

Self-expanding metallic stents are effective for the palliation of malignant obstruction. This study indicates that stents for bowel obstruction may allow for minimally invasive surgical intervention with a shorter hospital stay, lower stoma rate, and earlier chemotherapy administration.
Keywords: Colon obstruction, Self-expandable metallic stents, SEMS, Intraluminal stents
Abstract
Background and Objectives:
Acute colorectal obstruction is a potentially life-threatening emergency that requires immediate surgical treatment. Emergency procedures had an associated mortality rate of 10% to 30%. This encouraged development of other options, most notably self-expanding metallic stents. The primary endpoint of this study to is to report our group's experience.
Methods:
We performed a retrospective review of 37 patients who underwent self-expanding metallic stent placement for colorectal obstruction between July 2000 and May 2012. Data collected were age, comorbidities, diagnosis, intent of intervention (palliative vs bridge to surgery), complications, and follow-up.
Results:
The study comprised 21 men (56.76%) and 16 women (43.24%), with a mean age of 67 years. The intent of the procedure was definitive treatment in 22 patients (59.46%) and bridge to surgery in 15 (40.54%). The highest technical success rate was at the rectosigmoid junction (100%). The causes of technical failure were inability of the guidewire to traverse the stricture and bowel perforation related to stenting. The mean follow-up period was 9.67 months. Pain and constipation were the most common postprocedure complications.
Discussion:
The use of a self-expanding metallic stent has been shown to be effective for palliation of malignant obstruction. It is associated with a lower incidence of intensive care unit admission, shorter hospital stay, lower stoma rate, and earlier chemotherapy administration. Laparoscopic or robotic surgery can then be performed in an elective setting on a prepared bowel. Therefore the patient benefits from advantages of the combination of 2 minimally invasive procedures in a nonemergent situation. Further large-scale prospective studies are necessary.
INTRODUCTION
Approximately 103,000 new cases of colon cancer and 40,000 of rectal cancer are diagnosed every year in the United States.1 Of the patients with colorectal cancer, 10% to 30% will present with large bowel obstruction as the initial presentation. Eighty-five percent of acute colonic obstructions are caused by malignancy, and curative resection is not feasible in >25% of cases.2 Acute colorectal obstruction, irrespective of its malignant or benign nature, is a potentially life-threatening emergency that requires immediate surgical treatment.3 Several approaches have been reported, and the Hartmann procedure is the most common procedure performed.4
Emergency procedures had an associated mortality rate of 10% to 30% and a morbidity of 10% to 36%. This encouraged development of other options, most notably self-expanding metallic stents (SEMSs). SEMSs enable temporary relief of acute large bowel obstructions.5 First reported by Dohmoto6 in 1991, initially, their use was restricted to palliation of malignant disease.2
More recently, SEMSs have been used as a bridge to surgery.7 This approach relieves the obstruction, allowing the patient to have a standard preoperative bowel preparation, and converts an emergency situation into an elective scenario. The patient can undergo a laparoscopic or robotic-assisted procedure instead of a conventional open procedure. With this approach, the patient often avoids a colostomy, can be optimized for surgery, and benefits from the advantages of a combination of 2 minimally invasive procedures.7–10
The perceived advantages of using an intraluminal colonic wall stent include the following: it has long-lasting therapeutic effects, it is well tolerated, and it has low rates of morbidity and mortality.11,12 Furthermore, Karoui et al.13 recommend the use of an SEMS as the first-line option to treat colon cancer obstruction because it allows earlier administration of chemotherapy, shortens the hospital stay, and avoids a stoma in two-thirds of patients. Yet, despite the many reported advantages, SEMSs have not gained wide acceptance as a first-line approach. Therefore we reviewed our group's recent experience with the management of a left-sided large bowel obstruction due to benign or malignant disease with SEMSs both for palliation and as a bridge to minimally invasive surgery.
METHODS
A retrospective review was conducted of all patients who underwent SEMS placement for colorectal obstruction between July 2000 and May 2012. All SEMS procedures were performed by endoscopy-experienced, board-certified colorectal surgeons (G.P. and H.J.L.). During the study period, 37 patients underwent 39 SEMS placements. The following data were collected for each patient: age, sex, comorbidities, diagnosis, intent of intervention (palliative vs bridge to surgery), type of stent, complications, and follow-up. Data were recorded in an institutional review board–approved database.
Patients were included if they were aged [me]18 years presenting with clinical features and symptoms of left-sided colorectal obstruction. Obstructing lesions proximal to the splenic flexure are managed by immediate resection with or without diversion in our practice. Diagnosis was usually confirmed by computed tomography. Most patients underwent preoperative water-soluble contrast enema administration to better define the location and length of the stricture (at the discretion of the treating surgeon). All patients had endoscopic features of obstruction, and a colonoscope of 11 mm in diameter could not pass through the stricture. Patients were capable of understanding and giving signed consent for the procedure.
Technical success was defined as the passing of a guidewire and successful deployment and placement of the stent to cover the stricture. The definition of clinical success was colonic decompression with resolution of obstructive symptoms within 72 hours of stent placement.
Technique
Bowel preparation, nasogastric tube decompression, and intravenous antibiotics were individualized based on the clinical presentation, degree of obstruction, and treating surgeon's discretion. Enemas only are recommended before the procedure and are helpful in clearing the distal rectum and colon. The water-soluble enema routinely administered to identify the level of the obstruction and determine the length of the stricture also helps clear the distal bowel. SEMS procedures were performed in an endoscopy suite, radiology suite, or operating room and were dependent on the availability of staff and the day of the procedure. An anesthesiologist in all cases monitored intravenous sedation. We recommend the presence of at least 2 experienced endoscopy nurses to assist the endoscopist. For our first 10 cases, we also had the stent manufacturer representative attend the procedure for technical support.
The first step is an initial attempt to bypass the obstruction with an adult or pediatric gastroscope. When this approach is successful, the guidewire is placed under direct vision beyond the obstruction. This is ideal and possible in >60% of cases. This facilitates placement of the guidewire and eliminates a blind procedure. When the obstruction is too tight to allow a gastroscope, water-soluble contrast is injected through an endoscopic retrograde cholangiopancreatography catheter, and under fluoroscopy, the lumen is identified. Next, the guidewire is advanced under fluoroscopic guidance beyond the obstruction. If one is unable to safely place the guidewire, the case is aborted and the patient taken immediately to surgery for definitive treatment.
Once the guidewire is in position, an endoclip (Resolution Clip Device; Boston Scientific, Natick, MA, USA) is placed at the distal level of the obstruction with a colonoscope (Figure 1). This endoclip will later be used to facilitate stent deployment. On a Boston Scientific stent, there are 2 distal radiopaque markings. By keeping the second mark at the level of the endoclip while deploying the stent under fluoroscopy, proper stent placement is ensured. This maneuver ensures that adequate stent length will be distal to the obstruction (Figure 2).
Figure 1.
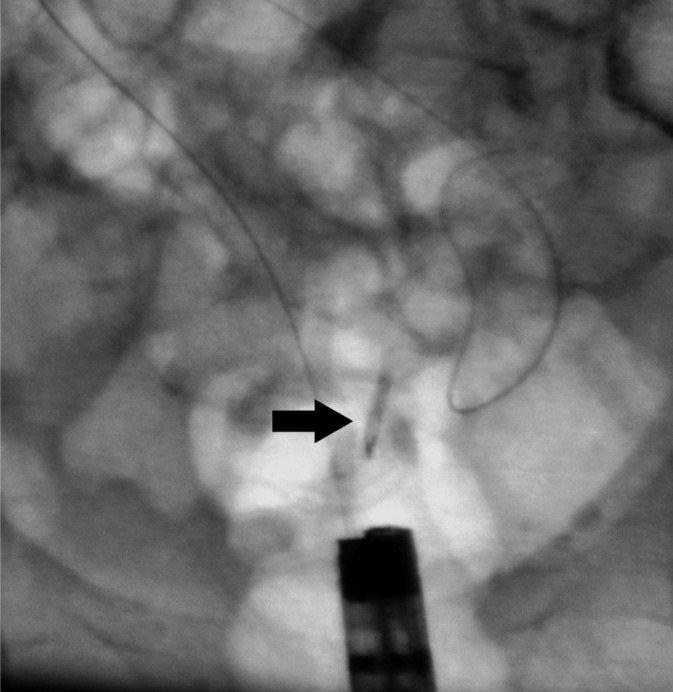
Arrow shows endoclip (Resolution Clip Device) deployed at distal level of obstruction.
Figure 2.

Stent completely deployed.
Alternatively, a paperclip or coin can be taped to the patient's skin to mark the distal level of obstruction. This is accomplished by placing the colonoscope tip at the level of obstruction for identification by fluoroscopy. The patient may need to be placed in a supine position for this to work. The previously described endoclip technique is ideal because it is more accurate and easy to see and the patient's position is not as important.
The next step is to advance an adult colonoscope over the guidewire. Typically, a biopsy forceps is used to pull the guidewire through the colonoscope. An adult colonoscope is necessary for stent placement because of the size necessary for the working channel to accommodate the stent. The colonoscope is now advanced to the level of the endoclip or obstruction. Finally, the stent is advanced over the guidewire, through the colonoscope, and through the obstruction under direct vision. This process is also monitored by fluoroscopy.
As mentioned earlier, deployment of the stent is carried out under both endoscopic and fluoroscopic guidance. Gentle back tension on the stent by the endoscopist as the assistant deploys the stent is necessary to keep the alignment between the endoclip and the second marking on the stent.
Once the stent is deployed, there is often a significant amount of air and liquid stool decompression. We prefer not to pass the colonoscope through the stent. This can result in dislodgement of the stent or damage to the colonoscope. We prefer to confirm proper position by appreciating the typical hourglass appearance of the stent where the obstruction is compressing the stent (Figure 3). This is seen on fluoroscopy as well as on the postprocedure abdominal radiograph. If necessary, a second stent can be placed if needed for longer strictures.
Figure 3.

Circle shows properly positioned stent demonstrating typical hourglass appearance of stent.
The choice of which SEMS to use (with respect to length and diameter, as well as wire guided vs through the colonoscope) was tailored according to the characteristics of the stricture. A Wallstent (Boston Scientific) was the SEMS available at our institution. Most SEMSs were uncovered, with a diameter of 90 × 25 mm. Stents with diameters of 90 × 20 mm, 60 × 25 mm, and 120 × 25 were also used. We used a covered stent in cases of reocclusion due to tumor ingrowth and for benign strictures where elective stent removal was planned. All patients were observed in the recovery unit for 1 to 3 hours and then transferred to the ward. A clear liquid diet was ordered immediately after the procedure and advanced as tolerated.
Candidates for semielective surgery, after clinical success of the procedure, were advised to undergo surgery during the same hospitalization period if possible. Urgent unplanned surgery was indicated in cases of technical failure of stenting, iatrogenic morbidity of SEMSs (bowel perforation), or clinical failure (the obstruction was not relieved). Diverting colostomy or ileostomy was necessary in these cases.
RESULTS
Patient Characteristics
The patients' characteristics are summarized in Table 1. During the study period, a total of 39 SEMS procedures were performed in 37 patients with colon obstruction. There were 21 men (56.76%) and 16 women (43.24%), with a mean age of 67 years (median, 68 years; range, 28–97 years). The intent of the procedure was definitive treatment (palliation) in 22 patients (59.46%) (23 cases [58.97%]) and bridge to surgery in 15 patients (40.54%) (16 cases [41.03%]).
Table 1.
Patient Characteristics
| Data | |
|---|---|
| Patients, n | 37 |
| Age (range), y | 67 (28–97) |
| Procedure, n (%) | |
| Definitive treatment | 22 (59.46) |
| Bridge to surgery | 15 (40.54) |
Location of Pathology and Technical Success Rate
The location of pathology and technical success rate are summarized in Table 2. The most common location of the obstruction was the rectum (n = 16, 43.24%), followed by the sigmoid colon (n = 11, 29.73%), descending colon (n = 6, 16.22%), and rectosigmoid junction (n = 4, 10.81%). The technical success rate was lower at the sigmoid colon (81.82%) and descending colon (83.33%) than at the rectum (100%) and rectosigmoid junction (100%). Low rectal tumors rarely obstruct and usually cannot be stented because the distal portion of the stent will impinge on the sphincters and levator ani or even protrude from the anus. This is poorly tolerated by the patient and often results in severe pain and tenesmus.
Table 2.
Location of Pathology and Technical Success Rate
| Location | n (%) | Technical Success Rate, % |
|---|---|---|
| Rectum | 16 (43.24) | 100 |
| Sigmoid colon | 11 (29.73) | 81.82 |
| Descending colon | 6 (16.22) | 83.33 |
| Rectosigmoid junction | 4 (10.81) | 100 |
Technical and Clinical Outcomes
The technical and clinical outcomes are summarized in Table 3. The SEMS procedure was undertaken for palliation of malignant obstruction in 17 patients (45.95%) (18 cases), with a technical success rate of 94.12%; bridge to surgery for colorectal cancers in 12 patients (32.43%) (13 cases), with a technical success rate of 75%; bridge to surgery for diverticular disease in 4 patients (10.81%), with a technical success rate of 75%; and postoperative anastomotic stenosis in 4 patients (10.81%), with a technical success rate of 100%. The causes of technical failure were inability of the guidewire to traverse the stricture in 3 patients and bowel perforation related to stenting in 2 patients.
Table 3.
Technical and Clinical Outcomes
| n (%) | Technical Success Rate, % | |
|---|---|---|
| Procedure | ||
| Palliation | 17 (45.95) | 94.12 |
| Unresectable distant metastases | 11 (64.71) | |
| Unresectable recurrent CRCa | 5 (29.41) | |
| Unresectable metastasis to colon | 1 (5.88) | |
| Bridge to surgery for CRC | 12 (32.43) | 75 |
| Bridge to surgery for DDa | 4 (10.81) | 75 |
| Postoperative anastomotic stenosis | 4 (10.81) | 100 |
| Time for procedure (range), min | 42.7 (12–90) | — |
| Clinical success rate | 32 (86.49) | — |
CRC = colorectal cancer, DD = diverticular disease.
All patients in the bridge-to-surgery subgroup underwent subsequent intervention. All technical success cases, 12 patients, underwent elective surgery with bowel preparation. The mean preoperative period after SEMS placement was 19 days (range, 4–60 days). The stoma creation rate was 8.33% in this group. All technical failure cases (n = 5) underwent emergency surgery; in 100% of cases, a stoma was created.
The most common reason for palliative treatment was unresectable distant metastases with primary colorectal cancer in 11 cases (64.71%), followed by unresectable recurrent colorectal cancer in 5 cases (29.41%) and unresectable metastasis to the colon in 1 case (5.88%).
The average time for the procedures was 42.7 minutes (range, 12–90 minutes), with a clinical success rate of 86.49% (32 patients) (94.12% for palliation and 75% as a bridge to surgery). The placement of a second stent during a second procedure was required in 2 patients; in 1 patient the first stent did not cover the entire length of the obstruction, and the other case was because of tumor ingrowth and reobstruction.
Procedure-Related Complications
Bowel perforation was observed in 2 cases. In case 1 the stent was accidently passed through the sigmoid colon wall because of severe dilatation and fixed angulation of the bowel. This patient had multiple comorbidities and was deemed high risk. The patient was a ward of the state, and informed consent and the management plan were obtained by committee. The Hartmann procedure was immediately performed; however, the patient died in the postoperative period. In case 2 a 94-year-old man with widely metastatic disease had perforation shortly after stent placement likely because of friability of the colon.
Postprocedure Complications
Complications were recorded as 1 per patient even if the patient had multiple complications, and are summarized in Table 4. During a mean follow-up period of 9.67 months, postprocedure complications were observed in 10 patients (27.03%). Pain and constipation were the most common, occurring in 5 cases (13.51%); in 3 of these cases, the stent was removed to control the pain at a mean of 31 days (range, 14–54 days), whereas the other 2 cases were managed conservatively. Stent migration was observed in 5 cases (13.51%); 4 stents were removed because of pain, and the other patient refused any further treatment. There was 1 case of stent reocclusion 3 months after initial stent placement because of tumor ingrowth; the patient underwent a second covered stent placement.
Table 4.
Complications
| n (%) | |
|---|---|
| Postprocedure complicationa | |
| Pain and constipation | 5 (13.51) |
| Stent migration | 5 (13.51) |
| Stent reocclusion | 1 (2.70) |
| Patients in whom complications occurred | 10 (27.03) |
More than one patient had more than one complication.
DISCUSSION
Since the 1990s, there have been numerous studies that have explored the role and documented the utility of endoscopic SEMSs to relieve metastatic and incurable large bowel obstruction.6,11,13–15 One of the purposes of SEMS placement is to avoid an emergency operation. An emergency operation is associated with high rates of mortality and morbidity when compared with elective surgery.2,16,17 Patients diagnosed with large bowel obstruction are usually elderly patients with comorbid diseases that can benefit from elective surgery.18 It is well recognized that a 1-stage procedure with primary anastomosis offers significant advantages. A shorter hospital stay, fewer complications, and avoidance of a stoma have all been reported.7
The use of an SEMS has been shown to be effective for palliation of malignant obstruction. It is associated with a lower incidence of intensive care unit admission, shorter hospital stay, lower stoma rate, and earlier chemotherapy administration.13,18 Recently, SEMSs have been used as a bridge to surgery. Laparoscopic or robotic surgery can be performed in a semielective setting on a prepared bowel. Therefore, the patient benefits from the advantages of the combination of 2 minimally invasive procedures in a nonemergent situation and avoids a stoma.3,7,8,10,11
According to a recent review, the technical and clinical success rates for SEMS placement are 75% to 100% and 84% to 100%, respectively.19,20 Our results showed a technical success rate of 94.12% for palliative cases, 75% for bridge to surgery, and 100% for postoperative anastomotic stenosis cases. The clinical success rate was 94.12% for palliative cases and 75% for bridge-to-surgery cases. The main cause of failure was inability to place the guidewire across the lesion. SEMS implantation for lesions located proximal to the left side of the colon is technically more difficult to perform.21 There are few reports of SEMS placement for obstructing lesions of the ascending and transverse colon.22 In our practice we perform SEMS placement for lesions distal to the splenic flexure. Right-sided and transverse colon-obstructing lesions are managed by right hemicolectomy with primary ileocolic anastomosis when possible. Transverse colon lesions are selectively diverted. Absolute contraindications to stenting are colonic or tumor perforation with peritonitis. A relative contraindication is a rectal tumor within 2 cm of the anal margin. Stenting in this circumstance leads to tenesmus and incontinence.23
Short-term complications such as perforation, bleeding, tenesmus, stent failure, pain, and incontinence and long-term complications such as recurrent obstruction and stent migration have been reported.9,24 Bowel perforation is the most serious complication because subsequent fecal peritonitis may be fatal. Delayed colonic perforation that is not related to the stent insertion procedure itself is rare and is usually caused by erosion of the colonic wall by the wire ends of the stent at the tumor site.25,26
Most authors report a rate of perforation < 5%.11,19,27 Song et al.28 have found the rate of perforation to be approximately 10%; in our study we found a rate of 5.41%. We had 2 cases of bowel perforation: 1 in the palliative group and 1 in the bridge-to-surgery group.
Migration is another well-reported complication. Some authors have reported a higher incidence of migration with coated stents. Migration occurs more frequently with these stents because they are more resistant to tumor ingrowth.19,27,29 However, in 1 study double-layered coated stents newly designed to prevent migration failed to improve migration rates.30 Migration is less likely with significant narrowing of the lumen. In other words, the tighter the stricture, the less likely migration will occur. We had 5 cases of migration (13.51%): 4 cases in patients treated for palliation and 1 case in which a stent was placed for a postoperative stenosis. Our rates of migration are similar to those reported in larger reviews (3–20%).11,19,27 Management was performed by removal of the stent in 4 cases; the other patient refused any further treatment.
Reocclusion of the stent is reported to occur in 10% of cases.11 We identified only 1 case of reocclusion (2.7%). The reocclusion was due to tumor ingrowth and was managed with a second coated stent. Minor complications such as bleeding, anal and abdominal pain, tenesmus, and transitory incontinence are reported less frequently and are generally tolerated by patients.27 In our study there were 5 cases of pain and constipation (13.51%): in 3 of these cases, the stent was removed to control the pain, whereas the other 2 cases were managed conservatively.
The postoperative mortality and survival rates are difficult factors to interpret. These numbers more likely reflect the progression of the malignant disease than the actual stent placement procedure. Studies to date have not shown a difference in survival rates in either group of stent patients (palliation or bridge to surgery), suggesting that stent placement probably does not increase the risk of tumor spread.27,29,31
Elective surgery after stent placement has been well reported; usually, the elective operation is performed in an open manner. Few authors have reported laparoscopic colectomy after SEMS placement. These reports are summarized in Table 5. We did not find any study reporting robotic surgery after stent insertion. We included our 2 cases of robotic-assisted left colectomy in the minimally invasive surgery group. In our study all patients who underwent bridging and presented for elective surgery underwent laparoscopic or robotic surgery, and thus benefited from the combination of 2 minimally invasive procedures. These cases were particularly gratifying for all the reasons outlined previously.
Table 5.
Stents as Bridge to Minimally Invasive Surgery
This study had several limitations. First, the number of patients was small. Second, although we included all cases with left-sided colorectal obstruction that received stenting, the possibility of selection bias may have been present because this study was conducted retrospectively. Many questions remain unanswered regarding stenting for colorectal obstruction. The ideal time to operate after stent placement has not been determined yet. Our own experience suggests that patients operated on during the same admission or within 3 weeks of surgery had technically easier operations.
Other authors have suggested that it is safe to administer adjuvant chemoradiation with a stent in place13; however, this is based on limited experience. In our study we had 1 patient who received radiation with a colonic stent placed for a completely obstructing upper rectal cancer. This patient was converted to open surgery because of severe pelvic fibrosis and a frozen pelvis. This patient remains free of disease but has a permanent stoma placed for a rectovaginal fistula. It remains unclear what role the combination of a stent and radiation played in the development of a severely inflamed, narrow, and fibrosed pelvis.
Unfortunately, we do not have data on patients with left-sided obstruction who were managed by immediate laparotomy for comparison with our patients treated with SEMSs. There is no consensus on whether outcomes are better, survival is lengthened, or quality of life is improved by stenting. Further large-scale prospective studies are necessary to overcome these limitations and answer these questions. It is our impression that with a careful, methodical team approach, excellent outcomes can be obtained in this patient population. As described in the “Methods” section, experienced surgical endoscopists, experienced endoscopy nurses and/or assistants, anesthesia and radiology technicians, and manufacturer representatives are all necessary for successful outcomes. It cannot be overemphasized how important the presence of representatives was during the learning curve; they were present for at least our first 10 cases and whenever possible. They provided not only invaluable technical support but also a second set of experienced eyes.
Our experience is consistent with the published literature and supports the notion that the treatment of left-sided large bowel obstruction with SEMSs is safe and effective and has low rates of morbidity and mortality. SEMSs avoid an emergency operation and stoma creation and allow for earlier chemotherapy in patients with disseminated disease. Despite several reports in the literature, the use of SEMSs as a bridge to surgery has been slow to gain wide acceptance. Furthermore, there are few reports to date on the combination of 2 minimally invasive techniques (SEMS insertion followed by laparoscopic or robotic colectomy). The perceived advantages have been described and seem to make intuitive sense. Determining whether this approach will improve outcomes for patients with colorectal obstruction will require further study.
Contributor Information
Henry J. Lujan, Laparoscopic Center of South Florida at Jackson South Community Hospital, Miami, FL, USA..
Guilherme Barbosa, Laparoscopic Center of South Florida at Jackson South Community Hospital, Miami, FL, USA..
Marianna S. Zeichen, Laparoscopic Center of South Florida at Jackson South Community Hospital, Miami, FL, USA..
Wilmer N. Mata, Laparoscopic Center of South Florida at Jackson South Community Hospital, Miami, FL, USA..
Victor Maciel, Surgery Department, Mount Sinai Medical Center, Miami Beach, FL, USA..
Gustavo Plasencia, Laparoscopic Center of South Florida at Jackson South Community Hospital, Miami, FL, USA..
Rene F. Hartmann, Laparoscopic Center of South Florida at Jackson South Community Hospital, Miami, FL, USA..
Manuel Viamonte, III, Laparoscopic Center of South Florida at Jackson South Community Hospital, Miami, FL, USA..
Roberto Fogel, Laparoscopic Center of South Florida at Jackson South Community Hospital, Miami, FL, USA..
References:
- 1. American Cancer Society Colorectal cancer. Available at: http://www.cancer.org/Cancer/ColonandRectumCancer/DetailedGuide/colorectal-cancer-key-statistics Accessed May 15, 2012
- 2. Piccinni G, Angrisano A, Testini M, Bonomo G. Definitive palliation for neoplastic colonic obstruction using enteral stents: personal case-series with literature review. World J Gastroenterol. 2004;10(5):758–764 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3. Fischer A, Schrag H, Goos M, Obermaier R, Hopt U, Baier P. Transanal endoscopic tube decompression of acute colonic obstruction: experience with 51 cases. Surg Endosc. 2007;22(3):683–688 [DOI] [PubMed] [Google Scholar]
- 4. Pirlet IA, Slim K, Kwiatkowski F, Michot F, Millat BL. Emergency preoperative stenting versus surgery for acute left-sided malignant colonic obstruction: a multicenter randomized controlled trial. Surg Endosc. 2010;25(6):1814–1821 [DOI] [PubMed] [Google Scholar]
- 5. Beck DE. Endoscopic colonic stents and dilatation. Colon Rectal Surg. 2010;23(1):37–41 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6. Dohmoto M. New method-endoscopic implantation of rectal stent in palliative treatment of malignant stenosis. Endosc Dig. 1991;3:1507–1512 [Google Scholar]
- 7. Morino M, Bertello A, Garbarini A, Rozzio G, Repici A. Malignant colonic obstruction managed by endoscopic stent decompression followed by laparoscopic resections. Surg Endosc. 2002;16(10):1483–1487 [DOI] [PubMed] [Google Scholar]
- 8. Balagué C, Targarona EM, Sainz S, et al. Minimally invasive treatment for obstructive tumors of the left colon: endoluminal self-expanding metal stent and laparoscopic colectomy. Dig Surg. 2004;21:282–286 [DOI] [PubMed] [Google Scholar]
- 9. Ziakas G, Haas EM. How to use stents for colorectal obstruction. Contemp Surg. 2007;63(10):492–497 [Google Scholar]
- 10. Stipa F, Pigazzi A, Bascone B, et al. Management of obstructive colorectal cancer with endoscopic stenting followed by single-stage surgery: open or laparoscopic resection? Surg Endosc. 2008;22(6):1477–1481 [DOI] [PubMed] [Google Scholar]
- 11. Khot UP, Lang AW, Murali K, Parker MC. Systematic review of the efficacy and safety of colorectal stents. Br J Surg. 2002;89(9):1096–1102 [DOI] [PubMed] [Google Scholar]
- 12. Faragher IG, Chaitowitz IM, Stupart DA. Long-term results of palliative stenting or surgery for incurable obstructing colon cancer. Colorectal Dis. 2008;10(7):668–672 [DOI] [PubMed] [Google Scholar]
- 13. Karoui M, Charachon A, Delbaldo C, et al. Stents for palliation of obstructive metastatic colon cancer: impact on management and chemotherapy administration. Arch Surg. 2007;142:619–623 [DOI] [PubMed] [Google Scholar]
- 14. Law WI, Choi HK, Lee YM, Chu KW. Palliation for advanced malignant colorectal obstruction by self-expanding metallic stents: prospective evaluation of outcomes. Dis Colon Rectum. 2004;47:39–43 [DOI] [PubMed] [Google Scholar]
- 15. Meisner S, Hensler M, Knop FK, West F, Wille-Jorgensen P. Self-expanding metal stents for colonic obstruction: experiences from 104 procedures in a single center. Dis Colon Rectum. 2004;47:444–450 [DOI] [PubMed] [Google Scholar]
- 16. Yoshihisa S, Toshiyuki E, Kazuhiro T, et al. Outcome of 141 cases of self-expandable metallic stent placements for malignant and benign colorectal strictures in a single center. Surg Endosc. 2011;25:1748–1752 [DOI] [PubMed] [Google Scholar]
- 17. Vitale MA, Villotti G, d'Alba L, Frontespezi S, Iacopini F, Iacopini G. Preoperative colonoscopy after self-expandable metallic stent placement in patients with acute neoplastic colon obstruction. Gastrointest Endosc. 2006;63:814–819 [DOI] [PubMed] [Google Scholar]
- 18. Law WL, Choi HK, Chu KW. Comparison of stenting with emergency surgery as palliative treatment for obstructing primary left-sided colorectal cancer. Br J Surg. 2003;91:1429–1433 [DOI] [PubMed] [Google Scholar]
- 19. Sebastian S, Johnston S, Geoghegan T, Torreggiani W, Buckley M. Pooled analysis of the efficacy and safety of self-expanding metal stenting in malignant colorectal obstruction. Am J Gastroenterol. 2004;99:2051–2057 [DOI] [PubMed] [Google Scholar]
- 20. Keymling M. Colorectal stenting. Endoscopy. 2003;35:234–238 [DOI] [PubMed] [Google Scholar]
- 21. De Gregorio M, Mainar A, Rodriguez J, et al. Colon stenting: a review. Semin Intervent Radiol. 2004;21(3):205–316 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22. Dronamraju SS, Ramamurthy S, Kelly SB, Hayat M. Role of self-expanding metallic stents in the management of malignant obstruction of the proximal colon. Dis Colon Rectum. 2009;52(9):1657–1661 [DOI] [PubMed] [Google Scholar]
- 23. Soriano A, Davis M. Malignant bowel obstruction: individualized treatment near the end of life. Cleve Clin J Med. 2011;78(3):197–206 [DOI] [PubMed] [Google Scholar]
- 24. Patel S, Patwardhan R, Levey J. Endoscopic stenting: an overview of potential complications. Pract Gastroenterol. 2003;27:44–54 [Google Scholar]
- 25. Trovato C, Fiori G, Ravizza D, et al. Delayed colonic perforation after metal stent placement for malignant colorectal obstruction. Endoscopy. 2006;2(Suppl 2):E96. [DOI] [PubMed] [Google Scholar]
- 26. Cho YK, Kim SW, Lee B, et al. Clinical outcome of self-expandable metal stent placement in the management of malignant proximal colon obstruction. Gut Liver. 2011;2:165–170 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27. Watt AM, Faragher IG, Griffin TT, Rieger NA, Maddern GJ. Self-expanding metallic stents for relieving malignant colorectal obstruction. Ann Surg. 2007;246:24–30 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28. Song HY, Kim JH, Shin JH, et al. A dual-design expandable colorectal stent for malignant colorectal obstruction: results of a multicenter study. Endoscopy. 2007;39:448–454 [DOI] [PubMed] [Google Scholar]
- 29. Alcantara M, Serra X, Bombardó J, et al. Colorectal stenting as an effective therapy for preoperative and palliative treatment of large bowel obstruction: 9 years' experience. Tech Coloproctol. 2007;11:316–322 [DOI] [PubMed] [Google Scholar]
- 30. Moon C, Kim T, Lee M, et al. Comparison of a newly designed double-layered combination covered stent and D-weave uncovered stent for decompression of obstructive colorectal cancer: a prospective multicenter study. Dis Colon Rectum. 2010;53:1190–1196 [DOI] [PubMed] [Google Scholar]
- 31. Iversen LH, Kratmann M, Boje M, Laurberg S. Self-expanding metallic stents as a bridge to surgery in obstructing colorectal cancer. Br J Surg. 2010;98:281–286 [DOI] [PubMed] [Google Scholar]
- 32. Dulucq JL, Wintringer P, Beyssac R, Barberis C, Talbi P, Mahajna A. One-stage laparoscopic colorectal resection after placement of self-expanding metallic stents for colorectal obstruction: a prospective study. Dig Dis Sci. 2006;51(12):2365–2371 [DOI] [PubMed] [Google Scholar]