

Abstract
Background
Prior studies found inverse associations between high-density-lipoprotein cholesterol (HDL-C) or apolipoprotein A-1 with cardiovascular disease (CVD). Whether this is consistent across levels of low-density-lipoprotein cholesterol (LDL-C) or total atherogenic particle burden (apolipoprotein B100) is less well studied, particularly in women.
Objective
To determine the association between HDL-C or apolipoprotein A-1 with CVD across a range of LDL-C or apolipoprotein B100.
Design
Prospective cohort study.
Setting
The Women’s Healthy Study, a cohort of US female health professionals.
Participants
26,861 initially healthy women, age ≥ 45 years at study entry (1992–1995), followed for a mean of approximately 11 years.
Measurements
Baseline lipids were measured directly, and apolipoproteins with immunoassays. Outcomes were incident total CVD (N=929), coronary events (N=602), and stroke (N=319).
Results
In multivariable analyses, HDL-C and apolipoprotein A-1 were inversely associated with CVD and coronary events but not stroke. Adjusted coronary hazard ratios (HRs) for decreasing quintiles of HDL-C were 1.00, 1.23 (95% CI, 0.85–1.78), 1.42 (CI, 0.98–2.06), 1.90 (CI, 1.33–2.71), and 2.19 (CI, 1.51–3.19), P for linear trend<0.001; and for apolipoprotein A-1 1.00, 0.98 (CI, 0.71–1.35), 1.02 (CI, 0.72–1.44), 1.37 (CI, 0.98–1.90), and 1.58 (CI, 1.14–2.20), P for linear trend=0.005. Consistent inverse associations were found for HDL-C with coronary events across a range of LDL-C, including among women with low LDL-C. No associations were noted for HDL-C or apolipoprotein A-1 among women with low apolipoprotein B100 (<90 mg/dL).
Limitations
Population of low risk women, small numbers of events in the lowest apolipoprotein B100 stratum, single baseline measurements, and potential residual confounding.
Conclusion
Consistent inverse associations were found for HDL-C with incident coronary events among women with a range of LDL-C. Among women with low total atherogenic particle burden (apolipoprotein B100<90 mg/dL), few events occurred and no associations were seen.
Low-density lipoprotein cholesterol (LDL-C) is a well-established risk factor for cardiovascular disease (CVD) and is the primary target of therapy (1). While LDL particles are the predominant circulating atherogenic lipoproteins, other triglyceride-rich lipoproteins such as very-low-density and intermediate-density lipoproteins have been implicated in atherogenesis (2). Apolipoprotein B100 reflects the total number of atherogenic lipoprotein particles that include not only LDL particles but also the triglyceride-rich very-low-density and intermediate-density lipoprotein particles, since all atherogenic particles carry an apolipoprotein B protein in a one-to-one fashion (2). By contrast, high-density-lipoprotein (HDL) particles do not carry apolipoprotein B100, but instead carry apolipoprotein A-1. Hence, apolipoprotein A-1 reflects the potentially anti-atherogenic HDL particles, although not in a one-to-one fashion, since each HDL particle may carry one or more apolipoprotein A-1 molecule.
The inverse association between HDL cholesterol (HDL-C) and CVD is well-established (3–9). However, whether this inverse association of HDL-C with CVD remains across different levels of LDL-C is less well-studied, and the clinical significance of low HDL-C in patients with low LDL-C is presently debated. Among men, the inverse association of HDL-C with CVD was consistent across a range of LDL-C in several studies (4,6,10). Among women, particularly healthy women, there is a dearth of studies examining the association of HDL-C across a range of LDL-C (11).
Similarly, while low concentrations of apolipoprotein A-1, the major protein carried by HDL particles, have been associated inversely with CVD (2), it is unclear whether apolipoprotein A-1 is inversely associated with CVD across a range of LDL-C. It is also unclear whether apolipoprotein A-1 or HDL-C are inversely associated with CVD when concentrations of apolipoprotein B100, i.e. total atherogenic particles (including the triglyceride-rich particles), are low.
Therefore, we examined the associations of HDL-C and apolipoprotein A-1 with incident CVD, including coronary and stroke events, in apparently healthy women across a range of concentrations for LDL-C and apolipoprotein B100. Furthermore, since clinicians encounter women with very high HDL-C concentrations and it is unknown if these women are more protected against CVD, a secondary aim of this study was to determine whether extreme elevation of HDL-C occurring spontaneously in these women provided additional protection.
Methods
Study Population
Study participants were drawn from the Women’s Health Study, a completed randomized, double-blinded, placebo-controlled trial of low-dose aspirin and vitamin E in the primary prevention of cardiovascular disease (CVD) and cancer in women (12–14). Participants were apparently healthy female health care professionals, ages 45 years or older, who were free of self-reported CVD and cancer at study entry (1992–1995). At the time of enrollment, women gave written informed consent and completed questionnaires on demographics, anthropometrics, medical history, and lifestyle factors. They were also asked to provide a baseline blood sample; 28,345 women did so, and of these, a total of 28,023 had baseline lipid measurements. We excluded women with missing values for any of the lipid or apolipoprotein measurements (N=275) or those on lipid lowering medication (N=887), resulting in 26,861 women for analysis (Figure). The study was approved by the institutional review board of the Brigham and Women’s Hospital (Boston, Mass).
Figure.
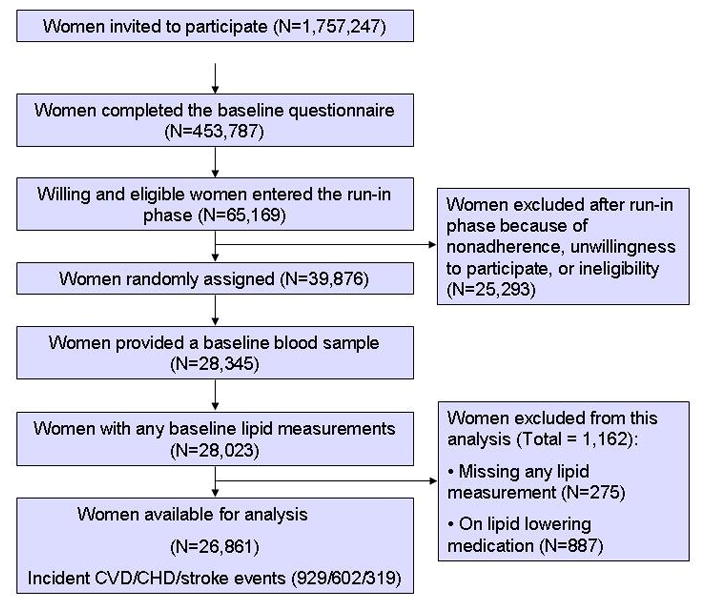
Study flow diagram. CVD = cardiovascular disease. CHD = coronary heart disease.
Laboratory measurements
EDTA blood samples were obtained at the time of enrollment and stored in vapor phase liquid nitrogen (−170°C). In a laboratory certified by the National Heart, Lung, and Blood Institute/Centers for Disease Control and Prevention Lipid Standardization program, baseline samples were thawed and analyzed for standard lipids. Direct determination of concentrations of HDL-C and LDL-C were simultaneously performed on the Hitachi 917 analyzer using reagents and calibrators from Roche Diagnostics (Indianapolis, IN). LDL-C was determined by a homogenous direct method from Roche Diagnostics. HDL-C was determined using a direct enzymatic colorimetric assay. Apolipoproteins A-1 and B100 were measured using immunoturbidimetric assays (DiaSorin, Stillwater, Minn). Coefficients of variation (CVs) for apolipoprotein A-1, LDL-C and HDL-C were <3%, and for apolipoprotein B100 <5%.
Ascertainment of CVD Events
The primary endpoints of interest were a composite endpoint of incident total CVD (nonfatal myocardial infarction, nonfatal stroke, percutaneous coronary intervention, coronary artery bypass grafting, or cardiovascular death), incident coronary disease (nonfatal myocardial infarction, percutaneous coronary intervention, coronary artery bypass grafting, or coronary death), or incident stroke. Every 6 months for the first year and annually thereafter, women received follow-up questionnaires about the occurrence of end points. Nonfatal endpoints were based on self-reports from follow-up questionnaires, letters, or telephone calls. For each reported CVD endpoint, we requested permission from the participant to examine the relevant medical records. A copy of the death certificate and additional records were requested as needed. Self-reported cases were classified as confirmed if they were reviewed by the Endpoints Committee and fulfilled the necessary confirmation criteria, and only confirmed events were included in analyses as previously described (14). The confirmatory rates among the records reviewed are 98.5% for CVD death, 95.8% for myocardial infarction, 97.8% for coronary artery bypass grafting, 94.9% for percutaneous coronary intervention, and 93.4% for stroke.
Statistical Analysis
Statistical analyses were done using STATA version 10.1. HDL-C and apolipoprotein A-1 were divided into quintiles based on their distribution among women who were not using postmenopausal hormones following guidelines from the Department of Health and Human Services for lipid standardization, and these quintile cut-points were then applied to the rest of the cohort (15). Survival analysis was performed using incidence rates and Cox proportional hazards regression models to adjust for covariates. P value for linear trend was obtained by using the median value for each quintile.
In order to compare our results with prior studies, we first adjusted for age (years), and then further adjusted for race, randomized treatment assignment, smoking status, systolic blood pressure, antihypertensive medication use, fasting status, alcohol use, and family history of premature coronary disease (Model 1), then added postmenopausal status, postmenopausal hormone use, body mass index, exercise, diabetes mellitus, high-sensitivity C-reactive protein, and triglycerides (Model 2). Models that did not stratify by LDL-C levels additionally included adjustment for LDL-C. Correlations between HDL-C or apolipoprotein A-1 and model covariates were low to moderate (Spearman r ≤|0.4|). Co-linearity of covariates was examined by comparing unadjusted with adjusted models, and no evidence of co-linearity was detected.
We then evaluated the associations of HDL-C and apolipoprotein A-1 with incident events by dividing participants by tertile cut-points for LDL-C or apolipoprotein B100, which were chosen in order to allow comparison of associations within similar strata of LDL-C and apolipoprotein B100.
Finally, we stratified according to baseline HDL-C or apolipoprotein A-1 deciles among non-hormone users in order to examine naturally-occurring extreme elevations in HDL-C or apolipoprotein A-1. We determined the associations and characteristics of women with extreme elevation of HDL-C or apolipoprotein A-1, defined as the top decile or the top 3% of concentrations. All reported P values were two-tailed with <0.05 considered significant.
Role of the Funding Source
The research for this article was supported by an investigator-initiated research grants to Dr. Mora from Merck. The study was additionally supported by the National Heart, Lung, and Blood Institute and the National Cancer Institute. Dr Cui is an employee of Merck, otherwise the funding sources played no role in the design, conduct, data management, analysis, or the decision to submit the manuscript for publication.
Results
The study participants were middle-aged women at baseline (Table 1), with mean (SD) concentrations of 1.40 (0.39) mmol/L (54 [15] mg/dL) for HDL-C and 151 (26) mg/dL for apolipoprotein A-1. As expected, baseline prevalence of cardiovascular risk factors was inversely associated with HDL-C. Similar results were found when these baseline risk factors were examined across quintiles of apolioprotein A-1 (data not shown).
Table 1.
Baseline Characteristics of 26,861 Participants in the Women’s Health Study
| Characteristic | All | High-density lipoprotein cholesterol quintile, mmol/L (mg/dL) | ||||
|---|---|---|---|---|---|---|
| N = 26861 | >1.60 (>61.6) | 1.37–1.60 (52.8–61.6) | 1.20–1.36 (46.2–52.7) | 1.03–1.19 (39.6–46.1) | ≤1.02 (≤39.5) | |
| Age, y | 54.5(7.0) | 55.0(6.9) | 54.5(7.0) | 54.2(6.9) | 54.4(7.2) | 54.4(7.3) |
| Hypertension, % | 24.2 | 19.2 | 20.3 | 23.6 | 27.9 | 34.8 |
| Current smoking, % | 11.6 | 8.3 | 9.7 | 11.6 | 13.0 | 18.3 |
| Diabetes, % | 2.5 | 1.1 | 1.5 | 2.0 | 2.9 | 6.4 |
| Postmenopausal, % | 53.7 | 59.3 | 53.8 | 50.7 | 51.0 | 50.3 |
| Postmenopausal hormone use, % | 43.3 | 57.6 | 47.0 | 39.7 | 34.7 | 28.9 |
| ≥ 1 Alcoholic drink/d | 10.3 | 17.1 | 11.5 | 8.1 | 6.0 | 4.8 |
| Exercise ≥ once/wk | 62.8 | 68.0 | 64.6 | 62.4 | 58.6 | 56.3 |
| Parental history, % | 12.6 | 11.1 | 12.0 | 13.2 | 13.3 | 14.4 |
| Body mass index, kg/m2 | 25.9 (5.0) | 23.7(3.6) | 25.0 (4.2) | 26.1 (4.8) | 27.4 (5.2) | 28.9 (5.7) |
| Apolipoprotein A-I, mg/dL | 151 (26) | 177 (20) | 157 (16) | 146 (16) | 136(14) | 122 (16) |
| Apolipoprotein B100, mg/dL | 103(28) | 92(24) | 99(25) | 105(27) | 110(28) | 116(29) |
| Total cholesterol, mmol/L | 5.46 (1.09) | 5.75 (1.11) | 5.46 (0.98) | 5.41 (1.01) | 5.36 (1.04) | 5.21 (1.14) |
| mg/dL | 211(42) | 222 (43) | 211 (38) | 209(39) | 207(40) | 201 (44) |
| Low-density lipoprotein cholesterol, mmol/L | 3.21 (0.88) | 3.13 (9.07) | 3.21 (0.85) | 3.29 (0.85) | 3.32 (0.85) | 3.11 (0.88) |
| mg/dL | 124 (34) | 121 (35) | 124 (33) | 127(33) | 128 (33) | 120(34) |
| Median triglycerides (25th, 75th percentile), mmol/L | 1.32 (0.94,4.48) | 1.04 (0.77,1.44) | 1.20 (0.86,1.70) | 1.36 (0.98,1.92) | 1.58 (1.13,2.21) | 2.02 (1.40,2.98) |
| mg/dL | 117 (83,173) | 92 (68,127) | 106(76,150) | 120 (87,170) | 140 (100,196) | 179 (124,264) |
| Median high-sensitivity C-reactive protein (25th, 75th percentile), mg/L | 2.0 (0.8,4.3) | 1.5(0.6,3.5) | 1.7(0.7,3.9) | 2.0 (0.8,4.2) | 2.3(1.0,4.8) | 3.0 (1.4,5.8) |
Values shown for continuous variables are percentage or mean (SD) unless otherwise indicated. P values were obtained from analysis of variance for continuous variables expressed as means, for nonparametric Cuzick’s extension to the Wilcoxon rank-sum test for trend comparing medians, and from chi-square tests for categorical variables. All P values were <0.001. Parental history defined as myocardial infarction occurring in a parent before age 60 years.
HDL-C, apolipoprotein A-1, and incident events
During a mean (SD) follow-up of 11.1 (1.3) years, there were 929 incident total CVD events, of which 602 were coronary (myocardial infarction, coronary revascularization, or coronary death) and 319 were stroke. The incident CVD and coronary event rates increased linearly with lower concentrations of HDL-C or apolipoprotein A-1 (P for linear trend, <0.001; Table 2), while only the lowest quintile of HDL-C had increased risk of stroke. After adjusting for known cardiovascular risk factors (models 1 and 2), HDL-C remained inversely associated with CVD and coronary events. Adjusted coronary event hazard ratios (HRs) for decreasing quintiles of HDL-C were 1.00 (reference), 1.23 (95% CI, 0.85–1.78), 1.42 (CI, 0.98–2.06), 1.90 (CI, 1.33–2.71), and 2.19 (CI, 1.51–3.19), P for linear trend<0.001. Broadly similar but generally weaker associations were noted for apolipoprotein A-1, with adjusted coronary event HRs for decreasing quintiles of apolipoprotein A-1 of 1.00 (reference), 0.98 (CI, 0.71–1.35), 1.02 (CI, 0.72–1.44), 1.37 (CI, 0.98–1.90), and 1.58 (CI, 1.14–2.20), P for linear trend=0.005.
Table 2.
Association of High-Density Lipoprotein Cholesterol and Apolipoprotein A-I with Cardiovascular Outcomes
| >1.60 (>61.6) | High-density lipoprotein cholesterol quintile, mmol/L (mg/dL) | P for linear trend | ||||
|---|---|---|---|---|---|---|
| 1.37–1.60 (52.8–61.6) | 1.20–1.36 (46.2–52.7) | 1.03–1.19 (39.6–46.1) | ≤1.02 (≤39.5) | |||
|
Total cardiovascular disease; No. CVD/Total N: 929/26,861
| ||||||
| Event rate/1000 p-y (95% CI) | 2.03 (1.74–2.36) | 2.38 (2.03–2.79) | 2.98 (2.55–3.48) | 3.93 (3.42–4.52) | 5.57 (4.93–6.29) | |
| HR (95% CI) | ||||||
| Age-adjusted | 1.0 | 1.21 (0.97–1.51) | 1.58 (1.27–1.96) | 2.01 (1.63–2.48) | 2.86 (2.35–3.49) | <0.001 |
| Model 1* | 1.0 | 1.16 (0.90–1.48) | 1.48 (1.16–1.89) | 1.63 (1.28–2.07) | 2.33 (1.86–2.93) | <0.001 |
| Model 2† | 1.0 | 1.13 (0.85–1.48) | 1.29 (0.98–1.71) | 1.47 (1.11–1.93) | 1.69 (1.27–2.26) | <0.001 |
|
| ||||||
|
Coronary heart disease‡; No. CHD/Total N: 602/26,861
| ||||||
| Event rate/1000 p-y (95% CI) | 1.12 (0.91–1.37) | 1.40 (1.14–1.72) | 1.86(1.53–2.26) | 2.70 (2.29–3.20) | 4.02 (3.48–4.64) | |
| HR (95% CI) | ||||||
| Age-adjusted | 1.0 | 1.29 (0.96–1.72) | 1.77 (1.33–2.36) | 2.51 (1.92–3.28) | 3.75 (2.92–4.83) | <0.001 |
| Model 1 | 1.0 | 1.31 (0.94–1.81) | 1.72 (1.25–2.36) | 2.08 (1.53–2.83) | 3.01 (2.24–4.04) | <0.001 |
| Model 2 | 1.0 | 1.23 (0.85–1.78) | 1.42 (0.98–2.06) | 1.90 (1.33–2.71) | 2.19 (1.51–3.19) | <0.001 |
|
| ||||||
|
Stroke; No. Stroke/Total N: 319/26,861
| ||||||
| Event rate/1000 p-y (95% CI) | 1.02 (0.82–1.26) | 0.90 (0.69–1.16) | 1.02 (0.78–1.33) | 0.97 (0.73–1.28) | 1.62(1.29–2.02) | |
| HR (95% CI) | ||||||
| Age-adjusted | 1.0 | 0.91 (0.65–1.28) | 1.08 (0.76–1.52) | 0.98 (0.69–1.40) | 1.64 (1.20–2.24) | 0.011 |
| Model 1 | 1.0 | 0.83 (0.57–1.23) | 0.98 (0.66–1.44) | 0.80 (0.53–1.21) | 1.38 (0.97–1.98) | 0.22 |
| Model 2 | 1.0 | 0.89 (0.58–1.35) | 1.03 (0.67–1.59) | 0.83 (0.52–1.32) | 1.21 (0.76–1.93) | 0.68 |
| Apolipoprotein A-I quintile, mg/dL | ||||||
| >159.7 | 146.3–159.7 | 135.5–146.2 | 124.1–135.4 | ≤ 124 | P for linear trend | |
|
| ||||||
|
Total cardiovascular disease; No. CVD/Total N: 929/26,861
| ||||||
| Event rate/1000 p-y (95% CI) | 2.62 (2.32–2.96) | 2.72 (2.33–3.18) | 2.87 (2.43–3.39) | 3.90 (3.36–4.54) | 4.64 (4.04–5.34) | |
| HR (95% CI) | ||||||
| Age-adjusted | 1.0 | 1.11 (0.91–1.36) | 1.19 (0.97–1.46) | 1.69 (1.40–2.05) | 2.11 (1.75–2.54) | <0.001 |
| Model 1* | 1.0 | 1.17(0.94–1.45) | 1.05 (0.83–1.33) | 1.58 (1.27–1.96) | 1.80(1.45–2.23) | <0.001 |
| Model 2† | 1.0 | 1.10 (0.86–1.40) | 0.99 (0.75–1.30) | 1.40 (1.09–1.81) | 1.36 (1.04–1.78) | 0.011 |
|
| ||||||
|
Coronary heart disease‡; No. CHD/Total N: 602/26,861
| ||||||
| Event rate/1000 p-y (95% CI) | 1.59 (1.37–1.86) | 1.61 (1.31–1.97) | 1.91 (1.56–2.34) | 2.50 (2.08–3.02) | 3.39 (2.88–4.00) | |
| HR (95% CI) | ||||||
| Age-adjusted | 1.0 | 1.07 (0.83–1.39) | 1.30 (1.00–1.67) | 1.77 (1.39–2.25) | 2.50 (2.00–3.14) | <0.001 |
| Model 1 | 1.0 | 1.11 (0.84–1.47) | 1.12 (0.84–1.51) | 1.68(1.28–2.20) | 2.09 (1.61–2.71) | <0.001 |
| Model 2 | 1.0 | 0.98 (0.71–1.35) | 1.02 (0.72–1.44) | 1.37 (0.98–1.90) | 1.58 (1.14–2.20) | 0.005 |
|
| ||||||
|
Stroke; No. Stroke/Total N: 319/26,861
| ||||||
| Event rate/1000 p-y (95% CI) | 1.12 (0.94–1.35) | 1.07 (0.83–1.37) | 0.76 (0.55–1.05) | 1.15 (0.88–1.52) | 1.27(0.97–1.66) | |
| HR (95% CI) | ||||||
| Age-adjusted | 1.0 | 1.02 (0.75–1.40) | 0.73 (0.51–1.06) | 1.17 (0.84–1.62) | 1.35 (0.97–1.86) | 0.195 |
| Model 1 | 1.0 | 1.15 (0.82–1.51) | 0.71 (0.47–1.09) | 1.08 (0.74–1.58) | 1.19 (0.82–1.74) | 0.64 |
| Model 2 | 1.0 | 1.17 (0.80–1.72) | 0.73 (0.45–1.18) | 1.20 (0.78–1.83) | 1.01 (0.64–1.60) | 0.93 |
Adjusted for age, race, randomized treatment assignment, smoking status, blood pressure, antihypertensive medication use, fasting status, alcohol use, and family history.
Adjusted for the covariates in Model 1 plus postmenopausal status, hormone use, body mass index, exercise, diabetes mellitus, high-sensitivity C-reactive protein, triglycerides, and LDL cholesterol.
Comprising myocardial infarction, coronary revascularization, and deaths from coronary heart disease.
Inverse associations were also noted for HDL-C and apolipoprotein A-1 with CVD and coronary events within subgroups of women stratified according to age, race, hypertension, smoking status, diabetes, hormone use, and body mass index (data not shown).
In multivariable analyses, no associations were noted for either HDL-C or apolipoprotein A-1 in relation to stroke.
Associations across strata of LDL-C
Since the associations of HDL-C and apolipoprotein A-1 with CVD were driven by coronary events and not stroke, we then performed stratified analyses to examine coronary events across concentrations for LDL-C. As shown in Table 3, the lowest event rates (0.62/1000 person-years) were seen among women with values in the top quintile of HDL-C (>1.60 mmol/L, 61.6 mg/dL) and concomitantly low LDL-C (<2.80 mmol/L, 108 mg/dL). After adjusting for other risk factors, the inverse association of HDL-C remained statistically significant for coronary events across a range of concentrations for LDL-C, even among women with low LDL-C (model 2 adjusted coronary HRs for decreasing quintiles of HDL-C were 1.00 [reference], 1.78 [CI, 0.77–4.08], 0.98 [CI, 0.33–2.84], 2.30 [CI, 0.99–5.34], and 2.71 [CI, 1.14–6.46], P for linear trend=0.031).
Table 3.
Association of High-Density Lipoprotein Cholesterol with Coronary Heart Disease Events According to Tertiles of Low-Density Lipoprotein Cholesterol
| >1.60 (>61.6) | High-density lipoprotein cholesterol quintile, mmol/L (mg/dL) | P for linear trend | ||||
|---|---|---|---|---|---|---|
| 1.37–1.60 (52.8–61.6) | 1.20–1.36 (46.2–52.7) | 1.03–1.19 (39.6–46.1) | ≤1.02 (≤39.5) | |||
|
LDL cholesterol
| ||||||
| Bottom third, LDL cholesterol <2.80 mmol/L (108mg/dL), mean 2.31 mmol/L (89 mg/dL) | ||||||
| No. CHD/Total N: 117/8,965
| ||||||
| Event rate/1000 p-y (95% CI) | 0.62 (0.40–0.97) | 0.85 (0.54–1.35) | 0.77 (0.44–1.35) | 1.68 (1.13–2.51) | 2.49 (1.93–3.49) | |
| Adjusted hazard ratios (95% CI) | ||||||
| Model 1* | 1.0 | 1.48 (0.75–2.95) | 1.36 (0.63–2.91) | 1.99 (1.00–3.95) | 3.22 (1.75–5.92) | <0.001 |
| Model 2† | 1.0 | 1.78 (0.77–4.08) | 0.98 (0.33–2.84) | 2.30 (0.99–5.34) | 2.71 (1.14–6.46) | 0.031 |
|
| ||||||
| Middle third, LDL cholesterol 2.80–3.50 mmol/L (108–135 mg/dL), mean 3.13 mmol/L (121 mg/dL) | ||||||
| No. CHD/Total N: 192/8,948
| ||||||
| Event rate/1000 p-y (95% CI) | 1.16 (0.81–1.65) | 1.19 (0.81–1.75) | 1.80 (1.28–2.54) | 2.38 (1.75–3.25) | 4.13 (3.22–5.28) | |
| Adjusted hazard ratios (95% CI) | ||||||
| Model 1 | 1.0 | 1.28 (0.71–2.30) | 1.97 (1.12–3.44) | 2.01 (1.14–3.55) | 3.72 (2.22–6.24) | <0.001 |
| Model 2 | 1.0 | 1.06 (0.55–2.03) | 1.46 (0.77–2.77) | 1.98 (1.06–3.69) | 2.22 (1.16–4.24) | 0.006 |
|
| ||||||
| Upper third, LDL cholesterol>3.50 mmol/L (135 mg/dL), mean 4.17 mmol/L (161 mg/dL) | ||||||
| No. CHD/Total N: 293/8,948
| ||||||
| Event rate/1000 p-y (95% CI) | 1.73 (1.27–2.36) | 2.14 (1.61–2.86) | 2.76 (2.12–3.60) | 3.75 (2.97–4.72) | 5.59 (4.49–6.96) | |
| Adjusted hazard ratios (95% CI) | ||||||
| Model 1 | 1.0 | 1.16 (0.72–1.86) | 1.51 (0.95–2.39) | 1.94 (1.25–3.02) | 2.41 (1.54–3.76) | <0.001 |
| Model 2 | 1.0 | 1.13 (0.67–1.91) | 1.44 (0.86–2.41) | 1.74 (1.04–2.90) | 1.75 (1.01–3.04) | 0.016 |
Coronary heart disease: defined as myocardial infarction, coronary revascularization, and deaths from coronary heart disease.
Model 1: adjusted for age, race, randomized treatment assignment, smoking status, blood pressure, antihypertensive medication use, fasting status, alcohol use, and family history.
Model 2: adjusted for the covariates in Model 1 plus postmenopausal status, hormone use, body mass index, exercise, diabetes mellitus, high-sensitivity C-reactive protein, and triglycerides.
Weaker inverse associations were found for apolipoprotein A-1 with coronary events (Appendix Table), particularly among women with LDL-C below 3.50 mmol/L (135 mg/dL). Further, there were no associations for HLD-C or apolipoprotein A-1 with stroke across strata of LDL-C after multivariable adjustment (data not shown).
Appendix Table.
Association of Apolipoprotein A-1 with Coronary Heart Disease Events According to Tertiles of Low-Density Lipoprotein Cholesterol or Apolipoprotein B100
| >159.7 | Apolipoprotein A-I quintile, mg/dL | P for linear trend | ||||
|---|---|---|---|---|---|---|
| 146.3–159.7 | 135.5–146.2 | 124.1–135.4 | ≤ 124 | |||
|
LDL cholesterol
| ||||||
| Bottom third, LDL cholesterol <2.80 mmol/L (108 mg/dL), mean 2.31 mmol/L (89 mg/dL) | ||||||
| No. CHD/Total N: 117/8,965
| ||||||
| Event rate/1000 p-y (95% CI) | 1.07 (0.79–1.46) | 0.80 (0.48–1.33) | 0.89 (0.52–1.53) | 1.48 (0.94–2.32) | 2.01 (1.40–2.90) | |
| Adjusted hazard ratios (95% CI) | ||||||
| Model 1 | 1.0 | 0.85 (0.45–1.60) | 0.85 (0.42–1.72) | 1.53 (0.82–2.84) | 1.85 (1.07–3.20) | 0.037 |
| Model 2 | 1.0 | 1.05 (0.48–2.27) | 0.96 (0.39–2.36) | 2.01 (0.91–4.44) | 1.72 (0.79–3.74) | 0.113 |
|
| ||||||
| Middle third, LDL cholesterol 2.80–3.50 mmol/L (108–135 mg/dL), mean 3.13 mmol/L (121 mg/dL) | ||||||
| No. CHD/Total N: 192/8,948
| ||||||
| Event rate/1000 p-y (95% CI) | 1.70 (1.31–2.20) | 1.39 (0.94–2.04) | 1.61 (1.10–2.36) | 2.38 (1.72–3.30) | 3.28 (2.46–4.38) | |
| Adjusted hazard ratios (95% CI) | ||||||
| Model 1 | 1.0 | 1.11 (0.68–1.81) | 1.09 (0.65–1.83) | 1.59 (0.99–2.54) | 1.93 (1.21–3.06) | 0.005 |
| Model 2 | 1.0 | 0.98 (0.56–1.72) | 0.95 (0.52–1.75) | 1.18(0.67–2.10) | 1.28 (0.72–2.28) | 0.43 |
|
| ||||||
| Upper third, LDL cholesterol>3.50 mmol/L (135 mg/dL), mean 4.17 mmol/L (161 mg/dL) | ||||||
| No. CHD/Total N: 293/8,948
| ||||||
| Event rate/1000 p-y (95% CI) | 2.14 (1.67–2.73) | 2.54 (1.93–3.33) | 3.03 (2.32–3.95) | 3.43 (2.64–4.47) | 4.96 (3.91–6.29) | |
| Adjusted hazard ratios (95% CI) | ||||||
| Model 1 | 1.0 | 1.19 (0.79–1.80) | 1.17 (0.76–1.80) | 1.67 (1.11–2.52) | 2.19 (1.47–3.27) | <0.001 |
| Model 2 | 1.0 | 0.99 (0.62–1.60) | 1.10 (0.68–1.78) | 1.36 (0.85–2.20) | 1.67 (1.03–2.70) | 0.032 |
|
Apolipoprotein B100
| ||||||
| Bottom third, apolipoprotein B100 <90 mg/dL (mean 75 mg/dL) | ||||||
| No. CHD/Total N: 78/8,989
| ||||||
| Event rate/1000 p-y (95% CI) | 0.99 (0.72–1.36) | 0.57 (0.31–1.02) | 0.55 (0.29–1.06) | 0.75 (0.41–1.40) | 0.81 (0.44–1.50) | |
| Adjusted hazard ratios (95% CI) | ||||||
| Model 1 | 1.0 | 0.64 (0.31–1.30) | 0.67 (0.32–1.40) | 0.66 (0.29–1.52) | 0.72 (0.32–1.58) | 0.192 |
| Model 2 | 1.0 | 0.69 (0.30–1.58) | 0.66 (0.27–1.62) | 0.92 (0.36–2.31) | 0.51 (0.18–1.48) | 0.25 |
|
| ||||||
| Middle third, apolipoprotein B100 90–113mg/dL (mean 101 mg/dL) | ||||||
| No. CHD/Total N: 174/8,940
| ||||||
| Event rate/1000 p-y (95% CI) | 1.39 (1.05–1.84) | 1.27 (0.86–1.88) | 1.72 (1.18–2.50) | 2.43 (1.75–3.39) | 2.85 (2.07–3.91) | |
| Adjusted hazard ratios (95% CI) | ||||||
| Model 1 | 1.0 | 1.22 (0.72–3.08) | 1.36 (0.77–2.38) | 2.11 (1.27–3.52) | 2.45 (1.47–4.08) | <0.001 |
| Model 2 | 1.0 | 1.03 (0.55–1.94) | 1.29 (0.67–2.48) | 1.52 (0.79–2.93) | 2.05 (1.10–3.83) | 0.025 |
|
| ||||||
| Upper third, apolipoprotein B100>113 mg/dL (mean 134 mg/dL) | ||||||
| No. CHD/Total N: 350/8,932
| ||||||
| Event rate/1000 p-y (95% CI) | 2.65 (2.12–3.32) | 3.03 (2.34–3.93) | 3.44 (2.66–4.47) | 3.97 (3.12–5.07) | 5.78 (4.73–7.07) | |
| Adjusted hazard ratios (95% CI) | ||||||
| Model 1 | 1.0 | 1.17 (0.80–1.71) | 1.11 (0.74–1.65) | 1.66 (1.15–2.40) | 2.10 (1.48–2.98) | <0.001 |
| Model 2 | 1.0 | 1.04 (0.67–1.61) | 0.98 (0.61–1.55) | 1.43 (0.92–2.20) | 1.57 (1.02–2.42) | 0.030 |
Coronary heart disease: defined as myocardial infarction, coronary revascularization, and deaths from coronary heart disease.
Model 1: adjusted for age, race, randomized treatment assignment, smoking status, blood pressure, antihypertensive medication use, fasting status, alcohol use, and family history.
Model 2: adjusted for the covariates in Model 1 plus postmenopausal status, hormone use, body mass index, exercise, diabetes mellitus, high-sensitivity C-reactive protein, and triglycerides.
Associations across strata of apolipoprotein B100
Associations were noted for HDL-C or apolipoprotein A-1 only among women with apolipoprotein B100 ≥ 90 mg/dL (Table 4 and Appendix Table), i.e. in the presence of atherogenic particles that include LDL and the triglyceride-rich lipoprotein particles. The P value for interaction of apolipoprotein B100 by HDL-C was 0.28, and for apolipoprotein B100 by apolipoprotein A-1 0.21. In multivariable analysis, there were no associations for HDL-C or apolipoprotein A-1 with stroke across strata of apolipoprotein B100.
Table 4.
Association of High-Density Lipoprotein Cholesterol with Coronary Heart Disease Events According to Tertiles of Apolipoprotein B100
| >1.60 (>61.6) | High-density lipoprotein cholesterol quintile, mmol/L (mg/dL) | P for linear trend | ||||
|---|---|---|---|---|---|---|
| 1.37–1.60 (52.8–61.6) | 1.20–1.36 (46.2–52.7) | 1.03–1.19 (39.6–46.1) | ≤1.02 (≤39.5) | |||
|
Apolipoprotein B100
| ||||||
| Bottom third, apolipoprotein B100 <90 mg/dL (mean 75 mg/dL) | ||||||
| No. CHD/Total N: 78/8,989
| ||||||
| Event rate/1000 p-y (95% CI) | 0.76 (0.53–1.09) | 0.63 (0.38–1.04) | 0.62 (0.33–1.15) | 1.16 (0.69–1.95) | 1.10 (0.57–2.11) | |
| Adjusted hazard ratios (95% CI) | ||||||
| Model 1* | 1.0 | 1.07 (0.56–2.04) | 1.01 (0.48–2.12) | 1.20 (0.57–2.54) | 1.31 (0.58–2.98) | 0.54 |
| Model 2† | 1.0 | 1.16 (0.56–2.40) | 0.95 (0.39–2.35) | 0.95 (0.38–2.34) | 0.53 (0.15–1.94) | 0.56 |
|
| ||||||
| Middle third, apolipoprotein B100 90–113 mg/dL (mean 101 mg/dL) | ||||||
| No. CHD/Total N: 174/8,940
| ||||||
| Eventrate/1000 p-y (95% CI) | 0.84 (0.55–1.28) | 1.54 (1.11–2.15) | 1.90 (1.37–2.65) | 2.22 (1.61–3.06) | 3.13 (2.34–4.19) | |
| Adjusted hazard ratios (95% CI) | ||||||
| Model 1 | 1.0 | 2.35 (1.26–4.39) | 3.02 (1.61–5.65) | 2.22 (1.14–4.35) | 4.51 (2.43–8.35) | <0.001 |
| Model 2 | 1.0 | 2.11 (1.05–4.22) | 2.24 (1.08–4.66) | 2.54 (1.21–5.33) | 3.92 (1.86–8.26) | <0.001 |
|
| ||||||
| Upper third, apolipoprotein B100>113 mg/dL (mean 134 mg/dL) | ||||||
| No. CHD/Total N: 350/8,932
| ||||||
| Event rate/1000 p-y (95% CI) | 2.60 (1.88–3.59) | 2.25 (1.65–3.06) | 2.85 (2.19–3.71) | 3.95 (3.19–4.88) | 5.56 (4.69–6.59) | |
| Adjusted hazard ratios (95% CI) | ||||||
| Model 1 | 1.0 | 0.82 (0.50–1.35) | 1.11 (0.70–1.76) | 1.59 (1.03–2.43) | 1.93 (1.28–2.92) | <0.001 |
| Model 2 | 1.0 | 0.75 (0.43–1.32) | 1.02 (0.61–1.72) | 1.45 (0.89–2.36) | 1.37 (0.83–2.27) | <0.001 |
Coronary heart disease: defined as myocardial infarction, coronary revascularization, and deaths from coronary heart disease.
Model 1: adjusted for age, race, randomized treatment assignment, smoking status, blood pressure, antihypertensive medication use, fasting status, alcohol use, and family history.
Model 2: adjusted for the covariates in Model 1 plus postmenopausal status, hormone use, body mass index, exercise, diabetes mellitus, high-sensitivity C-reactive protein, and triglycerides.
Sensitivity Analyses
We performed sensitivity analyses to assess the extent to which an unmeasured covariate might explain the results (16). An unobserved dichotomous covariate that is near-perfectly correlated with coronary events would have to increase the odds of having a low (below median) HDL-C by a factor of 1.90, or apolipoprotein A-1 by a factor of 1.35, in order to account for the results (at a 5% significance level), regardless of the assumed prevalence of the unobserved covariate.
In other sensitivity analyses that used clinically relevant cutpoints for LDL-C instead of LDL-C thirds, similar results were obtained.
Extreme Elevation of HDL-C and Incident Events
Finally, among non-hormone users (to examine naturally-occurring elevations), we stratified participants according to deciles of HDL-C or apolipoprotein A-1. There were inverse associations with coronary events that appeared to plateau above an HDL-C concentration of approximately 1.48 mmol/L (57 mg/dL, Appendix Figure). Compared with women in the bottom decile, women in the top decile of HDL-C (≥1.80 mmol/L, 69.6 mg/dL) or apolipoprotein A-1 (≥170.9 mg/dL) had age-adjusted HRs for coronary events of 0.21 (CI, 0.13–0.35) and 0.28 (CI, 0.18–0.45), respectively. These were only modestly attenuated after fully adjusting for LDL-C and the model 2 covariates (HRs 0.32, CI, 0.16–0.63, and 0.45, CI, 0.24–0.85).
Appendix Figure.
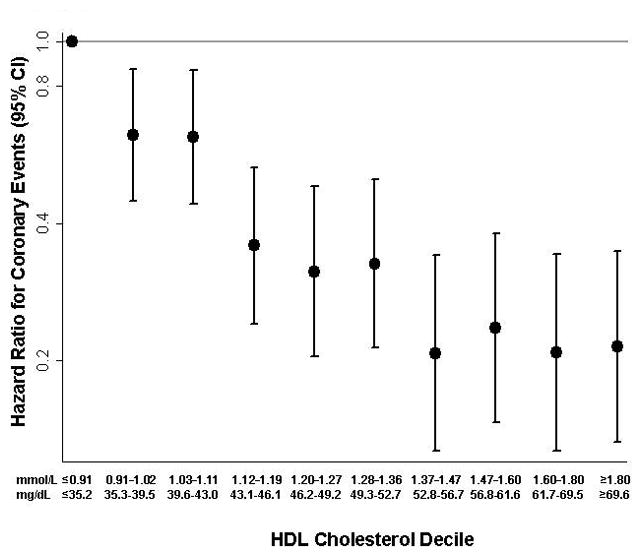
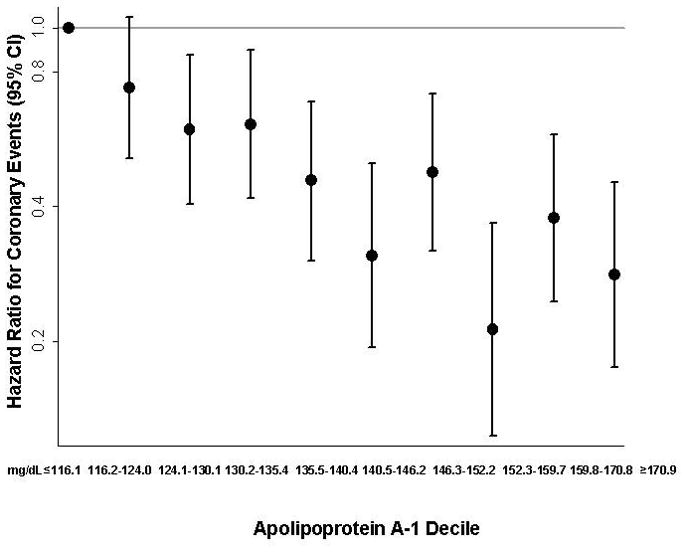
Coronary event age-adjusted hazard ratios (95% CIs) for deciles of HDL cholesterol and apolipoprotein A-1. The bottom decile is the reference group.
Women in the top decile of HDL-C experienced first events at older ages compared with women in the bottom decile (mean [SD] age of onset of first coronary event 70.3 [9.4] versus 63.8 [7.7] years, respectively; and age of onset of first CVD event 72.2 [8.8] versus 64.2 [8.3] years, respectively). Women who were in the top decile of HDL-C yet developed CVD were not only older but were more likely to have hypertension (48.7% vs 17.0%), diabetes (8.1% vs 1.1%), and higher concentrations of LDL-C (median 3.81 mmol/L [147 mg/dL] vs 3.06 mmol/L [118 mg/dL]) and triglycerides (median 0.97 mmol/L [86 mg/dL] vs 0.84 mmol/L [74 mg/dL]).
Lastly, the inverse association with coronary disease persisted among women with HDL-C ≥ 2.07 mmol/L (80 mg/dL; approximately the top 3% of women), with an age-adjusted HR of 0.20 (CI, 0.09–0.43) compared with women in the bottom decile. Similarly for women with the top 3% of apolipoprotein A-1 (≥185 mg/dL), the age-adjusted HR was 0.35 (CI, 0.18–0.66).
Discussion
In this prospective study of apparently healthy middle-aged women, baseline HDL-C was consistently and inversely associated with incident coronary and CVD events independent of other risk factors, while apolipoprotein A-1 showed weaker associations. Consistent inverse associations were found for HDL-C across a range of LDL-C, including among women with low LDL-C. Among women with decreased total atherogenic particle burden (as measured by apolipoprotein B100 <90 mg/dL), few events occurred and no associations were seen for either HDL-C or apolipoprotein A-1. Finally, neither HDL-C nor apolipoprotein A-1 was associated with stroke in multivariable analyses.
Beginning at puberty and continuing throughout their lifetime, women typically have higher HDL-C and apolipoprotein A-1 concentrations than men (17). The current study adds to the prior literature in finding statistically significant inverse association for HDL-C with coronary events (but not stroke) among women with different levels of LDL-C, including those with naturally occurring low LDL-C. The Framingham study was the first to report on the inverse association of HDL-C with coronary events, with each 1% risk in HDL-C associated with approximately 2% decline in coronary events (3,4). Among men, this inverse association was consistent across a range of LDL-C including men with low LDL-C (4), but the results were not reported by levels of LDL-C among women in the Framingham study. Subsequent studies confirmed the findings in men (6,10,18) but did not include women.
Although the data in women examining HDL-C associations with CVD across levels of LDL-C are scarce, one previous study from the Lipid Research Clinics, a study population enriched with lipoprotein abnormalities, found that the inverse association for HDL-C >1.30 mmol/L (50 mg/dL) with CVD mortality persisted in women with LDL-C <3.37 mmol/L (130 mg/dL) (11). In that study, which only had CVD mortality outcomes, HDL-C was not examined at lower LDL-C cut-points nor were comparison data for apolipoproteins available. Our study extends the results of prior studies by 1) analyzing the associations at a range of concentrations, including at lower levels of LDL-C among apparently healthy women, 2) including a detailed analysis of apolipoproteins A-1 and B100, and 3) examining coronary and stroke outcomes separately.
Less is known regarding apolipoprotein A-1 and CVD in individuals with naturally low LDL-C or apolipoprotein B100 (19). In a meta-analysis of 21 studies, apolipoprotein A-1 was inversely associated with CVD, with approximately 60% higher risk for the bottom tertile (20). We found that the inverse association of apolipoprotein A-1 with CVD in women became attenuated and no longer statistically significant when LDL-C was low. By comparison, the association of HDL-C remained statistically significant.
We can only speculate as to why HDL-C lost its association with CVD at lower concentrations of total atherogenic particles as measured by low apolipoprotein B100 concentrations. The number of coronary events among women with LDL-C <2.80 mmol/L (108 mg/dL) was lower than among women with apolipoprotein B100 <90 mg/dL (117 versus 78, respectively). Compared with LDL-C, apolipoprotein B100 is more closely related to insulin resistance and other features of the metabolic syndrome (21), such that the predictive value may be lower for HDL-C, a key component of insulin resistance and metabolic syndrome, when apolipoprotein B100 levels are already naturally low. It is also possible that HDL-C, which is essential for reverse cholesterol transport to the liver, is more “cardioprotective” in the presence of increased concentrations of total atherogenic particles.
Finally, we found that women with very high HDL-C concentrations were not immune to experiencing CVD. But, compared with women who had low HDL-C, they were at lower risk of incident CVD and experienced first CVD events at older ages. In contrast to a prior study that found increased risk of CVD when HDL-C was greater than 2.07 mmol/L (80 mg/dL) (22), we found reduced risk at the highest levels of HDL-C in these healthy women. Further, women with very high HDL-C who experienced events had concomitantly higher prevalence of other risk factors that may have overriden the beneficial effects of a high HDL-C. HDL-C can be raised naturally (by as much as 20% to 30%) through non-pharmacological modifications that include weight loss, aerobic exercise, tobacco cessation, and healthy dietary choices (23). Compared with men, women may sustain even greater HDL-C increases by participating in regular exercise programs for extended periods of time (24). While current guidelines are inconsistent as to whether HDL-C should be a primary, secondary, or tertiary target of therapy, they all recommend adoption of healthier lifestyle when HDL-C is low (1,25,26).
Limitations
It is unclear if the present findings in this population of low-risk primary prevention women would be applicable to higher-risk individuals such as those in secondary prevention settings or taking lipid lowering therapy. Fewer events occurred among those in the lowest apolipoprotein B100 stratum, and we cannot exclude that HDL-C would be inversely associated with CVD in women with low apolipoprotein B100 if there were more events. Only a single measurement of the lipids and lipoproteins was available at baseline, such that we were unable to examine the value of repeated measurements of these biomarkers. Our study population was limited to healthcare professionals who were mostly white. We can not rule out unmeasurable or residual confounding due to measurement error in the model variables or due to unmeasured variables.
Strengths
Strengths of our study include the reliable measurement of HDL-C, LDL-C, and apolipoproteins with high accuracy in a core laboratory. We had well-characterized risk factor profile of the participants allowing us to control for potential confounding for both lipid and non-lipid variables. The study also benefited from the large sample size, long duration of follow-up, and the ascertainment of coronary, stroke, and total incident CVD events.
Conclusion
In this prospective study of women, baseline concentrations of HDL-C and apolipoprotein A-1 were associated with incident coronary and CVD events independent of other risk factors. By contrast, there were no associations in relation to stroke after adjusting for other risk factors. Consistent inverse associations were found for HDL-C with CVD across a range of LDL-C, including low LDL-C. Among women with low total atherogenic particle burden (apolipoprotein B100<90 mg/dL), few events occurred and no associations were seen for HDL-C or apolipoprotein A-1.
Acknowledgments
Potential Financial Conflict of Interest
The research for this article was supported by an investigator-initiated research grant to Dr. Mora from Merck. Dr Cui is an employee of Merck.
Grant Support: The research for this article was supported by an investigator-initiated research grants to Dr. Mora from Merck. The study was additionally supported by grants K08 HL094375 (to Dr. Mora) and HL 43851, HL 080467 and CA 47988 from the National Heart, Lung, and Blood Institute and the National Cancer Institute.
Primary Funding Sources: Merck; National Heart, Lung and Blood Institute National Institute and the National Cancer Institute of the National Institutes of Health.
References
- 1.Third Report of the National Cholesterol Education Program (NCEP) Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults (Adult Treatment Panel III) final report. Circulation. 2002;106:3143–421. [PubMed] [Google Scholar]
- 2.Walldius G, Jungner I. The apoB/apoA-I ratio: A strong, new risk factor for cardiovascular disease and a target for lipid-lowering therapy--a review of the evidence. J Intern Med. 2006;259:493–519. doi: 10.1111/j.1365-2796.2006.01643.x. [DOI] [PubMed] [Google Scholar]
- 3.Gordon T, Castelli WP, Hjortland MC, Kannel WB, Dawber TR. High density lipoprotein as a protective factor against coronary heart disease. The Framingham Study. Am J Med. 1977;62:707–714. doi: 10.1016/0002-9343(77)90874-9. [DOI] [PubMed] [Google Scholar]
- 4.Castelli WP. Cholesterol and lipids in the risk of coronary artery disease--the Framingham Heart Study. Can J Cardiol. 1988;4 (Suppl A):5A–10A. [PubMed] [Google Scholar]
- 5.Schaefer EJ, Lamon-Fava S, Cohn SD, Schaefer MM, Ordovas JM, Castelli WP, et al. Effects of age, gender, and menopausal status on plasma low density lipoprotein cholesterol and apolipoprotein B levels in the Framingham Offspring Study. J Lipid Res. 1994;35:779–92. [PubMed] [Google Scholar]
- 6.Assmann G, Schulte H, von Eckardstein A, Huang Y. High-density lipoprotein cholesterol as a predictor of coronary heart disease risk. The PROCAM experience and pathophysiological implications for reverse cholesterol transport. Atherosclerosis. 1996;124 (Suppl):S11–20. doi: 10.1016/0021-9150(96)05852-2. [DOI] [PubMed] [Google Scholar]
- 7.Sharrett AR, Ballantyne CM, Coady SA, Heiss G, Sorlie PD, Catellier D, et al. Coronary heart disease prediction from lipoprotein cholesterol levels, triglycerides, lipoprotein(a), apolipoproteins A-I and B, and HDL density subfractions: The Atherosclerosis Risk in Communities (ARIC) study. Circulation. 2001;104:1108–13. doi: 10.1161/hc3501.095214. [DOI] [PubMed] [Google Scholar]
- 8.Luc G, Bard JM, Ferrieres J, Evans A, Amouyel P, Arveiler D, et al. Value of HDL cholesterol, apolipoprotein A-I, lipoprotein A-I, and lipoprotein A-I/A-II in prediction of coronary heart disease: The PRIME Study. Prospective epidemiological study of myocardial infarction. Arterioscler Thromb Vasc Biol. 2002;22:1155–61. doi: 10.1161/01.atv.0000022850.59845.e0. [DOI] [PubMed] [Google Scholar]
- 9.Di Angelantonio E, Sarwar N, Perry P, Kaptoge S, Ray KK, Thompson A, et al. Major lipids, apolipoproteins, and risk of vascular disease. JAMA. 2009;302:1993–2000. doi: 10.1001/jama.2009.1619. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.deGoma EM, Leeper NJ, Heidenreich PA. Clinical significance of high-density lipoprotein cholesterol in patients with low low-density lipoprotein cholesterol. J Am Coll Cardiol. 2008;51:49–55. doi: 10.1016/j.jacc.2007.07.086. [DOI] [PubMed] [Google Scholar]
- 11.Bass KM, Newschaffer CJ, Klag MJ, Bush TL. Plasma lipoprotein levels as predictors of cardiovascular death in women. Arch Intern Med. 1993;153:2209–16. [PubMed] [Google Scholar]
- 12.Cook NR, Lee IM, Gaziano JM, Gordon D, Ridker PM, Manson JE, et al. Low-dose aspirin in the primary prevention of cancer: The Women’s Health Study: A randomized controlled trial. JAMA. 2005;294:47–55. doi: 10.1001/jama.294.1.47. [DOI] [PubMed] [Google Scholar]
- 13.Lee IM, Cook NR, Gaziano JM, Gordon D, Ridker PM, Manson JE, et al. Vitamin E in the primary prevention of cardiovascular disease and cancer: The Women’s Health Study: A randomized controlled trial. JAMA. 2005;294:56–65. doi: 10.1001/jama.294.1.56. [DOI] [PubMed] [Google Scholar]
- 14.Ridker PM, Cook NR, Lee IM, Gordon D, Gaziano JM, Manson JE, et al. A randomized trial of low-dose aspirin in the primary prevention of cardiovascular disease in women. N Engl J Med. 2005;352:1293–304. doi: 10.1056/NEJMoa050613. [DOI] [PubMed] [Google Scholar]
- 15.Hainline A, Karon J, Lippel K. Manual of Laboratory Operations: Lipid Research Clinics Program and Lipid and Lipoprotein Analysis. Bethesda, Md: U.S. Dept of Health and Human Services; 1982. p. 628. [Google Scholar]
- 16.Rosenbaum PR. Discussing hidden bias in observational studies. Ann Intern Med. 1991;115:901–5. doi: 10.7326/0003-4819-115-11-901. [DOI] [PubMed] [Google Scholar]
- 17.Bittner V. Perspectives on dyslipidemia and coronary heart disease in women. J Am Coll Cardiol. 2005;46:1628–35. doi: 10.1016/j.jacc.2005.05.089. [DOI] [PubMed] [Google Scholar]
- 18.Pischon T, Girman CJ, Sacks FM, Rifai N, Stampfer MJ, Rimm EB. Non-high-density lipoprotein cholesterol and apolipoprotein B in the prediction of coronary heart disease in men. Circulation. 2005;112:3375–83. doi: 10.1161/CIRCULATIONAHA.104.532499. [DOI] [PubMed] [Google Scholar]
- 19.Barter PJ, Ballantyne CM, Carmena R, Castro Cabezas M, Chapman MJ, Couture P, et al. Apo B versus cholesterol in estimating cardiovascular risk and in guiding therapy: Report of the thirty-person/ten-country panel. J Intern Med. 2006;259:247–58. doi: 10.1111/j.1365-2796.2006.01616.x. [DOI] [PubMed] [Google Scholar]
- 20.Thompson A, Danesh J. Associations between apolipoprotein B, apolipoprotein AI, the apolipoprotein B/AI ratio and coronary heart disease: A literature-based meta-analysis of prospective studies. J Intern Med. 2006;259:481–92. doi: 10.1111/j.1365-2796.2006.01644.x. [DOI] [PubMed] [Google Scholar]
- 21.Sniderman AD. Apolipoprotein B versus non-high-density lipoprotein cholesterol: And the winner is. Circulation. 2005;112:3366–7. doi: 10.1161/CIRCULATIONAHA.105.583336. [DOI] [PubMed] [Google Scholar]
- 22.van der Steeg WA, Holme I, Boekholdt SM, Larsen ML, Lindahl C, Stroes ES, et al. High-density lipoprotein cholesterol, high-density lipoprotein particle size, and apolipoprotein A-I: Significance for cardiovascular risk: The IDEAL and EPIC-Norfolk studies. J Am Coll Cardiol. 2008;51:634–42. doi: 10.1016/j.jacc.2007.09.060. [DOI] [PubMed] [Google Scholar]
- 23.Singh IM, Shishehbor MH, Ansell BJ. High-density lipoprotein as a therapeutic target: A systematic review. JAMA. 2007;298:786–98. doi: 10.1001/jama.298.7.786. [DOI] [PubMed] [Google Scholar]
- 24.Warner JG, Jr, Brubaker PH, Zhu Y, Morgan TM, Ribisl PM, Miller HS, et al. Long-term (5-year) changes in HDL cholesterol in cardiac rehabilitation patients. Do sex differences exist? Circulation. 1995;92:773–7. doi: 10.1161/01.cir.92.4.773. [DOI] [PubMed] [Google Scholar]
- 25.Haffner SM. Dyslipidemia management in adults with diabetes. Diabetes Care. 2004;27 (Suppl 1):S68–71. doi: 10.2337/diacare.27.2007.s68. [DOI] [PubMed] [Google Scholar]
- 26.Grundy SM, Cleeman JI, Daniels SR, Donato KA, Eckel RH, Franklin BA, et al. Diagnosis and management of the metabolic syndrome: An American Heart Association/National Heart, Lung, and Blood Institute Scientific Statement. Circulation. 2005;112:2735–52. doi: 10.1161/CIRCULATIONAHA.105.169404. [DOI] [PubMed] [Google Scholar]