

Abstract
Objective:
To analyze the long-term results of distal pancreatectomy with en bloc celiac axis resection (DP-CAR), a newly designed extended surgical procedure for locally advanced cancer of the pancreatic body.
Summary Background Data:
Pancreatic body cancer often involves the common hepatic artery and/or the celiac axis and is regarded as an unresectable disease. We previously reported the feasibility and safety of DP-CAR in 10 patients and 3 preliminary cases; however, the long-term results are unknown.
Methods:
Between May 1998 and September 2005, 23 patients underwent DP-CAR. No reconstruction of the arterial system was required because of early development of the collateral arterial pathways via the pancreatoduodenal arcades from the superior mesenteric artery. We routinely used preoperative coil embolization of the common hepatic artery to enlarge the collateral pathways.
Results:
The postoperative mortality rate was 0%, despite a high morbidity rate (48%). The chief postoperative complications were pancreatic fistula and ischemic gastropathy. Contrary to expectations, postoperative diarrhea was mild. Preoperative intractable abdominal and/or back pain in 10 patients was completely alleviated immediately after surgery. The surgical margins were histologically negative in 21 patients (91%). The estimated overall 1- and 5-year survival rates were 71% and 42%, respectively, and the median survival was 21.0 months. The sites of recurrence were the liver in 6 patients and local recurrence in 2.
Conclusions:
DP-CAR offers a high R0 resectability rate and may potentially achieve complete local control in selected patients. The persisting early hepatic recurrence may indicate DP-CAR for the treatment of less advanced disease.
Distal pancreatectomy with en bloc celiac axis resection (DP-CAR), a newly designed extended surgical procedure for locally advanced cancer of the pancreatic body, offers a high R0 resectability rate. DP-CAR may potentially achieve complete local control in selected patients.
Locally advanced cancer of the body of the pancreas often involves the common hepatic artery and/or celiac axis with perineural invasion in the nerve plexus surrounding these arteries,1,2 and is regarded as an unresectable disease. To treat the disease, we have employed distal pancreatectomy with en bloc celiac axis resection (DP-CAR) and no arterial reconstruction, and we have used preoperative coil embolization of the common hepatic artery to decrease ischemia-related complications.3
In cancer of the head of the pancreas, the spread of the perineural invasion is directed towards the plexus around the superior mesenteric artery, via the pancreatic head plexus.4,5 Superior mesenteric artery resection and reconstruction is required to resect these plexuses en bloc; however, surgeons hesitate to perform this surgery because of technical difficulties and the risks related to arterial reconstruction.6,7 In addition, the poor postoperative quality of life, including severe diarrhea and malnutrition, discourages surgeons from performing a pancreatoduodenectomy combined with complete resection of the plexus surrounding the superior mesenteric artery.8 Finally, randomized controlled studies have shown that extended surgery does not contribute to long-term survival.9–11
To the contrary, in cancer of the body of the pancreas, perineural invasion spreads towards the celiac plexus and ganglions directly5 or via the nerve plexus surrounding the splenic and common hepatic arteries. DP-CAR enables en bloc resection of these structures without either arterial or pancreatobiliary-gastrointestinal reconstruction.
We previously reported the short-term results of DP-CAR in 10 patients and 3 preliminary cases.12 The purpose of this study was to analyze the long-term results of DP-CAR in 23 patients.
PATIENTS AND METHODS
In cases where pancreatic body tumors involved or touched the common hepatic artery, the root of the splenic artery, or the celiac axis, we employed DP-CAR provided that the gastroduodenal artery and superior mesenteric artery could be preserved (Fig. 1). Otherwise, we performed a conventional distal pancreatectomy. The procedures routinely included en bloc resection of the celiac, common hepatic, and left gastric arteries, the celiac plexus and ganglions, the nerve plexus around the superior mesenteric artery, a part of the crus of the diaphragm and the Gerota fascia, the left adrenal gland, the retroperitoneal fat tissues bearing lymph nodes above the left renal vein, the transverse mesocolon covering the body of the pancreas, and the inferior mesenteric vein (Figs. 2, 3). Resection of the portal vein and the middle colic vessels was optional. In general, no reconstruction of the arterial system was required because of early development of the collateral arterial pathways via the pancreatoduodenal arcades from the superior mesenteric artery (Fig. 4). Preoperative coil embolization of the common hepatic artery3 was routinely used to enlarge the collateral pathways and prevent ischemia-related complications. In addition, with preservation of the stomach, no reconstruction of the alimentary tract was required. Finally, the gallbladder was also preserved unless the arterial blood supply was compromised.

FIGURE 1. Late arterial phase contrast-enhanced CT showing a representative case. The common hepatic (H), splenic (S), and celiac (C) arteries are involved with a solid tumor (T) in the pancreatic body. However, the gastroduodenal artery (GDA) and superior mesenteric artery (SMA) can be preserved. An asterisk indicates the involved portal vein.

FIGURE 2. Schematic cross-sectional view showing the extent of a distal pancreatectomy with en bloc celiac axis resection. A dotted line indicates the dissection plane. adr, adrenal gland; Ao, aorta; CA, celiac axis; CHA, common hepatic artery; crus, crus of the diaphragm; Du, duodenum; g, celiac ganglion; IVC, inferior vena cava; pl, celiac plexus; PV, portal vein; SA, splenic artery; SV, splenic vein.

FIGURE 3. Operative photograph after completion of DP-CAR. Ao, aorta; CA, celiac axis; CHA, common hepatic artery; crus, crus of the diaphragm; GDA, gastroduodenal artery; graft, interposed iliac vein graft; IVC, inferior vena cava; RV, renal vein; SMA, superior mesenteric artery; SMV, superior mesenteric vein.
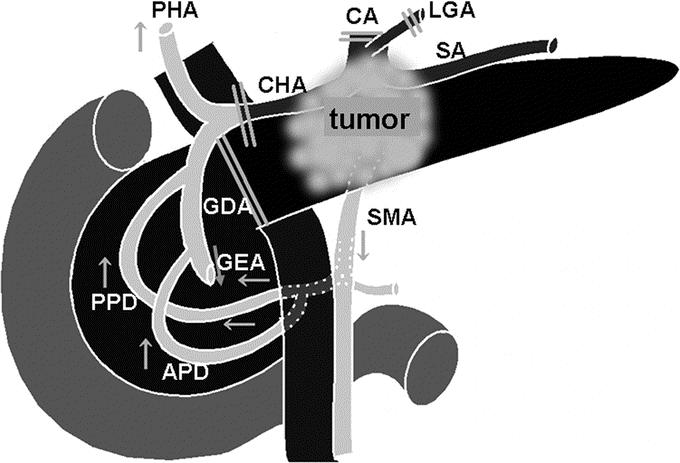
FIGURE 4. Schematic drawing of the collateral arterial pathways via the pancreatoduodenal arcades from the superior mesenteric artery following DP-CAR. APD, anterior pancreatoduodenal arcade; CA, celiac axis; CHA, common hepatic artery; GDA, gastroduodenal artery; GEA, right gastroepiploic artery; LGA, left gastric artery; PHA, proper hepatic artery; PPD, posterior pancreatoduodenal arcade; SA, splenic artery; SMA, superior mesenteric artery.
Between May 1998 and September 2005, 23 patients underwent DP-CAR. Informed consent was obtained from all patients. Their ages ranged from 54 to 75 years, with a median of 63 years, and the male/female ratio was 12/11. Ten patients had intractable abdominal and/or back pain, and 5 of these used morphine for preoperative pain control. Upon diabetic screening, 3 asymptomatic patients were diagnosed as having pancreatic tumors.
No definite chemotherapy or radiotherapy was added after surgery.
The median follow-up time for all 23 patients was 27.4 months. Estimated survival rates after surgery, including any deaths, were calculated using the Kaplan-Meier method.
RESULTS
Preoperative Arterial Embolization
Coil embolization of the common hepatic artery was planned in all patients and successfully performed in 19 patients between 1 and 16 days prior to the operation (median: 4 days prior). When the angiographic survey immediately after embolization showed favorable collateral flow from the superior mesenteric artery to the liver and stomach, DP-CAR was scheduled 1 or 2 days later. Embolization failed in 1 patient due to technical problems. Embolization was not required in 3 patients because of anatomic variation, such as the replaced hepatic artery from the superior mesenteric artery or the already dilated pancreatoduodenal arcades due to severe stenosis of the celiac axis.
There were no complications including hepatic dysfunction after embolization.
Operative Procedures
Concomitant portal vein resection was necessary in 16 patients, with 12 sleeves and 4 wedge resections. For reconstruction following the sleeve resections, end-to-end direct anastomosis was performed in 6 patients, and an autovein graft was interposed using the right external iliac vein in 4 patients and the left renal vein in 1 patient. In a patient with complete obstruction of the portal vein, portal reconstruction was not required due to preservation of the collateral venous pathways around the head of the pancreas. Unplanned arterial reconstruction was required in 3 patients due to accidental injuries during the operations. Two of the 3 patients underwent a middle colic artery-gastroepiploic artery bypass after injury to the inferior pancreatoduodenal artery13 and the other underwent end-to-end hepatic artery reconstruction.
The stomach was concomitantly resected in 3 patients (total, 2; wedge, 1), as was the colon in 3 patients and the jejunum in 1 due to direct cancer invasion. Total gastrectomy was required because partial distal gastrectomy with division of the right gastric and gastroepiploic arteries compromised arterial blood supply to the remnant stomach after celiac axis resection. Cholecystectomy was performed in 2 patients with cholecystitis and in 7 patients to prevent ischemia-related complications.
Operative time ranged from 348 to 732 minutes with a median of 532 minutes. Blood loss ranged from 490 to 4530 mL with a median of 1125 mL. Red blood cell transfusions were performed in 7 patients (30%).
Pathologic Findings
Tumor size varied from 20 to 100 mm with a median of 50 mm. According to the 2002 UICC TNM classification system,14 12 and 11 patients had T3 and T4 tumors, respectively, and 4, 8, 10, and 1 patients had stage IIA, IIB, III, and IV disease, respectively. However, according to the 2002 Japan Pancreatic Society (JPS) system (Table 1), 4 4, 16, and 3 patients had stage III, IVa, and IVb disease, respectively. Fifteen patients had lymph node metastasis, but not in the para-aortic area.
TABLE 1. 2002 JPS (Japan Pancreatic Society) Staging System of Pancreatic Cancer

The tumors were invasive ductal adenocarcinoma of the pancreas without any component of intraductal papillary mucinous neoplasm in all 23 patients. Histopathologic grading was G1 (well-differentiated) in 1 patient, G2 (moderately differentiated) in 13, and G3 (poorly differentiated) in 9. In 18 patients, extrapancreatic perineural invasion was present in the nerve plexus surrounding the celiac, common hepatic, splenic, and/or superior mesenteric arteries. The left adrenal gland was also involved in 2 patients. Lymphatic and venous invasion was detected in 17 and 20 patients, respectively. Intramural invasion of the resected portal vein was histologically confirmed in 13 of 16 patients who underwent portal vein resection, whereas intramural invasion of the celiac or common hepatic arteries was seen in only 2 patients, despite massive perineural invasion in the surrounding nerve plexuses. The surgical margins, including the retroperitoneum, were histologically clear (R0 resection) in 21 patients (91%).
Operative Morbidity and Mortality
The serum concentrations of alanine aminotransferase (ALT; normal range, 4–45 IU/L) and amylase (normal range: 40–160 IU/L) on postoperative day 1 ranged from 15 to 1853 (median: 102) and from 64 to 1385 (median: 212) IU/L, respectively (Fig. 5). Both returned to their normal ranges after several days. The patient with the exceptionally high levels of ALT (more than 1000 IU/L) developed asymptomatic hepatic infarction as demonstrated by routine postoperative CT. Two of the 3 patients with exceptionally high amylase levels (more than 500 IU/L) had received unplanned arterial reconstruction due to injuries to the inferior pancreatoduodenal artery, including several hours of pancreatic ischemia.
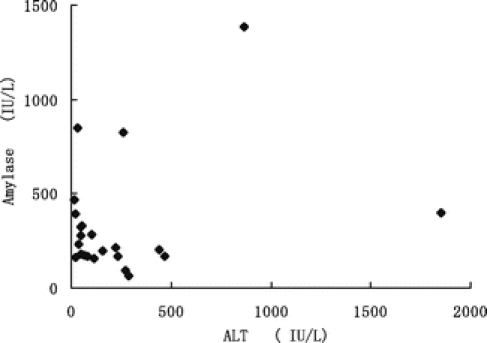
FIGURE 5. The serum concentrations of alanine aminotransferase (ALT) and amylase on postoperative day 1. Normal ranges: ALT, 4–45 IU/L; amylase, 40–160 IU/L.
The postoperative mortality rate was 0%, despite a high morbidity rate (48%). The primary postoperative complications were pancreatic fistula in 4 patients and ischemic gastropathy in 3. In the present study, ischemic gastropathy was defined as irregular, shallow, and wide ulcerations thought to be ischemic in origin.15 The other complications were ileus, omental necrosis, severe diarrhea, biliary infection, sepsis, myocardial infarction, and brain infarction in 1 patient each. Two patients required surgical intervention due to an ileus and intraperitoneal infection resulting from omental necrosis. Contrary to expectations, postoperative diarrhea was mild. Seven patients were regularly given loperamide hydrochloride, and only 1 was given tincture of opium. The preoperative intractable abdominal and/or back pain was completely relieved immediately after surgery in all 10 patients.
Postoperative Survival
Estimated overall 1- and 5-year survival rates were 71% and 42%, respectively, and the median survival was 21.0 months (Fig. 6). The median follow-up time for 14 survivors was 18.1 month. Estimated one- and five-year survival rates for the 16 patients with JPS stage IVa disease were 71% and 36%, respectively, and the median survival was 18.2 months. The 4 patients with JPS stage III disease are all alive 40, 35, 22, and 18 months after surgery, but the 3 patients with JPS stage IVb disease died of the disease within 16 months. The sites of recurrence in the patients who died were the liver in 6 patients and local recurrence in 2.

FIGURE 6. Estimated postoperative survival for patients who underwent DP-CAR.
DISCUSSION
DP-CAR has resulted in an estimated 5-year survival rate of 42% for patients with locally advanced cancer of the body of the pancreas involving or touching the common hepatic artery, the root of the splenic artery, and/or the celiac axis. These are cases that have previously been considered unresectable. Although we must be careful in assessing estimated survival rates since there has been only 1 actual 5-year survivor, the median survival time of 21.0 months is excellent considering the advanced stages of the disease. It is probable that DP-CAR may potentially achieve complete local control by en bloc resection of the distal pancreas, together with the entire surrounding structures, especially the nerve plexuses along the common hepatic, celiac, and superior mesenteric arteries. The high R0 resectability rate of 91% has not been achieved by conventional distal pancreatectomy.16–18
Despite the excellent local control, early hepatic recurrence still persists, especially in patients with more advanced stages of disease. Survival analysis according to JPS staging revealed a poor outcome for stage IVb disease, but an excellent result for stage III disease despite a small number of patients. This fact prompts the application of DP-CAR to less advanced disease, such as tumors in the body of the pancreas apart from the arteries. This is because even intraoperatively, it is difficult to identify perineural invasion into the periarterial nerve plexuses. DP-CAR, with its potential to provide complete local control, has proven its merit only against diseases that are unlikely to develop hepatic metastases.
The second advantage of DP-CAR is its safety based on the lack of the need for reconstruction of the arterial system and alimentary tract. The postoperative mortality rate was 0%, despite a high morbidity rate (48%) in the present study. Ischemic gastropathy,15 as seen in preliminary cases without preoperative coil embolization of the common hepatic artery, has decreased dramatically to an incidence of 13% after the introduction of embolization. Embolization has been safely performed without hepatic dysfunction in all patients including 8 nonresected patients who had minute peritoneal or hepatic metastasis discovered intraoperatively. Exceptionally high ALT (more than 1000 IU/L) and amylase (more than 500 IU/L) levels on postoperative day 1 suggest the presence of ischemia-related complications in the hepatobiliary and pancreatic system, and the possibility of injury to the pancreatoduodenal artery. It is recommended that surgeons identify the origin of the inferior pancreatoduodenal artery from the superior mesenteric artery by arteriography and contrast-enhanced arterial phase CT, both preoperatively and at the start of the surgical procedure, to avoid an accidental injury to this key vessel. Close attention should also be paid to signs of gastric ischemia. Arterial phase contrast-enhanced CT, which can be conducted postoperatively with less invasiveness, provides information about the postoperative arterial blood supply to the hepatobiliary, pancreatic, and gastrointestinal systems. When the arterial flow via the pancreatoduodenal artery is compromised, a middle colic artery-gastroepiploic artery bypass using microscopic techniques may rescue patients from fatal ischemia, as in the 2 patients of the present study.13
The third advantage of DP-CAR is the better postoperative quality of life that results from immediate and long-lasting relief of the intractable abdominal and/or back pain often caused by the disease.19 In addition, DP-CAR induces only minimal organ deficit that is limited to the distal pancreas, spleen, and left adrenal gland, and produces no or mild postoperative diarrhea and malnutrition. Although the excellent analgesic effect is understood by the complete clearance of the nerve plexuses and ganglions, the reason for the lack of serious diarrhea is unclear. Uncontrollable diarrhea is known to develop after pancreatoduodenectomy with circumferential resection of the nerve plexus around the superior mesenteric artery,8 and leads to poor appetite, malnutrition, and a generally poor quality of life. The extent of the clearance of autonomic nerve tissue is greater in DP-CAR, including resection of the celiac plexus and bilateral ganglions. The preserved continuity of the alimentary tract in its entirety might be responsible for the lack of or mild postoperative diarrhea.
In conclusion, DP-CAR for locally advanced pancreatic body cancer is feasible and safe, has the potential to achieve complete local control, and offers an improved quality of postoperative life. Because DP-CAR has proven its merit only against diseases that are unlikely to develop hepatic metastases, its application against less-advanced disease should be considered carefully. Further studies, including randomized trials, are necessary to elucidate its full impact on long-term survival and the effects of preoperative embolization.
ACKNOWLEDGMENTS
The authors thank Dr. Yuji Nimura, Dr. Hiroyuki Katoh, and Dr. Keiichi Maruyama for their support to this study.
Footnotes
This paper was partly presented at 13th meeting of the European Surgical Association, Zurich, on April 8, 2006.
Reprints: Satoshi Kondo, MD, Department of Surgical Oncology, Hokkaido University Graduate School of Medicine, N15 W7, Kita-ku, Sapporo 060-8638, Japan. E-mail: kondows@med.hokudai.ac.jp.
REFERENCES
- 1.Takahashi T, Ishikura H, Motohara T, et al. Perineural invasion by ductal adenocarcinoma of the pancreas. J Surg Oncol. 1997;65:164–170. [DOI] [PubMed] [Google Scholar]
- 2.Takahashi S, Hasebe T, Oda T, et al. Extra-tumor perineural invasion predicts postoperative development of peritoneal dissemination in pancreatic ductal adenocarcinoma. Anticancer Res. 2001;21:1407–1412. [PubMed] [Google Scholar]
- 3.Kondo S, Katoh H, Shimizu T, et al. Preoperative embolization of the common hepatic artery in preparation for radical pancreatectomy for pancreas body cancer. Hepatogastroenterology. 2000;47:1447–1449. [PubMed] [Google Scholar]
- 4.Japan Pancreas Society. Classification of Pancreatic Carcinoma, 2nd English ed. Tokyo: Kanehara Shuppan, 2003.
- 5.Yi SQ, Miwa K, Ohta T, et al. Innervation of the pancreas from the perspective of perineural invasion of pancreatic cancer. Pancreas. 2003;27:225–229. [DOI] [PubMed] [Google Scholar]
- 6.Fortner JG, Kim DK, Cubilla A, et al. Regional pancreatectomy: en bloc pancreatic, portal vein and lymph node resection. Ann Surg. 1977;186:42–50. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Nakano H, Bachellier P, Weber JC, et al. Arterial and vena caval resections combined with pancreaticoduodenectomy in highly selected patients with periampullary malignancies. Hepatogastroenterology. 2002;49:258–262. [PubMed] [Google Scholar]
- 8.Nagakawa T, Ueno K, Ohta T, et al. Evaluation of long-term survivors after pancreatoduodenectomy for pancreatoduodenal carcinoma. Hepatogastroenterology. 1995;42:117–122. [PubMed] [Google Scholar]
- 9.Farnell MB, Pearson RK, Sarr MG, et al. A prospective randomized trial comparing standard pancreatoduodenectomy with pancreatoduodenectomy with extended lymphadenectomy in resectable pancreatic head adenocarcinoma. Surgery. 2005;138:618–628. [DOI] [PubMed] [Google Scholar]
- 10.Pedrazzoli S, DiCarlo V, Dionigi R, et al. Standard versus extended lymphadenectomy associated with pancreatoduodenectomy in the surgical treatment of adenocarcinoma of the head of the pancreas: a multicenter, prospective, randomized study. Lymphadenectomy Study Group. Ann Surg. 1998;228:508–517. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Yeo CJ, Cameron JL, Lillemoe KD, et al. Pancreaticoduodenectomy with or without distal gastrectomy and extended retroperitoneal lymphadenectomy for periampullary adenocarcinoma, Part 2: Randomized controlled trial evaluating survival, morbidity, and mortality. Ann Surg. 2002;236:355–366. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Kondo S, Katoh H, Hirano S, et al. Results of radical distal pancreatectomy with en bloc resection of the celiac artery for locally advanced cancer of the pancreatic body. Langenbeck Arch Surg. 2003;388:101–106. [DOI] [PubMed] [Google Scholar]
- 13.Kondo S, Ambo Y, Katoh H, et al. Middle colic artery-gastroepiploic artery bypass for compromised collateral flow in distal pancreatectomy with celiac artery resection. Hepatogastroenterology. 2003;50:305–307. [PubMed] [Google Scholar]
- 14.International Union Against Cancer (UICC). TNM Classification of Malignant Tumors, 6th ed. New York: Wiley-Liss, 2002. [Google Scholar]
- 15.Kondo S, Katoh H, Hirano S, et al. Ischemic gastropathy after distal pancreatectomy with celiac axis resection. Surg Today. 2004;34:337–340. [DOI] [PubMed] [Google Scholar]
- 16.Shoup M, Conlon KC, Klimstra D, et al. Is extended resection for adenocarcinoma of the body or tail of the pancreas justified? J Gastrointest Surg. 2003;7:946–952. [DOI] [PubMed] [Google Scholar]
- 17.Kuhlmann KF, de Castro SM, Wesseling JG, et al. Surgical treatment of pancreatic adenocarcinoma; actual survival and prognostic factors in 343 patients. Eur J Cancer. 2004;40:549–558. [DOI] [PubMed] [Google Scholar]
- 18.Ozaki H, Kinoshita T, Kosuge T, et al. An aggressive therapeutic approach to carcinoma of the body and tail of the pancreas. Cancer. 1996;77:2240–2245. [DOI] [PubMed] [Google Scholar]
- 19.Kondo S, Katoh H, Omi M, et al. Radical distal pancreatectomy with en bloc resection of the celiac artery, plexus, and ganglions for advanced cancer of the pancreatic body: a preliminary report on perfect pain relief. JOP. 2001;2:93–97. [PubMed] [Google Scholar]