

Abstract
Objective:
To assess long-term outcome and prognostic factors for extreme surgery by vascular and plastic surgical teamwork for leg salvage in patients with critically ischemic large tissue defects.
Summary Background Data:
Combined vascular reconstruction and microvascular free-flap transfer has been used to improve distal perfusion and cover large tissue defects caused by the critical limb ischemia (CLI) in few dedicated centers during the past 15 years. Comorbidities compromise the results of these demanding operations, and it is unclear how far this mode of treatment should be extended.
Methods:
During 1989 to 2003, altogether 2157 vascular or endovascular revascularizations for CLI manifested as tissue lesions were performed. These included 81 revascularizations combined with microvascular free flap transfers in 79 patients (37–85 years). All the patients were candidates for major amputation. The patients were followed up at least 2 years or to death (mean follow-up, 62 months; SD, ±34 months).
Results:
One- and 5-year leg salvage rates were 73% and 66%, survival rates 91% and 63%, and amputation-free survival rates of 70% and 41%, respectively. Male gender and American Society of Anesthesiologists score 4 were associated with an increased risk of death, whereas the involvement of the heel mostly with calcaneal osteomyelitis and a large size of defect predicted major amputation.
Conclusions:
A combined vascular reconstruction and free-flap transfer offers an option for advanced limb salvage in a selected group of patients with CLI and a major tissue defect. Poor general condition, the involvement of the heel, and a large defect would indicate an amputation over extreme attempts for limb salvage.
Vascular and microvascular free-flap reconstructions were combined to salvage 81 critically ischemic legs with large tissue defects. Amputation-free survival was 70% at 1 year and 41% at 5 years. Poor general condition and male gender were associated with death, whereas large lesion size and location in the heel predicted poor leg salvage.
Aggressive treatment of ischemia of the lower extremities has decreased the number of amputations in both diabetic and nondiabetic patients.1,2 Despite vascular reconstruction, the extremity is threatened by a major amputation when bone, tendon, vascular graft, or artificial material is exposed. Some recent studies report closure of small lesions in the foot and lower leg with local muscle flap, foot-level free style amputation, or vacuum-assisted closure.3–5 However, these methods tend to have a poor outcome in patients with vascular disease, especially in the foot and ankle or when the lesion is excessive or vascular graft is largely exposed.6,7
To our knowledge, the idea of combining vascular reconstruction and microvascular free flap coverage of ischemic lesion of the lower leg was first published by Briggs et al in 1985.8 Since then, the technique has been used to cover the large tissue defects caused by the critical leg ischemia (CLI) in few centers during the past 15 years with encouraging early results.9–11
Patients with CLI often suffer from comorbidities, which compromise the results of these demanding operations. It is unclear how far this extreme treatment should be extended.
None of the previous studies has been large enough to allow proper assessment of risk factors for outcome. We report the largest long-term outcome study with an attempt to identify limits of the procedure.
METHODS
Patients
During a 15-year period (1989–2003), a total of 2157 vascular or endovascular operations were performed for CLI manifested as tissue lesions (Fig. 1). These included 81 (3.9%) microvascular free flap operations combined with vascular reconstruction in 79 patients (65% males; age, 37–85 years). The procedure was done as last attempt to save the leg as all limbs were estimated to need major amputation below the knee or higher had revascularization and free flap transfer not been performed.
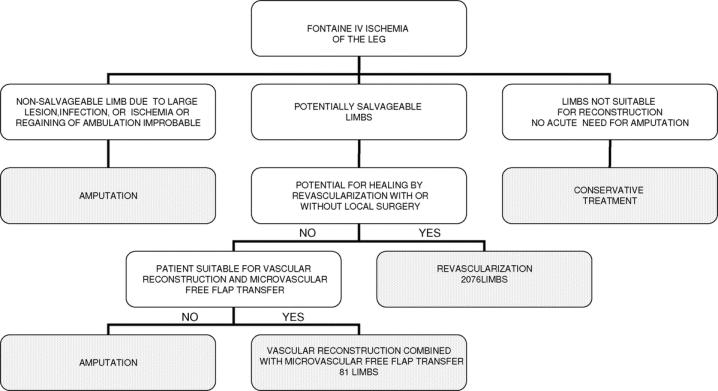
FIGURE 1. A decision tree for the treatment of critical ischemia and tissue loss of the leg in Helsinki University Central Hospital 1989–2003.
All patients had been ambulant before the manifestation of CLI and development of the tissue lesions. Nineteen patients had already had contralateral major lower limb amputation. Their mobility and independence were threatened by the loss of the other leg. In 2 patients, atherothrombotic disease proceeded later in the contralateral leg, necessitating also a combined reconstruction. These second combined operations were performed 12 and 13 months after first operation.
The patients typically had many risk factors, the most frequent being diabetes in 59 patients, renal insufficiency in 22, and coronary heart disease in 28 patients (Table 1).
TABLE 1. Preoperative Characteristics of 79 Patients

Tissue Lesions
Tissue lesions included 60 chronic ischemic defects with exposed bone or tendon classified as Fontaine IV12 or 2–3 D according to the University of Texas Wound Classification System.13 The rest were 14 vascular graft infections, wound healing problems related to 2 open fractures, 2 deep infections after a vascular reconstruction, 1 exposed arthroplasty, 1 reactivated osteomyelitis, and 1 large ischemic muscle necrosis after fasciotomy and vascular reconstruction. Thirty (37%) of the lesions were in the forefoot and 18 (22%) affected the heel area with osteomyelitis in 14 calcanei (Table 2). In 4 heels, reliable information on the presence or absence of osteomyelitis was not available. Of all the lesions, 41 (51%) had a plantar involvement.
TABLE 2. Location of Tissue Defects

Intervention
Teamwork
Preoperative evaluation and patient selection were always done as teamwork by vascular and plastic surgeon together. Selective antegrade lower extremity angiography was performed to evaluate the extent of arterial disease. Fulminant infection or septic foot necessitated debridement or minor amputation before the combined procedure could be undertaken. Simultaneous two-team approach was preferred in the operation whenever considered feasible. Plastic and vascular surgeon performed adequate debridement and final assessment of the foot viability together. Thereafter, the operation continued on 2 separate clean fields: the vascular surgeon harvested the vein and performed the bypass while the plastic surgeon raised the flap and performed the microvascular free flap transfer.
Vascular Reconstructions
Bypass grafts were connected to infrapopliteal arteries in 73 legs, 67 of the grafts were autologous veins, 1 PTFE prostheses, and 4 composite grafts with proximal PTFE prostheses. In 1 patient, the short occluded segment of anterior tibial artery was repaired with thoracodorsal artery also feeding serratus anterior muscle flap.
Two vein bypasses were connected to proximal popliteal artery and one femoral endarterectomy was made. Endovascular inflow procedure was done in 5 patients. Vascular reconstruction was anastomosed to plantar or pedal vessels in 39 cases (Fig. 2), in other infrapopliteal arteries in 21 cases, and end-to-end to the flap artery in 13 cases when no proper recipient artery for the bypass was available in the limb.

FIGURE 2. A, Ulceration of the MT amputation stump. B, DSA showing poor run off distal to popliteal artery: sequential vein bypass was made from common femoral artery to anterior tibial artery and further to dorsalis pedis artery. C, The middle anastomosis under construction. D, Fasciocutaneous radial forearm flap contouring the stump, pedicle area covered with split thickness skin graft to avoid tension.
The patients were given 100 IU heparin per kg at least 2 minutes before clamping a vessel. Postoperative anticoagulation with dalteparin sodium or enoxaparin sodium was given twice daily until the patients were mobilized. The patients had ASA 100 mg as a routine treatment before and after the operation.
Free Flaps
The most common free flaps used were latissimus dorsi (45), rectus abdominis (19), and forearm fasciocutaneous flap (10). Omentum, gracilis, and tensor fasciae latae muscles were used as flaps twice each and serratus muscle with a long segment of thoracodorsal artery once. Flap arteries were anastomosed end-to-side to the bypass graft in 60 limbs, end-to-end to the graft in 13 limbs with no proper recipient artery for bypass, and end-to-side to native artery distal to the vascular graft in 8 limbs. Muscular flaps were fixed under the undermined skin edges and covered with split-thickness skin grafting (Fig. 3).

FIGURE 3. A, Large forefoot defect after III and IV ray amputation in a 44-year-old uremic patient. B, Plantar view after amputation of the second toe. C, Latissimus dorsi free flap transfer after femorotibial bypass. D, Outcome at 2 months.
Follow-up
The follow-up lasted until the December 31, 2005 or to death. The mean follow up was 62 months (SD ± 34 months). Primary endpoints of the study were amputation-free survival, patient survival, and leg salvage. Secondary endpoints were time required for ulcer healing and the mobility after the operation. The ambulation at least with the assistance of cane, crutches, or walker was considered successful. As the outcome in terms of healing of the tissue defect and mobility is not a stable endpoint due to recurrences, a cross-sectional analysis of all patients was performed at the time when data were available from all patients.
Data Collection and Ethical Considerations
The data were collected from the patient records of our clinic and of other necessary healthcare providers. All the patients alive were able to give informed consent except 2, whose follow-up data were collected by a permission of Ministry of Social Affairs and Health. The study was approved by the Ethics Committee of Helsinki University Central Hospital.
Statistics
Kaplan-Meier analysis was used for survival data and log-rank test for comparison of 2 groups. Cox regression analysis was used for identification of factors influencing survival and major amputations and Pearson's χ2 test to compare the binominal data between 2 time periods. A subset of patients with chronic wounds was analyzed separately. The data were analyzed with SPSS 11.0 for Windows.
RESULTS
In 48 of the cases, both vascular and microvascular reconstructions were done in the same session, whereas the rest was performed staged mostly within 2 months after revascularization. Mean operation time was in simultaneous operations 384 minutes (SD ± 88 minutes), in separate vascular reconstructions 209 minutes (SD ± 63 minutes), and in separate free flap operations 289 minutes (SD ± 52 min). Mean stay at the intensive care unit was 2.6 days (SD ± 3.2 days). The mean stay in the surgical wards was 26 days (SD ± 16 days) and thereafter the patients were treated in basic or geriatric units for rehabilitation. The mean total hospital stay was 70 days (SD ± 60 days).
Operative Mortality
The perioperative 3-month mortality was 4.9%. Two of the 4 deaths were due to cardiac cause: 1 due to multiple organ failure and 1 due to sepsis-related to a large infected gluteal decubitus.
General Complications
General postoperative complications were encountered in 24 (30%) patients. Most frequent complications were cardiac insufficiency with pulmonary edema (7 patients), acute myocardial infarction (4 patients), reversible deterioration of renal function (3 patients), and sacral decubitus (3 patients).
Lower Extremity Complications
The healing was uneventful only in 22% of the legs. A total of 51 of 81 legs (63%) needed 1 to 4 reinterventions in the 30-day postoperative period. Six hematomas, 7 partial necroses, and 28 edge necroses of the flap as well as 14 wound infections were encountered postoperatively. Twenty three legs needed minor interventions as revisions, skin grafting, and minor amputations.
Altogether, 28 legs underwent major operations, including flap salvage operations, flap removals, and amputations (Table 3). Acute circulation problems of the flap necessitated a number of corrective procedures, including mostly reanastomosis of the flap vessels and evacuation of hematomas. Five out of 73 artery bypass grafts occluded within 3 months causing 3 amputations and one flap loss despite thrombectomy or regrafting.
TABLE 3. Lower Extremity Major Complications Related to Combined Vascular Reconstruction and Microvascular Free Flap Transfer for CLI Within the First 3 Months

During the first postoperative month, 8 major amputations were performed. Further 6 flaps were lost, but the defect could be debrided and covered with split-thickness skin grafting.
Within the first 3 postoperative months, altogether 15 amputations had to be performed; 7 of them were due to deep infection and persisting osteomyelitis of the foot or distal ischemia usually with functioning graft and viable flap (Table 3). After 3 months, further 13 major amputations were performed, 10 of them in 18 months (Table 4).
TABLE 4. The Reasons for Late Major Amputations After 3 Postoperative Months

To sum up the whole follow-up period, numerous reinterventions were necessary (mean, 2.4; SD ± 2.3; maximum, 12). The need for reinterventions was not associated with the use of any particular flap or type of revascularization.
Primary Endpoints
Long-term Outcome and Predicting Factors
One- and 5-year amputation-free survival rates were of 70% and 41% (Fig. 4), leg salvage rates of 73% and 66%, and survival rates of 91% and 63%, respectively. Male gender and ASA score 4 were independent predictors for death (Table 5). Patients with kidney transplantation had equal results compared with the other patients. In a subset of patients with chronic wounds the predicting factors in Cox regression analysis were similar.
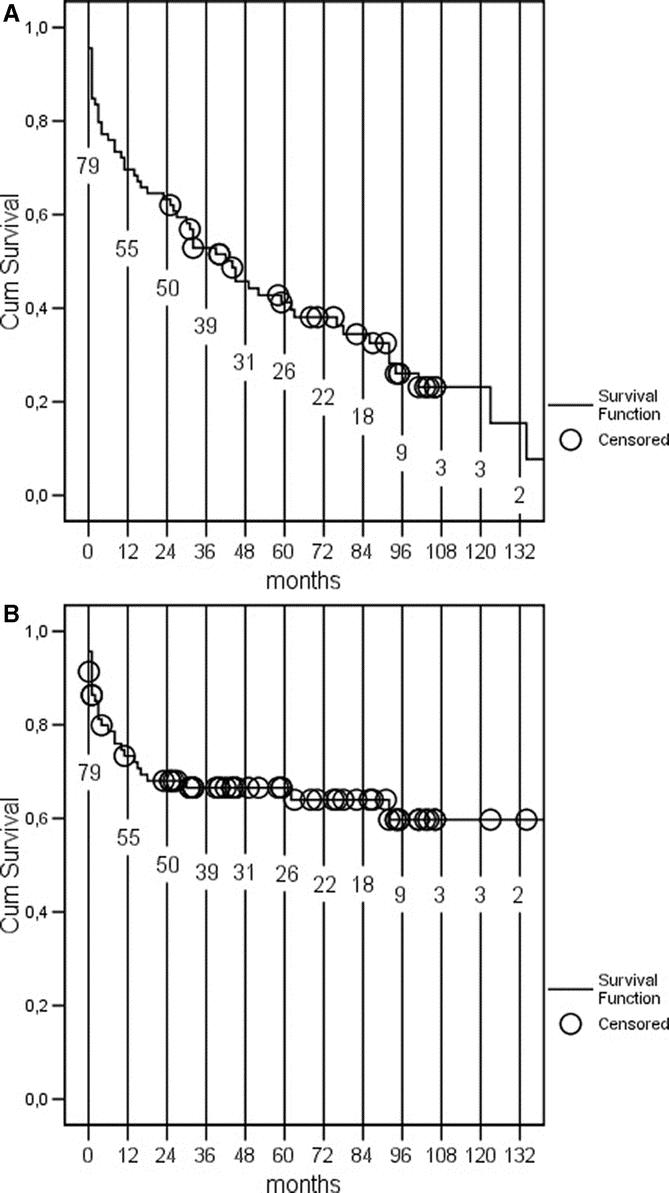
FIGURE 4. Amputation-free survival (A) and leg salvage (B) after combined vascular reconstruction and microvascular free flap transfer: Kaplan-Meier analysis. Numbers at risk are shown in the figure.
TABLE 5. Cox Regression Analysis: Variables Associated With Death and Amputation During the Follow-up

In the group of patients with ASA 4, 1- and 5-year amputation-free survival rates were of 45% and 30%, survival rates of 75% and 45%, and amputation rates of 61% and 61%, respectively. The survival was better in patients operated after the peak in operative activity in 1997 (Fig. 5). The survival of ASA 4 patients did not improve significantly between the 2 time periods, but their proportion was significantly smaller in the latter period (P = 0.005).

FIGURE 5. Yearly distribution of combined vascular reconstructions and microvascular free flap transfers in Helsinki University Central Hospital (1989–2003).
Secondary Endpoints
Location of the ulcer at the heel area and lesion diameter exceeding 10 cm were independently associated with increased risk of amputation (Table 5), whereas only the size was associated with leg salvage in patients with chronic wounds. Nevertheless, despite ulcers larger than 10 cm in diameter in the heel, 2 of 10 patients were alive with a leg at the end of follow-up at 146 and 64 months. Both had reulceration problem for years, but they had retained their legs and were ambulatory.
The lesions in the operated area healed in 46 patients (57% of all). The mean time for final healing in these patients was 9 months (SD ± 13 months). Mostly minor ulcer recurrence and new ulcer formation in the same region were encountered in 54% of the patients with primary skin healing.
All 75 surviving patients returned home. At 2 years, 41 patients were community and household ambulant with own leg (Fig. 6); 69 of 79 patients were alive and 21 of them were amputated. 7 patients needed wheelchair, but 5 of them were able to take few steps.

FIGURE 6. Cross-sectional analysis on the level of ambulation at 2 years after combined vascular reconstruction and free tissue transfer.
DISCUSSION
The early results of combining vascular reconstruction and free flap transfer for advanced leg salvage in patients with critically ischemic legs with large tissue defects were encouraging. The reports were, however, mostly anecdotal, and many of them repeated small series from same institutions. There are only 4 larger case series, giving an idea of midterm outcome.9–11,14 These studies included only 30, 45, 65, and 27 combined arterial revascularization and free flap transfers and were likely to be biased by small material, patient selection, and inadequate follow-up. The present study is largest so far and allows also some analysis of long-term outcome. Unfortunately, reliable long-term patency data could not be achieved as systematic Duplex surveillance was not available at all times, especially for patients living within a long distance. However, amputation-free survival should be considered the most important outcome measure for patients with advanced leg salvage.15 It illustrates which proportion of the patients can benefit from the operation. This is essential in patients with CLI who have high morbidity and mortality.16,17
Comparison of the Gent Study10 and the Rochester study11 to the results of our study is not easy, although all these studies had a multimorbid patient population. Our early results were in agreement with the Rochester study.11 The Belgians had a pure diabetic population, whereas the present study and the Rochester group11 had one fourth nondiabetic patients. The Rochester Group included also patients without need for vascular reconstruction. In their study, the combination of diabetes and renal insufficiency was identified as a strong predictor of limb loss and increased mortality.11 Previous studies have shown that end-stage renal disease, especially in combination with coronary disease, predicts very poor outcome.18,19 Patients in the present study had mostly moderate nephropathy or restored renal function after kidney transplantation. In the present study, specific effects of separate risk factors might have been masked by the poor general condition as illustrated by ASA score. Indeed, inclusion of a high proportion of multimorbid patients worsened the present results.
The defect size was an apparent predictor for poor outcome. The outcome of heel ulcers could be explained by a combination of factors. Factors on the background of heel ulcers, such as immobility, bed rest, and poor general condition are challenges for ulcer healing and rehabilitation. Neuropathy predisposes to ulcer recurrence. The calcaneal osteomyelitis was complicating most of the heel defects in the present series. It is difficult to treat and may need major resection of bone compromising the function of the heel. Indeed, at times major amputation was mandatory despite open graft and viable flap. Moreover, according to clinical experience, flaps in the heel are susceptible to shear stress.
Latissimus dorsi flap has traditionally been the most frequently used flap in our practice. The large muscle mass offers well-vascularized tissue to the ischemic area. Moreover, the flow in latissimus dorsi muscle is around 40 to 60 mL/min, providing a good outflow bed for vascular bypass grafts in case of insufficient native arterial outflow bed or when the bypass is anastomosed directly to the flap.20 Furthermore, donation site seldom has serious postoperative problems, the flap can be harvested simultaneously with vascular reconstruction, the pedicle is long, and thoracodorsal artery is not severely affected by the vascular disease.
As weight bearing is allowed gradually and late in these multimorbid patients, the hospital stays tend to get long. Persisting ulceration is another problem needing more evaluation in future. It may be explained by severe neuropathy. However, despite the high frequency of reulceration, most of the patients whose leg was salvaged achieved a good level of ambulation with their limb. These results are superior compared with those achieved by major amputations for vascular disease with only 22% to 42% of the patients achieving community or household ambulation.21–24 Yet, with optimal patient selection, the results could have been better as the present study highlighted the learning curve in patient selection. The more experience was gained during the years, the tighter inclusion criteria were used. The recommendation is not to include patients within ASA 4 score or with large tissue defects, especially if in heel and accompanied by osteomyelitis.
Teamwork between vascular and plastic surgeons is essential in this delicate surgery in preoperative, perioperative, and postoperative care, not to forget experts from other disciplines as well. As a consequence, centralizing this kind of surgery is necessary to gain the adequate experience and long-term outcome.
CONCLUSION
Combined vascular reconstruction and free-flap transfer offers an option for advanced limb salvage in a selected group of patients with CLI and a major tissue defect. Poor general condition, heel involvement especially with osteomyelitis, and a large defect support amputation over extreme attempts for limb salvage.
Discussions
Dr. Matthias Rothmund: I was asked by the Programme Committee to comment on this paper. I must confess I am not an expert in either of the fields of vascular or plastic surgery, so I get along rather well with this because I think there is no expert in the room except the 2 authors who presented this fantastic paper.
Reading the literature on this, I have found out that this is the largest study on this extreme limb salvage in a difficult subset of patients with this disease. It is really the tip of the iceberg of patients with advanced ischemic leg disease, which they have treated. They used the team approach as they did during their presentation, and this is obviously a very demanding task and you can take this from many aspects. One was most impressive for me: two thirds of the patients required 1 to 4 reoperations in the weeks and months after initial surgery.
I have 3 questions. You said that you usually did the distal anastomosis to the patient's own pedal artery. But in some you did anastomosis directly to the flap. Did this make a difference in results? Was the anastomosis to the flap more risky than to the patient's own artery? This would be my first question.
The second question is: you said you did some of the patients as a one-stage procedure and the others as a 2-stage procedure. What were your criteria to go ahead with a 1-stage compared with a two-stage procedure?
And the third question is that you used several different kinds of flaps: latissimus dorsi, rectus abdominis, forearm flap. How did you select the flaps? Which flap for what situation? And how did you make sure that the blood supply within the flap was good before you took out the flap at the donor site? These were my 3 questions.
Dr. Mauri Lepäntalo: Thank you very much for your questions. As a vascular surgeon, I can take the 2 first questions and Dr. Erkki Tukiainen, the plastic surgeon, will answer the third.
Every attempt was made to identify any suitable recipient artery for the bypass in the foot or in the calf, but in 13 cases no such artery could be identified. In these legs, the bypass was coupled directly with the free flap, most often the latissimus dorsi (LD) muscle. LD is a large muscle and can therefore serve rather as a good recipient vascular bed. Comparison of 13 such bypasses to the other 47 with chronic ischemic defects was problematic due to small sample size.
Dr. Matthias Rothmund: How many of these 13 flaps did survive?
Dr. Mauri Lepäntalo: At 2 years, when we had data on all patients, 8 of these 13 patients were alive with a viable flap and leg. There was no difference between the 2 small groups as to leg salvage or amputation-free survival.
Your other question was about whether to do a staged or a simultaneous procedure. We did staged only, if we were uncertain whether the leg would fare without a microvascular reconstruction or not. In these cases, we did the bypass, waited, and saw if the tissue lesion healed by wound excision and subsequent STSG. If not, we did the free flap transfer later. If we considered that, whatever the result of the bypass, the foot was going to be functionally poor, we did the procedures simultaneously. Of course, we like the simultaneous approach because it is a 6 and a half hour effort once rather than doing 2 operations, which are almost as long.
Dr. Erkki Tukiainen: The blood flow through the flaps depends on the size. Latissimus dorsi has a flow of 20 to 50 mL per minute, which is perhaps enough to keep a long bypass open. Rectus abdominis has a little bit less, gracilis has even less, and its arterial supply is often affected by occlusive disease. Forearm flaps have a very tiny flow, but we can make it much bigger by use of a trick. This involves use of the radial forearm flap as a bypass flap letting the radial artery go through the flap with a covering skin island and by connecting the distal end of the radial artery with the recipient vessel. In this way, a considerable flow of 50 to 70 mL per minute can be reached. This will hold the long vessel open.
Dr. Karl-Walter Jauch: I enjoyed your presentation very much and would like to congratulate you on the excellent results. I have 3 short questions.
First, how often did you combine reconstruction or intervention above the knee together with the distal flaps. The second question is: did you differentiate between the etiology and type of ischemia, such as diabetic patients or patients with thromboangiitis obliterans? Are the other results worse or not, and how do you deal with those patients?
And the third question is: did you look at quality of life, especially in those patients who failed on the long-term basis with the reconstruction? Because one problem is always those patients who fail and who have many reoperations and finally fail. It would be good if you can select those patients before reconstruction.
Dr. Mauri Lepäntalo: Three inflow procedures were done surgically and 5 endovascularly, 2 of these both above and blow the knee level.
Regarding the second question, the diabetic patients fared as well as the nondiabetic patients. Their arteriosclerosis is actually the same as that of the nondiabetic patients. The only major difference is the predominant below-knee location in the patients with diabetes. Patency rates in patients with diabetes and nondiabetics do not usually differ in the vascular literature.
We had no patients with Buerger's disease.
The quality of life issue is very important to look at. Despite obvious bias, we asked the patients in the present study, just to make it simple: “Now that you know what you have gone through, would you really have wanted to have it?” A total of 5% felt that it was a wrong decision to do it in the first place. Now we are comparing in another study the quality of life in these patients with those patients who ended up having major amputation primarily.
Dr. Pierre Clavien: Thank you for sharing with us your experience with this spectacular type of surgery and your excellent results. I have 1 question. The frontier between postoperative bleeding and thrombosis is probably quite tight in these types of complex vascular reconstruction. What did you use for anticoagulants in the short- and long-term follow-up of these patients?
Dr. Erkki Tukiainen: If we performed a combined operation, we always gave systemic heparin according to the vascular surgical scheme. Bleeding may be a problem when the operative field is very large and oozing is likely, while wound excision or minor amputation is done, the flap and vein are harvested, reconstructions performed and skin taken. The patient may have 4 or 5 wounds. If I only do the microsurgical work, I just use low molecular weight heparin and nothing else. This decreases the bleeding.
Dr. Mauri Lepäntalo: The patients have lifelong treatment at least with aspirin as an antithrombotic agent.
Footnotes
Supported by Grants Finska Läkaresällskapet.
Reprints: Erkki Tukiainen, MD, PhD, Department of Plastic Surgery, Helsinki University Central Hospital, PB 266, FIN 00029 HUS, Finland. E-mail: erkki.tukiainen@hus.fi.
REFERENCES
- 1.Luther M, Kantonen I, Lepäntalo M, et al. Arterial interventions and reduction in amputation for chronic critical leg ischaemia. Br J Surg. 2000;87:454–458. [DOI] [PubMed] [Google Scholar]
- 2.Eskelinen E, Luther M, Eskelinen A, et al. Infra-popliteal bypass reduces amputation incidence in elderly patients: a population-based study. Eur J Vasc Endovasc Surg. 2003;26:65–68. [DOI] [PubMed] [Google Scholar]
- 3.Attinger CE, Ducic I, Cooper P, et al. The role of intrinsic muscle flaps of the foot for bone coverage in foot and ankle defects in diabetic and non-diabetic patients. Plast Reconstr Surg. 1999;110:1047–1053. [DOI] [PubMed] [Google Scholar]
- 4.DeFranzo AJ, Argenta LC, Marks MW, et al. the use of vacuum-assisted closure therapy for the treatment of lower-extremity wounds with exposed bone. Plast Rec Surg. 2001;108:1184–1191. [DOI] [PubMed] [Google Scholar]
- 5.Attinger C, Venturi M, Kim K, et al. Maximizing length and optimizing biomechanics in foot amputations by avoiding cookbook recipes for amputation. Semin Vasc Surg. 2003;16:44–66. [DOI] [PubMed] [Google Scholar]
- 6.Tukiainen E, Biancari F, Lepäntalo M. Deep infection of infrapopliteal autogenous vein grafts: immediate use of muscle flaps in leg salvage. J Vasc Surg. 1998;28:611–616. [DOI] [PubMed] [Google Scholar]
- 7.Baumeister SP, Spierer R, Erdmann D, et al. A realistic complication analysis of 70 sural artery flaps in a multimorbid patient group. Plast Reconstr Surg. 2003;112:129–140. [DOI] [PubMed] [Google Scholar]
- 8.Briggs SE, Banis JC Jr, Kaebnick H, et al. Distal revascularization and microvascular free tissue transfer: an alternative to amputation in ischemic lesions of the lower extremity. J Vasc Surg. 1985;2:806–811. [DOI] [PubMed] [Google Scholar]
- 9.Tukiainen E, Biancari F, Lepäntalo M. Lower limb revascularization and free flap transfer for major ischemic tissue loss. World J Surg. 2000;24:1531–1536. [DOI] [PubMed] [Google Scholar]
- 10.Vermassen FE, van Landuyt K. Combined vascular reconstruction and free flap transfer in diabetic arterial disease. Diabetes Metab Res Rev. 2000;16(suppl):33–36. [DOI] [PubMed] [Google Scholar]
- 11.Moran SL, Illig KA, Green RM, et al. Free-tissue transfer in patients with peripheral vascular disease: a 10-year experience. Plast Rec Surg. 2002;109:999–1006. [DOI] [PubMed] [Google Scholar]
- 12.Fontaine R, Kim M, Kieny R. Die chirurgische behandlung der peripheren durchblutungsstörungen. Helv Chir Acta. 1954;21:499–533. [PubMed] [Google Scholar]
- 13.Lavery AL, Armstrong DG, Harkless LB. Classification of diabetic foot wounds. J Foot Ankle Surg. 1996;35:528–531. [DOI] [PubMed] [Google Scholar]
- 14.Czerny M, Trubel W, Zimpfer D, et al. Limb-salvage by femoro-distal bypass and free muscle flap transfer. Eur J Vasc Endovasc Surg. 2004;27:635–639. [DOI] [PubMed] [Google Scholar]
- 15.Luther M. Treatment of chronic critical leg ischaemia: a cost benefit analysis. Ann Chir Gynaecol. 1997;86(suppl 213:1–142). [PubMed] [Google Scholar]
- 16.Lepäntalo M, Mätzke S. Outcome of unreconstructed chronic critical leg ischemia. Eur J Vasc Endovasc Surg. 1996;153–157. [DOI] [PubMed] [Google Scholar]
- 17.Pomposelli FB, Kansal N, Hamdan AD, et al. A decade of experience with dorsalis pedis artery bypass: analysis of outcome in more than 1000 cases. J Vasc Surg. 2003;37:307–315. [DOI] [PubMed] [Google Scholar]
- 18.Biancari F, Kantonen I, Mätzke S, et al. Infra-inguinal endovascular and bypass surgery for critical leg ischemia in patients on long-term dialysis. Ann Vasc Surg. 2002;16:210–214. [DOI] [PubMed] [Google Scholar]
- 19.Ramdev P, Rayan SS, Sheahan M, et al. A decade experience with infrainguinal revascularization in a dialysis-dependent patient population. J Vasc Surg. 2002;36:969–974. [DOI] [PubMed] [Google Scholar]
- 20.Lorenzetti F, Tukiainen E, Albäck A, et al. Blood flow in a pedal bypass combined with a free muscle flap. Eur J Vasc Endovasc Surg. 2001;22:161–164. [DOI] [PubMed] [Google Scholar]
- 21.Kanellopoulos G, Sabharwal A, MacGregor C. Major lower limb amputation for vascular disease in the Grampian area: the outcome of rehabilitation. J R Coll Surg (Edinburgh). 1996;41:114–115. [PubMed] [Google Scholar]
- 22.Valentine RJ, Myers SI, Inman MH, et al. Late outcome of amputees with premature atherosclerosis. Surgery. 1996;119:487–493. [DOI] [PubMed] [Google Scholar]
- 23.Peng CW, Tan SG. Perioperative and rehabilitative outcomes after amputation for ischemic leg gangrene. Ann Acad Med. 2000;29:168–172. [PubMed] [Google Scholar]
- 24.Eskelinen E, Lepäntalo M, Hietala E-M, et al. Lower limb amputations in Southern Finland in 2000 and trends up to 2001. Eur J Vasc Endovasc Surg. 2004;27:193–200. [DOI] [PubMed] [Google Scholar]