

Abstract
INTRODUCTION
Sclerosing Angiomatoid Nodular Transformation of the spleen (SANT) is a rare benign vascular lesion of the spleen with extensive sclerosis and unknown etiology.
PRESENTATION OF CASE
We report a new case of SANT of the spleen found in a 53-year-old female following detection of a splenic mass on a routine computed tomography (CT). The patient underwent an uncomplicated laparoscopic splenectomy and the specimen was sent for histopathologic examination.
DISCUSSION
A review of the 97 reported cases of SANT found in the literature was undertaken. There were 43 males and 54 females with a median age of 46 years (range: 11–82 years). SANT is classically considered to be a female predominant disease, however 44.3% of reported case were male and the gender predilection may soon be neutralized as more cases are reported. 65 of the 97 (67%) patients were in 30–60 year age group. The majority of lesions (n = 50) were incidentally found on imaging, and for those patients presenting with symptoms, abdominal pain (n = 18) was the predominant symptom.
CONCLUSION
The diagnosis of SANT should be considered in any patient presenting with a splenic lesion that contains an angiomatoid or inflammatory component. As the differential diagnosis for SANT includes malignant pathologies, and currently no reliable diagnostic radiological feature has been identified to differentiate between these conditions, SANT will continue to be diagnosed on the basis of surgical histopathology.
Keywords: Spleen, Splenectomy
1. Introduction
Sclerosing Angiomatoid Nodular Transformation (SANT) of the spleen is a rare benign vascular lesion with extensive sclerosis first described by Martel and colleagues in 2004.1 In this paper we report a case of SANT of the spleen managed at our institution, and present a review of 97 other cases found in the literature.
2. Presentation of case
A 53 year old Caucasian female was referred to our department in consideration of splenectomy. She had been under the care of the hematology department following the detection of a splenic mass on a routine computed tomography (CT) scan performed for chronic back pain (Fig. 1). An ultrasound scan at that time demonstrated a 3.6 × 3.5 × 3.5 cm hypoechoic splenic density, and a magnetic resonance imaging (MRI) scan (Fig. 2) confirmed the mass within the inferior spleen demonstrating diffuse heterogeneous enhancement. At this time the differential diagnosis included Gaucher's disease, sarcoid or a low-grade lymphoma. Bone marrow biopsy, flow cytometry, chromosome analysis and angiotension converting enzyme levels were normal, and the above differential diagnoses ruled out.
Fig. 1.

Computed tomography (CT) scan showing the splenic lesion at the medial aspect of the lower spleen.
Fig. 2.
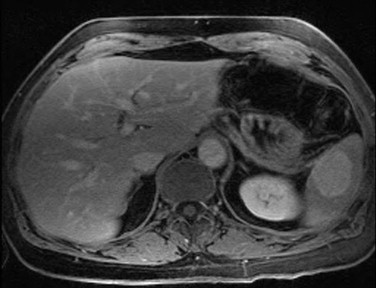
Magnetic resonance imaging (MRI) showing the lesion in the lower spleen.
Over a three year period the splenic mass increased in diameter to 5.9 cm and the referring hematologist was concerned for the possibility of an underlying malignancy. The patient remained asymptomatic and her examination benign, with no evidence of hepatosplenomegaly. The decision was made to proceed with an operation and the patient underwent a laparoscopic splenectomy.
2.1. Intraoperative findings
On entering the abdominal cavity significant adhesions were encountered in the region of the inferiolateral aspect of the spleen where the mass was clearly visible. When the spleen was placed into a bag for morcellation prior to extraction, it was noted that the mass was significantly harder than the rest of the spleen. As a result the surrounding normal splenic tissue was morcellated until only the mass was remaining, and this was then removed in its entirety and sent for histopathological examination.
2.2. Pathologic findings
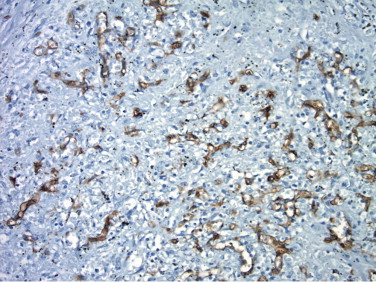
The splenic mass was composed of mutiple nodules of small vessels surrounded by sclerotic tissue and a scattered lymphoplasmacytic infiltrate. Immunohistochemical staining of the small vessels within the lesion were positive for CD34, CD31, CD68 and CD163, and negative for CD8 (Figs. 3–7). The histologic sections and immunohistochemical staining performed on the splenic lesion confirmed the diagnosis of SANT of the spleen.
Fig. 3.

The splenic parenchyma is replaced by innumerable well-circumscribed angiomatoid nodules separated by a fibrosclerotic and inflammatory stroma. The nodules are composed of a variety of cell types including capillaries, sinusoid-like spaces, and mononuclear inflammatory cells. Red blood cells are abundant.
Fig. 4.

CD31 immunostain highlights the abundant vascular structures (capillaries, sinusoid-like spaces, and veins) along with numerous single cells within the nodules, generating a complex network of CD31 immunoreactive cells.
Fig. 5.
CD34 immunostain highlights the capillaries, but not sinusoid-like spaces or any single cells.
Fig. 6.

CD8 immunostain highlights occasional sinusoid-like spaces (lower right) and scattered inflammatory cells, but is absent in other vascular structures (capillaries and veins).
Fig. 7.

CD68 immunostain highlights scattered single cells (presumably histiocytes) but no vessel-lining cells.
3. Discussion
The term SANT first appeared in the literature in a 2004 paper by Martel et al. which examined a series of 25 cases.1 This relatively uncommon splenic lesion had however been recognized earlier by other authors under different names such as splenic hamartoma, cord capillary hemangioma, and multinodular hemangioma.2 SANTs are benign, nodular vascular proliferations of splenic red pulp with considerable sclerosis.1,26 It usually affects middle-aged adults, and it is commonly found incidentally on radiographic imaging, or at the time of operation for an unrelated condition.20
Review of the existing literature revealed 97 patients consisting of 43 males and 54 females with a median age of 46 years (range: 11–82 years). SANT is considered to be a female predominant disease,26 however 43 of the 97 cases (44.3%) reported in the literature to date were male and the gender predilection may soon be neutralized as more cases are reported. 65 out of the 97 (67%) patients were in 30–60 year age group, so it appears that SANT predominantly affects adults in the fourth to seventh decades of life. The majority of lesions (n = 50) were incidentally found on imaging, and for those patients presenting with symptoms, abdominal pain (n = 18) was the predominant symptom. Other presentations included: a palpable left upper quadrant mass; cytopenias; flank pain; pelvic pain; and long-standing fever.
The weight of resected spleens in the literature exhibited significant variation from 68 to 2720 g. The typical macroscopic appearance of a SANT lesion was of a well-circumscribed non-encapsualted, bosselated mass with multiple dark brown nodules (hemorrhagic regions in angiomatoid nodules) interspersed with stellate whitish fibrotic stroma.1,26,27 The cases reported before 2008 had varying diagnoses that included hamartoma, inflammatory pseudotumor, hemangioma, angisarcoma, metastatic tumor, bacillary angiomatosis, but thereafter SANT has been the referring diagnosis.
There is minimal data available on the follow-up of patients with SANT. There are two reported deaths in the 25 cases published by Martel et al.1; a 56-year-old female who died of disseminated lung adenocarcinoma, and the other a 46-year-old male with concurrent bronchogenic squamous cell carcinoma who died of sepsis post-splenectomy. There is no data regarding the immunization status and use of antibiotic prophylaxis in these patients (Table 1).
Table 1.
Published SANT cases.
| Author | Age | Gender | Clinical features | Spleen weight | Gross features | Follow-up | Referring dx | Concurrent disease | |
|---|---|---|---|---|---|---|---|---|---|
| 1 | Martel1 N = 25 |
50 | Female | Incidental finding at laparotomy | 329 g | – | NED, 9 years | – | |
| 2 | 32 | Female | Incidental radiographic finding | 139 g | 5 cm mass with white fibrous bands | NED, 8 years | Hamartoma | ||
| 3 | 57 | Male | Incidental radiographic finding | – | 3.7 cm fibrotic mass | NED, 6 years | Hemangioma vs. angiosarcoma | ||
| 4 | 58 | Female | Incidental radiographic finding | 456 g | 9 cm firm mass | NED, 5 years | Hemangioma vs. IPT | ||
| 5 | 35 | Female | Pancytopenia, raised ESR | – | 8 cm well-circumscribed mass | NED, 4 years | Hemangioma | ||
| 6 | 71 | Female | Incidental radiographic finding | 704 g | 13.5 cm well-circumscribed fibrotic mass | NED, 4 years | Hemangioma vs. IPT | ||
| 7 | 23 | Male | 280 g | 7 cm well-circumscribed fibrotic mass | NED, 3 years | – | |||
| 8 | 59 | Female | Incidental finding at laparotomy | 130 g | 4 cm fibrotic mass | NED, 4 years | Angiosarcoma vs. IPT | ||
| 9 | 37 | Female | Abdominal pain | 280 g | 6 cm mass | NED, 1 year | Hemangioma vs. littoral cell angioma | ||
| 10 | 29 | Male | Abdominal pain | – | 10 cm mass | NED, 2 years | Hemangioma vs. IPT | ||
| 11 | 60 | Female | – | 1400 g | 12 cm mass | NED, 10 m | – | ||
| 12 | 74 | Male | Incidental finding at laparotomy | 160 g | 3 cm well-circumscribed multilobulated mass | NED, 6 m | Hemangioma | Renal cell carcinoma | |
| 13 | 57 | Female | Incidental finding at laparotomy | 173 g | 8 cm mass | NED, 6 m | Vascular tumor | ||
| 14 | 61 | Female | Splenomegaly | 68 g | 3.5 × 3.5 cm sharply demarcated, gray-white to red-purple mass | – | – | ||
| 15 | 56 | Female | Abdominal discomfort, anemia | 189 g | 5.5 cm well-circumscribed mass with red-brown nodules traversed by stellate fibrous bands | NED. Died of lung ca | IPT | ||
| 16 | 46 | Male | Hx of anemia and lung SCC. Presented with fever and splenomegaly | – | – | Died of sepsis post splenectomy | Bacillary angiomatosis vs. Kaposi sarcoma | ||
| 17 | 68 | Female | Carcinoma of colon 8 m prior with post-op chemo. Incidental finding | 285 g | 4.5 cm bosselated whitish mass surrounded by brown nodules | NED, 7 years | Benign Kaposi-like vascular tumor vs. bacillary angiomatosis vs. chemo-related changes | ||
| 18 | 63 | Male | RUQ pain. Incidental finding | 93 g | 4 cm mass | NED, 3 years | – | Early gastric carcinoma | |
| 19 | 56 | Male | Incidental finding | – | 10 cm circumscribed whitish mass with focal hemorrhage | – | IPT | ||
| 20 | 25 | Female | LUQ mass | 335 g | 8.5 × 6 × 5 cm circumscribed, grayish mass | NED, 3 years | IPT vs. sclerosedhemangioma vs. Castleman disease | ||
| 21 | 45 | Male | Incidental finding | 322 g | circumscribed firm, gray-white nodule with brown patches | NED, 3 yearss | Hemangioendothelioma vs. IPT | ||
| 22 | 43 | Female | Incidental finding | 250 g | – | NED, 2 m | N/A | ||
| 23 | 35 | Female | LUQ pain for 6 months | 240 g | 3.1 × 2.5 cm subcapsular mass, pale, sclerotic in center and brown-red at periphery | – | Hemangioepithelioma vs. Kaposi sarcoma | ||
| 24 | 23 | Female | Palpable mass | 1425 g | 17 × 11 cm irregular fibrous mass with thick capsule | NED, 1 year | Sclerosedhemangioma vs. hamartoma | von Willebrand disease | |
| 25 | 57 | Female | 105 g | 3.5 × 3.4 × 3.2 cm mass with multiple dark red nodules | NED, 18 m | Hemangioma | |||
| 26 | Li3 N = 1 |
59 | Male | Incidental finding on CT during workup for renal problems | 283 g | 3.3 × 3.3 cm firm yellow mass | HTN, DM, hypothyroidism, BPH | ||
| 27 | J.-C. Lee10 N = 1 |
43 | Female | Weight loss and left flank pain | 180 g | 3.5 × 3.5 × 3.0 cm and 3.0 × 2.0 × 2.0 cm Hemorrhagic nodules | Thrombosedhemangioma, lymphoma, chronic abscess | Hepatitis B+ | |
| 28 | D. Lee4 N = 1 |
58 | Male | Incidental finding on U/S. Deranged LFTs | 205 g | 8.7 × 6.5 × 5.5 cm | Metastatic melanoma to spleen | Previous malignant melanoma | |
| 29 | Weinreb5 N = 6 |
58 | Female | Lung Ca staging CT | 110 g | 1.9 cm | NED, 1 year | SANT | |
| 30 | 65 | Male | 320 g | 6.5 cm | Lost to f/u | Hamartoma | |||
| 31 | 73 | Female | Hypertension, hyperlipidemia, remote lung abscess, chronic cough | 324 g | 6.0 cm | NED, 16 m | Hemangioendothelioma | ||
| 32 | 51 | Male | Anemia | 2720 g | 12.0 cm | NED, 5 m | IPT | ||
| 33 | 41 | Female | Enlarging mass on serial U/S | 256 g | 6.5 cm | NED, 1 m | SANT | ||
| 34 | 59 | Female | Multiple splenic lesions 20 years post Whipple for periampullary Ca | – | 2.1 cm | NED, 1 year | IPT | ||
| 35 | Diebold11 N = 16 |
56 | Female | 2400 g | 3 nodules 1.0, 2.0 and 3.0 cm | Idiopathic myelofibrosis | |||
| 36 | 22 | Female | 220 g | 5.5 × 3.0 cm multinodular | Acute pyelonephritis | ||||
| 37 | 37 | Female | 590 g | 10.0 × 7.0 cm multinodular | |||||
| 38 | 33 | Female | Hypochromic anemia | 1760 g | multinodular | ||||
| 39 | 60 | Female | 430 g | 10.0 cm multinodular | |||||
| 40 | 44 | Male | Longstanding fever | 610 g | 15.0 cm multinodular | ||||
| 41 | 24 | Female | Hypochondral pain | 160 g | 5.0 cm multinodular | ||||
| 42 | Male | Gastric ulcer | 218 g | 1.0 cm | |||||
| 43 | 31 | Female | 180 g | 7.0 cm multinodular | |||||
| 44 | 46 | Male | Thrombocytopenia | 137 g | 4.0 cm multinodular | ||||
| 45 | 82 | Male | – | 2.0 cm multinodular | Colon carcinoma with mets to splenic hilum | ||||
| 46 | 53 | Male | 190 g | 5.0 cm multinodular | |||||
| 47 | 63 | Female | Fever, night sweats | 140 g | 1.5 × 1.0 × 1.0 cm multinodular | ||||
| 48 | 55 | Male | Anemia | 550 g | 8.0 cm multinodular | ||||
| 49 | 62 | Female | Abdominal pain | 4.0 cm multinodular | |||||
| 50 | 50 | Male | Anemia | 840 g | 9.0 cm multinodular | ||||
| 51 | El Demellawy12 N = 1 |
58 | Female | Incidental finding. Hx of RUL non-small cell carcinoma stage III | 110 g | 1.9 cm well-circumscribed but non-encapsulated nodule. Bosselated contour and whitish, firm, solid surface | Metastatic lung cancer | ||
| 52 | Karaosmanoglu13 N = 1 |
44 | Male | Vague pelvic pain | 650 g | Whitish firm nodule with hemorrhagic spiculations | |||
| 53 | Zeeb14 N = 1 |
36 | Female | LUQ Pain for 2 weeks | Multiple red-brown nodules with a prominent stellate scar | ||||
| 54 | Teng15 N = 1 |
37 | Female | Incidental finding with hepatolitiasis | 1080 g | 8.5 × 8.5 cm | |||
| 55 | 31 | Male | Incidental finding | 780 g | 8.0 × 8.0 cm | ||||
| 56 | 58 | Female | Flank/back pain for 1 month | 528 g | 6.5 × 4.5 cm | ||||
| 57 | 31 | Female | Upper abdominal discomfort × 2 years | 2106 g | 8.5 × 8.5 cm | SANT | |||
| 58 | 37 | Male | Incidental finding | 297 g | 3.0 × 3.0 cm | SANT | |||
| 59 | 37 | Male | Incidental finding | 473 g | 3.5 × 3.0 cm | SANT | |||
| 60 | 50 | Female | Incidental finding with hepatic angioma | 314 g | 2.6 × 2.4 cm | SANT | |||
| 61 | Kashiwagi16 N = 9 |
31 | Female | Incidental Finding | 230 g | 5.5 cm | – | IPT | |
| 62 | 34 | Male | Back discomfort | – | 7.0 cm | NED, 3 m | IPT | ||
| 63 | 37 | Male | Epigastric pain | 80 g | 3.0 cm | NED, 79 m | IPT | ||
| 64 | 44 | Female | Incidental Finding | – | 3.5 cm | NED, 25 m | SANT | Cholelithiasis | |
| 65 | 46 | Male | Incidental Finding | 110 g | 6.5 cm | – | IPT | Chronic hepatitis | |
| 66 | 50 | Male | Incidental Finding | 500 g | 11.0 cm | – | IPT | ||
| 67 | 60 | Male | Incidental Finding | 100 g | 2.5 cm | NED, 37 m | SANT | Gastric cancer | |
| 68 | 65 | Female | Incidental Finding | – | 5.1 cm | – | IPT | Cholelithiasis | |
| 69 | 72 | Female | Incidental Finding | – | 2.0 cm | NED, 113 m | IPT | Colon cancer | |
| 70 | Gutzeit17 N = 1 |
77 | Male | Incidental finding on CT. Patient had prostate cancer | 8 × 6 cm | Hamartoma | |||
| 71 | Koreishi6 N = 3 |
58 | Female | Abdominal pain | 307 g | 4.4 cm in inferior pole | NED; Alive | DM, hypothyroidism | |
| 72 | 72 | Female | Incidental finding or annual CT scan | 79 g | 2.3 cm | NED; Alive | Hx of high-grade urothelial carcinoma of renal pelvis and low-grade urothelial carcinoma of bladder | ||
| 73 | 64 | Female | Incidental finding on routine CT scan | 110 g | 2.1 cm | NED; Alive | Hx of carcinoma of fallopian tube, malignant melanoma in situ | ||
| 74 | Langer18 N = 1 |
44 | Male | Incidental finding on routine CT scan | 170 g | 2.0 cm mass; encapsulated reddish nodular | NED 4 m; Alive | Metastatic rectal cancer | |
| 75 | Chikkappa19 N = 1 |
40 | Female | Intermittent LUQ pain | 168 g | 4.7 × 4.0 × 6.5 cm peripheral circumscribed nodule, which was partly fibrous and partly nodular hemorrhagic | SANT | ||
| 76 | Thacker20 N = 1 |
80 | Male | Incidental radiographic finding | – | Granular and gray-purple with a lobulated 9 cm mass with hemorrhagic areas measuring 0.1–0.5 cm | SANT | MDS, Melanoma, Basal cell carcinoma and squamous cell carcinoma | |
| 77 | Kuybulu21 N = 1 |
11 | Female | Incidental finding on physical examination | Well circumscribed confluent vascular/angiomatoic nodules with mixed-type inflammatory cells | NED, 1 year | SANT | Short stature | |
| 78 | Kuo22 N = 10 |
32 | Female | Left flank soreness for 2 weeks | 139 g | Single 3 × 4 × 5 cm nodule | NED, 94 m | SANT | |
| 79 | 53 | Female | Diffuse abdominal pain | – | Single 3 × 3 cm nodule | NED, 166 m | SANT | ||
| 80 | 57 | Female | Incidental finding | 105 g | Single 3.5 × 3.4 × 3.2 cm nodule | – | SANT | ||
| 81 | 37 | Male | Incidental finding | 275 g | Single 6 × 6 cm nodule | – | SANT | ||
| 82 | 46 | Female | RUQ pain for 2 months | 104 g | Single 2.2 × 2 × 2 cm nodule | – | SANT | ||
| 83 | 39 | Male | Incidental finding | 278 g | Multinodular | NED, 14 m | SANT | ||
| 84 | 31 | Male | Right inguinal mass and Incidental radiographic finding | 654 g | Multinodular | NED, 6 m | SANT | ||
| 85 | 57 | Male | Left upper abdominal pain for 2 years | 142.5 g | Multinodular | – | SANT | ||
| 86 | 33 | Female | LUQ Pain for 1 year | 143.6 g | Single 5.2 × 5 × 4 cm | NED, 2 m | SANT | ||
| 87 | 44 | Male | Incidental finding | 212.6 g | Single 6.8 × 6 × 4.5 cm | NED, 1 m | SANT | ||
| 88 | Cao23 N = 3 |
36 | Male | Incidental radiographic finding | – | Mass was found to have an integrated envelope and a heterogenous cut surface | SANT | ||
| 89 | 37 | Female | Pain in the LUQ | – | Firm mass with a clear margin | SANT | |||
| 90 | 39 | Male | LUQ mass | – | – | SANT | |||
| 91 | Sitaraman24 N = 1 |
65 | Male | Incidental radiographic finding | 750 g | 2 cm well-circumscribed nodule with an area of central fibrosis | SANT | Retroperitoneal spindle cell sarcoma | |
| 92 | Subhawong25 N = 1 |
27 | Female | RUQ pain after motor vehicle crash | 474 g | 10.2 cm firm, white, nodular lesion infiltrating red irregularly | SANT | Unexplained anemia with history of transfusion | |
| 93 | Bamboat26 N = 1 |
17 | Male | Abdominal pain for 6 months | Lobulated 4 cm fibrotic mass with hemorrhagic areas | NED, 7 m | SANT | ||
| 94 | Raman27 N = 1 |
50 | Male | LUQ pain for 4 months | |||||
| 95 | Ki-Han28 N = 1 |
23 | Female | Incidental radiographic finding | – | 5.2 × 4.5 cm dark brown mass with a central large stellate fibrotic scar | SANT | ||
| 96 | Onder29 N = 1 |
48 | Male | Pelvic pain | 650 g | 8 cm solitary non-encapsulated mass composed of multiple nodules with wide area of hemorrhage and a central stellate scar | SANT | ||
| 97 | Vyas30 N = 1 |
11 | Male | Left flank pain since 2 months | 125 g | 5 × 4 × 4 cm well-circumscribed unencapsulated lesion with bulging cut surface and central fibrotic scar | NED, 3 years | SANT |
There is currently no pathognomonic finding for the diagnosis of SANT on cross-sectional imaging, however, the literature suggests that the diagnosis can be made if a contrast-enhanced MRI shows a “spoke-wheel pattern”.20,26 Gutzeit et al.17,23 propose the use of contrast-enhanced ultrasonography (CEUS) to diagnose SANT, but the role of CEUS needs to be further evaluated as data is limited. There have been two reports of F-18 fluorodeoxyglucose (FDG)-avid splenic lesions found to be SANT lesions,20 however other authors have reported SANT cases without PET activity.6
Martel et al. found three distinct types of blood vessels in the specimens they examined, mirroring the normal composition of splenic red pulp.1 The first were well-formed cord capillaries in an organized lobular arrangement that were CD34+/CD8−/CD31+. The second type of vessel were consistent with splenic sinusoids and were CD34−/CD8+/CD31+. The third type consisted of small veins arranged in a very intricate mesh-like patterns, and were CD34−/CD8−/CD31+. The nodules of vessels are separated by collagenous bands, and the stroma between nodules is sclerotic.
As SANT is a vascular lesion comprised of an over-proliferation of blood vessels, its differential diagnosis includes other benign lesions such as hamartomas, hemangiomas, hemangioendotheliomas, littoral cell angiomas, or inflammatory myofibroblastic lesions. Martel et al. noted that the pathogenesis of this entity is unclear and hypothesize that SANT may be a splenic hamartoma that has undegone an unusual form of sclerosis, with a peculiar reactionary transformation of red pulp due to an exaggerated stromal response.1 It appears that SANT is probably a reactive lesion rather than a true neoplastic process, a theory supported by the high prevalence of concurrent conditions in SANT patients.
The fact that SANT can resemble an inflammatory pseudotumour has prompted some authors to suggest that the two lesions may in fact be the same.5 In support of this hypothesis there have been reports of SANT cases which show EBER-1 (Epstein–Barr virus-encoded small RNAs) positive stromal cells.5 However, while the stroma of IPT and SANT may be histologically similar, IPT do not contain the angiomatoid nodules seen in SANT.8 Recently a number of authors have suggested that the proliferation seen in SANT may be related to IgG4 sclerosing lesions due to the presence of plasma cells found in its stroma.6,7
As this lesion is benign without risk of malignant transformation, the question arises whether an asymptomatic patient with SANT should undergo an operative procedure if the lesion is found incidentally? There is currently no sensitive and specific way to make a diagnosis of SANT without having a tissue sample, and as some lesions that resemble SANT are malignant in nature, we think it prudent to operate even if SANT is suspected. Core biopsy is a sensitive and specific way to diagnose both hematologic and non-hematologic splenic lesions.8,9 Weinreb et al. argue that due to its distinctive nodular pattern, lack of atypia, and unique immunohistochemical profile, that core biopsy can be used to distinguish SANT from other lesions in the differential diagnosis of SANT.5 However, an important factor which Weinreb et al. do not appear to consider, is the risk of intra-peritoneal seeding if the lesion being biopsied proves to be say an angiosarcoma.5
4. Conclusion
The diagnosis of SANT should be considered in any patient presenting with a splenic lesion that contains an angiomatoid or inflammatory component. There is a wide age distribution and the gender distribution appears to be equal. The majority of cases of SANT reported in the literature were incidental diagnoses, with the remainder presenting with a variety of non-specific symptoms. As the differential diagnosis for SANT includes malignant pathologies, and currently no reliable diagnostic radiological feature has been identified to differentiate between these conditions, SANT will continue to be diagnosed on the basis of surgical histopathology.
Conflict of interest statement
No disclosures for any of the authors.
Funding
No disclosures for any of the authors.
Ethical approval
Written informed consent was obtained from the patient for publication of this case report and accompanying images. A copy of the written consent is available for review by the Editor-in-Chief of this journal on request.
Author contributions
Gavin A. Falk – manuscript design, data collection, writing; Nishank P. Nooli – data collection, writing; Gareth Morris-Stiff – data collection, writing; Thomas P. Plesec – pathology review and writing; Steven Rosenblatt – manuscript design, writing.
References
- 1.Martel M., Cheuk W., Lombardi L., Lifschitz-Mercer B., Chan J.K.C., Rosai J. Sclerosing angiomatoid nodular transformation (SANT): report of 25 cases of a distinctive benign splenic lesion. American Journal of Surgical Pathology. 2004;28(October (10)):1268–1279. doi: 10.1097/01.pas.0000138004.54274.d3. [DOI] [PubMed] [Google Scholar]
- 2.Rodriguez F. Rosai and Ackerman's surgical pathology. American Journal of Surgical Pathology. 2004 [Google Scholar]
- 3.Li L., Fisher D.A., Stanek A.E. Sclerosing angiomatoid nodular transformation (SANT) of the spleen: addition of a case with focal CD68 staining and distinctive CT features. American Journal of Surgical Pathology. 2005;29(June (6)):839–841. doi: 10.1097/01.pas.0000160441.23523.d1. [DOI] [PubMed] [Google Scholar]
- 4.Lee D., Wood B., Formby M., Cho T. F-18 FDG-avid sclerosing angiomatoid nodular transformation (SANT) of the spleen: case study and literature review. Pathology. 2007;39(February (1)):181–183. doi: 10.1080/00313020601123904. [DOI] [PubMed] [Google Scholar]
- 5.Weinreb I., Bailey D., Battaglia D., Kennedy M., Perez-Ordoñez B. CD30 and Epstein–Barr virus RNA expression in sclerosing angiomatoid nodular transformation of spleen. Virchows Archiv: An International Journal of Pathology. 2007;451(July (1)):73–79. doi: 10.1007/s00428-007-0422-7. [DOI] [PubMed] [Google Scholar]
- 6.Koreishi A.F., Saenz A.J., Fleming S.E., Teruya-Feldstein J. Sclerosing angiomatoid nodular transformation (SANT) of the spleen: a report of 3 cases. International Journal of Surgical Pathology. 2009;17(October (5)):384–389. doi: 10.1177/1066896909342568. [DOI] [PubMed] [Google Scholar]
- 7.Nagai Y., Hayama N., Kishimoto T., Furuya M., Takahashi Y., Otsuka M. Predominance of IgG4+ plasma cells and CD68 positivity in sclerosing angiomatoid nodular transformation (SANT) Histopathology. 2008;53(October (4)):495–498. doi: 10.1111/j.1365-2559.2008.03118.x. [DOI] [PubMed] [Google Scholar]
- 8.Lal P., Mohan P., Sharma R., Sehgal A., Aggarwal A. Postcoital vaginal laceration in a patient presenting with signs of small bowel perforation: report of a case. Surgery Today. 2001;31(5):466–467. doi: 10.1007/s005950170143. [DOI] [PubMed] [Google Scholar]
- 9.López J.I., Del Cura J.L., De Larrinoa A.F., Gorriño O., Zabala R., Bilbao F.J. Role of ultrasound-guided core biopsy in the evaluation of spleen pathology. Acta Pathologica, Microbiologica, Et Immunologica Scandinavica. 2006;114(June (7–8)):492–499. doi: 10.1111/j.1600-0463.2006.apm_378.x. [DOI] [PubMed] [Google Scholar]
- 10.Lee J.-C., Lien H.-C., Hsiao C.-H. Coexisting sclerosing angiomatoid nodular transformation of the spleen with multiple calcifying fibrous pseudotumors in a patient. Journal of the Formosan Medical Association. 2007;106(3):234–239. doi: 10.1016/S0929-6646(09)60245-X. [DOI] [PubMed] [Google Scholar]
- 11.Diebold J., Le Tourneau A., Marmey B., Prevot S., Müller-Hermelink H.K., Sevestre H. Is sclerosing angiomatoid nodular transformation (SANT) of the splenic red pulp identical to inflammatory pseudotumour? Report of 16 cases. Histopathology. 2008;53(September (3)):299–310. doi: 10.1111/j.1365-2559.2008.03101.x. [DOI] [PubMed] [Google Scholar]
- 12.Demellawy El D., Nasr A., Alowami S. Sclerosing angiomatoid nodular transformation of the spleen: case report. Pathology, Research and Practice. 2009;205(4):289–293. doi: 10.1016/j.prp.2008.12.007. [DOI] [PubMed] [Google Scholar]
- 13.Karaosmanoglu D.A., Karcaaltincaba M., Akata D. CT and MRI findings of sclerosing angiomatoid nodular transformation of the spleen: spoke wheel pattern. Korean Journal of Radiology. 2008;9(July (Suppl)):S52–S55. doi: 10.3348/kjr.2008.9.s.s52. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Zeeb L.M., Johnson J.M., Madsen M.S., Keating D.P. Sclerosing angiomatoid nodular transformation. American Journal of Roentgenology. 2009;192(May (5)):W236–W238. doi: 10.2214/AJR.08.1487. [DOI] [PubMed] [Google Scholar]
- 15.Teng X., Yu X., Wang G., Xu L. Sclerosing angiomatoid nodular transformation of the spleen. Analytical & Quantitative Cytology & Histology. 2008 [PubMed] [Google Scholar]
- 16.Kashiwagi S., Kumasaka T., Bunsei N., Fukumura Y., Yamasaki S., Abe K. Detection of Epstein–Barr virus-encoded small RNA-expressed myofibroblasts and IgG4-producing plasma cells in sclerosing angiomatoid nodular transformation of the spleen. Virchows Archiv: An International Journal of Pathology. 2008;453(September (3)):275–282. doi: 10.1007/s00428-008-0648-z. [DOI] [PubMed] [Google Scholar]
- 17.Gutzeit A., Stuckmann G., Dommann-Scherrer C. Sclerosing angiomatoid nodular transformation (SANT) of the spleen: sonographic finding. Journal of Clinical Ultrasound. 2009;37(June (5)):308–311. doi: 10.1002/jcu.20549. [DOI] [PubMed] [Google Scholar]
- 18.Langer R., Dinges J., Dobritz M., Brauer R.B., Perren A., Becker K. Sclerosing angiomatoid nodular transformation of the spleen presenting as a rapidly growing tumour in a patient with rectal cancer. BMJ Case Reports. 2009 doi: 10.1136/bcr.11.2008.1191. bcr1120081191 [September 15] [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Chikkappa M.G., Morrison C., Lowe A., Antrim R., Swirsky D.M., Gokhale J. Case report and magnetic resonance images of sclerosing angiomatoid nodular transformation (SANT) of the spleen. BMJ Case Reports. 2009 doi: 10.1136/bcr.07.2009.2131. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Thacker C., Korn R., Millstine J., Harvin H., Van Lier Ribbink J.A., Gotway M.B. Sclerosing angiomatoid nodular transformation of the spleen: CT, MR, PET, and 99(m)Tc-sulfur colloid SPECT CT findings with gross and histopathological correlation. Abdominal Imaging. 2010;35(December (6)):683–689. doi: 10.1007/s00261-009-9584-x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Kuybulu A., Sipahi T., Topal I., Uner A. Splenic angiomatoid nodular transformation in a child with increased erythrocyte sedimentation rate. Pediatric Hematology and Oncology. 2009;26(September (7)):533–537. doi: 10.1080/07357900903114010. [DOI] [PubMed] [Google Scholar]
- 22.Kuo T.-T., Chen T.-C., Lee L.-Y. Sclerosing angiomatoid nodular transformation of the spleen (SANT): clinicopathological study of 10 cases with or without abdominal disseminated calcifying fibrous tumors, and the presence of a significant number of IgG4+ plasma cells. Pathology International. 2009;59(December (12)):844–850. doi: 10.1111/j.1440-1827.2009.02456.x. [DOI] [PubMed] [Google Scholar]
- 23.Cao J.-Y., Zhang H., Wang W.-P. Ultrasonography of sclerosing angiomatoid nodular transformation in the spleen. World Journal of Gastroenterology. 2010;16(Aug 7 (29)):3727–3730. doi: 10.3748/wjg.v16.i29.3727. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Sitaraman L.M., Linn J.G., Matkowskyj K.A., Wayne J.D. Sclerosing angiomatoid nodular transformation of the spleen masquerading as a sarcoma metastasis. Rare Tumors. 2010;2(4):e45. doi: 10.4081/rt.2010.e45. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Subhawong T.K., Subhawong A.P., Kamel I. Sclerosing angiomatoid nodular transformation of the spleen: multimodality imaging findings and pathologic correlate. Journal of Computer Assisted Tomography. 2010;34(February (2)):206–209. doi: 10.1097/RCT.0b013e3181bb4480. [DOI] [PubMed] [Google Scholar]
- 26.Bamboat Z.M., Masiakos P.T. Sclerosing angiomatoid nodular transformation of the spleen in an adolescent with chronic abdominal pain. Journal of Pediatric Surgery. 2010;45(July (7)):E13–E16. doi: 10.1016/j.jpedsurg.2010.04.020. [DOI] [PubMed] [Google Scholar]
- 27.Raman S.R., Parithivel V.S., Niazi M. Sclerosing angiomatoid nodular transformation of the spleen. Archives of Surgery. 2010;145(February (2)):205–206. doi: 10.1001/archsurg.2009.279-a. [Image of the month] [DOI] [PubMed] [Google Scholar]
- 28.Kim K.-H., Lee S., Youn S.H., Lee M.R., Kim M.C., Rha S.-H. Laparoscopic splenectomy for sclerosing angiomatoid nodular transformation of the spleen. Journal of the Korean Surgical Society. 2011;80(Suppl 1):S59–S62. doi: 10.4174/jkss.2011.80.Suppl1.S59. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Onder S., Kosemehmetoglu K., Himmetoglu C., Firat P., Uner A. Sclerosing angiomatoid nodular transformation (SANT) of spleen: a case report describing cytology, histology, immunoprofile and differential diagnosis. Cytopathology. 2011;2(August) doi: 10.1111/j.1365-2303.2011.00901.x. [DOI] [PubMed] [Google Scholar]
- 30.Vyas M., Deshmukh M., Shet T., Jambhekar N. Splenic angiomatoid nodular transformation in child with inflammatory pseudotumor-like areas. Indian Journal of Pathology and Microbiology. 2011;54(September (4)):829–831. doi: 10.4103/0377-4929.91543. [DOI] [PubMed] [Google Scholar]