

Abstract
A branchial cleft cyst (BCC) commonly presents as a solitary, painless mass in the neck of a child or young adult. They are most commonly located along the anterior border and the upper third of the sternocleidomastoid muscle in the anterior triangle of the neck. It is very rare for a BCC to manifest in other locations, especially in the posterior triangle of the neck. BCCs are believed to be derived from the branchial apparatus, mostly from the second branchial arch, although many theories have been proposed to explain the aetiology of BCCs. It is possible for BCCs to be easily misdiagnosed as other swellings of oral or paraoral origin owing to their location. Intraoral lymphoepithelial cysts have also been reported in the literature. It is imperative that clinicians make an accurate diagnosis so that appropriate treatment can be performed. If the cysts are excised properly, recurrence is rare. A rare case report of BCC arising in the neck from an unusual location with components in the posterior triangle is presented here.
Keywords: branchial cleft cyst, branchial arches, lymphoepithelial cyst, posterior triangle of neck
Introduction
Branchial cleft cyst (BCC) is a developmental cyst that has a controversial pathogenesis. The term “branchial cleft cyst” refers to the lesions which can be considered synonymous with the cervical lymphoepithelial cyst.1-5
BCC, although relatively rare, is the second major cause of head and neck pathology in childhood. Of the congenital masses related to embryonic remnants, approximately 70% are thyroglossal duct sinuses and cysts, 25% are branchial cysts and sinuses, and 5% are cystic hygromas.6
Various theories have been proposed regarding the origin of the BCC. Ascherson7 (1832), in his “branchial theory”, suggested that incomplete obliteration of branchial cleft mucosa, which remains dormant until stimulated to grow later in life, results in cyst formation. Since then, a number of investigators have reinforced this link between the pharyngeal arches and the branchial cyst.1,4,8
BCCs may arise from remnants of the first, second or third branchial arches; these are categorised in Table 1.1,4,9,10 Most BCCs are of second branchial arch origin and are commonly found in the anterior triangle of the neck anterior to the upper third of the sternocleidomastoid muscle. These have rarely been reported in the lower third of the sternocleidomastoid and in the posterior triangle of the neck.5,6
Table 1. Types of branchial cleft cyst1,4,9,10.
| Type of cyst | Branchial arch | Occurrence | Location |
| First branchial cleft cyst | First branchial arch | 8% | Type I: near external auditory canal or in parotid gland or at angle of mandibleType II: associated with submandiublar gland OR in the anterior triangle of neck |
| Second branchial cleft cyst | Second branchial arch | 95% | Along anterior border of upper third of sternocleidomastoid anywhere from skin of <1?show=[sr]?>lateral neck, between the internal and external carotid arteries and into the palatine tonsil |
| Third branchial cleft cyst | Third branchial arch | 2%—rare | Deep inside the sternocleidomastoid, may be with fistulous tract into larynx |
| Fourth branchial cleft cyst | Fourth branchial arch | Very rare | Arises from lateral neck and parallels recurrent laryngeal nerve. Various locations (including mediastinum) |
BCC is a unilateral, slow-growing, fluctuant soft-tissue swelling that typically appears in the lateral aspect of the neck. BCCs may be bilateral and cases have a tendency to cluster in families.2,4,11 BCCs are congenital in nature although clinically they present later in life, usually in late childhood or early adulthood. A close association with the external ear, angle of the mandible and upper lateral aspect of the neck is usually observed, which is consistent with the fetal location of the branchial apparatus. The swelling typically develops at the junction between the upper third and lower two-thirds of the anterior of the sternocleidomastoid muscle, but it can occur at any level from the hyoid to the suprasternal notch. Chandler and Mitchell12 described the location as being between the tragus and clavicle.3,4 About 60% of cysts occur on the left side.7
The intraoral counterparts have also been identified arising from oral lymphoid tissue. Intraorally, they appear as yellowish-white nodules in the tonsil area or at the posterior lateral border of the tongue.13,14
There is no gender or racial predilection according to most observers.4,11 However, some authors have found BCCs to occur more commonly in females,5 while others claim that 60% of cases occur in males.8 Many BCCs are asymptomatic; however, they may become tender, enlarged or inflamed, especially during periods of upper respiratory tract infection owing to the lymphoid tissue located beneath the epithelium. In some instances, BCC patients may present with locally compressive symptoms if the cyst grows to a large enough size to compress the adjacent structures in the neck.3,4,11 Depending on the size and the anatomical extension of the mass, local symptoms such as dysphagia, dysphonia and dyspnoea may occur. A few cysts may have a definite tract to the posterior pillar of the tonsil but most of them do not.5
It is rare for the BCC to manifest in locations such as in the lower third of the sternocleidomastoid muscle, in the posterior triangle and on the right side. Here the authors report on the case of a BCC situated in locations which possibly correspond to its origin from the third branchial arch.
Case report
A 10-year-old female reported to our hospital with the complaint of swelling on the right side of the neck for 4 months. The swelling was insidious in onset and gradually increased to the present size of 6 × 5 cm. In spite of the enormous size, the swelling was absolutely asymptomatic; there was no associated complaint such as pain, change in voice or difficulty in breathing or deglutition. The patient came to SRMMMT's Hospital, Sawangi-M, India, as the swelling had reached a significant size; there was no history of similar swelling.
On general examination and on laboratory investigation the patient was healthy, afebrile and well nourished. On examination, a globular or ovoid solitary swelling with well-defined margins was observed. The swelling was situated on the right lateral side of the neck in the anterior triangle with anteroposterior extension from the paramedian region to the sternocleidomastoid muscle and superoinferiorly from below the right mandibular angle region up to 1 cm from the base of the neck (Figure 1a,b).
Figure 1.

(a) Solitary globular swelling in the posterolateral aspect of neck along the sternocleidomastoid muscle and in the paramedian region of the neck. (b) Solitary globular swelling in the paramedian region of the neck
On palpation, local temperature was not elevated and the swelling was non-tender, soft, compressible, non-pulsatile and movable with normal overlying skin. The transillumination test was positive. Aspiration from the swelling gave amber-coloured fluid.
Examination of the nose, pharynx and larynx demonstrated no abnormality. Extraoral and intraoral examination revealed no significant findings except for proximal caries with a lower left deciduous first molar, and lymphadenopathy was absent.
Radiographs of the anterior and lateral neck were taken to check the patency of the trachea and revealed no abnormality.
On sonography, the cystic lesion measuring 4 × 3 cm was noted in the right anterior and posterior regions of the neck and below the angle of the mandible at the bifurcation of the common carotid artery, causing it and the superior jugular vein to be displaced medially; no lymph nodes were noted in the field. The submandibular and sublingual glands were of normal shape and size.
On axial and spiral contrast-enhanced CT (CECT) examination, a well-defined, non-enhancing 6.0 × 5.6 × 4.7 cm cystic lesion was noted in the neck, extending from the level of the C2 vertebra up to the level of the thyroid, lying lateral to the right lobe of the thyroid. It was located anterior to the sternocleidomastoid with its posterior component lying below the sternocleidomastoid in the posterior triangle. Anteriorly the lesion was abutting the submandibular gland, medially abutting the carotid vessels and was seen laterally just underneath the subcutaneous plane. It showed septation within the lesion. Laryngeal structures, pharynx and thyroid were normal. There was no evidence of lymphadenopathy. Vascular structures in the neck were normal in course, calibre and enhancement pattern. No other abnormality was detected (Figure 2a,b).
Figure 2.

(a) Contrast enhanced CT (CECT) image showing location of the lesion in the anterior triangle and a deep component extending in the posterior triangle on the right side of upper neck below the level of the C2 vertebra. S, sternocleidomastoid muscle; C, carotid vessels; I, internal jugular vein. White arrows show the extent of the cyst. (b) CECT image showing location of the lesion in the lower neck adjacent to thyroid on the right side. Arrows show the extent of the cyst
The surgical excision of the cyst was planned; the transverse incision was given to elevate the skin with platysma in the upper and lower flap and the cyst was dissected out carefully. Intraoperatively, the lesion was shown to be adherent to the sternocleidomastoid, superiorly to the submandibular gland, and the base was lying on the internal jugular vein. The adjacent vital structures in the neck such as the ansa cervicalis, internal jugular vein, carotid vessels, vagus nerve, hypoglossal nerve and superior thyroid artery were identified and the cyst was dissected out carefully in toto along with the lymph nodes.
The specimen was sent for histopathological examination, which revealed features suggestive of branchial cleft cyst (Figure 3). The patient was followed up for 2 years and no evidence of recurrence was observed.
Figure 3.
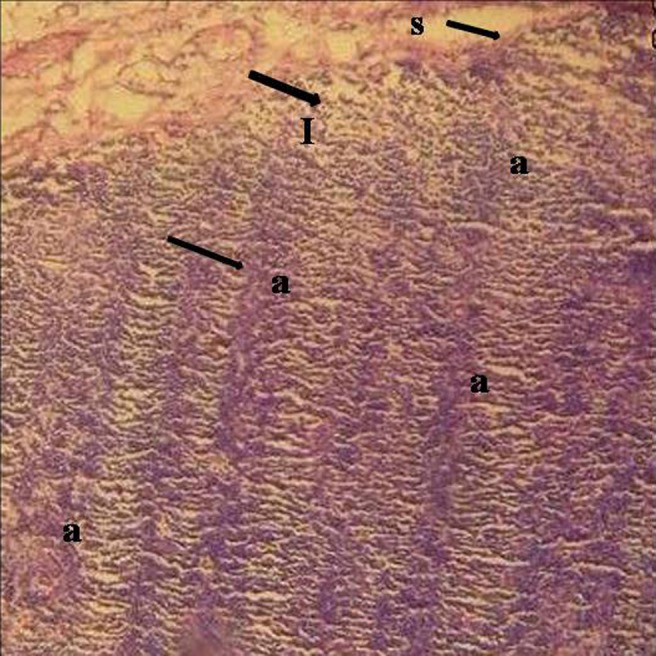
Photomicrograph showing the lymphoid aggregates lined by epithelium at various places; the features are suggestive of branchial cleft cyst. S, lining of stratified squamous epithelium; I, free lymphoid cells; a, lymphoid aggregates in band-like or follicular pattern
Discussion
Hunczovsky, in 1785, gave the first account of lateral cysts of the neck.1,5 At least four theories have been proposed regarding the origin of the BCC. These include incomplete obliteration of branchial mucosa, persistence of vestiges of the precervical sinus, thymopharyngeal ductal origin and cystic lymph node origin. Several investigators have emphasized the link between the pharyngeal arches and the branchial cyst.1,4,7,10 Later on, the theory of the cystic changes in the epithelium entrapped in the lymph node during development became popular, giving rise to the term “benign cystic lymph nodes” or “benign lymphoepithelial cyst”. The controversy over the aetiology of the swelling has given rise to a multitude of terms to describe the same lesion, such as dermoid cyst of sheath of the internal jugular vein, deep seated atheromatous tumour, congenital hydrocoele of the neck, hygroma colli, branchial cyst, tumour of branchial cleft, lateral lymphoepithelial cyst and benign cystic lymph node.1,15
The extensive literature review suggests that the terms “branchial cleft cyst” and “cervical lymphoepithelial cyst” are synonymous.1,4,8
The diagnosis of BCC is made primarily using medical history, clinical manifestations and exclusion. Pre-operative diagnostic procedures include CT, MRI, sonography and fine-needle aspiration.8
CT not only confirms the cystic nature of BCC, but also determines the extent and anatomical relationship with adjacent structures (Table 2).10,16
Table 2. Features of branchial cleft cysts on CT examination10,16.
| Type of cyst | Level of cyst | Mass attenuation on CECT | Location |
| First branchial cleft cyst | At level of hyoid bone | Ill-defined, non-enhancing mass | Type I: inferior and posterior to the tragus, near external auditory canal or in parotid gland or at angle of mandibleType II: associated with submandiublar gland OR in anterior triangle of neck |
| Second branchial cleft cyst | At level of hyoid bone | Well-defined, non-enhancing, water attenuation mass | Along anterior border of upper third of sternocleidomastoid between the internal and external carotid arteries and into the palatine tonsil |
| Third branchial cleft cyst | At level of thyroid cartilage | Well-defined, non-enhancing, water attenuation mass | Deep inside the sternocleidomastoid, may be with fistulous tract into larynx, medially displacing common carotid artery and internal jugular vein |
| Fourth branchial cleft cyst | – | – | Arises from lateral neck and parallels the course of the recurrent laryngeal nerve |
CECT, contrast-enhanced CT.
Both MRI and CT scanning are preferred in the evaluation of branchial cleft cysts.4,10,16 The choice of imaging technique depends on regional preferences; MRI is preferred over CT for Type I first branchial cleft cysts and for parapharyngeal masses that may be second branchial cleft cysts. It reliably confirms the cystic nature of the mass and more precisely defines the extent of the lesion and its relationship to the surrounding structures. It is also believed that all the clinically relevant information is available as clearly on CT scans as on MRI but with lower costs and with an easier imaging process.10 Limitations of CT and MRI are that both are unable to distinguish a branchial cleft cyst from a lymphangioma in children or metastatic squamous cell carcinoma from cervical nodes in adults.10
Ultrasonography, although a commonly used modality, does not adequately evaluate the extent and depth of neck lesions. It is useful in places where CT scanning and MRI are unavailable.10
BCC contains either straw- or brownish-coloured fluid or it may be a turbid, thick fluid consisting of cholesterol crystals and squamous epithelial cells on fine-needle aspiration cytology, usually with a positive transillumination test. More recently, Reynolds and Wolinski17 described uniform low- to medium-level echogenicity in cysts due to the presence of cholesterol crystals and cellular material.3,4
To detect the origin of these cysts and to study the nature of epithelium at the molecular level, immunohistochemistry was performed, particularly the cytokeratin expression profile. It is assumed that the respiratory epithelium is the native epithelium of the cysts and squamous metaplasia results from inflammation-induced stem cell hyperplasia in respiratory epithelium evidenced by coexpression of simple cytokeratins (CKs 7, 8, 18) and stratified epithelial-type cytokeratins (CKs 1, 10, 13).18
Histopathologically, BCCs are lined mostly by squamous or columnar epithelium, resting on a complete or incomplete band of lymphoid tissue corresponding to the tonsils and other lymphatic tissues in the pharynx with part of the cyst wall resembling a lymph node. The copious lymphoid tissue has a follicular pattern with a germinal centre or diffuse band-like pattern.4,6,12
The embryological model of intrauterine development of the fetus is used to explain the origins of all branchial apparatus anomalies. A basic understanding of cervical embryology is essential to predict these anomalies.19
The branchial apparatus develops during the second and sixth weeks of fetal life. At this stage, the neck is shaped like a hollow tube with circumferential ridges, which are termed branchial arches. By the end of the fourth week of gestation, the branchial apparatus consists of four well-defined pairs of mesodermal (branchial) arches separated from each other externally by ectodermally lined branchial clefts and internally by endodermally lined pharyngeal pouches; the fifth and sixth arches are small and cannot be seen on the embryonic surface.4,10,19
The second, third and fourth branchial clefts merge to form the sinus, which will normally become involuted. When a branchial cleft is not properly involuted, a branchial cleft cyst forms. The most accepted theory proposes that vestigial remnants result from incomplete obliteration of the branchial apparatus, and if cells are trapped in the branchial apparatus during the embryological stage, they can form branchial cysts later in life.
The first branchial apparatus completes its development into the maxilla, mandible, eustachian tube, external auditory canal and portions of the middle ear structures by the sixth and seventh weeks. As the parotid gland and facial nerve develop somewhat later, a vestigial first branchial anomaly is located around them. Thus, the first branchial cleft cyst can originate anywhere along the nasopharynx, middle ear cavity or external auditory canal and can extend from these areas in anterior or posterior directions to the pinna or down below the angle of the mandible. They may also involve the parotid gland or lie medially or superficially to it. This specifies the location for the first branchial cleft cyst.
The second branchial apparatus forms the facial muscles, pinna, styloid process and portions of the middle ear structure; this developmental process completes by the sixth or seventh week of gestation. The first and second arch vessels disappear, leaving the third vessel (common carotid artery and proximal internal carotid arteries) as the most cephalic vessel to persist. Because the external carotid artery arises from either the mesenchyma around the branchial arches or from the persistence of the ventral aorta, the second branchial cleft cyst formed above the third arch must pass between the internal and external carotid arteries. Then, the second branchial cleft cyst progressively moves upward and medially along a path between the anterior margin of the sternocleidomastoid muscle and the tonsillar fossa.
As the dorsal aorta between the third and fourth arches involutes, a third branchial anomaly must pass posterior to the common carotid artery or internal carotid arteries. Because of this relationship, most third branchial anomalies originate in the posterior compartment behind the sternocleidomastoid muscle. They may originate adjacent to or within the larynx.4,10,19
In our case, the cyst was larger in size and was located laterally in the neck adjacent to the sternocleidomastoid. The radiological interpretation suggests the large, well-defined, non-enhancing mass in the posterior cervical space medially displaces the carotid vessels and extends below and posterior to the sternocleidomastoid as well as below the level of the thyroid gland. Considering the embryogenic origin, the location of the first branchial cleft cyst will be in the vicinity of the external auditory canal, parotid or the angle of the mandible. It is superficial in location and lies at the higher level in the neck along the anterior surface of the sternocleidomastoid muscle, just below the platysma muscle.16 Radiologically, the cyst is usually a small, ill-defined lesion which may be located medially or superficially to the parotid at the level of the hyoid bone. Fourth branchial cleft anomalies are extremely rare and usually manifest as sinus tracts which arise from the pyriform sinus through the thyrohyoid membrane and descend into the mediastinum following the tracheoesophageal groove.16
Hence, the possibility of the cyst in our case originating from the first or fourth branchial arch cleft is ruled out.10,16,19
At times, it will not be easy to clinically differentiate the second branchial cleft cyst from the third branchial cleft cyst. The second branchial cleft cyst is found along the anterior surface of the sternocleidomastoid muscle, lateral to the carotid space and posterior to the submandibular gland at the level of the hyoid bone, while the third branchial cleft cyst is located below and posterior to the sternocleidomastoid at the level of the thyroid gland.
The clinical and radiological features of the cyst in our case suggest that the cyst’s origin is the third branchial arch. By understanding the embryological basis for these defects, the radiologist is better able to evaluate the location and the type of branchial cyst.4,10,16,19
The clinical differential diagnosis of BCC includes odontogenic infection, parotid swelling, tuberculous lymphadenitis, lipoma, cystic hygroma, carotid body tumours, thyroglossal duct cysts, suppurative lymphadenitis, branchial fistulas or sinus, dermoid cysts, neurofibroma, haemangioma, lymphangioma, teratoma, ectopic salivary tissue, pharyngeal diverticulum, laryngocele and plunging ranula. Clinicians must consider malignancies involving the lymph nodes, either primarily or secondarily, especially when the patient is elderly.4,8,10
In the present case, the transillumination test was performed for the swelling. The test is used to detect whether the swelling transmits the light passed through it brilliantly or not. It is a function of the optical density of the component elements of the swelling; a cyst containing clear fluid transilluminates brilliantly, e.g. hydrocoele and cystic hygroma, while one containing opalescent fluid transilluminates less well, e.g. spermatocele and fat (lipoma), and subcutaneous tissue transilluminates to a varying extent.
The cyst in this case showed a positive transillumination test; however, it is not brilliantly positive which, along with clinical history, excludes the possibility of cystic hygroma. The positive transillumination test and the fluctuant nature of the swelling also rules out the solid masses such as tumours involving various tissues in the submandibular region and neck as well as cervical lymphadenopathies. Besides, pharyngeal diverticulum and external laryngocele manifest in middle or old age and so will not be considered in the differential diagnosis for this case.
Plunging ranula is located in the submandibular region and extends downwards. Thyroglossal duct cysts present as a midline neck mass at or below the level of the hyoid bone and the mass moves with swallowing. Some patients will have neck or throat pain or dysphagia. Dermoid cysts occur in the midline and differ in location from the cyst in the present case. All of these differ in microscopic features from BCCs.
Thymic cysts and parathyroid cysts may be included in the differential diagnosis, especially on CT evaluation. Thymic cysts occur as soft-tissue swellings in the region from the level of hyoid bone up to the mediastinum. Similarly, parathyroid cysts are located around or are most commonly inferior to the thyroid gland. However, both can be differentiated from the BCC by their typical histopathological features.
Surgical excision of the BCC is the treatment of choice and is considered definitive. Complications of surgical treatment include recurrence, formation of a persistent fistula and damage to the cranial nerves. Alternative treatments, such as percutaneous sclerotherapy, are promising but remain unproven.3,4,10
Recurrences are known to occur following complete surgical excision of the BCCs, as seen in a large retrospective study where the overall recurrence rate was noted to be 4.9% after a 2 year follow-up period, while in other studies a recurrence rate of 3–20% was reported.6,10
In conclusion, the aetiology of BCC is yet to be delineated, although the majority of opinions suggest its origin is either from branchial apparatus or from lymphoid tissues. Considering the anatomical location and the radiological appearance, the precise embryological origin can be predicted.
BCC shares a clinical presentation with other pathological entities of the neck, making diagnosis difficult at times. Oral health professionals should be aware of this entity because it can be easily confused with an odontogenic infection and submandibular or parotid gland pathology, especially if it develops high up in the neck.
References
- 1.Thomaidis V, Seretis K, Tamiolakis D, Papadopoulos N, Tsamis I. Branchial cysts—a report of 4 cases. Acta Dermatoven APA 2006;15:85–89 [PubMed] [Google Scholar]
- 2.Berseth CL, Poenaru D. Structural anomalies of GIT. In: Tacusch HW, Ballard RA, Gleason CA, eds. Avery’s diseases of the newborn (8th edn). Philadelphia, PA: WB Saunders, 2005. pp. 1086–1087 [Google Scholar]
- 3.Howard DJ, Lund VJ. Pharynx, larynx and neck—branchial cleft cyst. In: NS Williams, CJK Butstrode, PR O’Connell, A Hodder, eds. Bailey and Love’s short practise of surgery (20th edn). London, UK: Harcourt, 2008. pp. 727–729 [Google Scholar]
- 4.Glosser JW, Pires CA, Feinberg SE. Branchial cleft or cervical lymphoepithelial cysts: etiology and management. J Am Dent Assoc 2003;134:81–86 [DOI] [PubMed] [Google Scholar]
- 5.Vaidya S, Pagare RS, Sharma VK. Lateral cervical cyst. Inter J Otorhinolaryngol 2008;7:1–6 [Google Scholar]
- 6.Aboud KA, Hawsawi KA, Ramesh V, Aboud DA, Githami AA. First branchial cleft sinus: discussion [accessed 17 July 2009]. Available from: http://www.medscape.com. [Google Scholar]
- 7.Ascherson GM. Defistulis Colli congenitis fissuratum branchialium in mammalibus avibusque historica succincta. CH Jonas, Berolini, 1832:1–21 [Google Scholar]
- 8.McClure MJ, McKinstry CS, Stewart R, Madden M. Case report—late presentation of branchial cyst. The Ulster Med J 1998;67:129–131 [PMC free article] [PubMed] [Google Scholar]
- 9.Neutze J. Branchial cleft cyst. MyPACS.net: Radiology teaching files, Penn State College of Medicine, PA [updated 23 April 2011; accessed 2 April 2009]. Available from: www.mypacs.net/cases/23511086.html. [Google Scholar]
- 10.Branstetter BF. Branchial cleft cysts, radiology, head and neck. [accessed 11 March 2009]. Available from: http//www.emedicine.medscape.com. [Google Scholar]
- 11.Hong CH, Richard C. Branchial cleft cyst, dermatology, pediatric diseases [accessed 11 March 2009]. Available from: http://www.emedicine.medscape.com. [Google Scholar]
- 12.Chandler JR, Mitchell B. Branchial cleft cysts, sinuses and fistulas. Otolaryngol Clin North Am 1981;14:175–186 [PubMed] [Google Scholar]
- 13.Intraoral lymphpepithelial cyst—oral and perioral soft tissue cyst In: Cawson RA, Binnie MW, Speight PM, Barrett AW, Wright JM, eds. Lucas’s pathology of tumours of oral tissues (5th edn). UK: Churchill Livingstone, 1998. pp. 159–165 [Google Scholar]
- 14.Neville BW, Damm DD, Allen CM, Bouquot JE. Non-odontogenic cyst and tumours. In: Neville BW, Damm DD, Allen C, Bouquot JE, eds. Oral and maxillofacial pathology. Missouri: Saunders Elseviers, 2009. pp. 36–37 [Google Scholar]
- 15.Golledge J, Ellis H. The etiology of lateral cervical (branchial) cysts: past and present theories. J Laryngol Otol 1994;108:653–659 [DOI] [PubMed] [Google Scholar]
- 16.Woo EK, Connor SEJ. Computed tomography and magnetic resonance imaging appearances of cystic lesions in the suprahyoid neck: a pictorial review. Dentomaxillofacial Radiol 2007;36:451–458 [DOI] [PubMed] [Google Scholar]
- 17.Reynolds JH, Wolinski AP. Sonographic appearance of branchial cysts. Clin Radiol 1993;48:109–110 [DOI] [PubMed] [Google Scholar]
- 18.Flanagan PM, Roland HJ, Jones AS. Cervical node metastases presenting with features of branchial cysts. J Laryngol Otol 1994;108:1068–1071 [DOI] [PubMed] [Google Scholar]
- 19.Benson MT, Dalen K, Mancuso VA, Kerr HH, Cacciarelli AA, Dalen K, et al. Congenital anomalies of the branchial apparatus: embryology and pathologic anatomy. RadioGraphics 1992;12:943–960 [DOI] [PubMed] [Google Scholar]