

Abstract
Objective
To assess the surgical results and clinicopathologic features of hepatic metastases from gastric adenocarcinoma to identify patients with a better probability of survival.
Summary Background Data
Many studies have reported the benefit of hepatic resection for metastatic tumors from colorectal cancer. However, indications for a surgical approach for gastric adenocarcinoma involving the liver have not been clearly defined.
Methods
Ninety (11%) of 807 patients with primary gastric cancer were diagnosed with synchronous (n = 78) or metachronous (n = 12) hepatic metastases. Of these, 19 underwent 20 resections intended to cure the metastatic lesion in the liver. The clinicopathologic features of the hepatic metastases in, and the surgical results for, the 19 patients were analyzed.
Results
The actuarial 1-year, 3-year, and 5-year survival rates after hepatic resection were, respectively, 77%, 34%, and 34%, and three patients survived for more than 5 years after surgery. Solitary and metachronous metastases were significant determinants for a favorable prognosis after hepatic resection. Pathologically, a fibrous pseudocapsule between the tumor and surrounding hepatic parenchyma was found in 13 of the 19 patients (68%). The presence of a peritumoral fibrous pseudocapsule and a well-differentiated histologic type of metastatic nodule were significant prognostic factors. Factors associated with the primary lesion were not significant prognostic determinants in patients who underwent curative resection of the primary cancer.
Conclusions
Solitary and metachronous metastases from gastric cancer should be treated by a surgical approach and confer a better prognosis. A new prognostic factor, the presence of a pseudocapsule, may be helpful in defining indications for postoperative adjuvant treatment.
Hepatic metastasis from gastrointestinal carcinoma is a frequent and crucial problem. Many studies have reported the benefit of hepatic resection for metastatic tumors from colorectal cancer, 1–3 and as the procedure has become safer, the indications for its use in this situation have been expanded. However, in the case of the equally common liver metastases from gastric carcinoma, only a few patients are candidates for hepatic resection because these are often multiple, scattered, bilobar metastases, and recurrence usually occurs with a combination of various patterns, such as peritoneal dissemination, lymph node metastases, and distant metastases. Only a few reports have dealt with the results of surgical resection of hepatic metastases from gastric cancer; the results have been disappointing. 4,5 The aims of this study were to identify prognostic determinants for hepatic metastases from gastric cancer and to evaluate the actual targets of surgical therapy.
METHODS
Patients
Between 1986 and 1999, 807 patients with gastric carcinoma underwent surgery in the First Department of Surgery, Kagawa Medical University, Japan. Of these, 78 (9.6%) were found to have synchronous hepatic metastases and 12 (1.5%) metachronous hepatic metastases. Of these 90 patients, 19 who underwent initial hepatic resection were selected for this study; these consisted of 13 men and 6 women with a mean age of 69 years (range 52–79). Hepatic resection was indicated for patients with synchronous metastases who did not have peritoneal dissemination or any other distant metastases, and patients with metachronous metastases who did not have any other recurrent lesions. All patients had complete resection of their primary gastric cancer. Synchronous en bloc resections of gastric cancer directly invading the liver were not included in this study. Overall resectability was therefore 21.2% (19/90) for all 90 patients, 16.6% (13/78) for synchronous metastases, and 50% (6/12) for metachronous lesions. No patient died during the initial hospital stay or within 1 month after surgery. Follow-up ranged from 13 to 148 months (median 36).
Methods
The following preoperative demographic and clinical information was obtained from the patient records: age, gender, interval between gastrectomy and hepatectomy, surgical procedure, postoperative chemotherapy, and mode of recurrence.
Macroscopically, the number, size, lobar distribution, and surgical margin of the tumors were recorded. The microscopic features evaluated were histologic differentiation and the presence of vascular invasion, of a fibrous pseudocapsule between the tumor and the liver parenchyma, 6 and of peritumoral lymphocytes surrounding the hepatic metastases. 7 In patients with multiple hepatic metastases, the pathologic findings of the largest tumor were taken as representative of those of the other tumors, because all the tumors showed similar pathologic features. The histologic type of the metastatic tumors was determined according to the World Health Organization classification. 8 The presence of a fibrous pseudocapsule between the tumor and the hepatic parenchyma was evaluated as described in our previous report. 6 The density of tumor-infiltrating lymphocytes between the tumor and the hepatic parenchyma was graded as weak or dense (weak < 50 per high-power field < dense). 7
Depth of invasion, extent of lymph node metastases, and lymphatic and venous invasion of the primary gastric cancer were also evaluated. The pathologic diagnosis and classification of the primary cancer were performed by a minimum of two pathologists according to the TNM classification of the UICC 9 and General Rules for Gastric Cancer Study in Surgery and Pathology in Japan. 10
Data Analysis
The clinicopathologic factors analyzed for prognostic significance using a Kaplan-Meier product-limit method with a log-rank test 11 were age; gender; interval between gastrectomy and hepatectomy; surgical procedure; postoperative chemotherapy; mode of recurrence; number, size, lobar distribution, and surgical margin of the metastatic nodules; presence of vascular invasion, of a fibrous pseudocapsule between the tumor and the liver parenchyma, or of peritumoral lymphocytes surrounding the hepatic metastases; and depth of invasion, extent of lymph node metastases, and lymphatic and venous invasion of the primary gastric cancer. Significance was defined as P < .05. The surgical procedure was classified as anatomic resection (segmentectomy and lobectomy) or limited resection (all resections less extensive than segmentectomy). Statistical analysis was performed with a statistical analysis program package (SPSS 9.0, SPSS Inc. Chicago, IL).
RESULTS
Clinicopathologic Data
Synchronous hepatic resection and gastrectomy was performed on 13 patients; the median interval between gastric and hepatic resection in the remaining 6 patients with metachronous metastases was 20 months (range 7–26). The median size of the metastatic tumor was 39 mm (range 3–100). The distribution of surgical procedures for hepatectomy was anatomic resection in 7 patients (37%), limited resection in 7 (37%), and combined procedures in 5 (26%). Adjuvant systemic chemotherapy was administered to six patients, intraarterial chemotherapy to three, and intraportal chemotherapy to two; eight patients did not receive chemotherapy. A pathologic study revealed that all tumors were adenocarcinomas. Two patients had gastric cancer arising from the remnant stomach (one with synchronous metastases). All except one had advanced gastric cancer with invasion deeper than the muscularis propria. Sixteen of the 19 patients had gastric cancer with lymph node involvement. There was no evidence of paraaortic lymph node metastases and peritoneal dissemination, so curative resection of the gastric carcinoma was performed in all cases. With regard to pathologic features in the peritumoral section of the metastatic lesion, fibrous tissue between the tumor and hepatic parenchyma was seen in 13 patients (68%) (Fig. 1). Lymphocytic infiltration between the tumor and hepatic parenchyma was graded as weak in 11 patients (58%) and dense in 8 (42%).
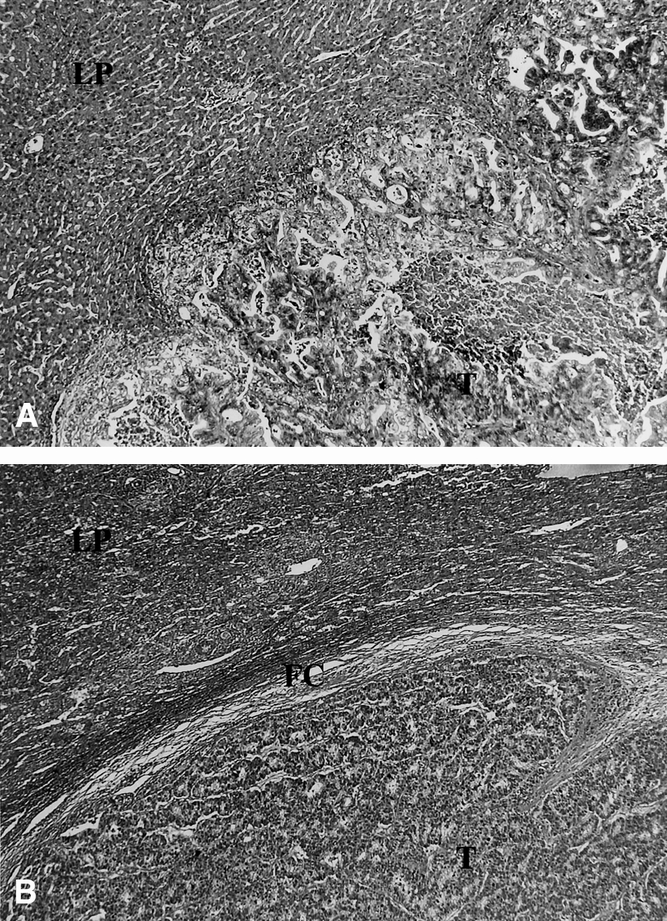
Figure 1. Fibrous capsule (fc) between the tumor (T) and surrounding hepatic parenchyma (LP). (A) Tumor cells directly infiltrate the hepatic sinusoid. (B) Thick collagen bundles have developed between the tumor and hepatic parenchyma. Hematoxylin and eosin, original magnification 100×.
Patient Outcome
The results of the analysis of prognostic factors are given in Table 1. The actuarial 1-year, 3-year, and 5-year survival rates after hepatic resection were, respectively, 77%, 34%, and 34%. Solitary (P = .044) and metachronous (P = .043) metastases were significant determinants for a favorable prognosis after hepatic resection. The surgical procedure and postoperative adjuvant chemotherapy were not significant prognostic factors. In terms of pathologic features, the presence of a peritumoral fibrous pseudocapsule (P = .015) and a well-differentiated histologic type of metastases (P = .02) were significant prognostic factors. The actuarial 1-year and 3-year survival rates were 87% and 51% for patients with a fibrous pseudocapsule and 57% and 0% for patients without a fibrous pseudocapsule. Factors associated with the primary lesion were not significant prognostic determinants. Cancer recurred in 14 (74%) of the 19 patients between 7 and 26 months after hepatic resection. The site of initial recurrence after hepatic resection was the liver in 12 patients, the lung in 3, and the lymph nodes in 2. Ten patients had died of cancer by the time this report was written. The details for three patients who survived more than 5 years after hepatic resection are summarized in Table 2.
Table 1. CLINICOPATHOLOGIC CHARACTERISTICS AND THEIR PROGNOSTIC SIGNIFICANCE

The significance of the difference was tested for equality of survival distributions for each parameter by the log-rank test.
* According to pTNM classification of UICC.
† According to the General Rules for Gastric Cancer Study in Surgery and Pathology in Japan.
Table 2. DETAILS OF PATIENTS WHO SURVIVED MORE THAN 5 YEARS AFTER HEPATIC RESECTION

fc, fibrous pseudocapsule around the tumor; ly, lymphatic invasion; well, well-differentiated adenocarcinoma; v, venous invasion.
* According to pTNM classification of UICC.
† According to the General Rules for Gastric Cancer Study in Surgery and Pathology in Japan.
Of the 71 patients with liver metastases who did not undergo hepatic resection, 24 had peritoneal dissemination, 15 had paraaortic lymph node metastases, and 27 had numerous scattered metastases in both lobes. Retrospectively, only 9 of the 71 were possible candidates for hepatic resection at their disease stage (P0, N0–2, and H1–2 according to the General Rules for Gastric Cancer Study in Surgery and Pathology in Japan). The actuarial 1-year and 3-year survival rates for these nine patients were 43% and 0%. Seven of the nine patients died of cancer during months 1 to 31 (median survival 6 months) after gastrectomy. The survival rate in the unresected group was significantly (P < .05) lower than in the resected group.
DISCUSSION
Hepatic resection, a potentially curative approach for patients with liver metastases from colorectal carcinoma, carries a 5-year survival rate of 30% to 50%. 12–20 The resection rate for hepatic metastases from colorectal carcinoma varies from 20% to 50%. 2,14 In contrast, for hepatic resection for metastases from gastric carcinoma, only 10% to 20% of patients with metastases are suitable for surgical treatment, and the procedure has a median survival of 5 to 8 months, with 15% to 50% survival at 1 year and 19% survival at 5 years. 4,5,21–23 Thus, the clinical benefit of resection of hepatic metastases from gastric carcinoma is still not widely accepted. However, nonsurgical treatments, including systemic or hepatic artery infusion chemotherapy, do not achieve satisfactory results. In patients treated by gastrectomy and chemotherapy, median survival times are reported to range from 2.9 to 11.8 months;21,22,24 however, in the present study, 3 patients survived more than 5 years after hepatic resection, and the median overall and disease-free survivals for all 19 patients were, respectively, 21 and 8.2 months. These results for a surgical approach for liver metastases from gastric cancer are better than those previously reported and may be due to proper patient selection and the use of a controlled procedure.
Many prognostic determinants have been reported for metastatic colorectal cancer after hepatic resection. 12–20 In the present series of gastric metastases, although the total number of patients was small, several parameters were found to be significant predictors of outcome. Solitary and metachronous metastases were significant determinants for a favorable prognosis after hepatic resection. In colorectal liver metastases, the number of metastases is no longer considered to be an important predictor of long-term survival; if complete excision can be achieved, survival after resection of up to eight metastases is similar to that after resection of a solitary metastasis. 2 The different results between colorectal and gastric metastases are thought to reflect the aggressive biologic behavior of gastric cancer. Indications for resection of hepatic metastases should be based on the biologic character of the primary tumor.
Ochiai et al 4 indicated that hepatic resection should be attempted in the absence of serosal involvement by the primary gastric tumor or if the primary cancer has no venous or lymphatic invasion in the case of metachronous metastases. However, Miyazaki et al 5 reported that there was no significant difference in terms of invasion of depth or lymph node metastases of the gastric cancer between surviving patients and those who died after hepatectomy; they concluded that hepatic resection improved the prognosis in patients with solitary metastases if adequate tumor-free margins (>10 mm) could be obtained. Our study failed to find any significant association between survival and factors related to the primary gastric cancer in patients who underwent curative resection of their primary cancer. In addition, the surgical procedure and the surgical margin for the metastatic lesion were not significant prognostic factors in our series. A positive resection margin is also not an independent prognostic factor in colorectal liver metastases because of its strong relationship with the number of tumors resected. 14 In approximately 70% of patients, recurrent disease developed after hepatic resection, most commonly in the liver. Recurrent tumors were more frequently distributed in both lobes than in the resected lobe, suggesting that liver recurrence is more probably derived from multiple metastatic foci from the primary disease than from intrahepatic remetastases of the liver lesion. In addition, recurrence after hepatic resection is more strongly associated with systemic spread through vessel infiltration than with local spread through lymphatic or serosal invasion of the primary tumor. A generous surgical margin may not be essential for curative hepatic resection of liver metastases, although positive surgical margins should be avoided. In recent years, postoperative adjuvant chemotherapy for liver metastases has advanced, with some studies showing that arterial chemotherapy significantly prevents hepatic recurrence. 25–28 To improve the results of surgical management for this disease, newer adjuvant treatments for systemic spread are thought to be required.
A key question was whether synchronous resection of liver metastases provided any long-term survival benefit. In our study, synchronous resection resulted in one long-term survivor who had solitary metastasis, and five patients survived with recurrent disease for about 2 years (18, 20, 21, 24, and 28 months). In comparison with other treatments, 22 it appears that gastrectomy combined with hepatectomy has a beneficial effect on short-term prognosis. However, we cannot as yet say whether synchronous hepatic resection in this setting can result in long-term cure.
In a previous study, we showed that the presence of a fibrous pseudocapsule between colorectal metastases and the hepatic parenchyma was a promising indicator of a better prognosis after resection for this disease. 6 In the current study, we showed that the presence of a fibrous pseudocapsule around liver metastases from gastric cancer was also closely associated with patient survival. In addition, four nodules in three patients, who survived more than 5 years after hepatic resection, had a thick fibrous pseudocapsule with more than 10 layers of collagen bundles between the tumor and hepatic parenchyma. Pseudocapsule formation is considered to be a consequence of a protective immunoinflammatory reaction by the noncancerous liver against the metastatic nodule. The presence of a fibrous pseudocapsule may be valuable as a prognostic factor reflecting the host defense reaction in patients with liver metastases. The longer disease-free interval after gastrectomy for primary disease and the well-differentiated nature of metastatic nodules in long-term survivors suggest that the tumor has an indolent biologic character. These features may be useful in designing an adjuvant treatment and follow-up schedule for patients after surgical resection. Variations in the biologic behavior of the metastatic nodule and the host reaction, rather than the surgical procedure or adjuvant chemotherapy, may affect the prognosis.
This study emphasizes that solitary or metachronous metastases from gastric cancer should be treated by surgical resection and that they confer a better prognosis. A surgical approach for multiple or synchronous metastases may be of value as part of combination therapy in carefully selected patients. As a new potential prognostic factor, the presence of a pseudocapsule may be helpful in defining indications for postoperative adjuvant treatment and the follow-up schedule for patients after surgical resection.
Footnotes
Correspondence: Keiichi Okano, MD, First Department of Surgery, Kagawa Medical University, 1750-1, Ikenobe, Miki-cho, Kida-gun, Kagawa 761-0793, Japan.
E-mail: kokano@kms.ac.jp
Accepted for publication May 3, 2001.
References
- 1.Scheele J, Stang R, Altendorf-Hoffmann A. Hepatic metastases from colorectal carcinoma: impact of surgical resection on the natural history. Br J Surg 1990; 77: 1241–1249. [DOI] [PubMed] [Google Scholar]
- 2.Scheele J, Stang R, Altendorf-Hoffmann A, et al. Resection of colorectal metastases. World J Surg 1995; 19: 59–71. [DOI] [PubMed] [Google Scholar]
- 3.Minagawa M, Makuuchi M, Torzilli G, et al. Extension of the frontiers of surgical indication in the treatment of liver metastases from colorectal cancer. Ann Surg 2000; 231: 487–499. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Ochiai T, Sasako M, Mizuno S, et al. Hepatic resection for metastatic tumours from gastric cancer: analysis of prognostic factors. Br J Surg 1994; 81: 1175–1178. [DOI] [PubMed] [Google Scholar]
- 5.Miyazaki M, Itoh H, Nakagawa K, et al. Hepatic resection of liver metastases from gastric carcinoma. Am J Gastroenterol 1997; 92: 490–493. [PubMed] [Google Scholar]
- 6.Okano K, Yamamoto J, Kosuge T, et al. Fibrous pseudocapsule of metastatic liver tumors from colorectal carcinoma. Cancer 2000; 89: 267–275. [PubMed] [Google Scholar]
- 7.Ropponen KM, Eskelinen MJ, Lipponen PK, et al. Prognostic value of tumour-infiltrating lymphocytes (TILs) in colorectal cancer. J Pathol 1997; 182: 318–324. [DOI] [PubMed] [Google Scholar]
- 8.Jass JR, Sobin LH. Histological typing of intestinal tumors. Berlin, Heidelberg, Germany: Springer-Verlag; 1989.
- 9.UICC (International Union Against Cancer). TNM classification of malignant tumours. Fifth fully revised ed. Berlin: Springer-Verlag; 1997.
- 10.Japanese Research Society for Gastric Cancer. General rules for gastric cancer studies in surgery and pathology. 13th fully revised ed. Tokyo: Kanehara-Shuppan; 1999.
- 11.Kaplan EL, Meier P. Nonparametric estimation from incomplete observations. J Am Stat Assoc 1958; 53: 457–481. [Google Scholar]
- 12.Fong Y, Fortner J, Sun RL, et al. Clinical score for predicting recurrence after hepatic resection for metastatic colorectal cancer. Ann Surg 1999; 230: 309–321. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Ambiru S, Miyazaki M, Isono T, et al. Hepatic resection for colorectal metastases: analysis of prognostic factors. Dis Colon Rectum 1999; 42: 632–639. [DOI] [PubMed] [Google Scholar]
- 14.Yamamoto J, Shimada K, Kosuge T, et al. Factors influencing survival of patients undergoing hepatectomy for colorectal metastases. Br J Surg 1999; 86: 332–337. [DOI] [PubMed] [Google Scholar]
- 15.Registry of Hepatic Metastases. Resection of the liver for colorectal carcinoma metastases: a multi-institutional study of indications for resection. Surgery 1988; 103: 278–288. [PMC free article] [PubMed] [Google Scholar]
- 16.Nakamura S, Suzuki S, Baba S. Resection of liver metastases of colorectal carcinoma. World J Surg 1997; 21: 741–747. [DOI] [PubMed] [Google Scholar]
- 17.Cady B, Stone MD, McDermott WV Jr. Technical and biological factors in disease-free survival after hepatic resection for colorectal cancer metastases. Arch Surg 1992; 127: 561–568. [DOI] [PubMed] [Google Scholar]
- 18.Yamamoto J, Sugihara K, Kosuge T, et al. Pathologic support for limited hepatectomy in the treatment of liver metastasis from colorectal cancer. Ann Surg 1995; 221: 74–78. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Yasui K, Hirai T, Kato T, et al. A new macroscopic classification predicts prognosis for patient with liver metastases from colorectal cancer. Ann Surg 1997; 226: 582–586. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Okano K, Yamamoto J, Moriya Y, et al. Macroscopic intrabiliary growth of liver metastases from colorectal cancer. Surgery. 1999; 126: 829–834. [PubMed] [Google Scholar]
- 21.Maehara Y, Moriguchi S, Kakeji Y, et al. Pertinent risk factors and gastric carcinoma with synchronous peritoneal dissemination or liver metastases. Surgery 1991; 110: 820–823. [PubMed] [Google Scholar]
- 22.Okuyama K, Isono K, Juan I, et al. Evaluation of treatment for gastric cancer with liver metastasis. Cancer 1985; 2498–2505. [DOI] [PubMed] [Google Scholar]
- 23.Bines SD, England G, Deziel DJ, et al. Synchronous, metachronous, and multiple hepatic resections of liver tumors originating from primary gastric tumors. Surgery 1993; 114: 799–805. [PubMed] [Google Scholar]
- 24.Yonehara Y, Matui N, Sakuma H. Effect of intra-hepatoarterial infusion of MMC and CDDP in gastric cancer patients with liver metastases. Surg Today 1992; 22: 253–259. [DOI] [PubMed] [Google Scholar]
- 25.Tsuji Y, Nishimura A, Katsuki Y, et al. Preventative chemotherapy for residual liver after resection of hepatic metastases from colorectal cancer. Gan To Kagaku Ryoho 1995; 22: 1493–1496. [PubMed] [Google Scholar]
- 26.Lygidakis NJ, Ziras N, Parissis J. Resection versus resection combined with adjuvant pre- and post-operative chemotherapy-immunotherapy for metastatic colorectal liver cancer. Hepato-Gastroenterology 1995; 42: 155–161. [PubMed] [Google Scholar]
- 27.Boku N, Ohtsu A, Shimada Y, et al. Phase II study of a combination of irinotecan and cisplatin against metastatic gastric cancer. J Clin Oncol 1999; 17: 319–323. [DOI] [PubMed] [Google Scholar]
- 28.Iwahashi M, Tanimura H, Nakamori M, et al. Clinical evaluation of hepatic arterial infusion of low dose-CDDP and 5-FU with hyperthermotherapy: a preliminary study for liver metastases from esophageal and gastric cancer. Hepato-Gastroenterology. 1999; 46: 2504–2510. [PubMed] [Google Scholar]