clostridium difficile. N Engl J Med 368:407–415. doi: 10.1056/NEJMoa1205037 [DOI] [PubMed] [Google Scholar]
- 2. Ansm . 2016. La transplantation de microbiote fécal et son encadrement dans les essais cliniques
- 3. Trang C, Scanzi J, Galperine T, Mosca A, Batista R, Sokol H. 2017. Transplantation de microbiote fécal dans le cadre des infections à Clostridium difficile récidivantes: actualisation des recommandations pour la pratique clinique courante. Hepato-Gastro Oncol Dig 24:319–325. doi: 10.1684/hpg.2017.1438 [DOI] [Google Scholar]
- 4. Youngster I, Sauk J, Pindar C, Wilson RG, Kaplan JL, Smith MB, Alm EJ, Gevers D, Russell GH, Hohmann EL. 2014. Fecal microbiota transplant for relapsing Clostridium difficile infection using a frozen inoculum from unrelated donors: a randomized, open-label, controlled pilot study. Clin Infect Dis 58:1515–1522. doi: 10.1093/cid/ciu135 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5. Hamilton MJ, Weingarden AR, Sadowsky MJ, Khoruts A. 2012. Standardized frozen preparation for transplantation of fecal microbiota for recurrent Clostridium difficile infection. Am J Gastroenterol 107:761–767. doi: 10.1038/ajg.2011.482 [DOI] [PubMed] [Google Scholar]
- 6. Satokari R, Mattila E, Kainulainen V, Arkkila PET. 2015. Simple faecal preparation and efficacy of frozen inoculum in faecal microbiota transplantation for recurrent Clostridium difficile infection--an observational cohort study. Aliment Pharmacol Ther 41:46–53. doi: 10.1111/apt.13009 [DOI] [PubMed] [Google Scholar]
- 7. Cammarota G, Ianiro G, Tilg H, Rajilić-Stojanović M, Kump P, Satokari R, Sokol H, Arkkila P, Pintus C, Hart A, et al. 2017. European consensus conference on faecal microbiota transplantation in clinical practice, p 569–580. In Gut. Vol. 66. BMJ Publishing Group. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8. Cammarota G, Ianiro G, Kelly CR, Mullish BH, Allegretti JR, Kassam Z, Putignani L, Fischer M, Keller JJ, Costello SP, et al. 2019. International consensus conference on stool banking for faecal microbiota transplantation in clinical practice. Gut 68:2111–2121. doi: 10.1136/gutjnl-2019-319548 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9. El-Salhy M, Hatlebakk JG, Gilja OH, Bråthen Kristoffersen A, Hausken T. 2020. Efficacy of faecal microbiota transplantation for patients with irritable bowel syndrome in a randomised, double-blind, placebo-controlled study. Gut 69:859–867. doi: 10.1136/gutjnl-2019-319630 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10. Sokol H, Galperine T, Kapel N, Bourlioux P, Seksik P, Barbut F, Scanzi J, Chast F, Batista R, Joly F, Joly A-C, Collignon A, Guery B, Beaugerie L, French Group of Faecal microbiota Transplantation (FGFT) . 2016. Faecal microbiota transplantation in recurrent Clostridium difficile infection: recommendations from the French group of faecal microbiota transplantation. Dig Liver Dis 48:242–247. doi: 10.1016/j.dld.2015.08.017 [DOI] [PubMed] [Google Scholar]
- 11. Batista R, Kapel N, Megerlin F, et al. 2015. Fecal microbiota transplantation in recurrent Clostridium difficile infections framework and pharmaceutical preparation aspects. Ann Pharm Fr 73:323–331. doi: 10.1016/j.pharma.2015.02.004 [DOI] [PubMed] [Google Scholar]
- 12. Ianiro G, Maida M, Burisch J, Simonelli C, Hold G, Ventimiglia M, Gasbarrini A, Cammarota G. 2018. Efficacy of different faecal microbiota transplantation protocols for Clostridium difficile infection: a systematic review and meta-analysis. United European Gastroenterol J 6:1232–1244. doi: 10.1177/2050640618780762 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13. Baunwall SMD, Lee MM, Eriksen MK, Mullish BH, Marchesi JR, Dahlerup JF, Hvas CL. 2020. Faecal microbiota transplantation for recurrent Clostridioides difficile infection: an updated systematic review and meta-analysis. EClinicalMedicine 29–30:100642. doi: 10.1016/j.eclinm.2020.100642 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14. Burz SD, Abraham A-L, Fonseca F, David O, Chapron A, Béguet-Crespel F, Cénard S, Le Roux K, Patrascu O, Levenez F, et al. 2019. A Guide for Ex Vivo Handling and Storage of Stool Samples Intended for Fecal Microbiota Transplantation. Sci Rep 9:8897. doi: 10.1038/s41598-019-45173-4 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15. Costello SP, Conlon MA, Vuaran MS, Roberts-Thomson IC, Andrews JM. 2015. Faecal microbiota transplant for recurrent Clostridium difficile infection using long-term frozen stool is effective: clinical efficacy and bacterial viability data. Aliment Pharmacol Ther 42:1011–1018. doi: 10.1111/apt.13366 [DOI] [PubMed] [Google Scholar]
- 16. Biclot A, Huys GRB, Bacigalupe R, D’hoe K, Vandeputte D, Falony G, Tito RY, Raes J. 2022. Effect of cryopreservation medium conditions on growth and isolation of gut anaerobes from human faecal samples. Microbiome 10:80. doi: 10.1186/s40168-022-01267-2 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17. Khoruts A, Sadowsky MJ. 2016. Understanding the mechanisms of faecal microbiota transplantation. Nat Rev Gastroenterol Hepatol 13:508–516. doi: 10.1038/nrgastro.2016.98 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18. Khoruts A, Staley C, Sadowsky MJ. 2021. Faecal microbiota transplantation for Clostridioides difficile: mechanisms and pharmacology. Nat Rev Gastroenterol Hepatol 18:67–80. doi: 10.1038/s41575-020-0350-4 [DOI] [PubMed] [Google Scholar]
- 19. Ott SJ, Waetzig GH, Rehman A, Moltzau-Anderson J, Bharti R, Grasis JA, Cassidy L, Tholey A, Fickenscher H, Seegert D, Rosenstiel P, Schreiber S. 2017. Efficacy of sterile fecal filtrate transfer for treating patients with Clostridium difficile infection. Gastroenterology 152:799–811. doi: 10.1053/j.gastro.2016.11.010 [DOI] [PubMed] [Google Scholar]
- 20. Sintes R, Navelli G, Delage S, et al. 2023. Best step to freeze faecal microbiota transplants: native faeces, faecal suspension or pharmaceutical forms. In GERPAC. Vol. 368. [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Follow-up after first fecal microbiota transplantation failure.