

Abstract
Purpose
To determine new-onset or worsening T2DM risk in patients with metastatic castration-resistant prostate cancer (mCRPC) receiving abiraterone acetate (AA) vs. enzalutamide (ENZA) in England.
Methods
Records of patients on AA and/or ENZA (2015−2021) were analysed retrospectively from UK- or England-wide databases and data sets. The primary endpoint was new-onset or worsening T2DM, analysed using a Cox model.
Results
Of 1382 patients, 84 (6.1%) met the primary endpoint; 42 of 826 patients (5.1%) received ENZA and 42 of 556 patients (7.6%) received AA. Among patients without baseline T2DM (n = 1049), 50 developed new-onset T2DM: 24 (3.9%) on ENZA and 26 (5.9%) on AA. Among patients with baseline T2DM (n = 333), 34 (10.2%) had worsening T2DM: 18 (8.3%) on ENZA and 16 (13.8%) on AA. Patients on ENZA had longer median follow-up (445 vs. 408 days) and treatment duration (164 vs. 139 days) than those on AA, who were also more likely to have new-onset or worsening T2DM than those on ENZA (HR: 1.8; 95% CI: 1.4–2.7; P = 0.0101). The number needed to harm for an additional patient to experience new-onset or worsening T2DM when receiving AA instead of ENZA was 40 overall, 50 in patients without baseline T2DM, and 18 in patients with baseline T2DM.
Conclusion
Patients with mCRPC receiving AA were more likely to experience new-onset or worsening T2DM than those on ENZA, despite having a shorter treatment duration. Further research is required to substantiate these findings in earlier disease settings with longer treatment duration.
Supplementary Information
The online version contains supplementary material available at 10.1007/s00345-024-05280-y.
Keywords: Abiraterone, Enzalutamide, Metastatic castration-resistant prostate cancer, Androgen receptor pathway inhibitor, Type 2 diabetes mellitus
Introduction
Prostate cancer (PC) is the second most prevalent cancer and the fifth most frequent cause of death worldwide, with approximately 1.4 million new cases and 375,000 deaths reported globally in 2020 [1]. In England, PC was the most common cancer reported in 2016−2018, with 52,300 new cases accounting for 27% of new cancer diagnoses in men in this period [2]. The 5- and 10-year survival rates for PC in England are 85% and 80%, respectively [3]. With regard to disease progression, patients with metastatic PC who are initially hormone sensitive become castration resistant, and this is a common cause of mortality in patients with PC [4].
Abiraterone acetate (AA), an androgen biosynthesis inhibitor, and enzalutamide (ENZA), an androgen receptor signalling inhibitor, are androgen receptor pathway inhibitors (ARPIs) that are added to androgen-deprivation therapy (ADT) for the treatment of metastatic castration-resistant PC (mCRPC). AA (in combination with prednisone or prednisolone) and ENZA have been recommended by the National Institute for Health and Care Excellence (NICE) for the treatment of mCRPC during or after docetaxel chemotherapy since 2012 and before chemotherapy since 2016 [5, 6]. Given that these drugs have similar clinical indications and there is no clear guidance for choosing between them, comparison of their outcomes and adverse effects may assist in treatment-related decision-making [7, 8].
Metabolic side effects, including the development of new or worsening type 2 diabetes mellitus (T2DM), have emerged as a concern with the use of ADT in patients with PC [9–12]. Literature reporting the metabolic outcomes of AA and ENZA is emerging, with regulatory agencies including a warning that AA has been associated with altered glucose metabolism [13, 14]. The HEAT study showed a higher rate of new-onset T2DM in patients receiving AA compared with those receiving ENZA [8]. Among patients with mCRPC enrolled in the COU-AA-302 study evaluating AA, hyperglycaemia of any grade occurred in 57% of patients [13]. Further, the European Society for Cardiology (ESC)’s cardio-oncology guidelines list diabetes as a common ADT-related cardiovascular (CV) toxicity for AA but not for ENZA [15].
Owing to the overlapping prevalence and detrimental impact of diabetes in PC, assessing the glycaemic effects of AA and ENZA added to ADT in patients with mCRPC in real-world practice is vital, as it would help in understanding the potential clinical impacts of long-term ARPI use. The present study compared the risk of new-onset or worsening T2DM between patients with mCRPC treated with AA and those treated with ENZA in England.
Methods
Study design and patient selection
This was a retrospective, observational study in England using a national sample of electronic medical records from the Clinical Practice Research Datalink (CPRD) GOLD (UK) and Aurum (England) databases, and the Hospital Episode Statistics, Public Health England Cancer Registry, and Systemic Anti-Cancer Treatment (SACT) data sets. Adult patients with PC treated with AA and/or ENZA (April 2015 to October 2021) were included. Patients were assumed to have mCRPC, as this was the only licensed and reimbursed indication for AA and ENZA during most of the study period. They were also assumed to be on ADT and receiving a concomitant steroid with AA.
Endpoints
The primary endpoint was new-onset T2DM or T2DM progression. Patients were categorised by treatment received (AA or ENZA). Patients switching from AA to ENZA were assigned to their original treatment cohort and censored for the Cox model at that point. New-onset T2DM was defined as T2DM in patients who did not have T2DM at the index date (date of initiation of ENZA or AA in the SACT data set) but subsequently developed it (any primary care prescription of antidiabetic medication) during the follow-up period. Worsening T2DM was defined as T2DM in patients who had T2DM at the index date and required intensified treatment (a shift from conservative management [no treatment] to first-line treatment or progression through the NICE treatment pathway) [16]. Refer to the Supplementary methods for detailed descriptions of endpoint assessment methods and a subgroup analysis performed to evaluate changes in haemoglobin A1C (HbA1c).
Secondary endpoints included persistence and duration of treatment (Supplementary methods) [16, 17], while exploratory endpoints included new-onset T2DM and deterioration of T2DM control. The endpoints were compared between patients receiving AA and ENZA. Patients who switched from AA to ENZA or vice versa were included in the group of the first product they received and then censored at the point of treatment change.
Statistical analyses
Baseline demographic and clinical data were summarised descriptively. New-onset or worsening diabetes was analysed using the reduced Cox regression model (Supplementary methods).
Medians, hazard ratios (HRs), and 95% confidence intervals (CIs) were reported for all models. Treatment persistence was assessed using Kaplan–Meier plots, and differences were analysed using the log-rank test. The duration of follow-up was not adjusted for treatment exposure. Number needed to harm (NNH) analysis was performed, defined as the number of patients who needed to be treated with AA for an additional patient to experience new-onset or worsening T2DM compared with those treated with ENZA. The intention-to-treat (ITT) population was used to evaluate the results; an on-treatment analysis was also performed.
Results
Patients
Of 1491 patients identified, 1382 patients met the eligibility criteria and were included in the final analysis (Supplementary Fig. 1). A total of 826 patients (59.8%) were prescribed ENZA, and 556 patients (40.2%) were prescribed AA; 1049 patients (75.9%) did not have baseline T2DM, while 333 patients (24.1%) did. Most baseline demographic and clinical characteristics were similar between the groups. However, patients in the ENZA group had a numerically higher rate of predisposing factors for T2DM (such as CV comorbidities, obesity, and smoking) than did those in the AA group (Fig. 1 and Supplementary Table 1).
Fig. 1.

Baseline clinical and demographic characteristics of the study population. *The proportion of patients with missing values was 23.8%, 13.6%, and 74.0% for LDL-C, HDL-C, and TC, respectively. AA, abiraterone acetate; AAB, Asian/Asian British; BACBB, Black/African/Caribbean/Black British; BMI, body mass index; ENZA, enzalutamide; HbA1c, haemoglobin A1C; HDL-C, high-density lipoprotein cholesterol; LDL-C, low-density lipoprotein cholesterol; TC, total cholesterol
Primary endpoint: new-onset or worsening T2DM
In the overall population, 84 patients (6.1%) met the primary endpoint after a median follow-up of 432 days (AA: 42 patients [7.6%]; ENZA: 42 patients [5.1%]) (Table 1). The cumulative incidence of the primary endpoint in the overall population at 6, 12, 24, and 36 months was 2.4%, 5.2%, 8.9%, and 10.7%, respectively. The cumulative incidence was higher in patients receiving AA than ENZA (HR: 1.8; 95% CI: 1.4–2.7; P = 0.0101) (Table 1; Fig. 2a, and Supplementary Fig. 2).
Table 1.
New-onset and/or worsening T2DM: primary and exploratory endpoints
| ENZA | AA | Total | |
|---|---|---|---|
| ITT analysis | |||
| Primary endpoint | n = 826 | n = 556 | N = 1382 |
| New-onset or worsening T2DM events, n (%) | 42 (5.1) | 42 (7.6) | 84 (6.1) |
| Cumulative incidence (number at risk), n (%) | |||
| 6 months | 651 (1.3) | 404 (4.0) | 1055 (2.4) |
| 12 months | 472 (3.4) | 272 (7.9) | 744 (5.2) |
| 24 months | 230 (7.6) | 134 (10.7) | 364 (8.9) |
| 36 months | 111 (9.4) | 63 (12.6) | 174 (10.7) |
| Reduced Cox HR (95% CI); P value | ref | 1.8 (1.4–2.7); 0.0101 | - |
| NNH | ref | 40 | - |
| Exploratory endpoints | |||
| Patients without T2DM at baseline | n = 609 | n = 440 | N = 1049 |
| Patients with new-onset T2DM, n (%) | 24 (3.9) | 26 (5.9) | 50 (4.8) |
| Cumulative incidence (number at risk), n (%) | |||
| 6 months | 488 (0.7) | 326 (2.5) | 814 (1.4) |
| 12 months | 352 (2.3) | 224 (6.2) | 576 (3.9) |
| 24 months | 172 (6.3) | 107 (8.7) | 279 (7.3) |
| 36 months | 78 (7.0) | 48 (9.9) | 126 (8.2) |
| Reduced Cox HR (95% CI); P value | ref | 1.9 (1.0–3.7); 0.0658 | - |
| NNH | ref | 50 | - |
| Patients with T2DM at baseline | n = 217 | n = 116 | N = 333 |
| Patients with worsening T2DM, n (%) | 18 (8.3) | 16 (13.8) | 34 (10.2) |
| Cumulative incidence (number at risk), n (%) | |||
| 6 months | 163 (3.0) | 78 (10.0) | 241 (5.4) |
| 12 months | 120 (6.5) | 48 (14.6) | 168 (9.2) |
| 24 months | 58 (11.6) | 27 (18.6) | 85 (14.0) |
| 36 months | 33 (15.8) | 15 (22.7) | 48 (18.2) |
| Reduced Cox HR (95% CI); P value | ref | 1.6 (1.0–2.8); 0.0868 | - |
| NNH | ref | 18 | - |
| On-treatment analysis | |||
| Primary endpoint | n = 826 | n = 556 | N = 1382 |
| New-onset or worsening T2DM events, n (%) | 13 (1.4) | 20 (3.6) | 33 (2.4) |
| Reduced Cox HR (95% CI); P value | ref | 2.6 (1.3–5.3); 0.0137 | - |
| NNH | ref | 49 | - |
| Exploratory endpoints | |||
| Patients without T2DM at baseline | n = 609 | n = 440 | N = 1049 |
| New-onset T2DM, n (%) | 7 (1.1) | 12 (2.7) | 19 (1.8) |
| Reduced Cox HR (95% CI); P value | ref | 2.4 (1.0–6.1); 0.064 | - |
| NNH | ref | 63 | - |
| Patients with T2DM at baseline | n = 217 | n = 116 | N = 333 |
| Worsening T2DM, n (%) | 6 (2.8) | 8 (6.9) | 14 (4.2) |
| Reduced Cox HR (95% CI); P value | ref | 2.8 (1.0–8.2); 0.0536 | - |
| NNH | ref | 24 | - |
AA: abiraterone acetate; ADT: androgen-deprivation therapy; CI: confidence interval; ENZA: enzalutamide; HR: hazard ratio; ITT: intention to treat; NNH: number needed to harm; T2DM: type 2 diabetes mellitus; ref: reference
Fig. 2.
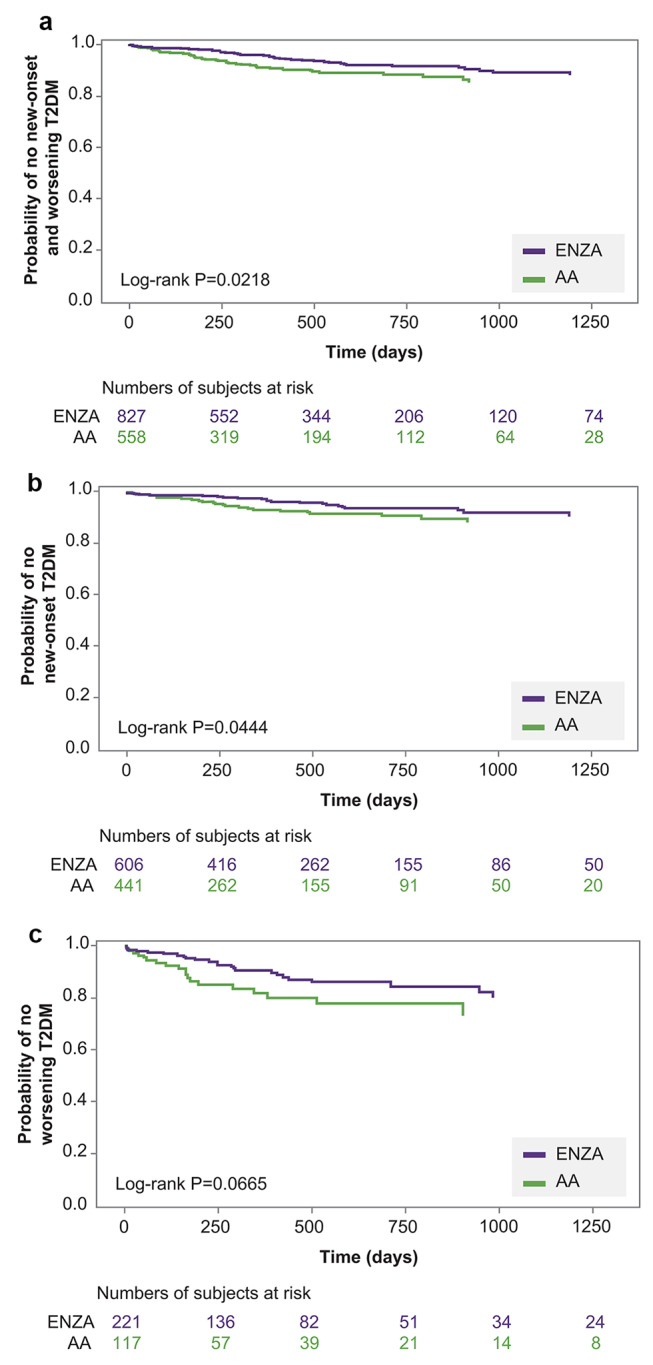
Kaplan–Meier curve of new-onset and worsening T2DM. a Primary endpoint: New-onset or worsening T2DM. b Exploratory endpoint: New-onset T2DM. c Exploratory endpoint: Worsening T2DM. AA, abiraterone acetate; ENZA, enzalutamide; T2DM, type 2 diabetes mellitus
Secondary endpoints: treatment exposure and persistence
Patients on ENZA had longer median durations of treatment (5.4 months vs. 4.6 months) and follow-up (14.6 months vs. 13.5 months) compared with those on AA. Patients without T2DM at baseline had a longer duration of follow-up than those with T2DM at baseline (14.5 months vs. 13.6 months). The trend of longer treatment exposure in patients receiving ENZA compared with AA remained when treatment persistence was considered (Supplementary Table 2).
Exploratory endpoints
Irrespective of T2DM status at baseline, a larger proportion of patients on AA developed new-onset or worsening T2DM compared with those on ENZA (Table 1). The cumulative incidence of new-onset T2DM was higher at all timepoints in patients receiving AA than ENZA (Table 1; Fig. 2). There was a greater likelihood of a new-onset and/or worsening diabetes event in patients receiving AA than those receiving ENZA (Table 1). The on-treatment analysis also showed a similar trend of an increased risk of new-onset or worsening T2DM with AA versus ENZA (Table 1).
NNH analysis
In the ITT population, the NNH was 40 overall, 50 in patients without baseline T2DM, and 18 in patients with baseline T2DM (Table 1).
Discussion
In the current study, the incidence and likelihood of new-onset or worsening T2DM was greater in patients who received AA than in those who received ENZA, both of which are ARPIs used for the treatment of mCRPC. Patients receiving AA had a shorter median duration of follow-up than those receiving ENZA, and despite this unadjusted difference, the latter were at a lower risk of new-onset or worsening T2DM.
Patients with advanced PC are already at a higher risk for metabolic and CV events due to their advanced age and concomitant use of ADT [18]. Given the high prevalence of diabetes (13–19%) in patients with PC, loss of diabetes control could influence overall outcomes in these patients [19, 20]. The metabolic risk might get aggravated by metabolic adverse events related to AA- or ENZA-based regimens affecting overall health status and quality of life. However, growing clinical evidence has shown a lower risk of metabolic events in patients using ENZA than those using AA. In the HEAT randomised trial, which was not primarily designed for this comparison, 12 weeks of treatment with AA was associated with a more unfavourable glycaemic profile than ENZA. This was evidenced by a pronounced increase in HbA1c (3.4 mmol/mol; 95% CI: 2.1–4.8; P = 0.001) and a higher incidence of new-onset T2DM, with eight patients in the AA group developing T2DM compared with none in the ENZA group (n = 85 in each treatment arm) [8]. In a recent national Medicare claims database analysis in the US, the new-onset diabetes risk was higher among patients treated with than without AA (HR: 1.37; 95% CI: 1.08–1.75); in contrast, the risk of diabetes was lower among those treated than not treated with ENZA (HR: 0.66; 95% CI: 0.45–0.98) [18]. Another study in veterans with mCRPC showed that patients with HbA1c ≥ 6.5% had longer survival when treated with ENZA than AA [21]. The worsening of diabetes may be relevant for patients with PC as uncontrolled diabetes can predict poor response to antiandrogens [22]. In a retrospective analysis, progression-free survival was 7 months shorter in patients with uncontrolled diabetes (HbA1c: 7.8–11.6%) than those with controlled diabetes (HbA1c: 4.7–5.9%) [22]. Based on the available evidence, diabetes is mentioned as a common ADT-related CV toxicity for AA, but not for ENZA, in the ESC cardio-oncology guidelines [15]. Findings from the current study align with previous data and ESC guidelines, that is, there is a greater likelihood of new-onset and/or worsening T2DM in patients on AA than ENZA.
A probable underlying reason for the difference in the risk of new-onset or worsening T2DM between AA and ENZA is that patients receiving AA also use prednisone or prednisolone, which may further increase the risk of metabolic side effects. Long-term corticosteroid use is known to be associated with disturbances in glucose metabolism [23, 24]. Moreover, there could be a different mechanism of hyperglycaemia due to differences in the pharmacokinetics or mechanism of action of AA and ENZA. Although both target the androgen receptor pathway, they differ mechanistically: AA inhibits androgen production, while ENZA blocks androgen receptor signalling [25].
In a previous study in veterans with mCRPC, the median treatment duration was longer for ENZA than for AA (11.4 vs. 8.6 months, P < 0.001). Overall survival was also higher among patients on ENZA than those on AA (23.2 vs. 20.5 months, P < 0.001) [26]. Similarly, in the present study, the median treatment duration was longer in patients on ENZA than those on AA, despite a numerically higher proportion of patients in the ENZA group having risk factors for CV disease, such as obesity, diabetes, current/ex smoking status, and non-White ethnicity. This may suggest a selection bias for patients prescribed AA, as they might have a lower risk of T2DM at baseline, which makes the results of this study even more relevant. It also suggests that even in patients with more factors predisposing them to T2DM, the safety and tolerability of ENZA allow for a longer treatment duration than AA. However, this needs to be substantiated in further studies in earlier disease settings, such as metastatic hormone-sensitive PC (mHSPC), with a longer treatment duration.
The findings of this study have important implications for patients with advanced PC. The NNH for new-onset or worsening T2DM was 50 in patients without baseline T2DM but a substantially lower 18 in patients with baseline T2DM. These findings are clinically relevant and may be impactful on a healthcare system level due to high resource use for T2DM in England [27]. Moreover, the use of AA and ENZA continues to evolve, with both now indicated for use in addition to ADT in metastatic castration-sensitive PC, and ENZA is indicated in non-metastatic castration-resistant PC [18]. In the US, ENZA is also approved for high-risk biochemically recurrent PC after local therapy with curative intent [28]. This could lead to treatment exposure of a larger population and for a longer duration. It remains to be elucidated whether the difference in the risk of new-onset or worsening T2DM seen even at a treatment duration of ~ 5 months in this study holds true in patients with mHSPC who receive treatment for longer durations. With the expanded use, the potential increase in non-PC morbidity, like T2DM, should be considered in the risk–benefit discussion during treatment-related decision-making.
The results of this study should be interpreted with caution due to limitations common to any administrative database study, such as missing information and lack of randomisation. Because of the time period of the study, it is possible that patients may have received chemotherapy with or without corticosteroids before receiving ENZA or AA. Patients with a previous history of T2DM or common risk factors for T2DM could have potentially been monitored at higher rates than other patients, which may have led to more of these patients being identified as having worsening T2DM. There was poor documentation of ADT and steroid use in the SACT and CPRD databases; therefore, it was not possible to analyse the confounding effects of ADT on event development in this study, although ADT is included in the regimen for both ENZA and AA. Patients had variable lookback periods, so information on previous cancer occurrence might have been missing for some patients. This could have influenced treatment selection and affected exposure and outcomes of interest in the present study. The on-treatment analysis included fewer patients, and the follow-up duration was shorter. It was difficult to attribute the cause of diabetes events to the use of prednisone or prednisolone because of the requirement for abiraterone to be used in combination with steroids. It was neither the intent of nor feasible in our analysis to address the contribution of each component of the AA regimen to the outcomes. Despite these limitations, the current study provides real-world evidence on the incidence of new-onset or worsening T2DM among patients with mCRPC receiving the two most commonly used ARPIs.
In summary, the likelihood of having a new-onset or worsening diabetes event is statistically significantly higher in patients on AA than ENZA, despite the shorter treatment duration for AA. These findings may have implications for treatment selection for mCRPC and need to be evaluated in earlier PC settings, where the treatment duration is likely to be longer with a potentially greater impact.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Author contributions
Snjider, Pranzo, and Martins were involved in the conception and/or design of the work; Sodatonou and Snjider were involved in data acquisition; Sodatonou, Snjider, Chilelli, Pranzo, Martins, Crawley, Bahl, and Rozario performed data analysis; and Sodatonou, Snjider, Chilelli, Pranzo, Martins, Bahl, and Merseburger were involved in data interpretation. All authors had access to the study results, reviewed and revised the manuscript, and approved the final draft submitted for publication.
Funding
This study was funded by Astellas Pharma Inc. Medical writing and editorial assistance were provided by Leena Patel (PhD), Olga Klibanov (PharmD), and Rucha Kurtkoti (MSc) from IQVIA, funded by the study sponsors.
Data availability
Researchers may request access to anonymised participant-level data, trial-level data, and protocols from Astellas-sponsored clinical trials at www.clinicalstudydatarequest.com. For the Astellas criteria on data sharing, see https://clinicalstudydatarequest.com/Study-Sponsors/Study-Sponsors-Astellas.aspx.
Declarations
Ethical approval
The data application/protocol was submitted to and approved by the Independent Scientific Advisory Committee (ISAC) at the Clinical Practice Research Datalink (CPRD), and the linked data were prepared by the CPRD.
Conflict of interest
AB received support for the present publication from Astellas; received payment or honoraria for lectures, presentations, speakers bureaus, publication writing, or educational events from Astellas and Janssen; received research funding to their institution and support for attending meetings and/or travel from Janssen; and participated on an advisory board for Janssen. AC, AP, NR, RS, and KM are full-time employees of Astellas Pharma Europe Ltd., Surrey, UK. HS was a full-time employee of Astellas Pharma Europe Ltd., Surrey, UK, at the time of the study. DC received support for the present publication from Astellas. AM received support for the present publication from Astellas; received grants or contracts, consulting fees, payment, or honoraria for lectures, presentations, speakers bureaus, publication writing, or educational events, as well as support for attending meetings and/or travel from AstraZeneca, Astellas, Bayer, Bristol-Myers Squibb, Ferring, Ipsen, Janssen, EUSAPharm, MSD, Merck Serono, Novartis, Takeda, Teva, Pfizer, Recordati, and Roche; and holds leadership or fiduciary roles in the EAU and DGU boards of directors.
Footnotes
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
References
- 1.Sung H, Ferlay J, Siegel RL et al (2021) Global cancer statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin 71:209–249. 10.3322/caac.21660 [DOI] [PubMed] [Google Scholar]
- 2.Cancer Research UK Prostate cancer statistics. https://www.cancerresearchuk.org/health-professional/cancer-statistics/statistics-by-cancer-type/prostate-cancer#heading-Zero. Accessed 18 December 2023
- 3.Cancer Research UK Survival of prostate cancer. https://www.cancerresearchuk.org/about-cancer/prostate-cancer/survival. Accessed 18 December 2023
- 4.Yang X, Chen H, Xu D et al (2022) Efficacy and safety of Androgen Deprivation Therapy (ADT) combined with modified docetaxel chemotherapy versus ADT combined with standard docetaxel chemotherapy in patients with metastatic castration-resistant prostate cancer: study protocol for a multicentre prospective randomized controlled trial. BMC Cancer 22:177. 10.1186/s12885-022-09276-y [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.National Institute for Health and Care Excellence Abiraterone for treating metastatic hormone-relapsed prostate cancer before chemotherapy is indicated. Technology appraisal guidance [TA387]. https://www.nice.org.uk/guidance/ta387/chapter/1-Recommendations. Accessed 18 December 2023
- 6.National Institute for Health and Care Excellence Enzalutamide for treating metastatic hormone-relapsed prostate cancer before chemotherapy is indicated. Technology appraisal guidance [TA377]. https://www.nice.org.uk/guidance/ta377/chapter/8-Sources-of-evidence-considered-by-the-Committee. Accessed 18 December 2023
- 7.Lin Y-T, Huang Y-C, Liu C-K, Lee T-S, Chen M, Chien Y-N (2021) Treatment-emergent co-morbidities and survival in patients with metastatic castration-resistant prostate cancer receiving abiraterone or enzalutamide. Front Pharmacol 12:669236 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Ternov KK, Sønksen J, Fode M et al (2022) Fatigue, health-related quality-of-life and metabolic changes in men treated with enzalutamide or abiraterone acetate plus prednisone for metastatic castration-resistant prostate cancer: a randomised clinical trial (HEAT). Eur J Cancer 171:75–84 [DOI] [PubMed] [Google Scholar]
- 9.Bosco C, Crawley D, Adolfsson J, Rudman S, Van Hemelrijck M (2015) Quantifying the evidence for the risk of metabolic syndrome and its components following androgen deprivation therapy for prostate cancer: a meta-analysis. PLoS ONE 10:e0117344. 10.1371/journal.pone.0117344 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Keating NL, Liu P-H, O’Malley AJ, Freedland SJ, Smith MR (2014) Androgen-deprivation therapy and diabetes control among diabetic men with prostate cancer. Eur Urol 65:816–824. 10.1016/j.eururo.2013.02.023 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Tsai H-T, Keating NL, Van Den Eeden SK et al (2015) Risk of diabetes among patients receiving primary androgen deprivation therapy for clinically localized prostate cancer. J Urol 193:1956–1962. 10.1016/j.juro.2014.12.027 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Crawley D, Chamberlain F, Garmo H (2018) A systematic review of the literature exploring the interplay between prostate cancer and type two diabetes mellitus. Ecancermedicalscience 12:802 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.United States Food and Drug Administration Zytiga prescribing information. https://www.accessdata.fda.gov/drugsatfda_docs/label/2011/202379lbl.pdf. Accessed 18 December 2023
- 14.European Medicines Agency EMA label for abiraterone acetate. https://www.ema.europa.eu/en/documents/product-information/abiraterone-krka-epar-product-information_en.pdf. Accessed 18 December 2023
- 15.Lyon AR, López-Fernández T, Couch LS (2022) 2022 ESC guidelines on cardio-oncology developed in collaboration with the European Hematology Association (EHA), the European Society for Therapeutic Radiology and Oncology (ESTRO) and the International Cardio-Oncology Society (IC-OS). Eur Heart J 43:4229–4361 [DOI] [PubMed] [Google Scholar]
- 16.National Institute for Health and Care Excellence Type 2 diabetes in adults: management. NICE guideline [NG28]. https://www.nice.org.uk/guidance/ng28. Accessed 18 December 2023
- 17.Public Health England Calculating treatment duration for oral drugs: Cancer Drugs Fund methodology document. PHE gateway number: GW-215. https://www.chemodataset.nhs.uk/view?rid=280. Accessed 18 December 2023
- 18.Lai LY, Oerline MK, Caram ME (2022) Risk of metabolic and cardiovascular adverse events with abiraterone or enzalutamide among men with advanced prostate cancer. J Natl Cancer Inst 114:1127–1134 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Rivera-Arkoncel MLC, Sagun M, Arkoncel FR, Jimeno C, Lapitan MC (2014) Prevalence of diabetes mellitus and metabolic syndrome in prostate cancer patients given androgen deprivation therapy. J ASEAN Fed Endocr Soc 29:42 [Google Scholar]
- 20.Edwards BK, Noone AM, Mariotto AB (2014) Annual Report to the Nation on the status of cancer, 1975-2010, featuring prevalence of comorbidity and impact on survival among persons with lung, colorectal, breast, or prostate cancer. Cancer 120:1290–1314 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Govindan S, Cheranda N, Riekhof F, Luo S, Schoen MW (2024) Effect of BMI and hemoglobin A1c on survival of veterans with metastatic castration-resistant prostate cancer treated with abiraterone or enzalutamide. Prostate 84:245–253 [DOI] [PubMed] [Google Scholar]
- 22.Karantanos T, Karanika S, Gignac G (2016) Uncontrolled diabetes predicts poor response to novel antiandrogens. Endocr Relat Cancer 23:691–698 [DOI] [PubMed] [Google Scholar]
- 23.Rice JB, White AG, Scarpati LM, Wan G, Nelson WW (2017) Long-term systemic corticosteroid exposure: a systematic literature review. Clin Ther 39:2216–2229 [DOI] [PubMed] [Google Scholar]
- 24.Schultz NM, Penson DF, Wilson S (2020) Adverse events associated with cumulative corticosteroid use in patients with castration-resistant prostate cancer: an administrative claims analysis. Drug Saf 43:23–33 [DOI] [PubMed] [Google Scholar]
- 25.Ternov KK, Sønksen J, Fode M (2019) Fatigue, quality of life and metabolic changes in men treated with first-line enzalutamide versus abiraterone plus prednisolone for metastatic castration-resistant prostate cancer (HEAT): a randomised trial protocol. BMJ Open 9:e030218 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Schoen MW, Carson KR, Eisen SA (2023) Survival of veterans treated with enzalutamide and abiraterone for metastatic castrate resistant prostate cancer based on comorbid diseases. Prostate Cancer Prostatic Dis 26:743–750 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Wang H-I, Han L, Jacobs R (2022) Healthcare resource use and costs for people with type 2 diabetes mellitus with and without severe mental illness in England: longitudinal matched-cohort study using the clinical Practice Research Datalink. Br J Psychiatry 221:402–409 [DOI] [PubMed] [Google Scholar]
- 28.United States Food and Drug Administration FDA approves enzalutamide for non-metastatic castration-sensitive prostate cancer with biochemical recurrence. https://www.fda.gov/drugs/resources-information-approved-drugs/fda-approves-enzalutamide-non-metastatic-castration-sensitive-prostate-cancer-biochemical-recurrence. Accessed 07 August 2024
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Data Availability Statement
Researchers may request access to anonymised participant-level data, trial-level data, and protocols from Astellas-sponsored clinical trials at www.clinicalstudydatarequest.com. For the Astellas criteria on data sharing, see https://clinicalstudydatarequest.com/Study-Sponsors/Study-Sponsors-Astellas.aspx.