

ABSTRACT
Introduction
Digital simulation in dental education has substantially evolved, addressing several educational challenges in dentistry. Following global lockdowns and sustainability concerns, dental educators are increasingly adopting digital simulation to enhance or replace traditional training methods. This review aimed to contribute to a uniform taxonomy for extended reality (XR) simulation within dental education.
Methods
This scoping review followed the PRISMA and PRISMA‐ScR guidelines. PubMed/MEDLINE, EMBASE, Web of Science and Google Scholar were searched. Eligible studies included English‐written publications in indexed journals related to digital simulation in dental/maxillofacial education, providing theoretical descriptions of extended reality (XR) and/or immersive training tools (ITT). The outcomes of the scoping review were used as building blocks for a uniform of XR‐simulation taxonomy.
Results
A total of 141 articles from 2004 to 2024 were selected and categorised into Virtual Reality (VR), Mixed Reality (MR), Augmented Reality (AR), Augmented Virtuality (AV) and Computer Simulation (CS). Stereoscopic vision, immersion, interaction, modification and haptic feedback were identified as recurring features across XR‐simulation in dentistry. These features formed the basis for a general XR‐simulation taxonomy.
Discussion
While XR‐simulation features were consistent in the literature, the variety of definitions and classifications complicated the development of a taxonomy framework. VR was frequently used as an umbrella term. To address this, operational definitions were proposed for each category within the virtuality continuum, clarifying distinctions and commonalities.
Conclusion
This scoping review highlights the need for a uniform taxonomy in XR simulation within dental education. Establishing a consensus on XR‐related terminology and definitions facilitates future research, allowing clear evidence reporting and analysis. The proposed taxonomy may also be of use for medical education, promoting alignment and the creation of a comprehensive body of evidence in XR technologies.
Keywords: augmented reality, dental education, extended reality, haptics, mixed reality, virtual reality
1. Introduction
The development of digital simulation in dental education emerged as a strategy to cope with imperative simodontal challenges. Limitations associated with extracted teeth for training, challenging recruitment of patients, curriculum overcrowding, and shortages of teachers in dental schools are recurrently reported in the literature. Furthermore, with the continuous aim to improve quality and growing accountability requirements for schools, the need to provide evidence of clinical competence together with the striving for patient‐free clinical assessments has drastically pushed forward technological innovation for dental training [1, 2, 3, 4, 5].
Following several worldwide lockdowns, current climate changes and growing sustainability requirements in dental training, dental educators have drastically changed their teaching strategies [5, 6, 7, 8]. Digital simulation technologies are increasingly being implemented in dental schools, complementing or replacing traditional preclinical and clinical training. These technologies offer opportunities such as haptics, rotative views, real‐time feedback and objective assessment, providing students with unlimited opportunities for practice at their own pace, without producing disposables or waste [4, 9, 10, 11, 12, 13]. These opportunities also facilitate training within the model of deliberate practice, essential for achieving expert performance outcomes, involving structured tasks with well‐defined goals, continuous feedback and ample opportunities for repetition, which are feasible in simulated digital environments as preparation for a clinical task [2, 13, 14].
At this point in the development and implementation of digital simulation in dentistry, different training systems, including desktop pcs, haptic desktops, digitally enhanced phantom heads, along with digital dental trainers based on haptic virtual reality (VR), augmented reality (AR) and mixed reality (MR), have been consistently addressed in the literature with the collective term of VR‐simulation [12, 15, 16, 17]. Several authors have delivered some theoretical structure to the matter of digital simulation in dental education. However, the variety of approaches reported in the literature entangles an accurate description of the available technologies, thus building up a puzzling body of evidence that challenges both device and research outcomes comparison [3, 12, 16, 18].
The conventional understanding of a VR environment is frequently addressed as a completely synthetic digital world in which the operator is entirely immersed, and interaction is achievable. The following three features are therefore key to defining VR: complete synthesis, immersion and interaction. Where VR and the real world merge, arises the concept of Mixed Reality (MR). MR includes several types of hybrid environments and is defined as any case in which an otherwise real environment is ‘augmented’ by means of virtual objects [19, 20]. The concepts of Extended Reality (XR) and Immersive Training Tools (ITT) gradually become prominent in the literature as more accurate collective terms for the different digital simulation options in healthcare training.
These concepts fit the understanding of a ‘virtuality continuum’ moving from reality to virtuality and the immersion prerequisite when it comes to digital simulation trainers [21, 22, 23, 24, 25].
The broad hardware differences between the available simulation devices and the various technologies incorporated, add another dimension of complexity when it comes to describing and comparing XR simulation for research purposes or to make educational choices [3, 21, 26]. Two main hardware components constitute the base of dental XR‐simulation: an ergonomic multi‐sensory collocation platform that facilitates an immersive interaction between the operator and the virtual environment and a haptic device to provide stable and high‐fidelity force/torque feedback to the operator's hand [27].
Defining key concepts and terms is critical in scoping reviews. In dentistry, however, the categories of XR‐simulation often intersect and are not distinctly defined [18]. Carroll et al. [28] also showed that 70% of the related articles in medical digital simulation either ‘misidentified or misclassified’ simulation types, highlighting the ambiguity surrounding proper definitions. Similarly, Kardong‐Edgren et al. [29] also noted that the terminology for VR in the field of medicine lacks consistency.
The present scoping review was conducted to assess the current use of XR‐related taxonomy in dental education research in order to generate a definitional uniformity. This involves examining how different XR technologies are described in dental education research and determining the feasibility of achieving a general description framework.
2. Materials and Methods
This review was peer‐reviewed and designed following the Preferred Reporting Items for Systematic reviews and Meta‐Analyses (PRISMA) and PRISMA extension for Scoping Reviews (PRISMA‐ScR) guidelines for conducting systematic scoping reviews [30, 31]. The study protocol was developed based on the PRISMA protocol guidelines (PRIMA‐p) and registered on the Open Science Framework (https://osf.io/ys849) [30]. PubMed/MEDLINE, EMBASE and Web of Science were searched in July 2024. Additional research was also carried out in the grey literature using Google Scholar, as well as a manual search on reference lists of the included studies. An online software reference manager (EndNote X7, Thomson Reuters, Philadelphia, PA) was used to collect references and remove duplicate articles.
2.1. Eligibility Criteria
Peer‐reviewed, English‐written publications in indexed journals, referring to development, implementation, assessment and/or research regarding digital simulation in dental/maxillofacial education were included in this review, without any limitations regarding study design or year of publication. Each study must include a theoretical description of XR and/or the investigated ITT.
2.2. Exclusion Criteria
Articles regarding digital simulation outside the dental/maxillofacial field, not providing definitions or a theoretical frame about the systems researched, and reports about the use of XR for dental phobia or any other purpose that did not involve dental education were excluded from this selection.
2.3. Selection of Sources of Evidence
The performed search strategy included the different variations of XR and hardware in dental ITT, together with their different applications in dental education. (Table 1) The selection was carried out in two phases. In phase one, three dentists/teachers experienced with XR‐simulation in dentistry, independently screened titles and abstracts of all identified references. In phase two, the same three reviewers applied the eligibility criteria to the full texts. Any disagreement was solved by a consensus discussion. The final selection was based on the full text of the publication. Collected data items included author, year, XR definition, used hardware and systems, and related description.
TABLE 1.
General search strategy.
| (“computer simulation”[tiab] OR “motion tracking”[tw] OR “augmented reality”[tiab] OR “virtual reality”[tiab] OR “mixed reality”[tiab]) AND (“force feedback”[tw] OR haptic*[tw] Or depth[tw] OR perception[tw] OR 3D [tw] OR stereoscopic[tw] OR immer*[tw] OR scan*[tw]) AND (dentistry[MeSH Terms] OR oral surgery[MeSH Terms] OR prosthodontics[MeSH Terms] OR orthodontics[MeSH Terms] OR endodontics[MeSH Terms] OR cariology[tw] OR crown[tw] OR preparation[tw] OR implant*[tiab] OR dent*[tiab] OR restorat*[tiab] OR exodont*[tiab] OR stomatol*[tiab] OR oral*[tw]) AND (educat*[tw] OR didact*[tw] OR learn*[tw] OR teach*[tw] OR train*[tw] OR licenc*[tw] OR test*[tw] OR assess*[tw]) |
A systematic narrative synthesis was completed with information presented in the text and tables to summarise and explain the characteristics and findings of the included studies. The narrative synthesis explored the relationship and findings both within and between the included studies to build general definitions for XR in dental education and achieve a uniform description of the existing technologies within the frame of the presented taxonomy. Atlas.ti (GmbH, Berlin, Germany) was used for this analysis.
3. Results
The literature search provided 1.197 results from 3 search engines: 485 from PubMed, 437 from Embase and 275 from Web of Science. Of these results, 838 were excluded during the title filtering process, leaving 359. After that, 52 duplicate studies were excluded, leaving 307. In the final screening, 166 papers were excluded after reviewing the full‐text articles. Afterwards, the reference lists were reviewed and assessed for eligibility, leaving 141 articles for the final review (Figure 1). The relevant articles spanned a period from 2004 to 2024. The selected studies were related to digital simulation in dental/maxillofacial education, including a theoretical description of XR.
FIGURE 1.

Preferred Reporting Items for Systematic Reviews and Meta‐Analyses (PRISMA) flowchart illustrating the process used in the selection of specific articles.
The selected studies were categorised based on the type of simulation: VR, MR, including AR, augmented virtuality (AV) and, finally, computer simulation (CS). (Figure 2).
FIGURE 2.
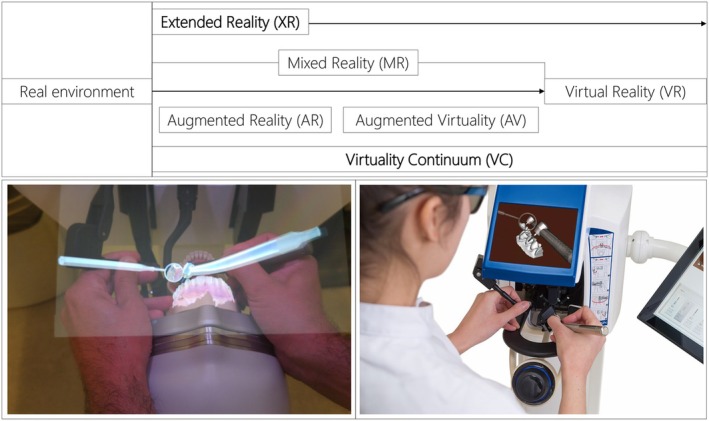
Virtuality continuum adaptation from Milgram & Kishino [19] (a) Augmented Reality (AR) – SimtoCare Dente (SimtoCare, Vreeland, the Netherlands). (b) Virtual Reality (VR) – Simodont Dental Trainer (Nissin, Nieuw Vennep, the Netherlands).
Within each category, definitions and/or descriptions were extracted and are presented in Table 2.
TABLE 2.
Categorisation of selected studies.
| Type of simulation | Countries | Years | N | References |
|---|---|---|---|---|
| Virtual Reality (VR) | Japan, Taiwan, China, Thailand, India, Korea, Israel, Iran, Saudi Arabia, Pakistan, Austria, Poland, Switzerland, England, France, the Netherlands, Italy, Portugal, Germany, Finland, the United States, Canada, Australia, Brazil, Mexico, Cyprus, Latvia, Qatar, Turkey | 2004–2024 | 95 | [2, 9, 16, 18, 20, 21, 22, 24, 26, 27, 31, 32, 33, 34, 35, 36, 37, 38, 39, 40, 41, 42, 43, 44, 45, 46, 47, 48, 49, 50, 51, 52, 53, 54, 55, 56, 57, 58, 59, 60, 61, 62, 63, 64, 65, 66, 67, 68, 69, 70, 71, 72, 73, 74, 75, 76, 77, 78, 79, 80, 81, 82, 83, 84, 85, 86, 87, 88, 89, 90, 91, 92, 93, 94, 95, 96, 97, 98, 99, 100, 101, 102, 103, 104, 105, 106, 107, 108, 109, 110, 111, 112, 113, 114, 115, 116, 117] |
| Mixed Reality (MR) | Austria, Italy, Portugal, Germany, England, Japan, the United States, Cyprus, Qatar, Singapore | 2016–2024 | 13 | [16, 20, 21, 24, 39, 74, 75, 96, 98, 99, 114, 118, 119] |
| Augmented Reality (AR) | Spain, Poland, Austria, England, Germany, Switzerland, Italy, Portugal, Serbia, Pakistan, Korea, Taiwan, Iran, China, Australia, the United States, Canada, Brazil, France, Qatar, Turkey, Saudi Arabia | 2004–2024 | 50 | [3, 16, 20, 21, 24, 37, 38, 39, 44, 48, 49, 50, 51, 53, 54, 55, 58, 60, 65, 66, 71, 74, 88, 89, 99, 102, 105, 107, 108, 109, 111, 120, 121, 122, 123, 124, 125, 126, 127, 128, 129, 130, 131, 132, 133, 134, 135, 136, 137] |
| Augmented Virtuality (AV) | France, Qatar | 2019, 2024 | 2 | [18, 36] |
| Computer Simulation (CS) | Germany, France, England, the United States, Mexico, China, Saudi Arabia | 2007–2022 | 9 | [9, 22, 36, 47, 138, 139, 140, 141, 142] |
Ninety‐five (n = 95) studies included a definition/description of VR. The most recurrent features within these definitions were stereoscopic (3D) visualisation of models and/or environments (n = 51) and different degrees of user immersion (n = 42), including complete immersion systems, semi‐immersion systems and non‐immersion systems. The ability of the user to interact with the simulated models (n = 47), and tactile sensation or haptic feedback (n = 29) were also repeatedly mentioned. The ability of the user to modify the virtual models was only mentioned in a smaller group of studies (n = 9) and different VR‐devices were mentioned: VR‐dental‐simulation‐devices (n = 6), VR‐Headsets (n = 27), VR‐desktop‐devices (n = 9) and smartphones (n = 2).
MR was only defined in thirteen (n = 13) of the selected studies, mainly as a blend between the physical and the virtual worlds. Fifty (n = 50) of the selected articles provided a definition of AR within dental or maxillofacial education. In these definitions, the most relevant features included AR as a combination, blend or superimposition of digital information on the real world (n = 47) that enhances, enriches or augments the real world with digital elements (n = 41) and allows interaction with the user (n = 16). These digital elements can be merely informative (textual or numerical data) but mostly include 3D models (n = 12). The concept of augmented virtuality (AV) is only mentioned twice (n = 2) as the inclusion of real elements in a virtual environment, digitally imposing an image of the user in the virtual environment, enhancing in this way the virtual world.
CS or desktop simulation was also described in nine (n = 9) of the selected articles. CS was mostly used as an umbrella term for computer‐assisted simulation in general (n = 6), while only three (n = 3) articles approached CS as desktop training modules.
General features of XR‐simulation in dentistry are presented in Table 3. XR features that were recurrently found in the reviewed literature included stereoscopic (3D) vision, users' immersion, interaction, modification possibilities and the presence of haptic feedback. These features are generally part of the description of XR devices and provide a standardisation ground, that is building blocks, for XR taxonomy in dentistry.
TABLE 3.
Digital simulation in dental education within the virtuality continuum and main available features.
| Simulation type Features | Virtual reality | Mixed Reality | Computer Simulation | |
|---|---|---|---|---|
| Augmented Reality | Augmented Virtuality | |||
| Stereoscopic vision | Available | Available | Available | Not available |
| Immersion | Complete/Semi | Complete/Semi | Complete/Semi | None |
| Interaction | Direct manipulation of virtual models | Direct manipulation of virtual models | Direct manipulation of virtual models | Mouse/keyboard/touch screen manipulation of virtual models |
| Haptic feedback | Available | Available | May or may not be available | May or may not be available |
| Modification | Direct modification of virtual models | Direct modification of virtual models | Direct modification of virtual models | Editing software |
Source: Adaptation from Saghiri, Vakhnovetsky & Nadershahi [18].
3.1. Stereoscopic Vision
The concept of stereoscopic vision is related to the ability to provide 3D images through binocular vision. To achieve the reception of 3D images by the human eyes in a digital environment, two identical images with a slight difference in the focus position with respect to the horizontal plane, positioned side by side, are projected using a polarised filter, which may be given by 3D glasses or a screen [92]. The result of this process provides the user with the perception of depth, which has a dominant effect on the feeling of immersion [79, 92, 143]. Several XR‐simulation devices in dental education are equipped with stereoscopic displays, for example Simodont Dental Trainer, SimtoCare Dente and Virteasy (HRV Simulation, Changé, France).
3.2. Immersion
This feature defines the degree of perception of the virtual world by the user. The higher the level of immersion, the deeper the user's mental engagement and the stronger the feeling of being in an authentic environment. To provide a high degree of immersion to the user in simulated dental procedures, various technological tools are used, such as optical devices that provide stereoscopic vision, devices for tracking movements (body, head) and haptic technology. The different degrees of immersion of the user have been defined as complete immersion, semi‐immersion and non‐immersion systems [3, 27, 53].
3.3. Interaction
In the field of digital dentistry, the concept of interaction refers to the ability of the user to perform different actions on a virtual object projected in a digital device, such as rotation, translation, increase or decrease of the size, selection or discarding. This interaction can be performed, among others, by using hands on a touch screen, a computer mouse, a keyboard, haptic gloves, virtual instruments and motion‐tracking devices [21, 51].
3.4. Modification
The term modification refers to the ability of the user to transform, in terms of shape and volume, a virtual object according to the task to perform. It differs from interaction in the capability of creating something new or delivering a new outcome from an existing model; that is, to say the capability to transform a digital model instead of only manipulating it [51].
3.5. Haptic Technology
The term ‘haptic’ means relating to or proceeding from the sense of touch [143]. In XR simulation it is possible to translate tactile sensations to the user and allow them to feel digital objects programmed under volumetric algorithms. A manipulation device is required to deliver force feedback; this is normally a robotic arm able to apply a degree of opposing force to the user along the x, y and z axes [52]. A remarkable characteristic is that the force feedback can vary depending on the simulated scenario, specifically in XR simulation for dental education, as there are several kinds of interaction algorithms made to replicate specific scenarios such as drilling into different dental tissues, ultrasound scaling or bone drilling [81]. This technology allows the users to interact with a 3D object and also bring modifications into the virtual world. Several authors have related the use of haptic technology to XR dental simulators as a crucial factor for successful implementation, users' acceptance and performance [33, 37, 42, 50]. McAlphin et al. [56] mentioned that a haptic‐enhanced XR simulator provides accurate skill training by means of hand‐eye coordination, the sense of resistance, touch and direct feedback.
4. Discussion
Articles included in this scoping review provided a wide definition range regarding the different environments available in dentistry within the virtuality continuum and their characteristic features. Although many authors agreed on the main features of XR‐simulation for dental education, the encountered classification and description of the different systems reported were widely dissimilar, challenging the consolidation of a general taxonomy for XR‐simulation while complicating evidence appraisal and comparisons between systems.
Available generic definitions from the XR‐engineering world may differ from those available for simulation in dentistry. This is due to the specificity of the simulated procedures and their characteristics in dentistry. To achieve a general taxonomy of XR‐simulation in dental education, features that were recurrently found in the reviewed literature were used as building blocks to achieve a general definition of AR, VR, MR, AV and CS in dentistry. These features included stereoscopic (3D) vision, different levels of user's immersion, interaction, modification possibilities and the presence of haptic feedback. Together with traditional definitions of XR, which originated from computer sciences, [19] general definitions of the different components of the virtuality continuum were formulated to facilitate a better understanding of the available evidence.
Based on this review, VR is frequently used in dental education as an umbrella term for all forms of XR‐simulation environments. The conventionally held view of a VR environment is a completely synthetic world in which the participant is totally immersed and able to interact with. Such a world may mimic the properties of some real‐world environments, either existing or fictional; however, it can also exceed the bounds of physical reality [1, 19, 90, 109]. What may be overlooked in this definition, however, is that the VR label is also frequently used in association with a variety of other environments, to which total immersion and complete synthesis do not necessarily pertain but which fit somewhere else along a virtuality continuum [17, 19, 61]. VR can be defined, therefore, specifically for dental education, as a completely synthetic world with stereoscopic vision in which the participant is totally immersed and able to interact with haptic feedback while also being able to modify virtual objects. An example of a VR dental simulator is the Simodont Dental Trainer. (Figure 2a) This simulator uses 3D glasses and a 3D display to acquire stereoscopic vision and an arm with haptic feedback connected to an air rotor to simulate hardness [92]. As mentioned before, when using the term VR to describe a system, it is important that there is a complete immersion of the user in the virtual environment [19, 20].
MR was only defined in thirteen of the selected studies, mainly as a blend between the physical and the virtual worlds. MR is the merging of the real and virtual worlds. The most straightforward way to view a MR environment is one in which objects from both the real and the virtual world are presented together within a single display, that is, anywhere between the extremes of the virtuality continuum [18, 19]. A rather uniform vision about MR was found in this scoping review; however, a more specific classification including AR and AV might be necessary to improve taxonomical accuracy in the literature. The level of immersion in the MR environment can be complete, semi‐immersive or non‐immersive depending on how the environment is displayed while the objects within the environment can be interacted with and modified. Immersion, interaction and modification can all be achieved on different levels in dental MR‐simulation, depending on the instruments available in the different environments, such as VR‐headsets, haptic feedback or specific cutting/rotary instruments [16, 20, 21, 22, 24, 39, 74, 96, 97].
Within the definitions or descriptions used in the selected literature for AR, the most frequent description found included AR as a superimposition of digital information into the real world that enhances or augments the real world with digital elements and allows interaction with the user, in line with the general definition of AR. These digital elements can be merely informative (textual or numerical data) but mostly include 3D models [19]. In consequence, an operational definition of AR in dental simulation includes any simulated environment in which an otherwise real environment is ‘augmented’ by means of virtual (computer generated) dentistry‐related objects. AR is often used in a digital simulation environment, superimposing virtual objects on real structures, allowing users to visualise the virtual content, such as surgical plans or anatomical structures, superimposed on the real surgical field [51, 58, 89, 144]. SimtoCare Dente is an accurate example of an AR‐dental trainer in which digital models are projected on a real phantom head for context and physical support in order to provide a close‐to‐reality experience [13]. (Figure 2b) On the other hand, AV can be defined as a subclass of MR in which a virtual environment is augmented by means of superimposed representations of real objects. The virtual environment and its objects can interact with the digital representation of real objects and be modified. In both AR and AV, the virtual environment and/or objects can be manipulated and modified; what changes is the original environment that is being augmented [3, 16, 18, 20, 21, 24, 36, 37, 39, 44, 49, 50, 51, 53, 54, 55, 58, 60, 65, 66, 71, 74, 88, 90, 120, 121, 123, 124, 125, 126, 127, 128, 129, 130, 131, 132, 133, 134, 135, 136, 137].
Finally, CS is an umbrella term used for computer‐assisted simulation in general, which presents a digital training environment where stereoscopic vision and immersion are not available as objects are displayed in a single screen. Interaction of the user with digital objects is only provided through mouse, keyboard or touch screen manipulation, although haptic feedback might be present through simple force feedback devices [9, 36, 47, 116, 117, 118]. CS has, however, not been placed in the virtuality continuum for dental XR simulation as it lacks any degree of immersion (Figure 2).
Agreeing on a general taxonomy for XR‐simulation in dental education provides the opportunity to review available literature from a standard perspective while correctly formulating and referring to simulation research in the future. Furthermore, it would be interesting to also carry out this exercise for XR‐technologies in the medical education domain to align terminologies between healthcare education and dentistry and allow the construction of a collective body of evidence.
Achieving a uniform taxonomy for XR simulation for dental education could also support the selection of suitable devices for the diverse needs of different dental schools. The present review focused on the taxonomy for XR technology in dental education and did not summarise the learning outcomes of XR training or the effect of the different components of this technology on the learning process, which could also support the selection of devices. Future research should consider longitudinal studies to describe the learning process with XR simulation including long‐term skill retention, transferability to clinical settings. Future reviews could also incorporate publications in other languages and a more diverse number of search engines.
Standardising XR terminology and methodologies through the development of guidelines and collaborative efforts will enhance comparability and consistency across studies, thus improving the generalisability of the findings. Enhancing technological accessibility by exploring cost‐effective solutions and improving usability can reduce barriers to adoption. Comprehensive studies on user experience and the development of robust training and support systems will also help maximise the potential of XR technologies in dental education.
5. Conclusion
This scoping review highlighted the challenges in establishing a general taxonomy for extended reality (XR) simulation in dental education. While agreement was found among authors regarding the main features of XR‐simulation, such as stereoscopic vision, immersion, interaction, haptic feedback and modification of digital models, there was a lack of consensus in the general definitions within the virtuality continuum. Virtual reality (VR) was commonly used as an umbrella term for several XR‐simulation environments, even though it encompasses a completely synthetic world where users are fully immersed, interact with the environment and can modify virtual objects. The presented taxonomy offers opportunities to relate findings more precisely to the specific technologies, avoiding misinterpretation of evidence. Mixed reality (MR) combines real and virtual worlds, allowing various levels of immersion, interaction and modification. Augmented reality (AR) augments the real world with virtual objects, enabling interaction and modification of the augmented environment. Augmented Virtuality (AV) augments a virtual environment with representations of real objects, offering similar interaction and modification capabilities.
Conflicts of Interest
The authors declare no conflicts of interest.
Acknowledgements
The authors sincerely thank the collaboration of Anton Mens and Klaas Jan van Egmond for their valuable input.
Funding: The authors received no specific funding for this work.
Data Availability Statement
The data that support the findings of this study are available from the corresponding author upon reasonable request.
References
- 1. Perry S., Bridges S. M., and Burrow M. F., “A Review of the Use of Simulation in Dental Education,” Simulation in Healthcare 10 (2015): 31–37. [DOI] [PubMed] [Google Scholar]
- 2. Serrano C. M., Wesselink P. R., and Vervoorn J. M., “First Experiences With Patient‐Centered Training in Virtual Reality,” Journal of Dental Education 84 (2020): 607–614. [DOI] [PubMed] [Google Scholar]
- 3. Towers A., Field J., Stokes C., Maddock C., and Martin N., “A Scoping Review of the Use and Application of Virtual Reality in Pre‐Clinical Dental Education,” British Dental Journal 226 (2019): 358–366. [DOI] [PubMed] [Google Scholar]
- 4. De Boer I. R., Bakker D. R., Serrano C. M., Koopman P., Wesselink P. R., and Vervoorn J. M., “Innovation in Dental Education: The “On‐The‐Fly” Approach to Simultaneous Development, Implementation and Evidence Collection,” European Journal of Dental Education 22 (2018): 215–222. [DOI] [PubMed] [Google Scholar]
- 5. Chu T.‐M. G., Makhoul N. M., Silva D. R., Gonzales T. S., Letra A., and Mays K. A., “Should Live Patient Licensing Examinations in Dentistry Be Discontinued? Two Viewpoints,” Journal of Dental Education 82 (2018): 246–251. [DOI] [PubMed] [Google Scholar]
- 6. Chuenjitwongsa S., Oliver R. G., and Bullock A. D., “Competence, Competency‐Based Education, and Undergraduate Dental Education: A Discussion Paper,” European Journal of Dental Education 22 (2018): 1–8. [DOI] [PubMed] [Google Scholar]
- 7. Duane B., Dixon J., Ambibola G., et al., “Embedding Environmental Sustainability Within the Modern Dental Curriculum—Exploring Current Practice and Developing a Shared Understanding,” European Journal of Dental Education 25 (2021): 541–549. [DOI] [PubMed] [Google Scholar]
- 8. Field J., Martin N., Duane B., et al., “Embedding Environmental Sustainability Within Oral Health Professional Curricula—Recommendations for Teaching and Assessment of Learning Outcomes,” European Journal of Dental Education 27, no. 3 (2023): 650–661. [DOI] [PubMed] [Google Scholar]
- 9. Nassar H. M. and Tekian A., “Computer Simulation and Virtual Reality in Undergraduate Operative and Restorative Dental Education: A Critical Review,” Journal of Dental Education 84 (2020): 812–829. [DOI] [PubMed] [Google Scholar]
- 10. Vincent M., Joseph D., Amory C., et al., “Contribution of Haptic Simulation to Analogic Training Environment in Restorative Dentistry,” Journal of Dental Education 84 (2020): 367–376. [DOI] [PubMed] [Google Scholar]
- 11. Serrano C. M., Botelho M. G., Wesselink P. R., and Vervoorn J. M., “Challenges in the Transition to Clinical Training in Dentistry: An ADEE Special Interest Group Initial Report,” European Journal of Dental Education 22 (2018): e451–e457. [DOI] [PubMed] [Google Scholar]
- 12. Moussa R., Alghazaly A., Althagafi N., Eshky R., and Borzangy S., “Effectiveness of Virtual Reality and Interactive Simulators on Dental Education Outcomes: Systematic Review,” European Journal of Dentistry 16 (2022): 14–31. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13. Serrano C. M., Bakker D. R., Zamani M., et al., “Virtual Reality and Haptics in Dental Education: Implementation Progress and Lessons Learned After a Decade,” European Journal of Dental Education 27, no. 4 (2023): 833–840. [DOI] [PubMed] [Google Scholar]
- 14. Ericsson A., “Deliberate Practice and Acquisition of Expert Performance: A General Overview,” Academic Emergency Medicine 15 (2008): 988–994. [DOI] [PubMed] [Google Scholar]
- 15. Higgins D., Hayes M. J., Taylor J. A., and Wallace J. P., “How Do We Teach Simulation‐Based Dental Education? Time for an Evidence‐Based, Best‐Practice Framework,” European Journal of Dental Education 24 (2020): 815–821. [DOI] [PubMed] [Google Scholar]
- 16. Monterubbianesi R., Tosco V., Vitiello F., et al., “Augmented, Virtual and Mixed Reality in Dentistry: A Narrative Review on the Existing Platforms and Future Challenges,” Applied Sciences 12 (2022): 877. [Google Scholar]
- 17. Leblanc V. R., Urbankova A., Hadavi F., and Lichtenthal R. M., “A Preliminary Study in Using Virtual Reality to Train Dental Students,” Journal of Dental Education 68 (2004): 378–383. [PubMed] [Google Scholar]
- 18. Al Hamad K. Q., Said K. N., Engelschalk M., et al., “Taxonomic Discordance of Immersive Realities in Dentistry: A Systematic Scoping Review.: Taxonomic Discordance of Immersive Realities,” Journal of Dentistry 146 (2024): 105058. [DOI] [PubMed] [Google Scholar]
- 19. Milgram P. and Kishino F., “A Taxonomy of Mixed Reality Visual Displays,” IEICE Transactions on Information and Systems 77 (1994): 1321–1329. [Google Scholar]
- 20. Blanchard J., Koshal S., Morley S., and Mcgurk M., “The Use of Mixed Reality in Dentistry,” British Dental Journal 233 (2022): 261–265. [DOI] [PubMed] [Google Scholar]
- 21. Ma S., Vakhnovetsky J., and Nadershahi N., “Scoping Review of Artificial Intelligence and Immersive Digital Tools in Dental Education,” Journal of Dental Education 86 (2022): 736–750. [DOI] [PubMed] [Google Scholar]
- 22. Liebermann A., Seefelder J. K., Huth K. C., and Erdelt K., “Mobile Virtual Tooth Morphology Teaching Environment for Preclinical Dental Students,” Journal of Dental Education 87 (2023): 130–138. [DOI] [PubMed] [Google Scholar]
- 23. Zweifach S. M. and Triola M. M., “Extended Reality in Medical Education: Driving Adoption Through Provider‐Centered Design,” Digital Biomarkers 3 (2019): 14–21. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24. Sukotjo C., Schreiber S., Li J., Zhang M., Chia‐Chun Yuan J., and Santoso M., “Development and Student Perception of Virtual Reality for Implant Surgery,” Education in Science 11 (2021): 176. [Google Scholar]
- 25. Taylor L., Dyer T., Al‐Azzawi M., Smith C., Nzeako O., and Shah Z., “Extended Reality Anatomy Undergraduate Teaching: A Literature Review on an Alternative Method of Learning,” Annals of Anatomy – Anatomischer Anzeiger 239 (2022): 151817. [DOI] [PubMed] [Google Scholar]
- 26. Imran E., Adanir N., and Khurshid Z., “Significance of Haptic and Virtual Reality Simulation (Vrs) in the Dental Education: A Review of Literature,” Applied Sciences 11 (2021): 10196. [Google Scholar]
- 27. Wang D., Li T., Zhang Y., and Hou J., “Survey on Multisensory Feedback Virtual Reality Dental Training Systems,” European Journal of Dental Education 20 (2016): 248–260. [DOI] [PubMed] [Google Scholar]
- 28. Carroll J., Hopper L., Farrelly A. M., Lombard‐Vance R., Bamidis P. D., and Konstantinidis E. I., “A Scoping Review of Augmented/Virtual Reality Health and Wellbeing Interventions for Older Adults: Redefining Immersive Virtual Reality,” Frontiers in Virtual Reality 2 (2021): 655338. [Google Scholar]
- 29. Kardong‐Edgren S. S., Farra S. L., Alinier G., and Young H. M., “A Call to Unify Definitions of Virtual Reality,” Clinical Simulation in Nursing 31 (2019): 28–34. [Google Scholar]
- 30. Shamseer L., Moher D., Clarke M., et al., “Preferred Reporting Items for Systematic Review and Meta‐Analysis Protocols (Prisma‐p) 2015: Elaboration and Explanation,” British Medical Journal 349 (2015): g7647. [DOI] [PubMed] [Google Scholar]
- 31. Sakowitz S. M., Inglehart M. R., and Ramaswamy V., “A Comparison of Two‐Dimensional Prediction Tracing and a Virtual Reality Patient Methods for Diagnosis and Treatment Planning of Orthognathic Cases in Dental Students: A Randomized Preliminary Study,” Virtual Reality 24 (2020): 399–409. [Google Scholar]
- 32. Urbankova A., Palomo L., and Engebretson S. P., “A Complex Haptic Exercise to Predict Pre‐Clinic Operative Dentistry Performance: A Prospective Study,” Journal of Dental Education 86 (2022): 1628–1633. [DOI] [PubMed] [Google Scholar]
- 33. Serrano C., Wesselink P., and Vervoorn J., “Real Patients in Virtual Reality: The Link Between Phantom Heads and Clinical Dentistry,” Nederlands Tijdschrift voor Tandheelkunde 125 (2018): 263–267. [DOI] [PubMed] [Google Scholar]
- 34. Razavi M., Talebi H. A., Zareinejad M., and Dehghan M. R., “A Gpu‐Implemented Physics‐Based Haptic Simulator of Tooth Drilling,” International Journal of Medical Robotics and Computer Assisted Surgery 11 (2015): 476–485. [DOI] [PubMed] [Google Scholar]
- 35. Iwanaga J., Kamura Y., Nishimura Y., et al., “A New Option for Education During Surgical Procedures and Related Clinical Anatomy in a Virtual Reality Workspace,” Clinical Anatomy 34 (2021): 496–503. [DOI] [PubMed] [Google Scholar]
- 36. Lutz J.‐C., Hostettler A., Agnus V., et al., “A New Software Suite in Orthognathic Surgery: Patient Specific Modeling, Simulation and Navigation,” Surgical Innovation 26 (2019): 5–20. [DOI] [PubMed] [Google Scholar]
- 37. Lin Y. K., Yau H. T., Wang I. C., Zheng C., and Chung K. H., “A Novel Dental Implant Guided Surgery Based on Integration of Surgical Template and Augmented Reality,” Clinical Implant Dentistry and Related Research 17 (2015): 543–553. [DOI] [PubMed] [Google Scholar]
- 38. Chen X. and Hu J., “A Review of Haptic Simulator for Oral and Maxillofacial Surgery Based on Virtual Reality,” Expert Review of Medical Devices 15 (2018): 435–444. [DOI] [PubMed] [Google Scholar]
- 39. Lungu A. J., Swinkels W., Claesen L., Tu P., Egger J., and Chen X., “A Review on the Applications of Virtual Reality, Augmented Reality and Mixed Reality in Surgical Simulation: An Extension to Different Kinds of Surgery,” Expert Review of Medical Devices 18 (2021): 47–62. [DOI] [PubMed] [Google Scholar]
- 40. Mansoory M. S., Azizi S. M., Mirhosseini F., Yousefi D., and Moradpoor H., “A Study to Investigate the Effectiveness of the Application of Virtual Reality Technology in Dental Education,” BMC Medical Education 22 (2022): 457. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 41. Rhienmora P., Haddawy P., Khanal P., Suebnukarn S., and Dailey M. M., “A Virtual Reality Simulator for Teaching and Evaluating Dental Procedures,” Methods of Information in Medicine 49 (2010): 396–405. [DOI] [PubMed] [Google Scholar]
- 42. Wu F., Chen X., Lin Y., et al., “A Virtual Training System for Maxillofacial Surgery Using Advanced Haptic Feedback and Immersive Workbench,” International Journal of Medical Robotics and Computer Assisted Surgery 10 (2014): 78–87. [DOI] [PubMed] [Google Scholar]
- 43. Suebnukarn S., Hataidechadusadee R., Suwannasri N., Suprasert N., Rhienmora P., and Haddawy P., “Access Cavity Preparation Training Using Haptic Virtual Reality and Microcomputed Tomography Tooth Models,” International Endodontic Journal 44 (2011): 983–989. [DOI] [PubMed] [Google Scholar]
- 44. Bosshard‐Gerber F., Valdec S., Dehghani N., Wiedemeier D., Fürnstahl P., and Stadlinger B., “Accuracy of Augmented Reality‐Assisted vs. Template‐Guided Apicoectomy—An Ex Vivo Comparative Study,” International Journal of Computerized Dentistry 20 (2022): 2305. [DOI] [PubMed] [Google Scholar]
- 45. Zorzal E., Paulo F., Rodrigues P., Mendes J. J., and Lopes D., “An Immersive Educational Tool for Dental Implant Placement: A Study on User Acceptance,” International Journal of Medical Informatics 146 (2020): 146. [DOI] [PubMed] [Google Scholar]
- 46. Pulijala Y., Ma M., Pears M., Peebles D., and Ayoub A., “An Innovative Virtual Reality Training Tool for Orthognathic Surgery,” International Journal of Oral and Maxillofacial Surgery 47 (2018): 1199–1205. [DOI] [PubMed] [Google Scholar]
- 47. Zaragoza‐Siqueiros J., Medellin‐Castillo H. I., De La Garza‐Camargo H., Lim T., and Ritchie J. M., “An Integrated Haptic‐Enabled Virtual Reality System for Orthognathic Surgery Planning,” Computer Methods in Biomechanics and Biomedical Engineering 22 (2019): 499–517. [DOI] [PubMed] [Google Scholar]
- 48. Zhou Y., Chen W., Zhao X., et al., “Application Evaluation of Virtual Reality Technology in Dental Implant Training: A New Dental Implant Training System: A Consort‐Compliant Trial,” Medicine 100 (2021): e27355. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 49. Dolega‐Dolegowski D., Proniewska K., Dolega‐Dolegowska M., et al., “Application of Holography and Augmented Reality Based Technology to Visualize the Internal Structure of the Dental Root—A Proof of Concept,” Head & Face Medicine 18 (2022): 12. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 50. Ayoub A. and Pulijala Y., “The Application of Virtual Reality and Augmented Reality in Oral & Maxillofacial Surgery,” BMC Oral Health 19 (2019): 238. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 51. Joda T., Gallucci G. O., Wismeijer D., and Zitzmann N. U., “Augmented and Virtual Reality in Dental Medicine: A Systematic Review,” Computers in Biology and Medicine 108 (2019): 93–100. [DOI] [PubMed] [Google Scholar]
- 52. Suebnukarn S., Haddawy P., Rhienmora P., Jittimanee P., and Viratket P., “Augmented Kinematic Feedback From Haptic Virtual Reality for Dental Skill Acquisition,” Journal of Dental Education 74 (2010): 1357–1366. [PubMed] [Google Scholar]
- 53. Huang T.‐K., Yang C.‐H., Hsieh Y.‐H., Wang J.‐C., and Hung C.‐C., “Augmented Reality (AR) and Virtual Reality (VR) Applied in Dentistry,” Kaohsiung Journal of Medical Sciences 34 (2018): 243–248. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 54. Fahim S., Maqsood A., Das G., et al., “Augmented Reality and Virtual Reality in Dentistry: Highlights From the Current Research,” Applied Sciences 12 (2022): 3719. [Google Scholar]
- 55. Haji Z., Arif A., Jamal S., and Ghafoor R., “Augmented Reality in Clinical Dental Training and Education,” Journal of the Pakistan Medical Association 71 (2021): s42. [PubMed] [Google Scholar]
- 56. Mcalpin E., Levine M., Brenner C., et al., “Evaluating the Effectiveness of a Virtual Reality Simulation for Preclinical Local Anaesthesia Dental Education,” European Journal of Dental Education 30 (2022): 1–12, 10.1111/eje.12854. [DOI] [PubMed] [Google Scholar]
- 57. Rantamaa H.‐R., Kangas J., Jordan M., et al., “Evaluation of Virtual Handles for Dental Implant Manipulation in Virtual Reality Implant Planning Procedure,” International Journal of Computer Assisted Radiology and Surgery 17 (2022): 1723–1730. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 58. Kwon H.‐B., Park Y.‐S., and Han J.‐S., “Augmented Reality in Dentistry: A Current Perspective,” Acta Odontologica Scandinavica 76 (2018): 497–503. [DOI] [PubMed] [Google Scholar]
- 59. Mirghani I., Mushtaq F., Allsop M. J., et al., “Capturing Differences in Dental Training Using a Virtual Reality Simulator,” European Journal of Dental Education 22 (2018): 67–71. [DOI] [PubMed] [Google Scholar]
- 60. Muff J. L., Heye T., Thieringer F. M., and Brantner P., “Clinical Acceptance of Advanced Visualization Methods: A Comparison Study of 3d‐Print, Virtual Reality Glasses, and 3d‐Display,” 3D Printing in Medicine 8 (2022): 5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 61. Gottlieb R., Lanning S. K., Gunsolley J. C., and Buchanan J. A., “Faculty Impressions of Dental students' Performance With and Without Virtual Reality Simulation,” Journal of Dental Education 75 (2011): 1443–1451. [PubMed] [Google Scholar]
- 62. Takagi D., Hayashi M., Iida T., et al., “Effects of Dental students' Training Using Immersive Virtual Reality Technology for Home Dental Practice,” Educational Gerontology 45 (2019): 670–680. [Google Scholar]
- 63. Maret D., Barrere S., Ros M., and Geeraerts T., “Clinical Gesture in Dental Education: Presentation of a New Immersive Virtual Reality Application in First Person Point‐Of‐View,” Journal of Dental Education 87, no. S1 (2022): 920–922. [DOI] [PubMed] [Google Scholar]
- 64. Hsu M.‐H., Yang H.‐W., Liu C.‐M., Chen C.‐J., and Chang Y.‐C., “Clinical Relevant Haptic Simulation Learning and Training in Tooth Preparation,” Journal of Dental Sciences 17 (2022): 1454–1457. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 65. Raja'a M. and Farid F., “Computer‐Based Technologies in Dentistry: Types and Applications,” Journal of Dentistry 13 (2016): 215. [PMC free article] [PubMed] [Google Scholar]
- 66. Farronato M., Maspero C., Lanteri V., et al., “Current State of the Art in the Use of Augmented Reality in Dentistry: A Systematic Review of the Literature,” BMC Oral Health 19 (2019): 135. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 67. Yoshida Y., Yamaguchi S., Kawamoto Y., Noborio H., Murakami S., and Sohmura T., “Development of a Multi‐Layered Virtual Tooth Model for the Haptic Dental Training System,” Dental Materials Journal 30 (2011): 1–6. [DOI] [PubMed] [Google Scholar]
- 68. Hattori A., Tonami K.‐I., Tsuruta J., et al., “Effect of the Haptic 3d Virtual Reality Dental Training Simulator on Assessment of Tooth Preparation,” Journal of Dental Sciences 17 (2022): 514–520. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 69. Maliha S. G., Diaz‐Siso J. R., Plana N. M., Torroni A., and Flores R. L., “Haptic, Physical, and Web‐Based Simulators: Are They Underused in Maxillofacial Surgery Training?,” Journal of Oral and Maxillofacial Surgery 76, no. e2424 (2018): e2421–e2424. [DOI] [PubMed] [Google Scholar]
- 70. Suebnukarn S., Haddawy P., Rhienmora P., and Gajananan K., “Haptic Virtual Reality for Skill Acquisition in Endodontics,” Journal of Endodontics 36 (2010): 53–55. [DOI] [PubMed] [Google Scholar]
- 71. Reymus M., Liebermann A., and Diegritz C., “Virtual Reality: An Effective Tool for Teaching Root Canal Anatomy to Undergraduate Dental Students–a Preliminary Study,” International Endodontic Journal 53 (2020): 1581–1587. [DOI] [PubMed] [Google Scholar]
- 72. Correa C. G., Machado M. A. A. M., Ranzini E., Tori R., and Nunes F. D. L. S., “Virtual Reality Simulator for Dental Anesthesia Training in the Inferior Alveolar Nerve Block,” Journal of Applied Oral Science 25 (2017): 357–366. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 73. Arora A., Swords C., Khemani S., et al., “Virtual Reality Case‐Specific Rehearsal in Temporal Bone Surgery: A Preliminary Evaluation,” International Journal of Surgery 12 (2014): 141–145. [DOI] [PubMed] [Google Scholar]
- 74. As F., Nicholson K., and Koka S., “Innovative Trends in Implant Dentistry Training and Education: A Narrative Review. Journal of,” Clinical Medicine 8 (2019): 1618. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 75. Lahoti K. S., Dandekar S. G., Jr G., Agrawal M. J., and Jaiswal K. V., “Knowledge, Attitude and Practice of Dental Students and Practitioners Towards Virtual Reality Based Technologies in Central India: A Cross Sectional Survey,” Journal of Pharmaceutical Research International 33 (2021): 174–183. [Google Scholar]
- 76. Huang Y., Cheng X., Chan U., et al., “Virtual Reality Approach for Orthodontic Education at School of Stomatology, Jinan University,” Journal of Dental Education 86 (2022): 1025–1035. [DOI] [PubMed] [Google Scholar]
- 77. Liebermann A. and Erdelt K., “Virtual Education: Dental Morphologies in a Virtual Teaching Environment,” Journal of Dental Education 84 (2020): 1143–1150. [DOI] [PubMed] [Google Scholar]
- 78. Rodrigues P., Esteves A., Botelho J., et al., “Usability, Acceptance, and Educational Usefulness Study of a New Haptic Operative Dentistry Virtual Reality Simulator,” Computer Methods and Programs in Biomedicine 221 (2022): 106831. [DOI] [PubMed] [Google Scholar]
- 79. Qi S., Yan Y., Li R., and Hu J., “The Impact of Active Versus Passive Use of 3d Technology: A Study of Dental Students at Wuhan University, China,” Journal of Dental Education 77 (2013): 1536–1542. [PubMed] [Google Scholar]
- 80. Yang P.‐Y. and Chang Y.‐C., “The Haptic 3d Virtual Reality Dental Training Simulator as a Good Educational Tool in Preclinical Simulation Learning,” Journal of Dental Sciences 17 (2022): 618–619. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 81. Li Y., Ye H., Ye F., et al., “The Current Situation and Future Prospects of Simulators in Dental Education,” Journal of Medical Internet Research 23 (2021): e23635. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 82. Curnier F., “Teaching dentistry by means of virtual reality–the Geneva project enseignement de l'odontologie en réalité virtuelle–l'expérience de genève,” International Journal of Computerized Dentistry 13 (2010): 251–263. [PubMed] [Google Scholar]
- 83. Dixon J., Towers A., Martin N., and Field J., “Re‐Defining the Virtual Reality Dental Simulator: Demonstrating Concurrent Validity of Clinically Relevant Assessment and Feedback,” European Journal of Dental Education 25 (2021): 108–116. [DOI] [PubMed] [Google Scholar]
- 84. Sohmura T., Hojo H., Nakajima M., et al., “Prototype of Simulation of Orthognathic Surgery Using a Virtual Reality Haptic Device,” International Journal of Oral and Maxillofacial Surgery 33 (2004): 740–750. [DOI] [PubMed] [Google Scholar]
- 85. Gb G., Ei W., Gafni N., and Ziv A., “Preliminary Assessment of Faculty and Student Perception of a Haptic Virtual Reality Simulator for Training Dental Manual Dexterity,” Journal of Dental Education 75 (2011): 496–504. [PubMed] [Google Scholar]
- 86. Hsu M.‐H., Yang H.‐W., and Chang Y.‐C., “Perspectives on the Implementation of Haptic Virtual Reality Simulator Into Dental Curriculum,” Journal of Dental Sciences 17 (2022): 1441–1442. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 87. Zafar S., Siddiqi A., Yasir M., and Zachar J., “Pedagogical Development in Local Anaesthetic Training in Paediatric Dentistry Using Virtual Reality Simulator,” European Archives of Paediatric Dentistry 22 (2021): 667–674. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 88. Mao R. Q., Lan L., Kay J., et al., “Immersive Virtual Reality for Surgical Training: A Systematic Review,” Journal of Surgical Research 268 (2021): 40–58. [DOI] [PubMed] [Google Scholar]
- 89. Badiali G., Ferrari V., Cutolo F., et al., “Augmented Reality as an Aid in Maxillofacial Surgery: Validation of a Wearable System Allowing Maxillary Repositioning,” Journal of Cranio‐Maxillofacial Surgery 42 (2014): 1970–1976. [DOI] [PubMed] [Google Scholar]
- 90. Suebnukarn S., Chaisombat M., Kongpunwijit T., and Rhienmora P., “Construct Validity and Expert Benchmarking of the Haptic Virtual Reality Dental Simulator,” Journal of Dental Education 78 (2014): 1442–1450. [PubMed] [Google Scholar]
- 91. Suebnukarn S., Phatthanasathiankul N., Sombatweroje S., Rhienmora P., and Haddawy P., “Process and Outcome Measures of Expert/Novice Performance on a Haptic Virtual Reality System,” Journal of Dentistry 37 (2009): 658–665. [DOI] [PubMed] [Google Scholar]
- 92. De Boer I. R., Wesselink P. R., and Vervoorn J. M., “Student Performance and Appreciation Using 3d vs. 2d Vision in a Virtual Learning Environment,” European Journal of Dental Education 20 (2016): 142–147. [DOI] [PubMed] [Google Scholar]
- 93. Farag A. and Hashem D., “Impact of the Haptic Virtual Reality Simulator on Dental students' Psychomotor Skills in Preclinical Operative Dentistry,” Clinics and Practice 12 (2021): 17–26. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 94. Pulijala Y., Ma M., Pears M., Peebles D., and Ayoub A., “Effectiveness of Immersive Virtual Reality in Surgical Training—A Randomized Control Trial,” Journal of Oral and Maxillofacial Surgery 76 (2018): 1065–1072. [DOI] [PubMed] [Google Scholar]
- 95. Germans D. M., Spoelder H. J. W., Renambot L., Bal H. E., Daatselaar S. V., and Stelt P. V. D., “Measuring in Virtual Reality: A Case Study in Dentistry,” IEEE Transactions on Instrumentation and Measurement 57 (2008): 1177–1184. [Google Scholar]
- 96. Fushima K. and Kobayashi M., “Mixed‐Reality Simulation for Orthognathic Surgery,” Maxillofacial Plastic and Reconstructive Surgery 38 (2016): 13. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 97. Bartella A. K., Kamal M., Kuhnt T., et al., “Mixed Reality in Oral and Maxillofacial Surgery: A Symbiosis of Virtual and Augmented Reality or a Pointless Technological Gadget,” International Journal of Computerized Dentistry 24 (2021): 65–76. [PubMed] [Google Scholar]
- 98. Hadjichristou C., Kokoti M., and Bakopoulou A., “Haptics in Fixed Prosthodontics and Their Role in Dental Education: A Literature Review,” Journal of Dental Education 88 (2024): 1020–1028, 10.1002/jdd.13533. [DOI] [PubMed] [Google Scholar]
- 99. Song S. J., Tang M., Gwartzman B., et al., “Augmented‐Reality‐Assisted Intraoral Scanning: A Proof‐Of‐Concept Study,” Journal of Prosthodontics 33 (2024): 550–557. [DOI] [PubMed] [Google Scholar]
- 100. Huang Y., Hu Y., Chan U., et al., “Student Perceptions Toward Virtual Reality Training in Dental Implant Education,” PeerJ 11 (2023): e14857. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 101. Rodrigues P., Nicolau F., Norte M., et al., “Preclinical Dental Students Self‐Assessment of an Improved Operative Dentistry Virtual Reality Simulator With Haptic Feedback,” Scientific Reports 13 (2023): 2823. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 102. Bochet Q., Raoul G., Lauwers L., and Nicot R., “Augmented Reality in Implantology: Virtual Surgical Checklist and Augmented Implant Placement,” Journal of Stomatology, Oral and Maxillofacial Surgery 125 (2024): 101813. [DOI] [PubMed] [Google Scholar]
- 103. Slaidina A., Ozolins K., Berzina S., and Abeltins A., “Patient‐Specific Virtual Simulation in the Clinical Training for Prosthetic Dentistry,” European Journal of Dental Education 20 (2023): 1–9, 10.1111/eje.12949. [DOI] [PubMed] [Google Scholar]
- 104. Iiyoshi K., Khazaaleh S., Dalaq A. S., Daqaq M. F., Korres G., and Eid M., “Origami‐Based Haptic Syringe for Local Anesthesia Simulator,” IEEE Transactions on Haptics 17 (2024): 39–44. [DOI] [PubMed] [Google Scholar]
- 105. Kim‐Berman H., Bui D., Lee K., et al., “Student Learning of Head and Neck Anatomy Using Cone Beam Computed Tomography and Immersive Virtual Reality,” Journal of Dental Education 87 (2023): 1180–1187. [DOI] [PubMed] [Google Scholar]
- 106. Philip N., Ali K., Duggal M., Daas H., and Nazzal H., “Effectiveness and Student Perceptions of Haptic Virtual Reality Simulation Training as an Instructional Tool in Pre‐Clinical Paediatric Dentistry: A Pilot Pedagogical Study,” International Journal of Environmental Research and Public Health 20 (2023): 4226. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 107. Carpegna G., Scotti N., Alovisi M., Comba A., Berutti E., and Pasqualini D., “Endodontic Microsurgery Virtual Reality Simulation and Digital Workflow Process in a Teaching Environment,” European Journal of Dental Education 35 (2023): 1–7, 10.1111/eje.12946. [DOI] [PubMed] [Google Scholar]
- 108. Yari A., Fasih P., Goodarzi A., Nouralishahi A., and Nikeghbal D., “The Effect of Augmented Reality Book on the Proficiency of Local Anesthesia Administration of the Inferior Alveolar Nerve,” Journal of Dental Education 88 (2024): 1000–1008, 10.1002/jdd.13522. [DOI] [PubMed] [Google Scholar]
- 109. Kanwal L., Gulzar M., Idrees W., Ikram F., Sukhia R. H., and Fida M., “The Application of Virtual Reality and Augmented Reality in Dentistry‐a Literature Review,” Journal of the Pakistan Medical Association 74 (2024): s126–s131. [DOI] [PubMed] [Google Scholar]
- 110. Wan T., Liu K., Li B., and Wang X., “Validity of an Immersive Virtual Reality Training System for Orthognathic Surgical Education,” Frontiers in Pediatrics 11 (2023): 1133456. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 111. Toker S., Akay C., Basmaci F., Kilicarslan M. A., Mumcu E., and Cagiltay N. E., “Expectancy From, and Acceptance of Augmented Reality in Dental Education Programs: A Structural Equation Model,” Journal of Dental Education 88 (2024): 1277–1286, 10.1002/jdd.13580. [DOI] [PubMed] [Google Scholar]
- 112. Alsufyani N., Alnamlah S., Mutaieb S., et al., “Virtual Reality Simulation of Panoramic Radiographic Anatomy for Dental Students,” Journal of Dental Education 87 (2023): 1200–1209. [DOI] [PubMed] [Google Scholar]
- 113. Koolivand H., Shooreshi M. M., Safari‐Faramani R., et al., “Comparison of the Effectiveness of Virtual Reality‐Based Education and Conventional Teaching Methods in Dental Education: A Systematic Review,” BMC Medical Education 24 (2024): 8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 114. Daud A., Matoug‐Elwerfelli M., Daas H., Zahra D., and Ali K., “Enhancing Learning Experiences in Pre‐Clinical Restorative Dentistry: The Impact of Virtual Reality Haptic Simulators,” BMC Medical Education 23 (2023): 948. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 115. Monaghesh E., Negahdari R., and Samad‐Soltani T., “Application of Virtual Reality in Dental Implants: A Systematic Review,” BMC Oral Health 23 (2023): 603. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 116. Lu J., Zhang L., and Ye L., “Construction and Application of Dental Virtual Reality Simulation Teaching System in China: Necessity and Strategies,” European Journal of Dental Education 20 (2023): 2526. [DOI] [PubMed] [Google Scholar]
- 117. Im J.‐E., Gu J.‐Y., Bae J.‐H., and Lee J.‐G., “Comparative Study of 360° Virtual Reality and Traditional Two‐Dimensional Video in Nonface‐To‐Face Dental Radiology Classes: Focusing on Learning Satisfaction and Self‐Efficacy,” BMC Medical Education 23 (2023): 855. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 118. Lamira J. M., Wilson C. S., Leppek N. C., Orr C. M., De La Rosa L. M., and Greany T. J., “A Pilot Study of Local Anesthesia Training Using a Mixed‐Reality Haptic Fidelity Model,” Journal of Dental Education 87 (2023): 583–591. [DOI] [PubMed] [Google Scholar]
- 119. Song Y. L. and Ng C. W. B., “A Mixed‐Reality Pedagogical Innovation for Miniscrew Implant Insertion,” Journal of Dental Education 20 (2023): 1–4, 10.1002/jdd.13407. [DOI] [PubMed] [Google Scholar]
- 120. Mahrous A., Elgreatly A., Qian F., and Gb S., “A Comparison of Pre‐Clinical Instructional Technologies: Natural Teeth, 3d Models, 3d Printing, and Augmented Reality,” Journal of Dental Education 85 (2021): 1795–1801. [DOI] [PubMed] [Google Scholar]
- 121. Mladenovic R., Dakovic D., Pereira L., Matvijenko V., and Mladenovic K., “Effect of Augmented Reality Simulation on Administration of Local Anaesthesia in Paediatric Patients,” European Journal of Dental Education 24 (2020): 507–512. [DOI] [PubMed] [Google Scholar]
- 122. Obispo C., Gragera T., Giovannini G., Zubizarreta‐Macho Á., and Aragoneses Lamas J. M., “Influence of Augmented Reality Appliances on Tooth Preparation Designs—An In Vitro Study,” Journal of Personalized Medicine 14 (2023): 37. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 123. Mc J., Alexandrescu L., Folguera F., and García I., “A Mobile Augmented Reality System for the Learning of Dental Morphology. Digital,” Education Review 30 (2016): 234–247. [Google Scholar]
- 124. Katić D., Spengler P., Bodenstedt S., et al., “A System for Context‐Aware Intraoperative Augmented Reality in Dental Implant Surgery,” International Journal of Computer Assisted Radiology and Surgery 10 (2015): 101–108. [DOI] [PubMed] [Google Scholar]
- 125. Faus‐Matoses V., Faus‐Llácer V., Moradian T., et al., “Accuracy of Endodontic Access Cavities Performed Using an Augmented Reality Appliance: An In Vitro Study,” International Journal of Environmental Research and Public Health 19 (2022): 11167. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 126. Mladenovic R., Matvijenko V., Subaric L., and Mladenovic K., “Augmented Reality as e‐Learning Tool for Intraoral Examination and Dental Charting During Covid‐19 Era,” Journal of Dental Education 86 (2022): 862–864. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 127. Zafar S. and Zachar J. J., “Evaluation of Holohuman Augmented Reality Application as a Novel Educational Tool in Dentistry,” European Journal of Dental Education 24 (2020): 259–265. [DOI] [PubMed] [Google Scholar]
- 128. Jiang W., Ma L., Zhang B., et al., “Evaluation of the 3d Augmented Reality–Guided Intraoperative Positioning of Dental Implants in Edentulous Mandibular Models,” International Journal of Oral & Maxillofacial Implants 33 (2018): 33–1228. [DOI] [PubMed] [Google Scholar]
- 129. Yao J., Zeng W., Zhou S., Cheng J., Huang C., and Tang W., “Augmented Reality Technology Could Be an Alternative Method to Treat Craniomaxillofacial Foreign Bodies: A Comparative Study Between Augmented Reality Technology and Navigation Technology,” Journal of Oral and Maxillofacial Surgery 78 (2020): 578–587. [DOI] [PubMed] [Google Scholar]
- 130. Mladenovic R., Alqahtani S., Mladenovic K., Bukumiric Z., and Zafar S., “Effectiveness of Technology‐Enhanced Teaching Methods of Undergraduate Dental Skills for Local Anaesthesia Administration During Covid‐19 Era: students' Perception,” BMC Oral Health 22 (2022): 40. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 131. Xia P., Lopes A. M., and Restivo M. T., “Virtual Reality and Haptics for Dental Surgery: A Personal Review,” Visual Computer 29 (2013): 433–447. [Google Scholar]
- 132. Ochandiano S., García‐Mato D., Gonzalez‐Alvarez A., et al., “Computer‐Assisted Dental Implant Placement Following Free Flap Reconstruction: Virtual Planning, CAD/CAM Templates, Dynamic Navigation and Augmented Reality,” Frontiers in Oncology 11 (2022): 5839. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 133. Llena C., Folguera S., Forner L., and Rodríguez‐Lozano F., “Implementation of Augmented Reality in Operative Dentistry Learning,” European Journal of Dental Education 22 (2018): e122–e130. [DOI] [PubMed] [Google Scholar]
- 134. Sharmin N., Chow A. K., Votta D., and Maeda N., “Implementing Augmented Reality to Facilitate the Learning of Oral Histology,” Healthcare Informatics Research 28 (2022): 170–175. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 135. Talaat S., Ghoneima A., Kaboudan A., Talaat W., Ragy N., and Bourauel C., “Three‐Dimensional Evaluation of the Holographic Projection in Digital Dental Model Superimposition Using Hololens Device,” Orthodontics & Craniofacial Research 22 (2019): 62–68. [DOI] [PubMed] [Google Scholar]
- 136. Pietruski P., Majak M., Światek‐Najwer E., et al., “Supporting Mandibular Resection With Intraoperative Navigation Utilizing Augmented Reality Technology – A Proof of Concept Study,” Journal of Cranio‐Maxillofacial Surgery 47 (2019): 854–859. [DOI] [PubMed] [Google Scholar]
- 137. Espejo‐Trung L. C., Elian S. N., and De Cerqueira Luz M. A. A., “Development and Application of a New Learning Object for Teaching Operative Dentistry Using Augmented Reality,” Journal of Dental Education 79 (2015): 1356–1362. [PubMed] [Google Scholar]
- 138. Legorburu B. G., Adanero Velasco A., Velasco J. R. M., and Pozo P. P. D., “A 3d Model of the Jaw Applied to Paediatric Dentistry,” Bioengineering 9 (2022): 143. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 139. Steinberg A. D., Bashook P. G., Drummond J., Ashrafi S., and Zefran M., “Assessment of Faculty Perception of Content Validity of Periosim©, a Haptic‐3d Virtual Reality Dental Training Simulator,” Journal of Dental Education 71 (2007): 1574–1582. [PubMed] [Google Scholar]
- 140. Al‐S L., Yeung C., Chu S., Wong Aw‐Y Y., and Oy C. C.‐H., “Use of Computer Simulation in Dental Training With Special Reference to Simodont,” Dentistry Journal 9 (2021): 125. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 141. Schendel S. A., “Computer Simulation in the Daily Practice of Orthognathic Surgery,” International Journal of Oral and Maxillofacial Surgery 44 (2015): 1451–1456. [DOI] [PubMed] [Google Scholar]
- 142. Al‐Saud L. M., Mushtaq F., Allsop M. J., et al., “Feedback and Motor Skill Acquisition Using a Haptic Dental Simulator,” European Journal of Dental Education 21 (2017): 240–247. [DOI] [PubMed] [Google Scholar]
- 143. Kusumoto N., Sohmura T., Yamada S., Wakabayashi K., Nakamura T., and Yatani H., “Application of Virtual Reality Force Feedback Haptic Device for Oral Implant Surgery,” Clinical Oral Implants Research 17 (2006): 708–713. [DOI] [PubMed] [Google Scholar]
- 144. Dutã M., Amariei C. I., Bogdan C. M., Popovici D. M., Ionescu N., and Nuca C. I., “An Overview of Virtual and Augmented Reality in Dental Education,” Oral Health and Dental Management 10 (2011): 42–49. [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Data Availability Statement
The data that support the findings of this study are available from the corresponding author upon reasonable request.