

Abstract
Aims
Optimal glenoid positioning in reverse shoulder arthroplasty (RSA) is crucial to provide impingement-free range of motion (ROM). Lateralization and inclination correction are not yet systematically used. Using planning software, we simulated the most used glenoid implant positions. The primary goal was to determine the configuration that delivers the best theoretical impingement-free ROM.
Methods
With the use of a 3D planning software (Blueprint) for RSA, 41 shoulders in 41 consecutive patients (17 males and 24 females; means age 73 years (SD 7)) undergoing RSA were planned. For the same anteroposterior positioning and retroversion of the glenoid implant, four different glenoid baseplate configurations were used on each shoulder to compare ROM: 1) no correction of the RSA angle and no lateralization (C-L-); 2) correction of the RSA angle with medialization by inferior reaming (C+M+); 3) correction of the RSA angle without lateralization by superior compensation (C+L-); and 4) correction of the RSA angle and additional lateralization (C+L+). The same humeral inlay implant and positioning were used on the humeral side for the four different glenoid configurations with a 3 mm symmetric 135° inclined polyethylene liner.
Results
The configuration with lateralization and correction of the RSA angle (C+L+) led to better ROM in flexion, extension, adduction, and external rotation (p ≤ 0.001). Only internal rotation was not significantly different between groups (p = 0.388). The configuration where correction of the inclination was done by medialization (C+M+) led to the worst ROM in adduction, extension, abduction, flexion, and external rotation of the shoulder.
Conclusion
Our software study shows that, when using a 135° inlay reversed humeral implant, correcting glenoid inclination (RSA angle 0°) and lateralizing the glenoid component by using an angled bony or metallic augment of 8 to 10 mm provides optimal impingement-free ROM.
Cite this article: Bone Jt Open 2024;5(10):851–857.
Keywords: Shoulder, Range of motion, Reverse shoulder arthroplasy, Lateralization, Software analysis, Glenoid augmentation, Inclination correction, reverse shoulder arthroplasty (RSA), RSA, glenoids, glenoid implant, adduction, flexion, humeral implant, abduction, glenoid inclination, glenoid component
Introduction
Glenoid baseplate configuration is crucial to avoid scapular notching, implant failure, and impingement-free range of motion (ROM).1-6 Positioning the baseplate as inferiorly as possible and correcting deformation in the axial plane has been well studied and agreed upon to avoid scapular notching and impingement.3,7,8 Two crucial factors are always taken into consideration: medialization or lateralization, and inclination correction. Superior inclination of the baseplate has been associated with increased stresses, glenoid baseplate loosening, and scapular notching.3,9-11
The implants available on the market exhibit considerable variation. Lateralization within the glenoid baseplate is not consistent in all implants.12 Lateralization can also be achieved using a bone graft,3,7 or a metal-augmented implant.13,14 Additionally, the extent of reaming on the glenoid side contributes to further medializing the glenoid baseplate.
There remains an ongoing debate regarding glenoid implant positioning. Lateralization and inclination correction are not consistently applied in a systematic manner, and there is a lack of consensus among surgeons regarding these aspects in reverse shoulder arthroplasty (RSA). The establishment of definitive golden rules concerning these parameters is still pending and necessary.15 Notably, these two parameters are interdependent. In situations where metallic or bone augmentation is not available, glenoid reaming becomes the sole method to achieve a neutral inclination. Our primary objective was to ascertain the configurations that offer the most and least impingement-free ROM using a validated 3D software (Blueprint; Stryker, USA). Our hypothesis was that correcting inclination and lateralization would yield the optimal impingement-free ROM.
Methods
Our study was approved by the Institutional Review Board (IRB), with the ethical approval reference number ICR-2023-SHR-09-1. This study included 41 shoulders from 41 patients: 24 females (59 %) and 17 males (41%), with a mean age of 73 years (SD 7). All patients underwent primary RSA performed by the senior author (PB) at our institution (Institut De Chirurgie Réparatrice, France). Inclusion criteria encompassed patients diagnosed with cuff tear arthropathy, primary osteoarthritis (OA), or massive rotator cuff tear. Exclusion criteria were revision surgery, secondary OA, type B3/C glenoids, and fracture sequelae. This aimed to mitigate potential influences from variations in glenoid and humerus morphology.
The diagnoses were primary OA in 21 cases, cuff tear arthropathy in 14 cases, and massive rotator cuff tear in 14 cases. Glenoid morphology was assessed by two surgeons (MM, MP) and categorized according to the Walch and Favard classifications.6,16 In the axial plane, there were 22 type A glenoid and 19 type B1 and B2 glenoid. In the sagittal plane, there were 18 type E0, 14 type E1, and 11 type E3 glenoid. Blueprint automatically calculates the RSA angle,17 glenoid inclination,18 and retroversion. The mean RSA angle was 13.39° (SD 6.27°), with a mean inclination of 6.24° (SD 5.5°) and a mean retroversion of 12.48° (SD 10.78°). Using a validated software (Blueprint), we simulated the four most used glenoid baseplate configurations.
Glenoid side
Our approach aimed to consistently place the glenoid baseplate as inferior as possible on the glenoid, ensuring a minimum of 5 mm glenosphere overhang inferiorly.19 The glenoid baseplate was typically set between 0° and 10° of retroversion, aligning the central peg within the glenoid vault. Throughout the different configurations between the groups, no alterations were made to retroversion, anteroposterior, or superoinferior positioning.
When bone augmentation was not required, our objective was to achieve a minimum of 80% glenoid baseplate seating. For smaller glenoids in females, a 25 mm diameter glenoid baseplate paired with a 36 mm glenosphere was used, while larger glenoids in men were addressed with a 29 mm diameter glenoid baseplate and a 42 mm glenosphere.
We made the planning based on four configurations, and we created four groups (Figure 1 and Figure 2):
Fig. 1.

The four tested configurations: a) no correction of the reverse shoulder arthroplasty (RSA) angle and no lateralization(C-L-); b) medialization with correction of the RSA angle (C+M+); c) correction of the RSA angle without lateralization (C+L-); d) correction of the RSA angle with lateralization (C+L+).
Fig. 2.

The reverse shoulder arthroplasty (RSA) angle is shown in red. The vertical purple line crosses the inferior glenoid edge and is used as the reference for medialization or lateralization.
No correction of the RSA angle and no lateralization (C-L-)
Medialization with correction of the RSA angle (C+M+)
Correction of the RSA angle without lateralization (C+L-)
Correction of the RSA angle with lateralization (C+L+)
The reference point for lateralization in the C+L+ group was the inferior glenoid rim (6 o’clock position) which was constantly found in all our CT scans. We arbitrary decided on a 4 mm of inferior lateralization to obtain about 8 to 10 mm of lateralization at the level of the central peg (Figure 3).20 To ensure consistent and reproducible glenoid baseplate positioning in the intended configuration, we calculated the bone graft. This approach aimed to maintain uniform implant positioning across patients and prevent any alterations in implant positioning.
Fig. 3.
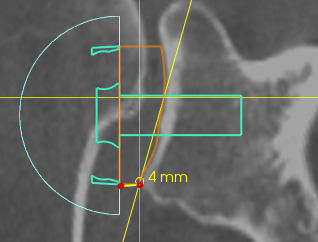
The inferior corner of the glenoid being used as the reference point for 4 mm lateralization.
Humeral side
We used the same inlay humeral implant (Tornier Perform Humeral Stem; Stryker) for all cases. A 135° humeral stem, along with a polyethylene (PE) liner + 3 mm, was consistently employed for all patients and across all configurations to maintain consistent results and to avoid humeral changes influencing the ROM.
Groups
The four glenoid configurations were planned for each 41 shoulders (41 patients), with four glenoid configurations planned for each of the 41 shoulders (total of 164 planned). Using Blueprint, glenohumeral impingement-free ROM was simulated and the following parameters were recorded: flexion, extension, adduction, abduction, internal rotation (IR), and external rotation (ER). All the planning was done and approved by two trained shoulder surgeons (MM, MP) under the direct supervision of the senior author (PB).
Statistical analysis
Normality and heteroskedasticity of data were assessed with the Shapiro-Wilk test and the Levene’s test. The difference between ROM according to modalities of GROUP was assessed with the Kruskal-Wallis test. If the null hypothesis of the Kruskal-Wallis test was rejected, post-hoc pairwise analyses were performed with Dunn-Bonferoni’s test. Alpha risk was set to 5% (α = 0.05). Statistical analysis was performed with EasyMedStat version 3.30 (EasyMedStat, France).21
Results
Figure 3 illustrates that the C+L+ (correction of inclination with maximum lateralization) group exhibited the most favourable mean ROM across adduction, abduction, extension, flexion, and external rotation. Notably, internal rotation remained relatively consistent across all groups. Conversely, the C+M+ group displayed the least favourable ROM in all movements. Mean ROM with the four configurations is summarized in Figure 4.
Fig. 4.

Impingement-free range of motion (ROM)° in each group. C-L-, no correction of the reverse shoulder arthroplasty (RSA) angle and no lateralization; C+M+, medialization with correction of the RSA angle; C+L-, correction of the RSA angle without lateralization; C+L+, correction of the RSA angle with lateralization.
When analyzing the ROM for each group, we found that in abduction the C+L+ group has the best impingement-free ROM, and that the C+M+ group performs the worst with a mean abduction of 58° (SD 13°) versus 74° (SD 11°) in the C+L+ group (p < 0.001). Pairwise analyses revealed differences for C-L- versus C+L+ (p = 0.036), C+M+ versus C+L- (p < 0.001), and C+M+ versus C-L- (p = 0.002) (Figure 5).
Fig. 5.

Mean value of abduction (ABD) in each group. C-L-, no correction of the reverse shoulder arthroplasty (RSA) angle and no lateralization; C+M+, medialization with correction of the RSA angle; C+L-, correction of the RSA angle without lateralization; C+L+, correction of the RSA angle with lateralization.
For adduction, the C+L+ group performed the best compared to all groups with a mean adduction of 40° (SD 9°), and the C+M+ performed the worst in adduction with a mean of 20° (SD 10°) (p < 0.001). Pairwise analyses revealed differences for C+L+ versus C+L- (p < 0.001), C-L- versus C+L+ (p < 0.001), C+M+ versus C+L- (p < 0.001), and C+M+ versus C-L- (p = 0.006) (Figure 6).
Fig. 6.

Mean value of adduction (ADD) in each group. C-L-, no correction of the reverse shoulder arthroplasty (RSA) angle and no lateralization; C+M+, medialization with correction of the RSA angle; C+L-, correction of the RSA angle without lateralization; C+L+, correction of the RSA angle with lateralization.
As for flexion, the C+L+ group performed the best with a mean value of 127° (SD 26°); the C+M+ group performed the worst with a mean value of 94° (SD 25°) (p < 0.001). Pairwise analyses revealed differences for C+L+ versus C+L- (p = 0.01), C-L- versus C+L+ (p < 0.001), and C+M+ versus C+L- (p = 0.001) (Figure 7).
Fig. 7.
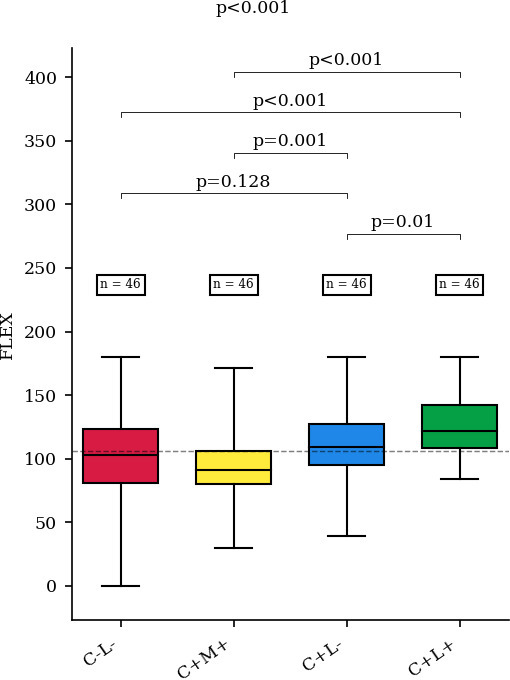
Mean value of flexion (FLEX) in each group. C-L-, no correction of the reverse shoulder arthroplasty (RSA) angle and no lateralization; C+M+, medialization with correction of the RSA angle; C+L-, correction of the RSA angle without lateralization; C+L+, correction of the RSA angle with lateralization.
For extension, the C+L+ group also performed the best in comparison with all groups with a mean value of 103° (SD 26°), and the C+M+ group performed the worst also with a mean value of 50° (SD 39°) (p < 0.001). Pairwise analyses revealed differences for C+L+ versus C+L- (p = 0.013), C-L- versus C+L+ (p < 0.001), and C+L+versus C+L- (p < 0.001) (Figure 8).
Fig. 8.
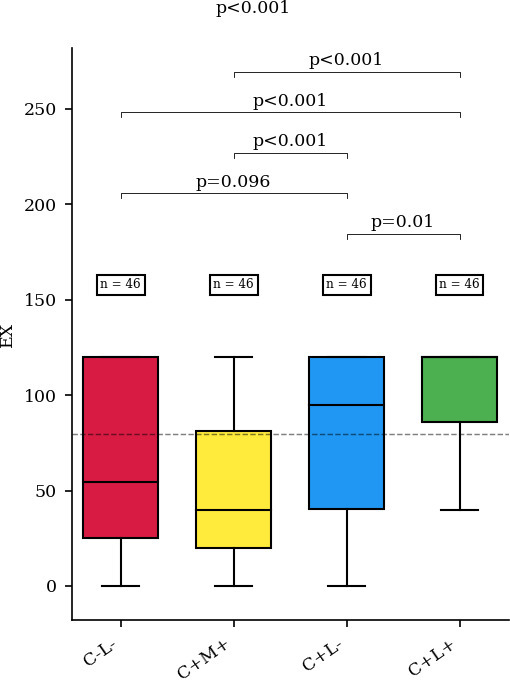
Mean value of extension (EX) in each group. C-L-, no correction of the reverse shoulder arthroplasty (RSA) angle and no lateralization; C+M+, medialization with correction of the RSA angle; C+L-, correction of the RSA angle without lateralization; C+L+, correction of the RSA angle with lateralization.
Regarding ER, the C+L+ had the best ROM with a mean of 59 (SD 11), and the C+M+ had the worst ROM with a mean of 37 (SD 18) (p < 0.001). Pairwise analyses revealed differences for C+ L+versus C+ L- (p = 0.003), C+L+ versus C-L- (p < 0.001), C+M+ versus C+L- (p < 0.001), and C+M+ versus C+L- (p = 0.032) (Figure 9).
Fig. 9.

Mean value of external rotation (ER) in each group. C-L-, no correction of the reverse shoulder arthroplasty (RSA) angle and no lateralization; C+M+, medialization with correction of the RSA angle; C+L-, correction of the RSA angle without lateralization; C+L+, correction of the RSA angle with lateralization.
Mean values of IR were not statistically different between all the different groups (p = 0.388) (Figure 10).
Fig. 10.

Mean value of internal rotation (IR) in each group. C-L-, no correction of the reverse shoulder arthroplasty (RSA) angle and no lateralization; C+M+, medialization with correction of the RSA angle; C+L-, correction of the RSA angle without lateralization; C+L+, correction of the RSA angle with lateralization.
We further categorized patients into three groups based on their diagnoses: primary OA, cuff tear arthropathy, and massive rotator cuff tear. Upon assessment, differences in the mean ROM were generally indistinguishable between these groups, except for flexion. Specifically, flexion exhibited a notably superior mean of 117° (SD 24°) in cuff tear arthropathy compared to a mean of 105° (SD 31°) in primary OA.
Discussion
Our software study shows that, when using a 135° inlay reversed humeral implant, correcting glenoid inclination (RSA angle 0°) and lateralizing the glenoid component by using an angled bony or metallic augment of 8 to 10 mm provides optimal impingement-free ROM. Conversely, the worst ROM is observed when the inclination was corrected by medializing the glenoid implant (i.e. by inferior reaming of the glenoid).
The correction of inclination and RSA angle can be achieved through two primary methods: either via inferior reaming with medialization of the glenoid baseplate, or through superior augmentation using metal or bone grafts.22 In our institution an angled autograft is systematically used to lateralize the glenoid and correct its inclination.3,17
In cuff tear arthropathy, bone loss commonly occurs in the superior or central areas of the glenoid, leaving the inferior corner of the glenoid intact. Therefore, the correction of this superior bone loss becomes essential to attain a neutral inclination and RSA angle.5,22,23
Even in primary glenohumeral OA, several studies have shown that the glenoid inclination is often superior.4,24,25 Only type C glenoids are frequently associated with posteroinferior bone loss and display glenoid inferior inclination.26-29 Our data suggest that correction of inclination and lateralization are both crucial to obtain the optimal ROM; correcting it through medialization is detrimental. RSA medialization has been consistently associated with complications such as glenoid loosening, scapular notching, and instability.2,3,30 Correction of inclination associated with glenoid lateralization offers several advantages: it diminishes the vertical shearing forces, which are a risk factor for glenoid loosening,9,22 and reduces scapular notching.4,10,11,22
In our study, we selected the inferior corner of the glenoid as the reference point for lateralization, considering the prevalent central and superior glenoid erosion observed in primary OA and cuff tear arthropathy cases. Our findings align with this approach, demonstrating that when inclination correction is coupled with a 4 mm lateralization from the inferior glenoid corner, superior outcomes in all ROM parameters, except for IR, were observed. Notably, glenoid lateralization is correlated with a reduction in scapular notching.1-3 Lateralization is also associated with better impingement-free ROM as demonstrated by several 3D software simulated ROM studies.25,31,32 In our analysis, despite the association between lateralization and inclination and the clinical improvement of IR,33 we did not observe statistically significant differences among the groups in terms of IR.
One possible explanation for this finding lies in the biomechanics involved in achieving IR. To position the arm behind the back, extension plays a pivotal role in conjunction with internal rotation. Hochreiter et al’s34 recent study emphasized the necessity of at least 40° of extension for functional internal rotation. Interestingly, our study highlighted that the C+M+ group exhibited notably poorer extension performance, with a mean extension value of 50° (SD 39°), in contrast to 103° (SD 26°) in the C+L+ group. When planning a RSA, attention to the extension should be made to avoid loss of functional IR postoperatively.
Excessive lateralization in RSA can lead to increased stress on the glenoid component, resulting in loosening and potential implant failure. Additionally, lateralization can disrupt soft-tissue balance, leading to tension imbalances that impair ROM and cause discomfort for the patient.20,35
Lateralization can also increase joint reaction forces, contributing to overstuffing and fractures of the scapular spine.20 Therefore, while lateralization can enhance certain aspects of shoulder mechanics, it must be carefully managed to avoid these complications.The significance of this study is tempered by certain limitations. Primarily, it is a computational study that virtually simulates ROM without accounting for scapulothoracic motion. Additionally, the software used lacks the capability to assess muscle tensioning and function, which notably influence RSA outcomes. However, this limitation did not affect the study’s objective, which aimed to evaluate impingement-free ROM.
Measurements were conducted solely via the 3D software, and planning was carried out by two surgeons. However, to maintain consistency across groups, the criteria for positioning the glenoid baseplate were rigorously adhered to, ensuring changes were made only to the intended entity, be it lateralization or inclination. Notably, the study did not explore the effects of humeral position or different implant configurations such as inlay and onlay designs. Instead, a uniform implant with identical features was employed across all groups to prevent humeral effects on ROM.
This study stands as the first to evaluate various glenoid baseplate positioning involving different combinations of lateralization, medialization, and inclination correction.
In conclusion, the data of our software study show that correcting inclination in tandem with lateralization is crucial to obtain optimal impingement-free ROM after RSA. Conversely, correcting inclination through medialization (at the expense of lateralization) leads to the worst impingement-free ROM.
Take home message
- Correcting glenoid inclination in tandem with lateralization is the best to obtain optimal impingement-free range of motion (ROM) after reverse shoulder arthroplasty.
- Correcting inclination through medialization leads to the worst impingement-free ROM.
Author contributions
M. Mouchantaf: Writing – original draft, Data curation, Formal analysis, Writing – review & editing
M. Parisi: Data curation, Formal analysis, Writing – original draft, Writing – review & editing
G. Secci: Methodology
M. Biegun: Software
M. Chelli: Formal analysis
P. Schippers: Methodology
P. Boileau: Project administration, Supervision, Writing – original draft, Writing – review & editing
Funding statement
The authors received no financial or material support for the research, authorship, and/or publication of this article.
ICMJE COI statement
P. Boileau reports the conception, and being the developer, of Blueprint software; and receiving royalties from Stryker and Depuy, We used the Bluprint software which is related to this work. M. Chelli discloses being the developer of EasyMedStat, which is also related to this manuscript.
Data sharing
The data that support the findings for this study are available to other researchers from the corresponding author upon reasonable request.
Ethical review statement
Our study was approved by the Institutional Review Board (with the ethical approval reference number ICR-2023-SHR-09-1).
Open access funding
The authors report that the open access funding for this manuscript was self-funded.
© 2024 Mouchantaf et al. This is an open-access article distributed under the terms of the Creative Commons Attribution Non-Commercial No Derivatives (CC BY-NC-ND 4.0) licence, which permits the copying and redistribution of the work only, and provided the original author and source are credited. See https://creativecommons.org/licenses/by-nc-nd/4.0/
Contributor Information
Mark Mouchantaf, Email: marc.mchantaf@hotmail.com.
Marco Parisi, Email: dr.marcoparisi@gmail.com.
Gregorio Secci, Email: secci.gregorio@gmail.com.
Manon Biegun, Email: m.biegun@yahoo.fr.
Mikael Chelli, Email: dr.chelli@icr-nice.com.
Philipp Schippers, Email: philipp.schippers@gmail.com.
Pascal Boileau, Email: pr.boileau@icr-nice.com.
Data Availability
The data that support the findings for this study are available to other researchers from the corresponding author upon reasonable request.
References
- 1. Athwal GS, MacDermid JC, Reddy KM, Marsh JP, Faber KJ, Drosdowech D. Does bony increased-offset reverse shoulder arthroplasty decrease scapular notching? J Shoulder Elbow Surg. 2015;24(3):468–473. doi: 10.1016/j.jse.2014.08.015. [DOI] [PubMed] [Google Scholar]
- 2. Boileau P, Moineau G, Roussanne Y, O’Shea K. Bony increased-offset reversed shoulder arthroplasty: minimizing scapular impingement while maximizing glenoid fixation. Clin Orthop Relat Res. 2011;469(9):2558–2567. doi: 10.1007/s11999-011-1775-4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3. Boileau P, Morin-Salvo N, Gauci M-O, et al. Angled BIO-RSA (bony-increased offset-reverse shoulder arthroplasty): a solution for the management of glenoid bone loss and erosion. J Shoulder Elbow Surg. 2017;26(12):2133–2142. doi: 10.1016/j.jse.2017.05.024. [DOI] [PubMed] [Google Scholar]
- 4. Frankle MA, Teramoto A, Luo Z-P, Levy JC, Pupello D. Glenoid morphology in reverse shoulder arthroplasty: classification and surgical implications. J Shoulder Elbow Surg. 2009;18(6):874–885. doi: 10.1016/j.jse.2009.02.013. [DOI] [PubMed] [Google Scholar]
- 5. Lévigne C, Boileau P, Favard L, et al. Scapular notching in reverse shoulder arthroplasty. J Shoulder Elbow Surg. 2008;17(6):925–935. doi: 10.1016/j.jse.2008.02.010. [DOI] [PubMed] [Google Scholar]
- 6. Sirveaux F, Favard L, Oudet D, Huquet D, Walch G, Molé D. Grammont inverted total shoulder arthroplasty in the treatment OF glenohumeral osteoarthritis with massive rupture OF the cuff. Results OF a multicentre study OF 80 shoulders. J Bone Joint Surg Br. 2004;86-B(3):388–395. doi: 10.1302/0301-620x.86b3.14024. [DOI] [PubMed] [Google Scholar]
- 7. Boileau P, Moineau G, Roussanne Y, O’Shea K. Bony increased-offset reversed shoulder arthroplasty: minimizing scapular impingement while maximizing glenoid fixation. Clin Orthop Relat Res. 2011;469(9):2558–2567. doi: 10.1007/s11999-011-1775-4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8. Simovitch RW, Zumstein MA, Lohri E, Helmy N, Gerber C. Predictors of scapular notching in patients managed with the Delta III reverse total shoulder replacement. J Bone Joint Surg Am. 2007;89-A(3):588–600. doi: 10.2106/JBJS.F.00226. [DOI] [PubMed] [Google Scholar]
- 9. Falaise V, Levigne C, Favard L, SOFEC Scapular notching in reverse shoulder arthroplasties: the influence of glenometaphyseal angle. Orthop Traumatol Surg Res. 2011;97(6 Suppl):S131–7. doi: 10.1016/j.otsr.2011.06.007. [DOI] [PubMed] [Google Scholar]
- 10. Gutiérrez S, Walker M, Willis M, Pupello DR, Frankle MA. Effects of tilt and glenosphere eccentricity on baseplate/bone interface forces in a computational model, validated by a mechanical model, of reverse shoulder arthroplasty. J Shoulder Elbow Surg. 2011;20(5):732–739. doi: 10.1016/j.jse.2010.10.035. [DOI] [PubMed] [Google Scholar]
- 11. Laver L, Garrigues GE. Avoiding superior tilt in reverse shoulder arthroplasty: a review of the literature and technical recommendations. J Shoulder Elbow Surg. 2014;23(10):1582–1590. doi: 10.1016/j.jse.2014.06.029. [DOI] [PubMed] [Google Scholar]
- 12. Werthel J-D, Walch G, Vegehan E, Deransart P, Sanchez-Sotelo J, Valenti P. Lateralization in reverse shoulder arthroplasty: a descriptive analysis of different implants in current practice. Int Orthop. 2019;43(10):2349–2360. doi: 10.1007/s00264-019-04365-3. [DOI] [PubMed] [Google Scholar]
- 13. Knowles NK, Ferreira LM, Athwal GS. Augmented glenoid component designs for type B2 erosions: a computational comparison by volume of bone removal and quality of remaining bone. J Shoulder Elbow Surg. 2015;24(8):1218–1226. doi: 10.1016/j.jse.2014.12.018. [DOI] [PubMed] [Google Scholar]
- 14. Theivendran K, Varghese M, Large R, et al. Reverse total shoulder arthroplasty using a trabecular metal glenoid base plate: functional and radiological outcomes at two to five years. Bone Joint J. 2016;98-B(7):969–975. doi: 10.1302/0301-620X.98B7.37688. [DOI] [PubMed] [Google Scholar]
- 15. Berhouet J, Jacquot A, Walch G, Deransart P, Favard L, Gauci M-O. Preoperative planning of baseplate position in reverse shoulder arthroplasty: still no consensus on lateralization, version and inclination. Orthop Traumatol Surg Res. 2022;108(3):103115. doi: 10.1016/j.otsr.2021.103115. [DOI] [PubMed] [Google Scholar]
- 16. Walch G, Badet R, Boulahia A, Khoury A. Morphologic study of the glenoid in primary glenohumeral osteoarthritis. J Arthroplasty. 1999;14(6):756–760. doi: 10.1016/s0883-5403(99)90232-2. [DOI] [PubMed] [Google Scholar]
- 17. Boileau P, Gauci M-O, Wagner ER, et al. The reverse shoulder arthroplasty angle: a new measurement of glenoid inclination for reverse shoulder arthroplasty. J Shoulder Elbow Surg. 2019;28(7):1281–1290. doi: 10.1016/j.jse.2018.11.074. [DOI] [PubMed] [Google Scholar]
- 18. Maurer A, Fucentese SF, Pfirrmann CWA, et al. Assessment of glenoid inclination on routine clinical radiographs and computed tomography examinations of the shoulder. J Shoulder Elbow Surg. 2012;21(8):1096–1103. doi: 10.1016/j.jse.2011.07.010. [DOI] [PubMed] [Google Scholar]
- 19. Boileau P, Morin-Salvo N, Bessière C, Chelli M, Gauci M-O, Lemmex DB. Bony increased-offset-reverse shoulder arthroplasty: 5 to 10 years’ follow-up. J Shoulder Elbow Surg. 2020;29(10):2111–2122. doi: 10.1016/j.jse.2020.02.008. [DOI] [PubMed] [Google Scholar]
- 20. Bauer S, Corbaz J, Athwal GS, Walch G, Blakeney WG. Lateralization in reverse shoulder arthroplasty. J Clin Med. 2021;10(22):5380. doi: 10.3390/jcm10225380. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.No authors listed . EasyMedStat; [4 October 2024]. www.easymedstat.com date last. accessed. [Google Scholar]
- 22. Boileau P, Gauci M-O, Wagner ER, et al. The reverse shoulder arthroplasty angle: a new measurement of glenoid inclination for reverse shoulder arthroplasty. J Shoulder Elbow Surg. 2019;28(7):1281–1290. doi: 10.1016/j.jse.2018.11.074. [DOI] [PubMed] [Google Scholar]
- 23. Werthel J-D, Villard A, Kazum E, Deransart P, Ramirez O. Accuracy of reverse shoulder arthroplasty angle according to the size of the baseplate. J Shoulder Elbow Surg. 2023;32(2):310–317. doi: 10.1016/j.jse.2022.07.006. [DOI] [PubMed] [Google Scholar]
- 24. Daggett M, Werner B, Collin P, Gauci M-O, Chaoui J, Walch G. Correlation between glenoid inclination and critical shoulder angle: a radiographic and computed tomography study. J Shoulder Elbow Surg. 2015;24(12):1948–1953. doi: 10.1016/j.jse.2015.07.013. [DOI] [PubMed] [Google Scholar]
- 25. Gauci M-O, Chaoui J, Berhouet J, Jacquot A, Walch G, Boileau P. Can surgeons optimize range of motion and reduce scapulohumeral impingements in reverse shoulder arthroplasty? A computational study. Shoulder Elbow. 2022;14(4):385–394. doi: 10.1177/1758573221994141. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26. Abboud JA, Bateman DK, Barlow J. Glenoid dysplasia. J Am Acad Orthop Surg. 2016;24(5):327–336. doi: 10.5435/JAAOS-D-15-00032. [DOI] [PubMed] [Google Scholar]
- 27. Gauci M-O, Athwal GS, Sanchez-Sotelo J, et al. Identification of threshold pathoanatomic metrics in primary glenohumeral osteoarthritis. J Shoulder Elbow Surg. 2021;30(10):2270–2282. doi: 10.1016/j.jse.2021.03.140. [DOI] [PubMed] [Google Scholar]
- 28. Currarino G, Sheffield E, Twickler D. Congenital glenoid dysplasia. Pediatr Radiol. 1998;28(1):30–37. doi: 10.1007/s002470050287. [DOI] [PubMed] [Google Scholar]
- 29. Trout TE, Resnick D. Glenoid hypoplasia and its relationship to instability. Skeletal Radiol. 1996;25(1):37–40. doi: 10.1007/s002560050029. [DOI] [PubMed] [Google Scholar]
- 30. Dilisio MF, Warner JJP, Walch G. Accuracy of the subchondral smile and surface referencing techniques in reverse shoulder arthroplasty. Orthopedics. 2016;39(4):e615–20. doi: 10.3928/01477447-20160610-04. [DOI] [PubMed] [Google Scholar]
- 31. Werner BS, Chaoui J, Walch G. The influence of humeral neck shaft angle and glenoid lateralization on range of motion in reverse shoulder arthroplasty. J Shoulder Elbow Surg. 2017;26(10):1726–1731. doi: 10.1016/j.jse.2017.03.032. [DOI] [PubMed] [Google Scholar]
- 32. Lädermann A, Tay E, Collin P, et al. Effect of critical shoulder angle, glenoid lateralization, and humeral inclination on range of movement in reverse shoulder arthroplasty. Bone Joint Res. 2019;8(8):378–386. doi: 10.1302/2046-3758.88.BJR-2018-0293.R1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33. Werner BC, Lederman E, Gobezie R, Denard PJ. Glenoid lateralization influences active internal rotation after reverse shoulder arthroplasty. J Shoulder Elbow Surg. 2021;30(11):2498–2505. doi: 10.1016/j.jse.2021.02.021. [DOI] [PubMed] [Google Scholar]
- 34. Hochreiter B, Wyss S, Gerber C. Extension of the shoulder is essential for functional internal rotation after reverse total shoulder arthroplasty. J Shoulder Elbow Surg. 2022;31(6):1166–1174. doi: 10.1016/j.jse.2021.11.006. [DOI] [PubMed] [Google Scholar]
- 35. Ascione F, Schiavone Panni A, Braile A, et al. Problems, complications, and reinterventions in 4893 onlay humeral lateralized reverse shoulder arthroplasties: a systematic review (part I-complications) J Orthop Traumatol. 2021;22(1):27. doi: 10.1186/s10195-021-00592-w. [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Data Availability Statement
The data that support the findings for this study are available to other researchers from the corresponding author upon reasonable request.