

Abstract
Background
Obesity is a significant global health issue. Metabolic and bariatric surgery (MBS) is the gold standard in the treatment of obesity due to its proven effectiveness and safety in the short and long term. However, MBS is not suitable for all patients. Some individuals are at high surgical risk or refuse surgical treatment, while others do not meet the criteria for MBS despite having obesity-related comorbidities. This gap has driven the development of endoscopic solutions like endoscopic sleeve gastroplasty (ESG), which offers a less invasive alternative that preserves organ function and reduces risks. A recent IFSO International Delphi consensus study highlighted that multidisciplinary experts agree on the utility of ESG for managing obesity in patients with class I and II obesity and for those with class III obesity who do not wish to pursue or qualify for MBS. This IFSO Bariatric Endoscopy Committee position statement aims to augment these consensus statements by providing a comprehensive systematic review of the evidence and delivering an evidence-based position on the value of ESG within the spectrum of obesity management.
Methods
A comprehensive systematic review followed the Preferred Reporting Items for Systematic Reviews and Meta-analyses (PRISMA) and Cochrane guidelines.
Results
Systematic Review: The systematic review included 44 articles encompassing 15,714 patients receiving ESG. The studies varied from large case series to cohort studies and a randomized controlled trial (RCT). The mean baseline BMI was 37.56 kg/m2. The review focused on weight loss outcomes and safety data.
Meta-analysis:
| Time point | Mean %EWL | Mean %TBWL |
|---|---|---|
| 6 months | 48.04 | 15.66 |
| 12 months | 53.09 | 17.56 |
| 18 months | 57.98 | 16.25 |
| 24 months | 46.57 | 15.2 |
| 36 months | 53.18 | 14.07 |
| 60 months | 45.3 | 15.9 |
These results demonstrate significant weight loss following ESG.
Safety: The pooled serious adverse event (SAE) rate was 1.25%. This low rate of SAEs indicates that ESG is a relatively safe procedure.
Quality of Evidence: The quality of evidence from the included observational studies was assessed as very low, primarily due to the inherent limitations associated with observational study designs, such as potential biases and lack of randomization. In contrast, the quality of evidence from the single randomized controlled trial was rated as MODERATE, reflecting a more robust study design that provides a higher level of evidence despite some limitations.
Conclusions
The IFSO Bariatric Endoscopy Committee, after conducting a comprehensive systematic review and meta-analysis, endorses endoscopic sleeve gastroplasty (ESG) as an effective and valuable treatment for obesity. ESG is particularly beneficial for patients with class I and II obesity, as well as for those with class III obesity who are not suitable candidates for metabolic bariatric surgery. ESG provides significant weight loss outcomes and demonstrates a favorable safety profile with a low rate of serious adverse events. Despite the limitations of the included observational studies, the randomized controlled trial included in the analysis reinforces the efficacy and safety of ESG and provides an evidence-based foundation for the position statement. Thus, the IFSO position statement supports and provides an evidence base for the role of ESG within the broader spectrum of obesity management.
Keywords: Obesity, Endoscopic Sleeve Gastroplasty, Meta-analysis
Introduction
Obesity rates are galloping, though regional, cultural, and socioeconomic factors contribute to disparities in distribution, prevalence, and incidence across the globe [1]. Still, the World Health Organization (WHO) estimates that 1.9 billion people are overweight, with 650 million having obesity as of 2016 [2]. In the United States, around 40% of the population currently live with obesity [3, 4], and prediction models estimate that this number will increase to 51% by 2030 [5]. After unsuccessful non-invasive therapies, metabolic and bariatric surgery (MBS) is the gold-standard treatment to address moderate to severe obesity. Most recently, it has also been proposed for mild obesity if it is associated with refractory metabolic diseases [6]. MBS is effective and safe in the short and long term, promoting sustained weight loss and reliable reduction in all-cause mortality rates [7].
Data show that MBS procedures have increased over decades [8, 9]. However, the rate of obesity growth is outpacing the growth in surgical interventions [10]. In addition, several patients refuse surgical treatment, others are at high surgical risk, and some suffer from overweight or mild obesity but are still not eligible for MBS. Nevertheless, obesity-related complications increase in states of overweight and mild obesity [11]. Altogether, a gap between the needs of patients with obesity and what we can offer in terms of medical and surgical interventions exists.
This unmet need has driven the development of endoscopic solutions to address obesity, particularly when MBS is not feasible or indicated. Endoscopic bariatric therapies offer several advantages, including organ preservation, an improved risk profile, reduced healthcare utilization, and decreased burden of compliance on the patient. These benefits potentially enable the scalability of procedural offerings to effectively combat excess adiposity. Endoscopic sleeve gastroplasty (ESG) is one such solution that has gained global adoption from patients and providers in the past few years. In its current clinically adopted and regulatory approved form (Fig. 1) [12], ESG employs the Apollo Overstitch™ platform (Boston Scientific, Marlborough, MA, USA)—a full-thickness endoscopic suturing device to create apposition of the anterior against the posterior wall of the stomach, passing through the greater curvature [13, 14]. The Overstitch™ platform is currently the only US FDA–approved endoscopic suturing device for an obesity indication. Suturing starts at the transition between the gastric body and antrum, moving proximally toward the fundus, which is typically partially reduced with the preservation of a small pouch to allow fundal accommodation. Thus, it tubularizes the gastric body, altering satiety and satiation [15]. Although different stitching patterns have been proposed and discussed [16–18], the above-mentioned anatomic principles are consistent across centers and providers; thus, the procedure is clinically mature, homogeneous, and reproducible [19].
Fig. 1.
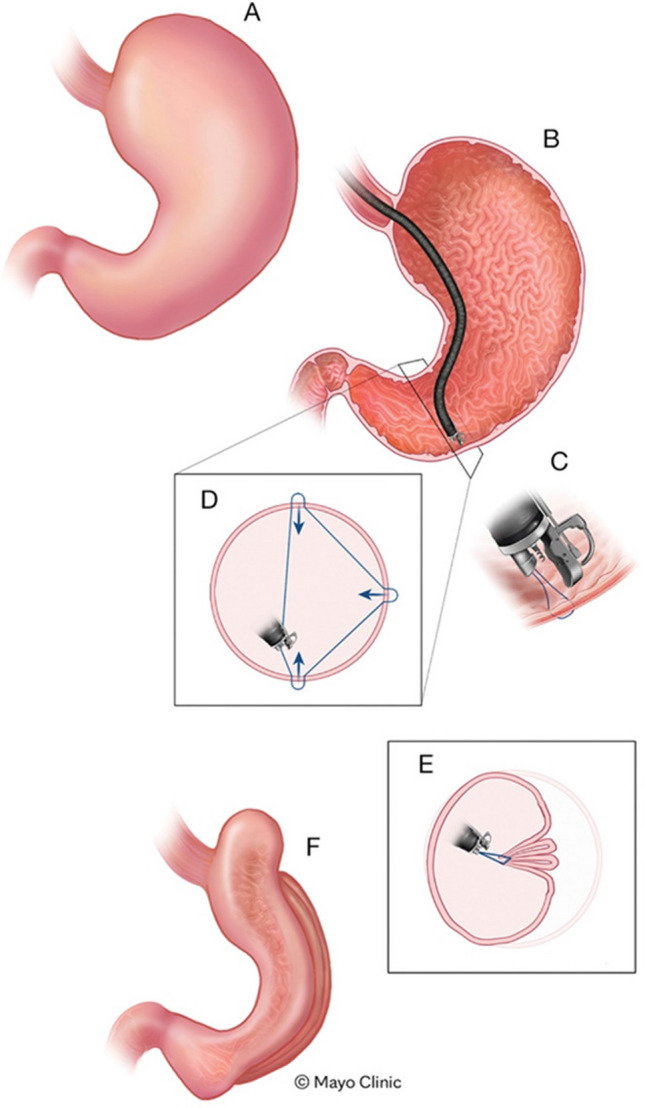
Schematic representation of the endoscopic sleeve gastroplasty procedure
The evidence concerning the efficacy and safety of the ESG has been mounting. More than 200 international medical articles have been published on this topic, with study designs varying from large cases series [20] to cohort studies [21] and, more recently, also includes an open-label, multicenter randomized trial with 24 months follow-up [22]. The procedure is currently employed clinically in all continents, and more than 40,000 clinical procedures have been performed to date. A recent IFSO International Delphi consensus conference highlighted that multidisciplinary experts agree on the utility of ESG for managing obesity in patients with class I and II obesity and for those with class III obesity who do not wish to pursue or qualify for MBS in the context of a comprehensive multidisciplinary obesity program [23]. This IFSO Bariatric Endoscopy Committee position statement aims to augment these consensus statements by providing a comprehensive systematic review of the evidence and delivering an evidence-based position on the value of ESG within the spectrum of obesity care.
Methods
This position statement is derived after a comprehensive systematic review to retrieve all available data on the outcomes of ESG. All the Preferred Reporting Items for Systematic Reviews and Meta-analyses (PRISMA) [24] and Cochrane Handbook for Systematic Reviews of Interventions [25] guidelines were rigorously followed for this position statement’s systematic review and meta-analysis portion. Two independent researchers (VOB and NJ) conducted all literature searches and a third independent reviewer adjudicated discrepancies. After defining the eligibility criteria, final inclusion was determined by consensus with two additional researchers (RK and BAD). One researcher collected data from the included studies using a standardized shared spreadsheet, and another independently validated the data extraction. Methodologists’ names and affiliations are in the “Acknowledgements” section.
The risk of bias in the included studies was assessed using the Joanna Briggs Institute Critical Appraisal checklist for case series [26], the New-Castle Ottawa scale for cohort studies [27], and both JADAD score [28] and a modified Cochrane Collaboration Risk of Bias tool (available from https://www.ncbi.nlm.nih.gov/books/NBK132494/bin/appf-fm1.pdf).
We used the Review Manager (Version 5.4, the Cochrane Collaboration, 2020) for pooling comparative data and the Comprehensive Meta-analysis software (Version 4, Biostat, Englewood, NJ, USA, 2022) to pool non-comparative data. Means and standard deviations (SDs) were estimated from medians and ranges based on previously validated mathematical formulas [29]. The estimation of standard deviation based on interquartile ranges, or 95% confidence interval (CI), followed the instructions in the Cochrane Handbook (Chapter 06, Section 6–5-2) [25]. If the article did not provide any measure for dispersion or sample size, we attempted to obtain them by emailing the authors. If unsuccessful, we proceeded with data input based on the SD of articles with similar sample sizes and time points (per Cochrane Handbook’s guidance).
Continuous variables were expressed preferably as means and standard deviation, while categorical ones were expressed as rates or frequencies. A p-value < 0.05 was considered statistically significant for a 95%CI. As a measure of effect, we employed main difference (MD) with fixed-effect mode analysis to compare data. Then, we assessed for heterogeneity among studies with the Higgins test (I2). I2 higher than 50% indicated high heterogeneity, and sensitivity analyses utilizing forest plots were undertaken to assess for outliers. If no true outliers were identified, the heterogeneity was considered true, and we switched from fixed to random-effect mode analysis to mitigate its impact on the summary estimate.
Using the results from the critical appraisal/risk of bias assessment and the meta-analysis, we evaluated the quality of the current evidence using the Grading of Recommendations, Assessment, Development, and Evaluations (GRADE) approach [30]. This standardized methodology analyzes data per outcome and uses several aspects of the studies (study design, risk of bias, imprecision, inconsistency, indirectness, publication bias, magnitude of effect, dose–response gradient, impact of residual confounding on the summary estimate) to classify the quality of the pooled evidence into 4 different categories: VERY LOW, LOW, MODERATE, and HIGH. This assessment demonstrates our certainty on how close the actual effect is to the effect estimated in our meta-analysis. All the data was input into the GRADEpro GDT online software (GRADEpro Guideline Development Tool, McMaster University, and Evidence Prime, 2022) for analysis and generation of the overall quality of evidence.
Finally, considering all the information gathered from the systematic literature review and meta-analysis, balancing the benefits and harms of the therapy, clinicians’ values and preferences, resource utilization, and cost-effectiveness, the committee determined the final position statement and level of support.
Results
Safety and Efficacy of ESG
Outcomes of ESG
Systematic Review
Two independent researchers (VOB and NJ) ran separate literature searches assessing eligible studies. We searched MEDLINE (PubMed), EMBASE, and gray literature from January 1, 2013 (the year ESG was described), to October 1, 2022. The final strategy was as follows:
MEDLINE (PubMed): (total weight loss) OR (total body weight loss) OR (excess weight loss) OR (absolute weight loss) OR (excess body weight loss) OR (responders rate) OR (adverse event) OR (BMI reduction) OR (BMI decrease) OR (complication) AND (endoscopy) OR (endoscopic) OR (transoral*)OR (peroral*)OR (incisionless) AND (sleeve) OR ( overstitch) OR (gastroplasty) OR (gastric plication) OR (gastric imbrication) AND (overweight) OR (obesity) AND ("2013/01/01"[Date—Publication]: "3000"[Date—Publication])
EMBASE: endoscopic AND sleeve AND gastroplasty OR (apollo AND overstitch) AND [embase]/lim NOT ([embase]/lim AND [medline]/lim) AND ('article'/it OR 'article in press'/it OR 'conference review'/it OR 'note'/it OR 'review'/it)
The eligibility criteria included:
Articles published online from 1 Jan. 2013 until 1 Oct. 2022 (last search update);
ESG performed with the Apollo Overstitch device (no restriction as to stitching pattern);
No language restriction;
Full-text articles only;
Study designs case series with sample ≥ 10, cohort studies, case–control studies, and randomized trials. For the non-comparative meta-analysis, we extracted results from the ESG cohort from comparative studies;
To avoid overestimating the real sample, only the most recent or the most representative (larger sample) study was considered for each center if repeated data was suspected;
Studies describing outcomes at predetermined time points: 6, 12, 18, 24, 36, > 36 months;
Studies reporting efficacy and/or safety data.
The initial search retrieved 3015 records. After screening titles and abstracts, 100 articles were selected for full-text assessment. Finally, 44 articles were included in the qualitative and quantitative analyses. Figure 2 shows the screening and inclusion/exclusion flowchart.
Fig. 2.

PRISMA flowchart for the literature screening and inclusion/exclusion process for the overall outcomes of ESG (non-comparative analysis)
Descriptive Analysis
-
Baseline and Demographic Data
Among the 44 articles, we identified 29 case series, 14 cohort studies, and 1 randomized controlled trial (RCT). Among the cohort studies, 7 compared ESG to LSG, 1 compared ESG to lifestyle intervention alone, 1 compared ESG versus ESG plus anti-obesity medication (liraglutide), 2 compared ESG and intragastric balloons, and 3 compared ESG cohorts with different stitching patterns. Table 1 summarizes the overall and baseline data of the qualitative analysis of the included studies.
Among the 44 articles, the total sample included 49,848 patients (15,714 ESG and 34,134 controls, including LSG, laparoscopic adjustable gastric banding, and IGB). At baseline, the mean age and BMI were 44.24 (SE 1.405, 95%CI 41.48–46–99, 41 articles n = 13,562) and 37.56 (SE 0.45 95%CI 36.66–38.46, 42 articles, n = 13,876), respectively. Most patients were female (11,449 females, 83.2% and 2304 males, 16.8%, 42 articles, n = 13,753).
Table 1.
Baseline data of the 44 articles included in the meta-analysis of the ESG outcomes
| Author (year) | Study design | Single vs. multicenter | Retrospective vs. prospective | Population (total sample) | Intervention (n) | Comparison (n) | Observations | Inclusion criteria (BMI) | Age | Sex | Mean baseline BMI (kg/m2) | Type II Diabetes |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Abu Dayyeh, B. K., et al. [31] | Case series | Single center | Prospective | 25 | ESG | - | Study of gastric physiology | BMI > 30 and < 40 | 47.6 (10) | 21 women | 35.5 (2.6) | 1 |
| Abu Dayyeh, B. K., et al. [22] | Randomized clinical trial | 9 centers | Prospective | 209 | ESG (85) | Lifestyle intervention (124) | Open-label FDA-regulated trial | BMI > 30 and < 40 | 47.3 (9.3) ESG and 45.7 (10) lifestyle intervention | 68 (88%) ESG and 91 (84%) lifestyle intervention | 35.5 (2.6) ESG and 35.7 (2.6) lifestyle intervention | 18 ESG and 36 lifestyle intervention |
| Alqahtani, A., et al. [20] | Case series | Single center | Prospective | 1000 | ESG | - | - | Ineligible for or refuse bariatric surgery | 34.4 (9.5) | 897 (89.7) women | 33.3 (4.5) | 17 |
| Alqahtani, A., et al. [32] | Case series | Single center | Prospective | 109 | ESG | - | Patients aged < 21 years old | BMI > 120% of the 95th percentile | 17.6 (2.2) | 99 (91.7) women | 33 (4.7) | NR |
| Alqahtani, A. R., et al. [33] | Cohort (propensity score-matched) | Single center | Retrospective | 6036 | ESG (3018) | LSG (3018) | - | BMI > 27.5 | 33.8 (9.6) ESG and 33.9 (9.7) LSG | 2686 (89%) women for both groups | 32.5 (3.1) ESG and 32.9 (3.5) LSG | 112 ESG |
| Asokkumar, R., et al. [34] | Case series | Single center | Prospective | 35 | ESG | - | - | BMI > 27.5 | 43.6 (11.3) | 20 (52.7%) women | 34 (4.9) | 8 (23%) |
| Badurdeen, D., et al. [35] | Cohort (propensity score-matched) | 3 centers | Prospective | 52 | ESG (26) | ESG + Liraglutide (26) | - | BMI > 27 | 41.15 (10.64) ESG and 40.65 (8.69) ESG + Liraglutide | 16 women ESG and 17 women ESG + Liraglutide | 35.56 (1.68) ESG and 35.83 (2.33) ESG + Liraglutide | 16 (8 and 8) |
| Barrichello, S., et al. [36] | Case series | 7 centers | Retrospective | 193 | ESG | - | - | BMI > 25 | 42.3 (9.6) | 148 women | 34.11 (2.97) | NR |
| Bhandari, M., et al. [37] | Case series | Single center | Retrospective | 53 | ESG | - | - | BMI > = 28 | 40.54 (13.79) | 43 (81.1%) | 34.78 (5.20) | 10 |
| Callahan, Z. M., et al. [38] | Case series | Single center | Retrospective | 10 | ESG | - | Study on GI tract suturing including 10 ESG cases | NR | 50.2 (12.2) | 10 women | NR | NR |
| Carr, P., et al. [39] | Cohort | Single center | Prospective | 61 | ESG (16) | LSG (45) | - | BMI > 26 with comorbidity or BMI > 30 | 41.4 (10.4) vs 40.4 (9.0) | 31 women (57.4%) ESG and 59 (71.1%) LSG | 35.5 (5.2) vs 40.7 (5.6) | 0 ESG and 2 LSG |
| Cheskin, L. J., et al. [40] | Cohort (propensity score-matched) | Single center | Retrospective | 386 | ESG (105) | Lifestyle intervention (281) | - | NR | 47.58 (11.97) ESG and 48.17 (12.18) Lifestyle intervention | 75 (71.42%) women ESG and 189 (67.2%) women Lifestyle intervention | 40.5 (7.89) ESG and 39.85 (7.62) lifestyle intervention | NR |
| Espinet-Coll, E., et al. [41] | Case series | Single center | Prospective | 38 | ESG | - | Focus on persistence of sutures | BMI > 27 | 47 (5.5)* | 30 women | 37.6 (3)* | NR |
| Espinet-Coll, E., et al. [42] | Cohort | 2 centers | Retrospective | 88 | ESG (standard stitching pattern = "TBp") | ESG with different stitching patterns ("Lp" and "TMp") | Comparison of 3 different stitching patterns | BMI > 27 | Overall 46.1 (12.3) | 61 women | Overall 39.40 (4.69) | Overall 11 (12.5%) |
| Farha, J., et al. [43] | Cohort | 2 centers | Retrospective | 247 | ESG (98) | ESG with fundal suturing (149) | - | BMI > 30 | 44.9 (9.4) vs 47.2 (11.5) | 84 (85.7%) and 107 (71.8%) | 38.3 (5.6) vs 39.4 (7.3) | Overall 16 |
| Fayad, L., et al. [44] | Cohort | Single center | Retrospective | 137 | ESG (54) | LSG (83) | - | NR | 48 (12) ESG and 47.75 (6.16) LSG* | 31 women (57.4%) ESG and 59 (71.1%) LSG | 43.07 (8.85) ESG and 44.12 (5.78) LSG* | 3.7% ESG and 20.48% LSG |
| Fayad, L., et al. [45] | Cohort | Single center | Retrospective | 105 | ESG (58) | IGB (47) | - | BMI > 27 for IGB and BMI > 30 for ESG | 48.2 (11.8) ESG and 47.7 (12.4) IGB | 34 women (58.6%) ESG and 46 (97.9%) IGB | 41.5 (8.2) ESG and 34.5 (6.7) IGB | 3 (5.2) ESG and 4 (8.5) IGB |
| Fiorillo, C., et al. [46] | Cohort | Single center | Retrospective | 46 | ESG (23) | LSG (23) | Focus on quality of life after 6 months | NR | 41 (2) ESG and 37 (4.5) LSG* | 16 women ESG and 17 LSG | 39.5 (2) ESG and 41 (1.27) LSG* | 2 ESG and 3 LSG |
| Ghoz, H., et al. [47] | Case series | Single center | Retrospective | 20 | ESG | - | Focus on nutritional deficiencies | NR | 46.2 (14.1) | 17 women | 36.4 (4.1) | 2 |
| Glaysher, M. A., et al. [48] | Cohort | Single center | Prospective | 32 | ESG without longitudinal compression (9) | ESG with longitudinal compression (23) | - | BMI > 30 | 45 (12) ESG and 43 (10) ESG with compression | 5 women ESG and 18 ESG with compression | 36.62 (3.72) ESG and 36.42 (3.27) ESG with compression* | NR |
| Graus Morales, J., et al. [49] | Case series | Single center | Prospective | 148 | ESG | - | ESG with modified stitching pattern | BMI > 30 | 41.53 (10) | 121 women | 35.11 (5.5) | NR |
| Gudur, A. R., et al. [50] | Cohort | Multicenter (database) | Retrospective | 36,323 | ESG (6,053) | LSG (30,270) | MBSAQIP database cohort study | - | 47.47 (11.44) and 44.87 (11.94) | 5116 and 24926 women | 40.54 (8.65) and 42.8 (6.17) | 1040 and 5775 |
| Hajifathalian, K., et al. [51] | Case series | Single center | Prospective | 118 | ESG | - | Focus on NAFLD scores | BMI > 30 and NAFLD | 46 (13) | 80 (68%) women | 40 (7) | 35 |
| Hill, C., et al. [52] | Case series | Single center | Prospective | 21 | ESG | - | Focus on learning curve | NR | 47.7 (11.2) | 13 women | 41.8 (8.5) | NR |
| Jagtap, N., et al. [53] | Case series | Single center | Prospective | 26 | ESG | - | Focus on NAFLD scores | BMI > 27.5 and NAFLD | 41.5 (9.58) | 16 women | 36.55 (5.07) | 13 |
| James, T. W., et al. [54] | Case series | Single center | Retrospective | 100 | ESG | - | Non-academic setting | NR | 45 (9) | 86 women | 38.41 (5.44) | 4 |
| Kumar, N., et al. [55] | Case series | Multicenter (NS) | Prospective | 122 | ESG (23 in phase 1, 22 in phase 2, 77 in phase 3) | - | Focus on technical refinement over time | BMI > 30 | Phase 1 37.7 (1.9); Phase 2 39.2 (1.6); Phase 3 41.3 (1.1) | Phase 1 19 women; phase 2 20 women; phase 3 59 women | Phase 1 34.2 (1.1); Phase 2 34.3 (1); Phase 3 36.1 (0.6) | NR |
| Li, R., et al. [56] | Case series | Single center | Prospective | 24 | ESG | - | Focus on high-risk cases | BMI > 50, severe comorbidities, or impenetrable abdomen | 55.6 (9.2) | 6 women | 49.9 (14.4) | 15 |
| Lopez-Nava, G., et al. [57] | Case series | Single center | Retrospective | 435 | ESG | - | BMI > 30 | 48.5 (10.2) | 314 women | 38.9 (5.3) | NR | |
| Lopez-Nava, G., et al. [58] | Cohort | 2 centers | Prospective | 24 | ESG (12) | LSG (12) | Focus on enterohormonal changes | BMI > 30 | 49.3 (2.4) ESG and 50.5 (1.9) LSG | 9 women ESG and 9 women LSG | 38.3 (1.8) ESG and 39.2 (1.5) LSG | 0 ESG and 3 preDM LSG |
| Lopez-Nava, G., et al. [59] | Case series | 3 centers | Prospective | 248 | ESG | - | - | NR | 44.5 (10) | 181 women | 37.8 (5.6) | NR |
| Manos, T., et al. [60] | Case series | Single center | Retrospective | 191 | ESG | - | Single-channel endoscope device (Overstitch SX) | BMI > 30 | 36.9 (no SD) | 173 women | 33.7 (4.18)* | NR |
| Matteo, M. V., et al. [61] | Case series | Single center | Prospective | 18 | ESG | - | Patients > 65 years old | BMI > 30 | 67 (4.5) | 10 women | 41.2 (5.9) | 4 |
| Maydeo, A., et al. [16] | Case series | Single center | Prospective | 58 | ESG | - | Different stitching pattern ("accordion") | BMI > 28 | 42.1 (8.7) | 55 women | 37.88 (5.76) | 17 |
| Mehta, A., et al. [62] | Case series | Single center | Prospective | 50 | ESG | - | Focus on quality of life and mental health | NR | 49.5 (14) | 37 women | 38.5 (5.8) | 9 |
| Neto, M. G., et al. [63] | Case series | 4 centers | Prospective | 233 | ESG | - | - | BMI > 30 and < 40 | 41.1 (10.5) | 170 women | 34.7 (2.6) | 12 |
| Neto, M. G., et al. [64] | Case series | Multicenter (NS) | Retrospective | 1828 | ESG | - | Clinical consensus gathering 47 Brazilian endoscopists | NR | NR | NR | NR | NR |
| Novikov, A. A., et al. [65] | Cohort | Single center | Retrospective | 278 | ESG (91) | LSG (120) and LAGB (67) | - | BMI > 30 | 43.86 (11.26) ESG, 40.71 (11.95) LSG, and 41.94 (13.31) LAGB | 62 women ESG, 94 women LSG, and 54 women LAGB | 38.61 (6.98) ESG, 47.22 (7.84) LG, and 44.98 (6.45) LAGB | 20 ESG, 31 LSG, and 15 LAGB |
| Pizzicannella, M., et al. [66] | Case series | Single center | Prospective | 133 | ESG | - | Focus on durability of sutures and their correlation with weight loss | NR | NR | NR | 43.2 (8.6) | NR |
| Rapaka, B., et al. [67] | Cohort | 2 centers | Prospective | 41 | ESG (23) | IGB (18) | - | NR | 47.69 (5.06) ESG and 41.06 (8.81) IGB | 20 women ESG and 18 IGB | 41.21 (5.38) ESG and 34.5 (4.46) | NR |
| Sarkar, A., et al. [68] | Case series | 6 centers | Retrospective | 91 | ESG | - | Focus on new bariatric endoscopy programs | BMI > 30 | 39.7 (11.6) | 56 women | 38.7 (4.4)* | 46 |
| Sartoretto, A., et al. [69] | Case series | 3 centers | Retrospective | 112 | ESG | - | - | BMI > 27 | 45.1 (11.7) | 77 women | 37.9 (6.7) | 14 |
| Saumoy, M., et al. [70] | Case series | Single center | Prospective | 128 | ESG | - | Focus on learning curve | BMI > 30 | 43.62 (11.37) | 86 women | 38.92 (6.95) | NR |
| Sharaiha, R. Z., et al. [71] | Case series | Single center | Retrospective | 216 | ESG | - | Long-term follow-up | BMI > 30 or > 27 with comorbidities | 46 (13) | 146 women | 39 (6) | 67 |
*Calculated field
Risk of Bias/Critical Appraisal Assessment
All included studies were assessed for their risk of bias using specific tools based on the study design. Case series were evaluated using the Joanna Briggs Institute Critical Appraisal Checklist. Ten items are scored based on the perceived risk, and the scoring is positive. The scale ranges from 0 to 10, with 0 being the highest risk of bias and 10 being the lowest. The included case series (29 articles) had a mean score of 7.5 ± 1.8. Reporting of outcomes, and follow-up, and statistical analyses were the two topics with the worst positive scoring (16/29, 55.2%).
For cohort studies, we employed the New-Castle Ottawa scale that assesses 8 topics for bias. The scale ranges from 0 to 9, with 0 being the highest risk of bias and 9 being the lowest. The 14 included cohort articles scored an average of 6.07 ± 1.43. The selection of a non-exposed cohort and the duration of follow-up were the two topics with the worst scoring, thus most subject to bias (0.42 ± 0.51 and 0.35 ± 0.49).
For the single RCT [22], the JADAD score was 3, which is the maximum score for open-label trials. As to the modified Cochrane risk of bias tool, the trial was at low risk for selection and reporting bias. However, we detected a high risk of other biases: performance, detection, and attrition. The GRADE assessment of the quality of evidence later weighted the impact of those biases. Tables 2, 3, and 4 summarize the assessment of biases for case series, cohorts, and RCT, respectively.
Table 2.
Critical appraisal and risk of bias assessment for the included case series
| CASE SERIES | |||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Author, year | Study design | JBI Critical appraisal checklist domains | |||||||||||
| Articles (n) = 29 | Were there clear criteria for inclusion in the case series | Was the condition measured in a standard, reliable way for all participants included in the case series? | Were valid methods used for identification of the condition for all participants included in the case series? | Did the case series include consecutive participants? | Did the case series have complete inclusion of participants? | Was there clear reporting of the demographics of the participants in the study? | Was there transparent reporting of clinical information of the participants? | Were the outcomes or follow−up results of cases clearly reported? | Was there transparent reporting of the demographic information of the presenting site(s)/clinic(s)? | Was statistical analysis appropriate? | Obs. | Total of "yes" (max=10) | |
| Abu Dayyeh, B. K., et al. [31] | Case series | yes | yes | yes | yes | yes | yes | yes | no | yes | no | 8 | |
| Alqahtani, A., et al. [20] | Case series | yes | yes | yes | yes | yes | yes | yes | no | yes | no | 8 | |
| Alqahtani, A., et al. [32] | Case series | yes | yes | yes | yes | yes | yes | yes | yes | yes | no | Pediatric population | 9 |
| Asokkumar, R., et al. [34] | Case series | yes | yes | yes | yes | yes | yes | yes | no | yes | no | 8 | |
| Barrichello, S., et al. [36] | Case series | yes | yes | yes | yes | yes | yes | yes | no | yes | no | 8 | |
| Bhandari, M., et al. [37] | Case series | yes | yes | yes | yes | yes | yes | yes | no | yes | no | 8 | |
| Callahan, Z. M., et al. [38] | Case series | yes | yes | yes | yes | yes | yes | yes | no | yes | no | 8 | |
| Espinet−Coll, E., et al. [41] | Case series | yes | yes | yes | yes | yes | yes | no | no | yes | no | 7 | |
| Ghoz, H., et al. [47] | Case series | yes | yes | yes | yes | yes | yes | no | no | no | no | 6 | |
| Graus Morales, J., et al. [17, 49] | Case series | yes | yes | yes | yes | yes | yes | yes | no | yes | no | 8 | |
| Hajifathalian, K., et al. [51] | Case series | yes | yes | yes | yes | yes | yes | yes | no | yes | no | 8 | |
| Hill, C., et al. [52] | Case series | yes | yes | yes | yes | yes | yes | yes | no | yes | no | Only for adverse events, no efficacy data | 8 |
| Jagtap, N., et al. [53] | Case series | yes | yes | yes | yes | yes | yes | yes | no | yes | yes | 9 | |
| James, T. W., et al. [54] | Case series | yes | yes | yes | yes | yes | yes | yes | yes | yes | yes | 10 | |
| Kumar, N., et al. [55] | Case series | yes | unclear | unclear | no | unclear | no | no | yes | no | yes | 3 | |
| Li, R., et al. [56] | Case series | yes | yes | yes | no | unclear | yes | yes | yes | yes | yes | 8 | |
| Lopez−Nava, G., et al. [57] | Case series | yes | yes | yes | unclear | no | yes | no | yes | yes | yes | 7 | |
| Lopez−Nava, G., et al. [59] | Case series | yes | yes | yes | yes | unclear | yes | unclear | yes | yes | yes | 8 | |
| Manos, T., et al. [60] | Case series | yes | yes | yes | unclear | unclear | yes | no | yes | no | yes | 6 | |
| Matteo, M. V., et al. [61] | Case series | yes | yes | yes | yes | yes | yes | yes | yes | yes | yes | 10 | |
| Maydeo, A., et al. [16] | Case series | yes | yes | yes | unclear | unclear | yes | yes | unclear | yes | yes | 7 | |
| Mehta, A., et al. [62] | Case series | unclear | unclear | yes | unclear | unclear | yes | yes | yes | yes | yes | 6 | |
| Neto, M. G., et al. [63] | Case series | yes | yes | yes | unclear | unclear | yes | yes | yes | yes | yes | 8 | |
| Neto, M. G., et al. [64] | Case series | no | unclear | unclear | unclear | unclear | no | no | yes | no | unclear | Only for adverse events, no efficacy data | 1 |
| Pizzicannella, M., et al. [66] | Case series | yes | yes | yes | yes | yes | no | no | yes | yes | yes | 8 | |
| Sarkar, A., et al. [68] | Case series | yes | yes | yes | unclear | unclear | yes | yes | yes | no | yes | 7 | |
| Sartoretto, A., et al. [69] | Case series | yes | yes | yes | yes | unclear | yes | yes | yes | yes | yes | 9 | |
| Saumoy, M., et al. [70] | Case series | yes | yes | yes | yes | yes | yes | no | yes | yes | yes | 9 | |
| Sharaiha, R. Z., et al. [71] | Case series | yes | yes | yes | yes | yes | yes | yes | yes | yes | yes | 10 | |
| Summary |
Yes = 27 (93.1%) No = 1 (3.4%) Unclear = 1 (3.4%) |
Yes = 26 (89.7%) No = 0 Unclear = 3 (10.3%) |
Yes = 27 (93.1%) No = 0 Unclear = 2 (6.9%) |
Yes = 27 (93.1%) No = 1 (3.4%) Unclear = 1 (3.4%) |
Yes = 18 (62.1%) No = 1 (3.4%) Unclear = 10 (34.5%) |
Yes = 26 (89.6%) No = 3 (10.4%) Unclear = 0 |
Yes = 20 (69%) No = 8 (27.6%) Unclear = 1 (3.4%) |
Yes = 16 (55.2%) No = 12 (41.4%) Unclear = 1 (3.4%) |
Yes = 24 (82.8%) No = 5 (17.2%) Unclear = 0 |
Yes = 16 (55.2%) No = 12 (41.4%) Unclear = 1 (3.4%) |
7.5 +/− 1.89 | ||
Table 3.
Critical appraisal and risk of bias assessment for the included cohort studies
| COHORT STUDIES | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Author, year | Study design | New Castle-Ottawa Scale for cohort studies domains | ||||||||
| Representativeness of the exposed cohort (1) | Selection of the non-exposed cohort (1) | Ascertainment of exposure (1) | Demonstration that outcome of interest was not present at start of study (1) | Comparability of cohorts based on the design or analysis (2) | Assessment of outcome (1) | Was follow-up long enough for outcomes to occur (1) | Adequacy of follow-up of cohorts (1) | Total score (max = 9) | ||
| Alqahtani, A. R., et al. [33] | Cohort | 1 | 0 | 0 | 1 | 1 | 1 | 0 | 1 | 5 |
| Badurdeen, D. et al. [35] | Cohort | 1 | 0 | 0 | 1 | 0 | 1 | 0 | 1 | 4 |
| Carr, P., et al. [39] | Cohort | 1 | 0 | 0 | 1 | 1 | 1 | 0 | 1 | 5 |
| Cheskin, L. J., et al. [40] | Cohort | 1 | 0 | 1 | 1 | 1 | 1 | 0 | 1 | 6 |
| Espinet-Coll, E., et al. [41] | Cohort | 1 | 0 | 1 | 1 | 1 | 1 | 0 | 1 | 6 |
| Farha, J., et al. [43] | Cohort | 1 | 1 | 0 | 1 | 1 | 1 | 1 | 1 | 7 |
| Fayad, L., et al. [44] | Cohort | 1 | 1 | 0 | 1 | 1 | 1 | 0 | 1 | 6 |
| Fayad, L., et al. [45] | Cohort | 1 | 0 | 0 | 1 | 1 | 1 | 0 | 1 | 5 |
| Fiorillo, C., et al. [46] | Cohort | 1 | 0 | 1 | 1 | 1 | 1 | 0 | 1 | 6 |
| Glaysher, M. A., et al. [48] | Cohort | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 9 |
| Gudur, A. R., et al. [50] | Cohort | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 9 |
| Lopez-Nava, G., et al. [58] | Cohort | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 9 |
| Novikov, A. A., et al. [65] | Cohort | 1 | 1 | 1 | 1 | 0 | 1 | 1 | 0 | 6 |
| Rapaka, B., et al. [67] | Cohort | 1 | 1 | 1 | 1 | 0 | 1 | 1 | 0 | 6 |
| Summary | 1 (0) | 0.42 (0.51) | 0.5 (0.51) | 1 (0) | 0.78 (0.42) | 1 (0) | 0.35 (0.49) | 0.85 (0.36) | 6.07 (1.43) | |
Table 4.
Critical appraisal and risk of bias assessment for the included randomized clinical trial
| RANDOMIZED TRIALS | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Author, year | Study design | Cochrane risk of bias tool | JADAD score | |||||||||
| Selection bias: Random Sequence generation | Selection bias: Allocation Concealment | Reporting Bias: Selective Reporting | Other Bias - other sources of bias | Performance bias | Detection bias | Attrition bias | Randomization | Blinding | Withdrawals | Total | ||
| Abu Dayyeh, B. K., et al. [22] | Randomized clinical trial | Low | Low | Low | Low | High | High | High | 2 | 0 | 1 | 3 |
Meta-analysis
Forty-two articles reported %Excess Weight Loss (%EWL) and/or %Total Body Weight Loss (%TBWL) at least in one time point of interest (6, 12, 18, 24, 36, > 36 months). Two articles [50, 64] only reported safety outcomes. Continuous variables (%EWL and %TBWL) were pooled using the CMA software, and the results are presented ahead of time according to time points. Categorical variables were pooled using absolute numbers to calculate pooled rates. Four articles reported the responder rate as ≥ 5%TWL at 12 months, and 9 reported it as ≥ 10%TBWL. The pooled rates were 422/478 (88.3%) and 632/768 (82.3%). Forty articles reported the SAEs rate (according to the FDA definition from https://www.fda.gov/safety/reporting-serious-problems-fda/what-serious-adverse-event). Among 15,398 ESG procedures, 194 events fulfilled the criteria for SAE for a pooled rate of 1.25%. Table 5 shows all outcomes of the included studies according to follow-up time points, and Fig. 2 graphically depicts weight loss outcomes over time.
Table 5.
Outcomes of the studies included in the non-comparative meta-analysis
| Author (year) | Population (total sample) | Intervention (n) | Comparison (n) | %EWL | n | 6 months | n | 12 months | n | 18 months | n | 24 months | n | ≥36 months | %TBWL |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Abu Dayyeh, B. K., et al. [31] | 25 | ESG | − | 25 | 53 (17) | 10 | 54 (40) | 8 | 45 (41) | − | − | − | − | ||
| Abu Dayyeh, B. K., et al. [22] | 209 | ESG (85) | Lifestyle intervention (124) | − | − | 77 | 49.2 (32) | − | − | 50 | 41 (32) | − | − | ||
| Alqahtani, A., et al. [20] | 1000 | ESG | − | 369 | 64.3 (56.2) | 216 | 67.5 (52.3) | 54 | 64.7 (55.4) | − | − | − | − | ||
| Alqahtani, A., et al. [32] | 109 | ESG | − | 82 | 80.1 (63.3) | 43 | 87.1 (59.5) | 24 | 70.9 (55.5) | 17 | 63.8 (52.3) | ||||
| Alqahtani, A. R., et al. [33] | 6036 | ESG (3018) | LSG (3018) | 2490 | 67.0 (28.6) | 2243 | 77.1 (24.6) | − | − | 1911 | 75.2 (47.9) | 854 | 59.7 (57.1) | ||
| Asokkumar, R., et al. [34] | 35 | ESG | − | − | − | − | − | − | − | − | − | − | − | ||
| Badurdeen, D. et al. [35] | 52 | ESG (26) | ESG + Liraglutide (26) | 26 | 69.94 (6.3) | − | − | − | − | − | − | − | − | ||
| Barrichello, S., et al. [36] | 193 | ESG | − | 181 | 56.15 (22.93) | 121 | 59.41 (25.69) | − | − | − | − | − | − | ||
| Bhandari, M., et al. [37] | 53 | ESG | − | − | − | − | − | − | − | − | − | − | − | ||
| Callahan, Z. M., et al. [38] | 10 | ESG | − | − | − | 3 | 17.6 (47.3) | − | − | 4 | 12.7 (16.9) | − | − | ||
| Carr, P., et al. [39] | 61 | ESG (16) | LSG (45) | 13 | 51 (11) | 9 | 57 (32) | − | − | − | − | − | − | ||
| Cheskin, L. J., et al. [40] | 386 | ESG (105) | Lifestyle intervention (281) | − | − | − | − | − | − | − | − | − | − | ||
| Espinet−Coll, E., et al. [41] | 38 | ESG | − | − | − | − | 48.3 (18.5)* | − | − | − | − | − | − | ||
| Espinet−Coll, E., et al. [18] | 88 | ESG (standard stitching pattern = "TBp") | ESG with different stitching patterns ("Lp" and "TMp") | − | − | 88 | 46.41 (20.6) | − | − | − | − | − | − | ||
| Farha, J., et al. [43] | 247 | ESG (98) | ESG with fundal suturing (149) |
82 99 |
54.7 (19.2) 37.7 (17.3) |
57 66 |
65.3 (21.1) 40.6 (23.5) |
− | − | − | − | − | − | ||
| Fayad, L., et al. [44] | 137 | ESG (54) | LSG (83) | − | − | − | − | − | − | − | − | − | − | ||
| Fayad, L., et al. [45] | 105 | ESG (58) | IGB (47) | − | − | − | − | − | − | − | − | − | − | ||
| Fiorillo, C., et al. [46] | 46 | ESG (23) | LSG (23) | 23 | 39.05 (20.7)* | − | − | − | − | − | − | − | − | ||
| Ghoz, H., et al. [47] | 20 | ESG | − | − | − | − | − | − | − | − | − | − | − | ||
| Glaysher, M. A., et al. [48] | 32 | ESG without longitudinal compression (9) | ESG with longitudinal compression (23) |
5 7 |
42.4 (18.1)* 65.6 (23.9)* |
− | − | − | − | − | − | − | − | ||
| Graus Morales, J., et al. [17, 49] | 148 | ESG | − | 148 | 64.93 (51) | 148 | 75.4 (85) | 72 | 79.25 (43) | − | − | − | − | ||
| Gudur, A. R., et al. [50] | 36,323 | ESG (6,053) | LSG (30,270) | − | − | − | − | − | − | − | − | − | − | ||
| Hajifathalian, K., et al. [51] | 118 | ESG | − | 114 | 45.3 (29.39)* | 100 | 47.8 (32.65)* | − | − | 78 | 45.5 (33.11)* | − | − | ||
| Hill, C., et al. [52] | 21 | ESG | − | − | − | − | − | − | − | − | − | − | − | ||
| Jagtap, N., et al.[53] | 26 | ESG | − | 26 | 32.67 (19.51) | 26 | 51.33 (17.33) | − | − | − | − | − | − | ||
| James, T. W., et al. [54] | 100 | ESG | − | 34 | 48.9 (19.9) | 12 | 66.1 (21.5) | − | − | − | − | − | − | ||
| Kumar, N., et al. [55] | 122 | ESG (23 in phase 1, 22 in phase 2, 77 in phase 3) | − | − | − | − | − | − | − | − | − | − | − | ||
| Li, R., et al. [56] | 24 | ESG | − | 12 | 25 (9.1) | 7 | 29.1 (17.9) | − | − | − | − | − | − | ||
| Lopez−Nava, G., et al. [57] | 435 | ESG | − | − | − | − | − | − | − | − | − | − | − | ||
| Lopez−Nava, G., et al. [58] | 24 | ESG (12) | LSG (12) | − | − | − | − | − | − | − | − | − | − | ||
| Lopez−Nava, G., et al. [59] | 248 | ESG | − | − | − | − | − | − | − | − | − | − | − | ||
| Manos, T., et al. [60] | 191 | ESG | − | 84 | 41.6 (20**) | 69 | 34.7 (22**) | − | − | − | − | − | − | ||
| Matteo, M. V., et al. [61] | 18 | ESG | − | 18 | 39.25 (5.5)* | 12 | 38.25 (10.97)* | 10 | 40.25 (13.26)* | 10 | 41 (8.08)* | − | − | ||
| Maydeo, A., et al. [16] | 58 | ESG | − | 52 | 42.8 (13.1) | − | − | − | − | − | − | − | − | ||
| Mehta, A., et al. [62] | 50 | ESG | − | 47 | 46.9 (22.4) | 39 | 50.5 (24.9) | 47 | 47.7 (26.5) | − | − | − | − | ||
| Neto, M. G., et al. [63] | 233 | ESG | − | 178 | 47.1 (18) | 123 | 54.8 (17.4) | − | − | − | − | − | − | ||
| Neto, M. G., et al. [64] | 1828 | ESG | − | − | − | − | − | − | − | − | − | − | − | ||
| Novikov, A. A., et al. [65] | 278 | ESG (91) | LSG (120) and LAGB (67) | − | − | − | − | − | − | − | − | − | − | ||
| Pizzicannella, M., et al. [66] | 133 | ESG | − | 87 | 34.5 (19.8) | 41 | 34.3 (21.9) | − | − | − | − | − | − | ||
| Rapaka, B., et al. [67] | 41 | ESG (23) | IGB (18) | 23** | 16.17 (5.69) | − | − | − | − | − | − | − | − | ||
| Sarkar, A., et al. [68] | 91 | ESG | − | 52 | 35.6 (20**) | − | − | − | − | − | − | − | − | ||
| Sartoretto, A., et al. [69] | 112 | ESG | − | 52 | 50.3 (22.4) | − | − | − | − | − | − | − | − | ||
| Saumoy, M., et al. [70] | 128 | ESG | − | − | − | − | − | − | − | − | − | − | − | ||
| Sharaiha, R. Z., et al. [71] | 216 | ESG | − | − | − | 142 | 47.9 (33.11)* | − | − | − | − |
36 months = 68 60 months = 56 |
45.1 (42.67)* 45.3 (47.32)* |
||
| Total | 49848 | − | − | 4329 | 48.04 (SE 3.59) | 3652 | 53.09 (SE 4.15) | 215 | 57.98 (SE 7.38) | 2070 | 46.57 (SE 9.85) | 36 months = 922 | 36 months = 53.18 (SE 7.25) |
| Author (year) | n | 6 months | n | 12 months | n | 18 months | n | 24 months | n | ≥36 months | 12−month Responder rate (≥5%TBWL) | 12−month Responder rate (≥10%TBWL) | SAEs | Obs. | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Abu Dayyeh, B. K., et al. [31] | − | − | − | − | − | − | − | − | − | − | − | − | 3/25 | ||
| Abu Dayyeh, B. K., et al. [22] | − | − | 77 | 13.6 (8.0) | − | − | 50 | 11.4 (8.4) | − | − | 70/77 | 48/77 | 6/150 | ||
| Alqahtani, A., et al. [20] | 369 | 13.7 (6.8) | 216 | 15 (7.7) | 54 | 14.8 (8.5) | − | − | − | − | 193/216 | − | 24/1000 | ||
| Alqahtani, A., et al. [32] | 82 | 14.4 (6.5) | 43 | 16.2 (8.3) | 24 | 15.4 (9.2) | 17 | 13.7(8) | − | − | − | − | 1/109 | ||
| Alqahtani, A. R., et al. [33] | 2490 | 15.1 (6.1) | 2243 | 19.2 (7.7) | − | − | 1911 | 16.2 (9.7) | 854 | 14 (12.1) | − | − | 14/3018 | ||
| Asokkumar, R., et al. [34] | 10 | 16.2 (4.9) | − | − | − | − | − | − | − | − | − | − | 0/35 | ||
| Badurdeen, D. et al. [35] | 26 | 20.51 (1.68) | − | − | − | − | − | − | − | − | − | − | 1/52 | ||
| Barrichello, S., et al. [36] | 181 | 14.25 (5.26) | 121 | 15.06 (5.22) | − | − | − | − | − | − | − | − | 2/193 | ||
| Bhandari, M., et al. [37] | 42 | 14.25 (6.17) | 42 | 19.94 (4.89) | − | − | − | − | − | − | − | − | 0 | 37/42 (88%) had >15% TWL at 12 months | |
| Callahan, Z. M., et al. [38] | − | − | − | − | − | − | − | − | − | − | − | − | 2/10 | ||
| Carr, P., et al. [39] | 13 | 15 (6) | 9 | 18 (11) | − | − | − | − | − | − | − | − | 0 | ESG 78% >25% EWL and 55.6% >20%TBWL at 12months | |
| Cheskin, L. J., et al. [40] | 63 | 17.7 (6.4) | 43 | 20.6 (8.3) | − | − | − | − | − | − | 41/43 | 39/43 | 5/105 | 28/105 presented >20% TBWL | |
| Espinet−Coll, E., et al. [41] | − | − | − | 17.1 (3.1)* | − | − | − | − | − | − | − | 36/38 | 1/38 | ||
| Espinet−Coll, E., et al. [18] | − | − | 88 | 17.36 (6.09) | − | − | − | − | − | − | − | 84/88 | 0/88 | ||
| Farha, J., et al. [43] |
82 99 |
17.3 (4.5) 16.2 (7.0) |
57 66 |
21.3 (6.2) 17.5 (10.2) |
− | − | − | − | − | − | − | − | 6/247 | ||
| Fayad, L., et al. [44] | 35 | 17.1 (6.5) | − | − | − | − | − | − | − | − | − | − | 3/54 | 39/54 had >15% TBWL 72.2% at 6 months | |
| Fayad, L., et al. [45] | 25 | 19.5 (5.7) | 21 | 21.3 (6.6) | − | − | − | − | − | − | − | − | 3/58 | ||
| Fiorillo, C., et al. [46] | 23 | 13.87 (6.55)* | − | − | − | − | − | − | − | − | − | − | 0/23 | ||
| Ghoz, H., et al. [47] | 13 | 13.7 (9.3) | 10 | 16.2 (10.4) | − | − | − | − | − | − | − | − | NR | ||
| Glaysher, M. A., et al. [48] |
5 7 |
12.4 (3.1)* 20.5 (5)* |
− | − | − | − | − | − | − | − | − | − | 0/32 | ||
| Graus Morales, J., et al. [17, 49] | 148 | 15.45 (5.9) | 148 | 17.53 (7.57) | 72 | 18.66 (7.3) | − | − | − | − | − | − | 2/148 | ||
| Gudur, A. R., et al. [50] | − | − | − | − | − | − | − | − | − | − | − | − | 86/6053 | ||
| Hajifathalian, K., et al. [51] | 114 | 14.6 (7.07)* | 100 | 15.6 (8.92)* | − | − | 78 | 15.5 (10.13)* | − | − | − | 75/100 | 0/118 | 60 (74%) >10% TBWL at 2 years; improvement in ALT, AST, HSI, NAFLD fib score, HbA1c, HOMA−IR and Leptin | |
| Hill, C., et al. [52] | − | − | − | − | − | − | − | − | − | − | − | − | 1/31 | Learning curve plateau at 7 cases | |
| Jagtap, N., et al. [53] | 26 | 11.33 (4.99) | 26 | 18.07 (3.35) | − | − | − | − | − | − | − | − | 0/26 | 23/26 (88.4%) >15%TBWL at 12 months; improvement in ALT, HSI, NAFLD fib score, FIB−4, and APRI at 12 months | |
| James, T. W., et al. [54] | 34 | 16.41 (5.4) | 12 | 23.1 (7.5) | − | 12/12 | 2/100 | ||||||||
| Kumar, N., et al. (2018). |
Phase 2 Phase 3 NO SAMPLE |
17.3 (1.7) 16 (0.8) |
Phase 2 (20) Phase 3 (44) |
17.3 (2.6) 17.6 (2.1) |
− | − | − | − | − | − | − | − | 0/122 | ||
| Li, R., et al. [56] | 12 | 11.3 (4.7) | 7 | 12.2 (8.9) | − | − | − | − | − | − | − | − | 1/24 | ||
| Lopez−Nava, G., et al. [57] |
Class I = 99 Class II = 151 Class III = 146 |
14.9 (6.5) 16.8 (6.3) 16.8 (6.3) |
Class I = 50 Class II = 77 Class III = 84 |
17.1 (6.7) 19 (8) 22.2 (9.3) |
− | − | − | − | − | − | − |
42/50 67/77 78/84 |
6/435 | ||
| Lopez−Nava, G., et al. [59] | 12 | 13.3 (7) | − | − | − | − | − | − | − | − | − | − | 0/12 | ||
| Lopez−Nava, G., et al. [59] | 215 | 15.17 (7.66)* | − | − | − | − | 57 | 18.6 (11.15)* | − | − | − | 48/57 | 5/248 | ||
| Manos, T., et al. [61] | 84 | 22.4 (8**) | 69 | 18.7 (8**) | − | − | − | − | − | − | − | − | 2/191 | ||
| Matteo, M. V., et al. [61] | 18 | 14.97 (4.56)* | 12 | 15.27 (5.25)* | 10 | 16 (7.38)* | 10 | 15.55 (6.93)* | − | − | − | − | 0/18 | ||
| Maydeo, A., et al. [16] | 52 | 17.1 (4.3) | − | − | − | − | − | − | − | − | − | − | 0/58 | ||
| Mehta, A., et al. [62] | 47 | 14.8 (5.3) | 39 | 15.5 (7.2) | 47 | 15.4 (9.8) | − | − | − | − | − | − | 0/50 | Significant improvement in depression scores | |
| Neto, M. G., et al. [63] | 178 | 16.9 (6.2) | 123 | 19.7 (5.7) | − | − | − | − | − | − | − | − | 0/233 | ||
| Neto, M. G., et al. [64] | − | − | − | − | − | − | − | − | − | − | − | − | 15/1828 | ||
| Novikov, A. A., et al. [65] | 61 | 14.37 (7) | 28 | 17.57 (8.1) | − | − | − | − | − | − | − | − | 1/91 | ||
| Pizzicannella, M., et al. [66] | 87 | 13.2 (7.4) | 41 | 13.1 (8.1) | − | − | − | − | − | − | − | − | − | Experience improved the proportion of intact ESG at 12 months | |
| Rapaka, B., et al. [67] | − | − | − | − | − | − | − | − | − | − | − | − | − | Delay in T50 correlated with %TBWL at 3 months | |
| Sarkar, A., et al. [68] | 52 | 17.4 (6.5**) | − | − | − | − | − | − | − | − | − | − | − | ||
| Sartoretto, A., et al. [69] | 52 | 14.9 (6.1) | − | − | − | − | − | − | − | − | − | − | 3/112 | ||
| Saumoy, M., et al. [70] | 74 | 13.43 (7.4) | 60 | 15.8 (9.5) | − | − | − | − | − | − | − | − | 2/128 | Learning curve: efficiency at 29 and mastery at 55 cases | |
| Sharaiha, R. Z., et al. [71] | − | − | 142 | 15.6 (9.11)* | − | − | − | − |
36 months = 68 60 months = 56 |
14.9 (11.77)* 15.9 (16.79)* |
118/142 | 103/142 | 3/216 | ||
| Total | 5227 | 15.66 (SE 0.35) | 4118 | 17.56 (SE 0.39) | 207 | 16.25 (SE 0.95) | 2123 | 15.2 (SE 0.93) | 36 months = 922 | 36 months = 14.07 (SE 0.39) | 422/478 (88.3%) | 632/768 (82.3%) | 194/15,398 (1.25%) |
* Calculated fields
** Inputted data
Summary of Weight Loss Outcomes After ESG (Table 6 and Fig. 3)
Table 6.
Summary of weight loss outcomes after ESG
| Time | Mean %EWL | Mean %TBWL |
|---|---|---|
| 6 months | 48.04% (SE 3.59, 95%CI 40.98–55.09, 24 articles, 4329 patients) | 15.66% (SE 0.35, 95%CI 14.95–16.36, 33 articles, 5227 patients) |
| 12 months | 53.09% (SE 4.15, 95%CI 44.95–61.23, 21 articles, 3652 patients) | 17.56% (SE 0.39, 95%CI 16.8–18.32, 27 articles, 4118 patients) |
| 18 months | 57.98% (SE 7.38, 95%CI 43.5–72.46, 6 articles, 215 patients) | 16.25% (SE 0.95, 95%CI 14.38–18.13, 5 articles, 207 patients) |
| 24 months | 46.57% (SE 9.85, 95%CI 27.26–65.88, 6 articles, 2070 patients) | 15.2% (SE 0.93, 95%CI 13.36–17.04, 6 articles, 2123 patients) |
| 36 months | 53.18% (SE 7.25, 2 articles, 922 patients) | 14.07% (SE 0.39, 2 articles, 922 patients) |
| 60 months | 45.3 (SD 47.32, 1 article, 56 patients) | 15.9 (SD 16.79, 1 article, 56 patients) |
*SE standard errors, CI confidence interval, EWL excess weight loss, TBWL total body weight loss
Fig. 3.

Figure displaying the mean percentage of excess weight loss (%EWL) and total body weight loss (%TBWL) over different time points following endoscopic sleeve gastroplasty (ESG) with standard error bars. The sample sizes and the number of articles at each time point are incorporated above the bars for clarity and additional context
Quality of Evidence Assessment
All pooled outcomes were assessed for the quality of evidence according to the GRADE methodology. Since this analysis included only non-comparative data, all endpoints were rated as VERY LOW quality of evidence. Table 7 depicts the GRADE assessment.
Table 7.
GRADE assessment of the quality of evidence for the non-comparative meta-analysis

(a) Data from case series
Direct Comparative ESG Studies
Systematic Review
Two independent researchers (VOB and NJ) ran separate literature searches assessing eligible studies. We searched MEDLINE (PubMed), EMBASE, and gray literature from January 1, 2013 (the year ESG was described), to October 1, 2022. The step-by-step construction of the search strategy is provided in SUPPL 3. The final strategy was as follows:
MEDLINE (PubMed):(excess weight) OR (overweight) OR (obesity) AND (endoscopy) OR (endoscopic) OR (transoral*) OR (peroral*) OR (incisionless) AND (sleeve) OR (overstitch) OR (gastroplasty) OR (gastric plication) OR (gastric imbrication) AND (lifestyle) OR (diet) OR (exercise) OR (counseling) OR (sham) OR (placebo)
EMBASE: endoscopic AND sleeve AND gastroplasty OR (apollo AND overstitch) AND [embase]/lim NOT ([embase]/lim AND [medline]/lim) AND ('article'/it OR 'article in press'/it OR 'conference review'/it OR 'note'/it OR 'review'/it)
The eligibility criteria included:
Articles published online from 01/JAN/2013 until 01/OCT/2022 (last search update);
ESG performed with the Apollo Overstitch device (no restriction as to stitching pattern);
No language restriction;
Full-text articles only;
Comparative study designs: cohort studies, case–control studies, and randomized trials;
Studies reporting efficacy and/or safety data.
The initial search retrieved 537 records. After screening titles and abstracts, 13 articles were selected for full-text assessment. Finally, only 2 articles were included in the qualitative and quantitative analyses. Figure 4 shows the screening and inclusion/exclusion flowchart.
Fig. 4.

PRISMA flowchart for the literature screening and inclusion/exclusion process for only comparing ESG and lifestyle intervention
Descriptive Analysis
Cheskin et al. [40] and Abu Dayyeh et al. [22] were eligible studies for directly comparing ESG and lifestyle intervention. The first was a case-matched (1 ESG: 2–3 controls) cohort study comparing ESG plus low-intensity diet and lifestyle therapy (LIDLT) versus high-intensity diet and lifestyle therapy (HIDLT). This study included patients with obesity class 1 or higher. For both groups, patients paid out-of-pocket for the treatment (total cost ESG: U$ 16,000; total cost HIDLT: U$ 3200). A total of 386 patients (105 ESG, 281 control) were included in the study, with similar baseline characteristics. The final follow-up visit was at 12 months.
Abu Dayyeh et al. [22] was a multicenter, US FDA–regulated, open-label, randomized trial comparing ESG plus lifestyle interventions to lifestyle intervention alone (MERIT Trial). Only patients with obesity classes I and II (BMI 30–40 kg/m2) were included and allocated to ESG or control group in a 1–1.5 ratio. After 52 weeks, compliant control patients crossed over to ESG. Two hundred and nine patients (85 ESG, 124 control) were enrolled and had similar baseline characteristics. The primary endpoints were %EWL and %TBWL at 12 months, but there was an extended follow-up at 24 months for the intervention group and a 12-month follow-up for the control group crossing over to intervention.
The baseline data and the critical appraisal/risk of bias assessment for the studies are summarized in Tables 1, 3, and 4.
Meta-analysis
The two studies differ in design (cohort vs. RCT) and population (non-specified obesity vs. class I and II). According to the Cochrane Handbook [25], data from different study designs should not be pooled when few eligible studies exist. Therefore, we analyzed data from Cheskin et al. 2020 and Abu Dayyeh et al. 2022 separately. Since we could not pool data from different studies, heterogeneity, and sensitivity analyses do not apply.
-
A)Outcomes from MERIT Trial [22]
Fig. 5.

Forest plot for %EWL at 12 months in comparing ESG vs. lifestyle intervention for patients with class I and II obesity
Fig. 6.

Forest plot for %TBWL at 12 months in comparing ESG vs. lifestyle intervention for patients with class I and II obesity
The quality of evidence Abu Dayyeh et al. generated was MODERATE according to the GRADE methodology. Overall, data coming from a single study (imprecision) and the absence of double blinding were the two factors downgrading the quality of evidence. Table 8 summarizes the GRADE assessment.
-
B)Outcomes from Cheskin et al. (ADD REF here)
Table 8.
GRADE assessment of the quality of evidence for comparing ESG vs. lifestyle intervention for patients with mild and moderate obesity

CI confidence interval, MD mean difference, OR odds ratio. (a) Open-label trial (detection bias) and loss to follow-up rates (20% intervention, 29% control group). Attrition bias present. (b) Single RCT with 77 patients in the intervention arm and 110 in the control arm. Large SDs: mean 49.2 ± 32 versus 3.2 ± 18.6. (c) Single RCT with 77 patients in the intervention arm and 110 in the control arm. Large SD: mean 13.6 ± 8 versus 0.8 ± 5. (d) Single RCT with 77 patients in the intervention arm and 110 in the control arm
Fig. 7.

Forest plot for %TBWL at 12 months in the comparison of ESG vs. high-intensity lifestyle intervention for patients with obesity (all classes)
The quality of evidence Cheskin et al. generated was VERY LOW according to the GRADE methodology. Overall, data from a single study (imprecision) and a non-randomized study design (selection bias) led to the final quality of evidence. Table 9 summarizes the GRADE assessment.
Table 9.
GRADE assessment of the quality of evidence for comparing ESG vs. lifestyle intervention for patients with mild and moderate obesity. Question: ESG plus lifestyle modification compared to Lifestyle modification alone for obesity

CI confidence interval, MD mean difference, OR odds ratio. (a) Selection bias (matched controls). Channeling bias. Confounding variables (socio-economic status), high loss to follow-up rates. (b) Single study, small total sample size/small number of events, large SDs
IFSO Bariatric Endoscopy Position Statement and Future Direction
Based on a comprehensive systematic review and meta-analysis, the IFSO Bariatric Endoscopy Committee endorses endoscopic sleeve gastroplasty (ESG) as an effective and valuable intervention for managing obesity. ESG is particularly beneficial for patients with class I and II obesity, as well as for those with class III obesity who are not suitable candidates for traditional MBS. This minimally invasive procedure not only achieves significant weight loss outcomes in the short and mid-terms but also maintains a favorable safety profile, as evidenced by a low incidence of serious adverse events.
The systematic review encompassed numerous observational studies, which, despite being categorized as very low quality, consistently reported positive and similar outcomes from different cohorts and practice settings globally, indicating reproducibility, generalizability, and maturity of ESG. Additionally, including a single randomized controlled trial in the meta-analysis provided moderate quality evidence, further substantiating the efficacy and safety of ESG. This dual-source evidence base enhances the robustness of the findings, lending more significant support to the recently published IFSO International Delphi Consensus statement on the position of ESG in the spectrum of obesity care [23].
It is important to emphasize the crucial role of integrating and complementing any obesity intervention, such as ESG, with a comprehensive and longitudinal healthy living program. This program should include a healthy diet, physical activity, adequate sleep, and mindfulness to maintain the weight loss benefits and maximize the overall impact on health by the intervention. By incorporating ESG into a comprehensive program, healthcare providers can offer a broader spectrum of options for obesity management tailored to the needs and circumstances of individual patients. This integrated approach enhances the effectiveness of ESG but also ensures long-term health benefits for patients.
Future Direction
In this report, we investigated endoscopic sleeve gastroplasty utilizing the Apollo Overstitch™ platform (Boston Scientific, Marlborough, MA, USA) based on the maturity of the technique, regulatory approvals (https://www.accessdata.fda.gov/cdrh_docs/pdf21/DEN210045.pdf, https://www.nice.org.uk/guidance/ipg783) and cost-effectiveness [72–74]. Other endoscopic gastric remodeling techniques, including the Primary Obesity Surgery Endoluminal 2.0 (USGI Medical, San Clemente, CA), Endomina™ Gastric Plication (Endo Tools, Gosselies, Belgium), and the Endozip™ automated suturing device (Caesarea, Israel), are at different stages of clinical trials and evidence generation and are demonstrating similar safety and efficacy profiles. The committee will update its position statement to reflect and incorporate the evolving evidence base as the clinical evidence continues to mature for these procedures.
Advancements in obesity management medication now offer effective options for selected patients. The value proposition and comparative effectiveness of ESG compared to, or in addition to, obesity pharmacotherapies is an active area of investigation. Observational studies have demonstrated the benefits of combining or sequencing ESG with obesity pharmacotherapies, particularly in enhancing the durability of the response [75].
However, given the limited follow-up in the existing literature—typically extending to five years or less—additional data is required to better understand the different archetypes of response to ESG over the long term. This data will also help in defining optimal personalized approaches to maximize the durability of the response and improve long-term health outcomes.
Acknowledgements
Acknowledgements: The IFSO Bariatric and Metabolic Endoscopy Committee would like to extend their sincere appreciation to the following experts for their invaluable contributions to the systematic review, evidence extraction, evidence grading, meta-analyses, and the drafting of tables and figures: Dr. Vitor O. Brunaldi (VOB): Methodologist and researcher at the University of São Paulo, specializing in endoscopic techniques. Dr. Nitin Jagtap (NJ): Expert in systematic reviews and meta-analyses at the Asian Institute of Gastroenterology. Dr. Rakesh Kalapala (RK): Senior Consultant at the Asian Institute of Gastroenterology, India. His content expertise ensured the clinical relevance and accuracy of this work. Dr. Barham Abu Dayyeh (BAD): Professor of Medicine and Chair of the IFSO Bariatric and Metabolic Endoscopy Committee during the preparation of this document. IFSO Scientific Committee: For critical review and multiple rounds of revisions of this document prior to approval. IFSO Executive Board: For critical review and multiple rounds of revisions of this document prior to approval.
Author Contribution
B.K.A: Conception of the study, critical review of the data, drafting of the manuscript, tables, and figures. Chair, IFSO Bariatric Endoscopy Committee at the time of study initiation. C.S.: Conception of the study, critical review of the data and manuscript. Chair, IFSO Bariatric Endoscopy Committee at the time of study conclusion. A.A.: Conception of the study, review of the manuscript. Member, IFSO Bariatric Endoscopy Committee. R.S.: Conception of the study, review of the manuscript. Member, IFSO Bariatric Endoscopy Committee. M.B.: Conception of the study, review of the manuscript. Member, IFSO Bariatric Endoscopy Committee. S.P.: Conception of the study, review of the manuscript. Member, IFSO Bariatric Endoscopy Committee. S.P.J.: Conception of the study, review of the manuscript. Member, IFSO Bariatric Endoscopy Committee. G.P.: Critical review of the data and manuscript. IFSO President during the conduct of the study. R.C.: Critical review of the data and manuscript. IFSO President at the conclusion of the study.
Funding
Open access funding provided by SCELC, Statewide California Electronic Library Consortium
Data Availability
No datasets were generated or analysed during the current study.
Declarations
Competing Interests
Barham K. Abu Dayyeh: Received research support and educational consulting fees from Boston Scientific; previously Apollo Endosurgery. Additionally, received research support from USGI Medical. Christine Stier: Consulting and educational engagements with Boston Scientific. Aayed Alqahtani: Consulting and educational engagements with Boston Scientific. Reem Sharaiha: Consulting and educational engagements with Boston Scientific. Mohit Bandhari: Consulting and educational engagements with Boston Scientific. Silvana Perretta: Consulting and educational engagements with Boston Scientific. Sigh Pichamol Jirapinyo: Consulting and educational engagements with Boston Scientific. Gerhard Prager: Declares no conflicts of interest related to this study. Ricardo Cohen: Declares no conflicts of interest related to this study.
Footnotes
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Change history
11/15/2024
A Correction to this paper has been published: 10.1007/s11695-024-07580-z
References
- 1.Worldwide trends in body-mass index. underweight, overweight, and obesity from 1975 to 2016: a pooled analysis of 2416 population-based measurement studies in 128·9 million children, adolescents, and adults. Lancet. 2017;390:2627–42. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.World Healh Organization. Overweight and obesity - global observatory data. https://www.who.int/news-room/fact-sheets/detail/obesity-and-overweight.
- 3.Hales CM, Carroll MD, Fryar CD, et al. Prevalence of obesity among adults and youth: United States, 2015–2016. NCHS Data Brief. 2017;288:1–8. [PubMed] [Google Scholar]
- 4.Hales CM, Fryar CD, Carroll MD, et al. Trends in obesity and severe obesity prevalence in US youth and adults by sex and age, 2007–2008 to 2015–2016. JAMA. 2018;319:1723–5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Finkelstein EA, Khavjou OA, Thompson H, et al. Obesity and severe obesity forecasts through 2030. Am J Prev Med. 2012;42:563–70. [DOI] [PubMed] [Google Scholar]
- 6.Eisenberg D, Shikora SA, Aarts E, et al. American Society for Metabolic and Bariatric Surgery (ASMBS) and International Federation for the Surgery of Obesity and Metabolic Disorders (IFSO): indications for metabolic and bariatric surgery. Surg Obes Relat Dis. 2022;18:1345–56. [DOI] [PubMed] [Google Scholar]
- 7.Carlsson LMS, Sjöholm K, Jacobson P, et al. Life expectancy after bariatric surgery in the Swedish obese subjects study. N Engl J Med. 2020;383:1535–43. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Angrisani L, Santonicola A, Iovino P, et al. Bariatric Surgery Survey 2018: similarities and disparities among the 5 IFSO chapters. Obes Surg. 2021;31:1937–48. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Angrisani L, Santonicola A, Iovino P, et al. IFSO Worldwide Survey 2016: primary, endoluminal, and revisional procedures. Obes Surg. 2018;28:3783–94. [DOI] [PubMed] [Google Scholar]
- 10.Ogden CL, Carroll MD, Kit BK, et al. Prevalence of childhood and adult obesity in the United States, 2011–2012. JAMA. 2014;311:806–14. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Whitlock G, Lewington S, Sherliker P, et al. Body-mass index and cause-specific mortality in 900 000 adults: collaborative analyses of 57 prospective studies. Lancet (London, England). 2009;373:1083–96. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Abu Dayyeh BK, Rajan E, Gostout CJ. Endoscopic sleeve gastroplasty: a potential endoscopic alternative to surgical sleeve gastrectomy for treatment of obesity. Gastrointest Endosc. 2013;78:530–5. [DOI] [PubMed] [Google Scholar]
- 13.Galvao-Neto MDP, Grecco E, Souza TFd, et al. Endoscopic sleeve gastroplasty - minimally invasive therapy for primary obesity treatment. Arquivos brasileiros de cirurgia digestiva : ABCD = Brazilian Archiv of Digestive Surgery. 2016;29Suppl 1:95–97. [DOI] [PMC free article] [PubMed]
- 14.Lopez-Nava G, Galvão MP, Bautista-Castaño I, et al. Endoscopic sleeve gastroplasty: how i do it? Obes Surg. 2015;25:1534–8. [DOI] [PubMed] [Google Scholar]
- 15.Vargas EJ, Rizk M, Gomez-Villa J, et al. Effect of endoscopic sleeve gastroplasty on gastric emptying, motility and hormones: a comparative prospective study. Gut 2022. 10.1136/gutjnl-2022-327816 [DOI] [PMC free article] [PubMed]
- 16.Maydeo A, Patil G, Dalal A, et al. An Indian experience of endoscopic treatment of obesity by using a novel technique of endoscopic sleeve gastroplasty (accordion procedure). J Assoc Physicians India. 2020;68:14–7. [PubMed] [Google Scholar]
- 17.Graus Morales J, Crespo Perez L, Marques A, et al. Modified endoscopic gastroplasty for the treatment of obesity. Surg Endosc. 2018;32:3936–42. [DOI] [PubMed] [Google Scholar]
- 18.Espinet-Coll E, Nebreda-Durán J, Galvao-Neto M, et al. Suture pattern does not influence outcomes of endoscopic sleeve gastroplasty in obese patients. Endoscopy international open. 2020;8:E1349–58. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.López-Nava Breviere G, Bautista-Castaño I, Fernández-Corbelle JP, et al. Endoscopic sleeve gastroplasty (the Apollo method): a new approach to obesity management. Rev Esp Enferm Dig. 2016;108:201–6. [DOI] [PubMed] [Google Scholar]
- 20.Alqahtani A, Al-Darwish A, Mahmoud AE, et al. Short-term outcomes of endoscopic sleeve gastroplasty in 1000 consecutive patients. Gastrointest Endosc. 2019;89:1132–8. [DOI] [PubMed] [Google Scholar]
- 21.Cheskin LJ, Hill C, Adam A, et al. Endoscopic sleeve gastroplasty versus high-intensity diet and lifestyle therapy: a case-matched study. Gastrointest Endosc. 2020;91:342-349.e1. [DOI] [PubMed] [Google Scholar]
- 22.Abu Dayyeh BK, Bazerbachi F, Vargas EJ, et al. Endoscopic sleeve gastroplasty for treatment of class 1 and 2 obesity (MERIT): a prospective, multicentre, randomised trial. Lancet. 2022;400:441–51. [DOI] [PubMed] [Google Scholar]
- 23.Salminen P, Kow L, Aminian A, et al. IFSO consensus on definitions and clinical practice guidelines for obesity management-an international delphi study. Obes Surg. 2024;34:30–42. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Moher D, Liberati A, Tetzlaff J, et al. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. BMJ (Clinical research ed). 2009;339:b2535–b2535. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Higgins JPT, Thomas J, Chandler J, Cumpston M, Li T, Page MJ, Welch VA. Cochrane Handbook for Systematic Reviews of Interventions (Version 6.3, updated February 2022). Cochrane. 2022. Available from: https://training.cochrane.org/handbook.
- 26.The Joanna Briggs Institute. Joanna Briggs Institute Reviewers' Manual: 2016 ed. Australia: the joanna briggs institute. 2016. Available from: https://jbi.global/research/handbook.
- 27.Wells GA, Shea B, O'Connell D, et al. The Newcastle-Ottawa Scale (NOS) for assessing the quality of nonrandomised studies in meta-analyses [Internet]. 2021. Available from: http://www.ohri.ca/programs/clinical_epidemiology/oxford.asp.
- 28.Jadad AR, Moore RA, Carroll D, et al. Assessing the quality of reports of randomized clinical trials: is blinding necessary? Control Clin Trials. 1996;17:1–12. [DOI] [PubMed] [Google Scholar]
- 29.Hozo SP, Djulbegovic B, Hozo I. Estimating the mean and variance from the median, range, and the size of a sample. BMC Med Res Methodol. 2005;5:13–13. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Schünemann H, Brożek J, Guyatt G, Oxman A. GRADE handbook for grading quality of evidence and strength of recommendations. The GRADE Working Group. 2013. Available from: https://gdt.gradepro.org/app/handbook/handbook.html.
- 31.Abu Dayyeh BK, Acosta A, Camilleri M, et al. Endoscopic sleeve gastroplasty alters gastric physiology and induces loss of body weight in obese individuals. Clin Gastroenterol Hepatol. 2017;15:37-43.e1. [DOI] [PubMed] [Google Scholar]
- 32.Alqahtani A, Elahmedi M, Alqahtani YA, et al. Endoscopic sleeve gastroplasty in 109 consecutive children and adolescents with obesity: two-year outcomes of a new modality. Am J Gastroenterol. 2019;114:1857–62. [DOI] [PubMed] [Google Scholar]
- 33.Alqahtani AR, Elahmedi M, Aldarwish A, et al. Endoscopic gastroplasty versus laparoscopic sleeve gastrectomy: a noninferiority propensity score-matched comparative study. Gastrointest Endosc. 2022;96:44–50. [DOI] [PubMed] [Google Scholar]
- 34.Asokkumar R, Lim CH, Tan AS, et al. Safety and early efficacy of endoscopic sleeve gastroplasty (ESG) for obesity in a multi-ethnic Asian population in Singapore. JGH Open. 2021;5:1351–6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.Badurdeen D, Hoff AC, Hedjoudje A, et al. Endoscopic sleeve gastroplasty plus liraglutide versus endoscopic sleeve gastroplasty alone for weight loss. Gastrointest Endosc. 2021;93:1316-1324.e1. [DOI] [PubMed] [Google Scholar]
- 36.Barrichello S, Hourneaux de Moura DT, Hourneaux de Moura EG, et al. Endoscopic sleeve gastroplasty in the management of overweight and obesity: an international multicenter study. Gastrointest Endosc 2019;90:770–780. [DOI] [PubMed]
- 37.Bhandari M, Jain S, Mathur W, et al. Endoscopic sleeve gastroplasty is an effective and safe minimally invasive approach for treatment of obesity: first Indian experience. Digestive endoscopy : official journal of the Japan Gastroenterological Endoscopy Society 2019. 10.1111/den.13508 [DOI] [PubMed]
- 38.Callahan ZM, Su B, Kuchta K, et al. Endoscopic suturing results in high technical and clinical success rates for a variety of gastrointestinal pathologies. J Gastrointest Surg. 2020;24:278–87. [DOI] [PubMed] [Google Scholar]
- 39.Carr P, Keighley T, Petocz P, et al. Efficacy and safety of endoscopic sleeve gastroplasty and laparoscopic sleeve gastrectomy with 12+ months of adjuvant multidisciplinary support. BMC Prim Care. 2022;23:26. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 40.Cheskin LJ, Hill C, Adam A, et al. Endoscopic sleeve gastroplasty versus high-intensity diet and lifestyle therapy: a case-matched study. Gastrointest Endosc. 2020;91:342-349.e1. [DOI] [PubMed] [Google Scholar]
- 41.Espinet-Coll E, Díaz-Galán P, Nebreda-Durán J, et al. Persistence of sutures and gastric reduction after endoscopic sleeve gastroplasty: radiological and endoscopic assessment. Obes Surg. 2022;32:1969–79. [DOI] [PubMed] [Google Scholar]
- 42.Espinet-Coll E, Nebreda-Durán J, Galvao-Neto M, et al. Suture pattern does not influence outcomes of endoscopic sleeve gastroplasty in obese patients. Endosc Int Open. 2020;8:E1349-e1358. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 43.Farha J, McGowan C, Hedjoudje A, et al. Endoscopic sleeve gastroplasty: suturing the gastric fundus does not confer benefit. Endoscopy. 2021;53:727–31. [DOI] [PubMed] [Google Scholar]
- 44.Fayad L, Adam A, Schweitzer M, et al. Endoscopic sleeve gastroplasty versus laparoscopic sleeve gastrectomy: a case-matched study. Gastrointest Endosc. 2019;89:782–8. [DOI] [PubMed] [Google Scholar]
- 45.Fayad L, Cheskin LJ, Adam A, et al. Endoscopic sleeve gastroplasty versus intragastric balloon insertion: efficacy, durability, and safety. Endoscopy 2019. 10.1055/a-0852-3441 [DOI] [PubMed]
- 46.Fiorillo C, Quero G, Vix M, et al. 6-month gastrointestinal quality of life (QoL) results after endoscopic sleeve gastroplasty and laparoscopic sleeve gastrectomy: a propensity score analysis. Obes Surg. 2020;30:1944–51. [DOI] [PubMed] [Google Scholar]
- 47.Ghoz H, Bryant M, Fritz H, et al. Endoscopic sleeve gastroplasty and postprocedural nutritional deficiencies: results from a single center exploratory study. Eur J Gastroenterol Hepatol. 2021;33:e1039–41. [DOI] [PubMed] [Google Scholar]
- 48.Glaysher MA, Moekotte AL, Kelly J. Endoscopic sleeve gastroplasty: a modified technique with greater curvature compression sutures. Endosc Int Open. 2019;7:E1303-e1309. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 49.Graus Morales J, Crespo Pérez L, Marques A, et al. Modified endoscopic gastroplasty for the treatment of obesity. Surg Endosc. 2018;32:3936–42. [DOI] [PubMed] [Google Scholar]
- 50.Gudur AR, Geng C, Kshatri S, et al. Comparison of endoscopic sleeve gastroplasty versus surgical sleeve gastrectomy: a metabolic and bariatric surgery accreditation and quality improvement program database analysis. Gastrointest Endosc 2022. 10.1016/j.gie.2022.07.017 [DOI] [PubMed]
- 51.Hajifathalian K, Mehta A, Ang B, et al. Improvement in insulin resistance and estimated hepatic steatosis and fibrosis after endoscopic sleeve gastroplasty. Gastrointest Endosc. 2021;93:1110–8. [DOI] [PubMed] [Google Scholar]
- 52.Hill C, El Zein M, Agnihotri A, et al. Endoscopic sleeve gastroplasty: the learning curve. Endosc Int Open. 2017;5:E900-e904. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 53.Jagtap N, Kalapala R, Katakwar A, et al. Endoscopic sleeve gastroplasty - minimally invasive treatment for non-alcoholic fatty liver disease and obesity. Indian J Gastroenterol. 2021;40:572–9. [DOI] [PubMed] [Google Scholar]
- 54.James TW, Reddy S, Vulpis T, et al. Endoscopic sleeve gastroplasty is feasible, safe, and effective in a non-academic setting: short-term outcomes from a community gastroenterology practice. Obes Surg. 2020;30:1404–9. [DOI] [PubMed] [Google Scholar]
- 55.Kumar N, Abu Dayyeh BK, Lopez-Nava Breviere G, et al. Endoscopic sutured gastroplasty: procedure evolution from first-in-man cases through current technique. Surg Endosc. 2018;32:2159–64. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 56.Li R, Veltzke-Schlieker W, Adler A, et al. Endoscopic sleeve gastroplasty (ESG) for high-risk patients, high body mass index (> 50 kg/m(2)) patients, and contraindication to abdominal surgery. Obes Surg. 2021;31:3400–9. [DOI] [PubMed] [Google Scholar]
- 57.Lopez-Nava G, Laster J, Negi A, et al. Endoscopic sleeve gastroplasty (ESG) for morbid obesity: how effective is it? Surg Endosc. 2022;36:352–60. [DOI] [PubMed] [Google Scholar]
- 58.Lopez-Nava G, Negi A, Bautista-Castaño I, et al. Gut and metabolic hormones changes after endoscopic sleeve gastroplasty (ESG) vs. laparoscopic sleeve gastrectomy (LSG). Obes Surg. 2020;30:2642–51. [DOI] [PubMed] [Google Scholar]
- 59.Lopez-Nava G, Sharaiha RZ, Vargas EJ, et al. Endoscopic sleeve gastroplasty for obesity: a multicenter study of 248 patients with 24 months follow-up. Obes Surg. 2017;27:2649–55. [DOI] [PubMed] [Google Scholar]
- 60.Manos T, Costil V, Karsenty L, et al. Safety of endoscopic sleeve gastroplasty with a single-channel endoscope. Obes Surg. 2022;32:3074–8. [DOI] [PubMed] [Google Scholar]
- 61.Matteo MV, Bove V, Pontecorvi V, et al. Outcomes of endoscopic sleeve gastroplasty in the elder population. Obes Surg 2022. 10.1007/s11695-022-06232-4 [DOI] [PMC free article] [PubMed]
- 62.Mehta A, Hajifathalian K, Shah SL, et al. Quality of life, mental health, and weight loss outcomes following endoscopic sleeve gastroplasty. J Gastrointestinal Surg : Off J Soc Surg Alimentary Tract. 2022;26:469–71. [DOI] [PubMed] [Google Scholar]
- 63.Neto MG, Moon RC, de Quadros LG, et al. Safety and short-term effectiveness of endoscopic sleeve gastroplasty using overstitch: preliminary report from a multicenter study. Surg Endosc. 2020;34:4388–94. [DOI] [PubMed] [Google Scholar]
- 64.Neto MG, Silva LB, de Quadros LG, et al. Brazilian consensus on endoscopic sleeve gastroplasty. Obes Surg. 2021;31:70–8. [DOI] [PubMed] [Google Scholar]
- 65.Novikov AA, Afaneh C, Saumoy M, et al. Endoscopic sleeve gastroplasty, laparoscopic sleeve gastrectomy, and laparoscopic band for weight loss: how do they compare? J Gastrointest Surg. 2018;22:267–73. [DOI] [PubMed] [Google Scholar]
- 66.Pizzicannella M, Lapergola A, Fiorillo C, et al. Does endoscopic sleeve gastroplasty stand the test of time? Objective assessment of endoscopic ESG appearance and its relation to weight loss in a large group of consecutive patients. Surg Endosc. 2020;34:3696–705. [DOI] [PubMed] [Google Scholar]
- 67.Rapaka B, Maselli DB, Lopez-Nava G, et al. Effects on physiologic measures of appetite from intragastric balloon and endoscopic sleeve gastroplasty: results of a prospective study. Chin Med J (Engl). 2022;135:1234–41. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 68.Sarkar A, Tawadros A, Andalib I, et al. Safety and efficacy of endoscopic sleeve gastroplasty for obesity management in new bariatric endoscopy programs: a multicenter international study. Ther Adv Gastrointest Endosc. 2022;15:26317745221093884. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 69.Sartoretto A, Sui Z, Hill C, et al. Endoscopic sleeve gastroplasty (ESG) is a reproducible and effective endoscopic bariatric therapy suitable for widespread clinical adoption: a large, international multicenter study. Obes Surg. 2018;28:1812–21. [DOI] [PubMed] [Google Scholar]
- 70.Saumoy M, Schneider Y, Zhou XK, et al. A single-operator learning curve analysis for the endoscopic sleeve gastroplasty. Gastrointest Endosc. 2018;87:442–7. [DOI] [PubMed] [Google Scholar]
- 71.Sharaiha RZ, Hajifathalian K, Kumar R, et al. Five-year outcomes of endoscopic sleeve gastroplasty for the treatment of obesity. Clin Gastroenterol Hepatol. 2021;19:1051-1057.e2. [DOI] [PubMed] [Google Scholar]
- 72.Kelly J, Menon V, O’Neill F, et al. UK cost-effectiveness analysis of endoscopic sleeve gastroplasty versus lifestyle modification alone for adults with class II obesity. Int J Obes (Lond). 2023;47:1161–70. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 73.Saumoy M, Gandhi D, Buller S, et al. Cost-effectiveness of endoscopic, surgical and pharmacological obesity therapies: a microsimulation and threshold analyses. Gut. 2023;72:2250–9. [DOI] [PubMed] [Google Scholar]
- 74.Haseeb M, Chhatwal J, Xiao J, et al. Semaglutide vs endoscopic sleeve gastroplasty for weight loss. JAMA Netw Open. 2024;7:e246221. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 75.Gala K, Ghusn W, Brunaldi V, et al. Outcomes of concomitant antiobesity medication use with endoscopic sleeve gastroplasty in clinical US settings. Obes Pillars. 2024;11:100112. [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Data Availability Statement
No datasets were generated or analysed during the current study.