

Abstract
This Classic Article is a reprint of the original work by G. Perthes, On juvenile arthritis deformans. An accompanying biographical sketch of G. Perthes is available at DOI 10.1007/s11999-012-2432-2. The Classic Article is © 1910 and is reprinted from Über Arthritis deformans juvenilis. Deutsch Zeitschr Chir. 1910;107:111–159.
Electronic supplementary material
The online version of this article contains two supplementary documents available to authorized users. A PDF of the original article in German (doi:10.1007/s11999-012-2433-1) and searchable PDF of the reset article in German (doi:10.1007/s11999-012-2433-1).
In February 1909, an 11-year old boy was taken to the outpatients’ clinic because his parents had noticed a slightly limping gait. The clinical examination showed a freely mobile right hip in terms of flexion and abduction, however adduction and rotation movements were completely abolished. The trochanter was 1 cm above the Roser-Nélentonschen line. There was no pain on flexion, even with compressive force on the joint. The radiograph showed our first impression of a coxa vara was incorrect. The femoral neck angle was completely normal, however, a conical rather than spherical femoral head. The absence of abduction and rotation movements but free flexion was a consequence of the mechanical ratios. Further observation over one year showed increasingly clear signs of arthritis deformans emerge. After this was being directed by our attention to the first observation of juvenile arthritis deformans of the hip joint, within a year we saw no less than six of the same species.
The reasons these observations are published here is not in the least due to the practical relevance of this interesting affection which is considerably higher than one was previously inclined to believe. The rarity of the affection is highlighted by almost all authors who have written about juvenile arthritis deformans, the very great rarity of the affection is highlighted. After Maydl reported the first such cases there were initially scarce publications on the topic. It took 6 years until v. Brunn brought new attention to it in in-depth work in 1903. More recently each year has brought whole new sets of observations, and with the addition of our own observations the present material now comprises 38 cases, of which 26 – 5 of our own observations – are unilateral, and 12 – including one of ours – are bilateral. The fact was that in our clinic after only one case diagnosed correctly we observed six cases within one year suggests that we had seen similar cases earlier without having been properly diagnosed and would, I think, suggest there are probably similar cases elsewhere with the incorrect diagnosis of coxa vara or early tuberculous coxitis.
However, the attached list of the currently available observational material enlists 6 cases (A. 23, 24, 25, 26, and B. 11,12) in which striking symptoms were observed only after completion of bone growth. Whether one may presume joint inflammation in these cases as a juvenile, is questionable. We shall see, however, that at the onset of symptoms there are usually already severe anatomical changes in the joint. Therefore, since the onset of the disease probably always precedes the onset of clinical symptoms for a long time, there is a probability of disease onset in youth in these latter cases, and the ages noted may therefore be used with a grain of salt.
Among the 26 cases of unilateral disease are 16 males and 10 females, and among the 12 bilateral cases, 5 males and 7 females. A pronounced predilection of one gender cannot be noted so far.
Pathologic changes
Of course, the study of pathologic changes in the x-ray cannot replace the direct pathologic-anatomical investigation; however, it can provide valuable supplement especially for the early stages, the more so as the existing pathologic-anatomical material of the arthritis deformans juvenilis is rather sparse and almost exclusively originates from cases in which the disease was well advanced.
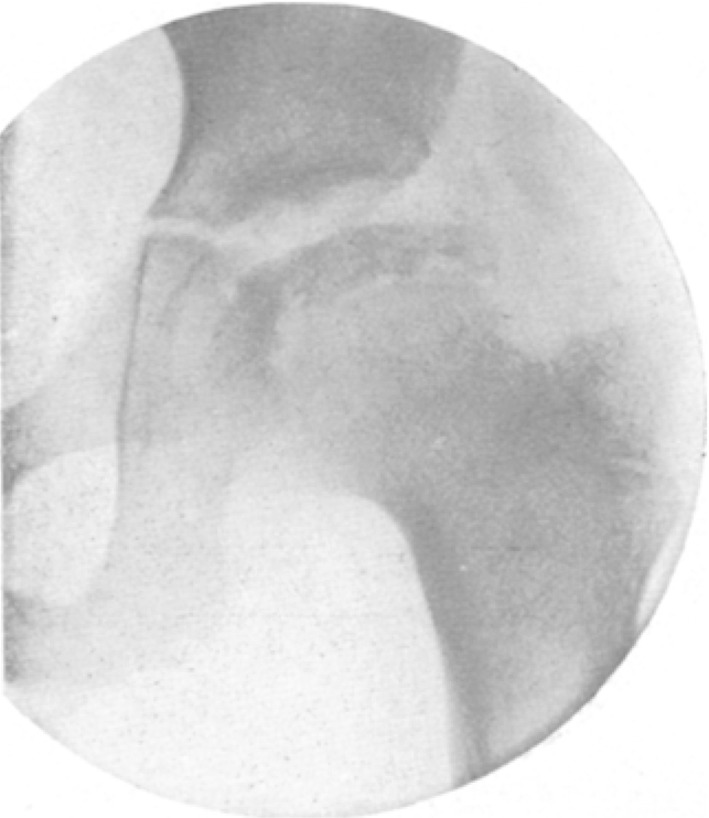
The first and most important changes are found on the head of the femur. Among the 7 diseased hip joints of our 6 patients, in 5 the head cap is indeed deformed, but still well preserved, while in the other two the epiphysis had largely disappeared . In the 5 first-mentioned joints (case 1, 2, 4, 5 and 6 right hip joint), all of which undoubtedly were in a relatively early stage of the disease, there was striking a flattening of the head at the upper end. The height of the femoral epiphysis above the growth plate was reduced accordingly, and it was remarkable that height reduction of the head cap in the cases checked for a year increased gradually. Thus, the head height above the epiphyseal line decreased in the case 1 from 16 to 10 mm, and in case 2 from 12 to 10 mm, while the rest of the bone measures increased according to the growth of the children. In the case 4 (Fig. 5) the height of the head cap appears smaller by one half when compared to the other side. A second flat is noted in the images of the femur on the medial side of these five joints. The upper and the medial border lines of the head form an obtuse angle which is almost a right angle and its slightly rounded tip is located approximately in the extension of the femoral neck.
Fig. 5.

Case 4. 13 year-old boy. Left hip. See also Fig. 16
The x-ray projection of the bones in one plane alone does not allow for a complete perception of the shape of the femoral head in space. However, the combination of X-ray images with the observed deformity, which we will deal with in more detail later, provides additional information. In all five cases, the flexion was either normal or slightly limited, while abduction, adduction and rotation, were substantially reduced or absent. Obviously we must conclude from this limitation of certain movements and from consideration of the x-ray that rather than a ball shape of the femoral head a cone shape appears with the axis approximately in line with the femoral neck axis. One might also consider it a cylindrical or bee-hive shape, a shape that is well known to us in the arthritis deformans of higher ages.
It is likely the deformity of the femoral head we observed in our five cases is typical for the onset of the disease. We gather this from the few pictures of preparation of the resected specimen and X-ray images in the literature; however only one case from Frangenheim corresponds to this shape as seen in our Figs. 2, 4 and 5, but this case is also the only one in the literature published at a fairly early stage of the disease. So perhaps it would be worthwhile to question whether the conical deformation of the femoral head we observed at the onset of arthritis deformans in adolescents is a frequent or even regular finding.
Fig. 2.

The same case as in Fig. 1, but on March 17, 1910. Also see radiograph in Fig. 13
Fig. 4.

The same case as in Fig. 3, but right hip (Editor’s note. The hips appear reversed, although the wording is correct; presumably these are PA views rather than AP.) on June 12, 1910. See also Fig. 14
In the x-rays, which enable the understanding of the bony structure, the architecture of the bony trabeculae of the (femoral) neck appears (‘behaves’) normal. The bony trabeculae of the neck on the diseased and normal side run in exactly the same direction clearly up to the epiphyseal line, and the shape of the neck on both sides is similar. The changes in these early stages affect only the head cap of the femur.
The X-ray images of two cases (cases 1 and 2) show some striking bright spots (Figs. 2, 4, 13 and 14) that certainly indicate a lack of normal bone mass at these points, i.e., focal subchondral bone loss. I would suggest the details of the radiograph would have no value were they not so strikingly consistent with pathologic findings. Since the Ziegler’s investigations, “On the subchondral changes in bone in arthritis deformans” in 1877, it has been known that the bone changes in arthritis deformans are by no means completely described by abrasions and local cartilage bone loss and bone proliferation elsewhere, but that the deformation is partly due to subchondral bone loss. Ziegler speaks of small cysts that develop rapidly in the immediate vicinity of the joint cartilage, sometimes deep in the bone due to bone resorption. Recently Wollenberg examined these subchondral resorption cysts filled with gelatinous material and depicted them in the radiographs. In juvenile arthritis deformans of the resection specimens of Maydl’s second case “resorption lacunae filled with calcareous bony detritus which penetrated up to ¾ cm deep into the neck cancellous bone” were found and Axhausen likewise reported in arthritis deformans juvenilis up to hazelnut-sized, cyst-like cavities “with fluid content that verifiably originates in many locations from degeneration of dense connective tissue”. With these results of the anatomic investigations we will not go wrong when we relate the light spots in the x-ray’s bone shade of the femoral head to such bony resorption processes. These subchondral resorption regions are obviously of considerable importance for the development of the head deformity. It is readily understood that to some extent the cartilage is undermined and sinks, thus creating the flattening of the femoral head.
Fig. 6.

The same case as in Fig. 5, but a normal right hip
Fig. 13.

Case 1 on March 17, 1909
Fig. 14.
Case 2 on June 12, 1910
In the later stages, as seen in the more affected joints, Case 3 and Case 6, left hip joint, the femoral head epiphysis has for the most part disappeared. In addition to the bone atrophy there are proliferation processes that lead to the formation of osteophytes. Thus, the femoral head in case 3 (Figs. 7 and 8) has developed a wide mushroom cap appearance, as is common in advanced cases of arthritis deformans in old age. Bony growths similar to those on the femoral head can also be found on the greater trochanter as in the case 3. They extend towards the head and have almost bridged the region between the osteophytes of the head and the trochanter. The neck of the femur in these cases is also involved now. It appears shortened and thickened. Especially in case 3 the distance between the trochanter and the femur joint surface is significantly reduced. In the radiograph that was taken in the same position of the leg it is only about half of the normal side. The upper part of the femur has thus completely lost a spherical shape. The femoral axis has shifted significantly toward the joint.
Fig. 7.

Case 3. 13 year-old boy. Right hip on June 15, 1909
Fig. 8.

The involvement of the acetabulum is most clearly demonstrated in our cases in the X-ray image of case 3, which has the highest grade changes we have detected. There is significant broadening of the acetabulum with upward placement. The head is centered in a higher position relative to the center of the acetabulum. There is a enlargement of the acetabulum, as it has repeatedly been shown in juvenile arthritis deformans in X-ray images (Preiser, Hesse), and with the head resection (Maydl, Riedel-Zesas, Küster-Zesas). In our case 5 the acetabulum was not enlarged, but had adapted well to the deformed head. The remaining cases showed no such pathological changes in the acetabulum.
There is a very peculiar enormous hypertrophy of the greater trochanter that at the same time occurred with a significant shortening of the femoral neck angle in four cases (Figs. 11 and 12). It can be seen how the trochanter developed into of a bulky structure on the affected as well as the contralateral normal side which projects far above the head and is at least three times the size usually seen in a girl of that age. The upper femoral shaft appears substantially thicker than normal. The neck angle is reduced to 110°–115° on both sides. Since these changes appear in both hip joints but the arthritis deformans only in the left hip, we must assume this anomaly is a complication independent of the arthritis deformans. Only once have I found in the literature similar hypertrophy of the trochanter which was shown in a specimen of juvenile coxa vara from Professor Jordan, of Heidelberg and depicted by Hofmeister in his Handbook of Orthopedic Surgery. Whether it is a congenital anomaly or later acquired remains to be determined. Apart from this one case we did not find coxa vara in any of our cases. Only in the more affected side of our case of bilateral disease (6) we must consider it likely that through further progression of bone resorption at the top of the femoral head and osteophytes on the lower edge it will ultimately develop into a coxa vara (Fig. 9).
Fig. 11.

Case 5. 13 year-old girl. Left hip
Fig. 12.

Same case as in Fig. 11, but right hip
Fig. 9.

Case 6. 9 year-old boy. Left hip
Symptoms
Amongst the symptoms of the disease, the limited flexibility and pathologic position of the hip joint are of foremost interest.
As a general principle the limited mobility is due to the mechanical conditions caused by the deformation of the joint and that reflex muscle tension or adhesions of the joint do not play a role. These major distinctions with tuberculous coxitis are obvious.
From the overview of the cases in the initial stages of the disease, the rule can be established that the restriction of motion in different directions occurs at different rates. Often mobility is limited only in a single direction. This observation provides the distinction between coxitis deformans and tuberculous coxitis. It follows directly from the above-mentioned fact that the change in bone shape and especially the deformation of the femoral head causes the mechanical limitation of motion.
It almost seems as if this rule be further specified so that at least in the early stages certain motion limitations occur more frequently. In the seven observed diseased joints the most affected motion was abduction and flexion was the least impaired. In cases 1, 2, 4 and 6 (left hip) abduction was completely abolished while flexion was free. The rotational motion and the adduction from resting position in these joints were either also abolished or restricted to a few degrees despite the completely free flexion. However, with time we saw in two cases, 1 and 2, with initially absent abduction, that after one year the lateral movement became slightly free with progressive deformity of the femoral head, and that in cases with progressive conditions in the initial x-ray flexion was not entirely free, but abduction and adduction were completely abolished. In these cases also an obvious discrepancy existed between the free flexion and abduction limitation.
In our material the basic position of the hip in three cases (1, 3 and 6, left joint more affected) was normal, in four cases moderately adducted (7–15°) that did not compensate due to the aforementioned abduction limitation. With respect to the rotation in one case a change was seen (internal rotation von 45°, Case 5) . Therefore, if any overall pathologic position existed in our material it was an adduction contracture.
Due to the fact that the discrepancy between flexion mobility and abduction limitation was found in all our cases and was most clearly pronounced where – on the basis of X-ray image – there was relatively little deformation, I am inclined to suspect that this is a typical finding for the early stages of the juvenile coxitis deformans. However, it must be admitted that the abnormal shape of the femoral head and its dependent functional disorder may be nothing more than the patient’s continued use of the affected joint in a certain direction. As the arthritis deformans juvenilis is associated in the beginning with almost no pain, the children run around as before. The reduced bony strength of the affected femoral head leads to a deformation under the effect of body load. Thus, the only shape of the femoral head that allows movement in all directions, the spherical shape has been lost. The head is remodeled mostly by the movements that are performed most frequently, so that at each step, the repetitive flexion movement shapes the developing head. This creates the roller or cone shape, which enables flexion movements but does not permit abduction movements. As bone loss progresses, then the initially inhibited movements are again permitted (our cases 2 and 3) but due to bone overgrowth are again limited; in short, it is conceivable how the initially formed type disappears in later stages and subsequent irregular shapes take its place.
The literature contains so far mainly cases of very late stages of arthritis deformans juvenilis where the disease had already produced high-grade changes in the joints that had existed for many years. In the few cases that can be considered early-stage (case Zesas 1909, two cases of Hofmeister, Fridberg case, 14 year old boy), as well as in our observations free flexion with no or largely limited abduction was seen. After all, the investigation of much more material/larger cohort is highly desirable.
As a result of the partial disappearance of the femoral head, we generally observed minor trochanter elevations (0.5–2 cm) and a corresponding real shortening of the limb which added to the apparent shortening due to the adduction contracture. Only in case 3 the trochanter elevation and shortening increased to 3½ cm due to simultaneous enlargement of the acetabulum. The substantial trochanteric elevation we observed in case 5 was only related to one side and only to a small degree due to the deformity of the femoral head. This was mainly due to the enormous hypertrophy of the trochanter and simultaneous coxa vara.
Even though in all our cases a substantial deformity of the femoral head occurred by the end of our observation period, we observed crepitation in only two joints: a sudden loud crack with certain abduction and adduction movements in Cases 5 and 6. Similarly, in the cases of the literature, crepitation during movement was reported only in a relatively small fraction of cases, such as Riedel Cornils, Zesas 1909, Preiser, Hesse (left joint) as stated above. In some cases, for example, Hesse (right joint), von Brunn (case 2), the authors explicitly reported crepitus was absent. This absence of crepitation in spite of marked deformation can be explained: the joint surfaces rubbed against each other and were rendered perfectly smooth. More likely, however, is that in the earlier stages, no rubbing of bone parts is noted, because the deformation is based on subchondral destruction and a defect of articular cartilage is not yet present.
We could not diagnose an abnormal palpation of the hip region. Only in very advanced cases with considerable bone formation around the joint, case Axhausen, Negroni, can we detect abnormalities by palpation.
The pain behavior in juvenile arthritis deformans is interesting. Despite severe deformity of the femoral head, which dates back at least several months, pain was absent. The 13-year-old boy we observed (case 4) could not only walk normally, but also run and jump without feeling the slightest discomfort and only because of his shaking “wobbly” lame gait did he present to us.
In most cases, however, some spontaneous pain is observed, the pain usually occurring only after prolonged walking or even after prolonged sitting (our Case 2, 3, 5 and 6), and not uncommonly is transferred to the knee as in the tuberculous coxitis (our case 6, numerous cases of the literature, eg, Preiser, Guhl, Fridberg, Axhausen). In our cases this spontaneous pain is not very considerable, and in no case did it give rise to the children staying away from school. However, sometimes the discomfort is considerable, for example in the cases described by Hesse, Zesas 1909.
It is noteworthy that in all of our cases, including those where spontaneous complaints were reported with certainty, the movements were pain-free insofar as possible, especially complete flexion was possible without any discomfort. However, the passive movements as well as pressure on the trochanter or pushing the femoral head into the acetabulum caused pain and only in cases 3 and 4 was strong anterior hip joint pressure considered less sensitive.
This lack of pain during movements despite high-grade destruction of the (femoral) head has been observed by other authors (v. Brunn, Case 2, Zesas, Hesse). Sometimes the contrast between the spontaneous pain in one hand and the absence of pain during clinical examination in the other hand was more striking than was in our cases, because – for example, in the patients of Zesas and Hesse – spontaneous pain seemed to reach much higher levels than in our material.
The limping gait in the juvenile arthritis deformans deserves particular attention. In many cases it is the main issue; in the completely painfree patients it is the only symptom patient recognizes and causes him to consult a physician. Various factors contribute to the emergence of the limping. It is obvious that apparent shortening of the extremity impairs gait by an uncorrectable abduction position of the hip joint, especially if it is combined with real shortening caused by the bone loss in the upper end of the femur. However, this is not the most important cause because in the children we observed also those were limping who did not reveal an adduction contracture or only a slight actual shortening. The gait of our patients exclusively resembled that of a patient with a high degree unilateral congenital hip luxation. When stepping onto the affected leg the trunk tilted towards the ipsilateral side. This rocking motion was not always as pronounced as observed in the luxations but it always appeared similarly.
As is well known, Trendelenburg attributed the swaying gait of congenital hip luxation to an insufficiency of the gluteal muscles. We therefore observed the function of the abductor muscles of the leg. In fact, all our patients showed a significant Trendelenburg sign. When standing on the affected leg – and we will return to the case with bilateral disease below/later – the pelvis dropped to the opposite side, while the upper body leaned over the contralateral side as compensatory action. The pelvis was not stabilized relative to the femur in the normal manner by the gluteus muscles. It was rather tilted towards the opposite side so that the body could be held in equilibrium only by balancing on the femoral head. The insufficiency of the abductor muscles, primarily the gluteus medius and minimus, was thus established. In some of the cases muscle atrophy could be detected by palpation as well. Undoubtedly, this muscle insufficiency is largely aggravated by the high position of the trochanter. With a pronounced trochanteric elevation, the line of action of the gluteus medius in particular is shifted in such a way that its abduction action is extremely elevated, as Trendelenburg has shown for congenital hip dislocation and Alsberg for coxa vara. Even with minor elevation, which does not involve a significant shift in the direction of pull – and several of our children limped with only of minor elevation – the approximation of insertion and origin of the muscles will diminish the tension that is necessary for proper functioning, and will relax the muscles, and thus lead to a weakening of muscle strength.
Finally, a third factor comes into consideration. In our cases 5 and 6 a high trochanter was found bilaterally yet the sway of the trunk occurred only on one side. The Trendelenburg sign was positive only on one side. Case 5 had bilateral coxa vara with arthritis deformans only on one side; and case 6 had bilateral coxitis. The explanation may be sought in the fact that in such cases a bony restriction limited abduction from the neutral position on the side of a positive Trendelenburg sign, so that the abductor strength was weakened from disuse. As a result of this inactivity-induced atrophy, they were obviously not up to their task of keeping the pelvis in neutral position and prevent it from tilting into adduction.
However one explains the weakness of the abductors in the juvenile arthritis, it is nevertheless a fact. It offers us an explanation for the similarity of the gait of coxitis deformans and congenital dislocation of the hip and makes us realize that the limp, as reported by the parents of our patients, was more pronounced when the children were fatigued, i.e. when the already weak abductors failed completely.
Differential diagnosis
The similarity of the symptoms with those of coxa vara and coxitis deformans is evident. In both cases we find limitations of motion only in certain directions, while in the rest movement is not only feasible, but also painless, and a high trochanter develops. In both affections we frequently have spontaneous pain, which occurs after considerable exercise, and sometimes radiates to the knee. On the other hand, in both affections we may fail to observe pain of any kind. Considering that both affections involve juvenile individuals whose illness has evolved very gradually, it is obvious that in many cases the two conditions cannot be distinguished by ordinary clinical examination. If there is no marked crepitation indicating deformation of the femoral head, which is rare in juvenile arthritis, then the differential diagnosis can be made by x-ray with certainty. The differential diagnostic symptom specified by Maydl – i.e. the shift of the trochanter towards the midline of the body and reduced size of the relevant half of the pelvis in arthritis deformans, the corresponding increase in coxa vara – is not useful not only because the coxa vara, as emphasized by Hofmeister, behaves very inconsistently, but also because in the early stages of arthritis deformans, in which only a flattening of the upper cap of the femoral head develops, the trochanter is not shifted towards the median line, and the sizes of both pelvic hips do not necessarily exhibit a measurable difference.
The juvenile arthritis is more or less similar to congenital subluxation with respect to the gait pattern, the positive Trendelenburg sign, and the elevated trochanter, but hardly ever the differential diagnosis is seriously questioned, as the history of juvenile arthritis deformans indicates that the children walked normally without limping in the early stages of their development. In the early stages of the arthritis the trochanter elevation is not as pronounced as in congenital dislocation.
In contrast, a confusion of the presently interesting affection with tuberculous coxitis cannot be fully excluded. However, the differential diagnosis will be made most often based on the fact that in tuberculous coxitis movement is inhibited by muscle tension in all directions, rather than an absolute bony restriction in a few or only one directions; furthermore, the painful movements, the tenderness of the joint, which is absent in arthritis deformans.
Doubts are possible as shown by a case published by Alban Köhler as “Coxitis with bony origin in the caput femoris”, which I cite here because the perfectly reproduced radiography has very far-reaching similarities to our cases: 9 year old boy whose mother died of phthisis (tuberculosis) 4½ months earlier. No complaints, normal mobility except for limited abduction. The patient had not the slightest pain even at the maximum effort, with pressure on the joint region, with strong blow to the foot sole. Shortening of the leg by 1 cm. Strong suspicion of coxa vara. Coxitis is being considered, but considered very unlikely. Radiogram: dorsal view. Generally normal calcium content in all bones. Acetabulum apparently normal, as well as the irregular contour of the cranio-posterior acetabular rim regarded as normal with a sharp tear drop. Normal femur except for femoral epiphysis which shows a generally normal mineralization, but is squeezed flat with irregularity of its periphery and a bright spot medially. The same seems to communicate with the joint space. On the basis of the radiograph it was assumed, this is a case of ossale coxitis, that a circumscribed spot approximately perpendicular to the epiphyseal line is a fungal focus is resp. (sic) that the bone is decalcified here by fungous masses. The spot has not yet penetrated into the joint, as far as can be seen in the clinical findings. On the X-ray image there is a very thin cortical layer between the spot and so-called joint space, but even if they would not exist the articular cartilage above the spot may not be penetrated. “After months of immobilization and then a Hessing’s walking cast the process was completely halted. 15 months later: The same clinical findings, complete mobility with moderate limitation of abduction. X-ray: The epiphyseal head is even flatter and looks slightly fissured, almost divided into individual pieces. Yet even here the clinical findings suggest that a penetration into the joint may not have occurred.”
In such a case, based on the experiences acquired in the last years, I would not hesitate a moment to diagnose coxitis deformans rather than tuberculous coxitis in spite of the phthisis of the boy’s mother. I have never seen a tuberculosis coxitis existing for months without causing tenderness or pain on movement. The normal range of motion except for limited abduction is characteristic of arthritis deformans juvenile, not tuberculous coxitis. In Koehler’s case the diagnosis was not made from the clinical findings, but from radiographs. However, almost exactly characteristics occurred in the X-ray images of our cases 1, 2 and 4. However, the fact that the presence of foci of subchondral bone loss has easily led a shrewd X-ray diagnostician as Alban Köhler make the diagnosis of tuberculosis, without considering the possibility of arthritis deformans juvenilis, causes me to point out the occurrence of subchondral lesions in arthritis deformans.
Course (of the disease)
If we try to get a picture of the course of juvenile arthritis, the most important finding is the steady progress of the pathological-anatomical changes. There is no case with long followup in which there is a stalling of the process with relatively minor changes. In our cases followed longer than one year with repeated radiographs the progress of the deformity was unmistakable without exception, especially in the earliest cases.
The pace of progress may vary. An example of a relatively rapid development is the first case of Maydl. The patient was completely healthy until she was 14 years old and fell down about 6 steps on a staircase on her right side. After the fall, she noticed that the right foot was a little shorter, and with prolonged walking, she had moderate pain in the middle of the right thigh. Only 14 days later did the pain localize in the right hip. A year later on clinical examination, and subsequent resection revealed significant changes in the hip joint: substantial expansion and extension of the acetabulum anteriorly and superiorly, patchy cartilage loss, significant deformation of the head with flattening, widening and lengthening, so that it projected a pear shape perpendicular to the surface with narrowing at the top. On the contrary, the following cases were slow to develop. The patient of v. Brunn, for example, who got the disease at 16 years of age was still working at the fire department from age 18–20 years and came to the clinic at age 23. Axhausen’s patient began suffering about age 20 but by 30 had no major problems, and only then began to have a rapid deterioration, with increasing problem with his gait, and at age 35 surgery was necessary. The patient of Guhl also exhibited slow, apparently steady development of suffering from age 7 to 36. Most likely the period over which the disease extends will be short if trauma does not mark the start of the pathological changes, for the first start of the pathological changes occurs in a proportion of cases without symptoms but already not inconsiderable pathological changes were present when the first symptoms led the patient to the physician.
Despite a steady increase of the bone deformation, an escalation of the subjective discomfort of functional impairments does not always occur in parallel.
Despite the progress of the pathological process on the radiographs, the initial pain may disappear spontaneously, at least temporarily. Our cases 1, 2 and 3 offer proof. von Hofmeister observed a young girl that at age of 15, fell ill with hip pain, then was pain-free at a follow-up after 3 years, but nevertheless with increasingly limited motion. On the other hand, it is also possible that pain appears later after a long pain-free initial period. Such was the case in the 34 year old female patient of Hesse who up to 30 years of life had been free of symptoms, apart from a minor limp, and only gradually began to have increasing pain her left hip after prolonged walking or standing.
The limited motion can decrease at least temporarily despite the increased deformation. One could observe in our cases 2 and 3 after a year that the initially limited abduction was restored to a considerable degree. The progressive destruction apparently removed the bone that had originally inhibited the motion. A healing of the pathological process, however, is not proven by better function. The functional improvement may well represent only a temporary stage, and if one follows the patient over even greater periods of time, it will probably always be noted that despite the temporary improvement there will be overall progression of the disorder, such as that in the case Hofmeister observed over 3 years. In the final stage that we encounter, for example, in Axhausen’s observation, massive bone growths that form around the head, cause an almost complete fixation of the joint, without a coalescence of head and acetabulum as in a true ankylosis. Whether all of our cases over the years or decades will meet such a sad end stage, is not proven, but must be presumed with the available material as probable.
It appears not uncommonly that after the illness of one hip joint, disease in the other follows. Therefore, the temporary pain in the other hip of our patient No. 3 that is not proven to be affected is at least suspicious. When the right hip joint was resected in case 1 of Frangenheim, small bone growths were detected in the junction of head and neck in the other/contralateral femur in the X-ray image. In the patient of Hesse, who sought care only because of discomfort in the left hip, X-rays detected an already quite considerable deformity on the contralateral hip.
A participation of other joints apart from the hip joints has not been observed in juvenile arthritis deformans with the exception of a single case1.
The lack of a disease progression from one joint to the other, as highlighted by Wollenberg, is a characteristic that distinguishes the arthritis deformans, not only in the juvenile form, but also from the chronic rheumatic polyarthritis in the same way as the peculiar pathologic-anatomic findings.
Therapy
Reported experiences of treating juvenile arthritis deformans are sparse. Several times treatment by traction has been attempted: v. Brunn, case 1; Zesas, Hofmeister, Fridberg. Notable success was not achieved. Nevertheless, Zesas and Hofmeister observed a rapid reduction of pain during traction application, but the pain reappeared in both cases after a while; in Zesa’s case it was not influenced by repeated application of the traction whereas in the case of Hofmeister the pain disappeared again without treatment and with the patient resting. Unfortunately the traction was applied for one month in the case of v. Brunn. Even though the gait before the traction was indeed difficult and the patient fatigued quickly, after terminating the extension “he was able to walk a few steps only with great pain and his gait was much more awkward than previously. Only a vigorous treatment with gymnastic exercises, and light baths, caused improvements.” One cannot say that the available evidence justifies more experiments with extension treatments.
It is certain that immobilization, including traction have an adverse effect in older patients with arthritis deformans. It suggests that the conditions in the juvenile form of this disease is not significantly different. We saw in our cases that the restriction of movement developed primarily in the abduction movements while repetitive flexion movements during walking maintained their path. Therefore, it is conceivable that with passive movements, either manual or with a medico-mechanical apparatus, the formation of bony restrictions can be prevented or reduced. Even though the process in the bone cannot be stopped, at least we can hope that through remodeling the joint develops in such a way that it allows extensive movement excursions. It is advisable to support such medico-mechanical treatment by massage of the atrophied hip muscles, particularly the abductors, as well as by appropriate bath treatments. The recommendation of a systematic movement therapy appears even more justified as passive movements are painless, even in those cases with spontaneous pain. A loading of the joint, which could act to advance the deformation, does not occur in these passive movements.
Unfortunately, we were not able to carry out such a systematic treatment in our cases because all six patients were living far away from Leipzig. We had to content ourselves to prescribe an imperfect massage by parents and mud baths. We determined that full freedom of movement that we allowed for the children did not cause any harm, and that even in some of the cases the movements became less limited in spite of the progress of pathological changes during therapy and spontaneous pain disappeared. After our experience, even when the pain is greater than that in our patients, I would not follow the recommendation of Bibergeil to apply a plaster walking cast and would rather recommend passive motion and perform massage while resting in bed if walking was not tolerated without pain.
There is general agreement that resection can be considered in case of high-grade walking pain, i.e. in late stages of the disease. In these cases Küster and Riedel achieved healing “with mobile, well-functioning joints”. The patient operated by Küster was able to walk up to four hours without an assistive device two years after surgery. In the resection cases of Maydl, Negroni, and Frangenheim nothing is reported about the final outcome.
The operative modeling of the femoral head, as performed by Axhausen in his 35-year old patient with an arthritis deformans that arose in his adolescence, appears very efficient. The very pronounced bone masses were chiseled off and the head was reconstructed to normal size and shape and repositioned in the acetabulum. At discharge from the hospital movements in the right hip joint were markedly increased especially in flexion as compared to before surgery. However, this operation will be reserved only for the late stages of the disease.
Etiology
Finally, if we consider the etiology of the juvenile arthritis deformans of the hip joint and the concepts of this disease, we only propose hypotheses and can do nothing but test these unproven opinions.
In his last edition of the handbook of practical surgery Hoffa remarked that juvenile arthritis deformans of the hip occurs only after a trauma. Hoffa would no longer agree with this statement. However, it appears proven that in young individuals arthritis deformans can occur after a mild or severe trauma in the hip as well as in other joints, such as occurred in the case of Küster-Zesa, immediately following repositioning of a hip dislocation. In any case, trauma relatively rarely plays an etiologically important role. Among our 6 cases five denied trauma with certainty and in only case was I told that the limping occurred after the child was shoved into a ditch when throwing snowballs. However, injury sequelae were not found in this child on medical examination the next day. As in the other 5 patients, at the time of disease onset the child had not missed school.
If we survey existing literature, among the 12 cases of bilateral disease a history of trauma is mentioned three times, but in v. Brunn’s case he appropriately concludes there was no indication that the minor trauma, which occurred 1/2 year before the onset of the disease, had any relations with the hip disorder. Frangenheim maintains in his case 1, “considering the changes found at operation 4 months after the trauma it is more likely that the disease has existed for a long time before the trauma.” In the case of Bibergeil’s 11 year-old patient, the child had fallen from the high bar in gymnastics and was able to walk home, but during the night pain developed. Later a plaster cast was applied for 4 weeks but after its removal the girl limped permanently. From the outset it is unlikely that such a slight trauma should have seriously damaged both hips.
Among the 26 reported cases of unilateral disease in six (Küster-Zesas, Riedel-Zesas, Maydl, Immelmann, Schmidt, our case 1) the disease can be related with a certain probability to previous trauma2. In the large majority of cases of juvenile osteoarthritis deformans the trauma therefore played no significant role in etiology.
G. Smith stated that as a result of a contusion of the epiphyseal plate on the proximal femur in young individuals, there may be gradual slipping of the femoral epiphysis. Consequently the top portion of the femur slips forward so that a coxa vara develops, while the nutritional disturbance of the epiphysis generates degenerative processes with the appearance of coxitis deformans. One cannot deny that this combination of traumatic coxa vara and joint inflammation as observed by Schmidt may occur occasionally. But it has to be denied that the slipping of the head of the cartilaginous cap due to contusion in juvenile arthritis is the rule, as Schmidt assumes, because by far the majority of cases with juvenile coxitis deformans have no history of trauma. Furthermore, our X-rays show that a formation of a traumatic coxa vara after slipping of the intermediate cartilage is not the case. The top cap was reduced in height and slightly deformed, but it was not shifted downward and forward.
The opinion of Preiser, who ascribed the development of chronic joint inflammation to the joint incongruity, has played a recent role. If the cartilaginous part of the femoral head protrudes from the acetabulum, thus losing contact, then the protruding part will, according to Preiser, be damaged by non-use such that a deforming arthritis results. According to Preiser the cause of the incongruence is primarily related to the acetabulum in an aberrant position and consequently a high position of the trochanter, but there are also incongruity created by femoral neck fractures with healing in a displaced position, by coxa vara, by congenital deformity of the femoral head, and finally by resorption processes of the head and the acetabulum.
I therefore checked our material to see if one of the forms of joint incongruity suggested by Preiser were present. In four cases (1, 2, 4 and 6) we found a trochanter height no greater than 1 cm in the affected hip on the initial observation. This trochanter elevation is too small to suggest incongruence in the sense suggested by Preiser. Preiser himself (Deutsche Zeitschr f. Chirurgie, Volume 89, page 550) considered trochanter heights of 1 cm in children and 2 cm in adults to be negligible and did not consider them when calculating the percentage of patients with a normal hip and the trochanteric elevation. In our two remaining cases, 3 and 5 the greater trochanteric height was not associated with an abnormal acetabulum position. Rather in case 3 it was attributed to the loss of the head and apparently simultaneous expansion of the acetabulum, therefore was not, as Preiser assumed, the cause but rather the consequence of arthritis deformans. In case 5 both sides had severe reduction of the femoral neck angle and hypertrophy of the trochanter which were a sufficient explanation for the elevation of the trochanter. There is no reason to assume an abnormal position of the acetabulum with a subsequent incongruence. I do not believe that the coxa vara3 in case 5 caused the incongruence and coxitis deformans because of a similar extension of the femoral neck angle on both sides, but the deforming arthritis was only present on one side.
Finally Preiser interpreted the barrel-shaped deformity of the femoral head found in a 35-year-old man with juvenile arthritis as a congenital anomaly, although this has not been previously described as a cause of incongruence and thus should be considered as arthritis deformans. While considering our first case (2) I was also initially inclined to consider the abnormal shape of the head as a congenital deformity which allowed flexion without any restriction but limited abduction. However, considering that the boy’s limp undoubtedly occurred with the joint deformity only in recent years, I decided against this interpretation. In later observations in case 1 we observed during our observation period the evolution of a nearly normal shaped head of the femur into a similar cone shape as a result of deforming arthritis, as it had appeared in the initially observed case as a congenital deformity. I therefore regard this roller or cone shape not as a congenital malformation, but rather a result of arthritis deformans, as is so often observed in a similar way in arthritis deformans in older patients. I do not agree, as Preiser writes, “that such a severe deformity of the head can, as in Preisers’ case, develop over 1/2 year with only temporary pain in the hip from arthritis deformans coxae “. As we observed in our case 4, it seems not a common experience that arthritis deformans can occur without any pain at all and yet already caused a severe deformity of the femoral head. Altogether, we have found in our material no evidence that arthritis deformans is the consequence of incongruence.
Hesse considers his cases to be the result of an underlying nerve disorder, but as Hesse emphasized, the absence of any of other nervous symptoms like motor, sensitive, trophoneurotic, vasomotor, and reflex characteristics, shows that such an interpretation is purely based on a hypothesis.
The same could be said of Okada’s new view. Okada found in 3 patients suffering from arthritis deformans of 53, 50 and 17 years of age, the signs of infantilism, a phenomena reminiscent in some respects to myxedema, particularly the disturbed development of the thyroid gland and the genitals as well as reduced intelligence. Okada now considers arthritis deformans as a secondary disease due to the failure of a gland of internal secretion which is a phenomenon as part of infantilism. One cannot say that the material to support this new theory gives the impression of great supportive value. In his first case, Okada justified the diagnosis of arthritis deformans neither by palpation nor by X-ray. In the second case the evidence of an ankylosing hip disorder is associated with a very brief report on one “X-ray from an external radiographic lab”, which the author no longer had at his disposal anymore. In the third case, that of a 17 year old patient, bilateral arthritis deformans was undoubtedly detected by X-ray. But convincing evidence is lacking that the disease which occurred in the 7th year of life with pain in the hip joints, forced the previously healthy patient to lie in bed for a long time and was treated by a doctor as arthritis deformans; this disease was likely a result of arrested development, and not just randomly combined with developmental disabilities. Of course one still must consider the coexistence of such diseases. So far, nowhere else is a single case of arthritis deformans of the hip the phenomena of “infantilism” reminiscent of cretinism were observed.
Bacterial infection is considerably more important in the etiology of juvenile arthritis deformans.
The boy who was transferred to us in his 13th year with a right-sided deforming hip joint inflammation (case 3) had been treated in the Leipzig outpatient clinic for “osteomyelitis femoris dextri” at 10 weeks of age. The phenomena, at that time well-observed by the parents, securely indicate a finding of acute inflammation of the right hip joint and make it at least probable that the clinical diagnosis of osteomyelitis of the proximal femur as a cause of arthritis in infancy was indeed correct. An abscess had not occurred. The disease was treated indifferently and in 5–6 months the problem resolved and from then on the boy behaved perfectly normal in every respect until the age of 10 years as the first symptom of the present disease a limping gait was observed. Despite the long interval, we believe that the arthritis deformans in this case was most likely due to the acute inflammatory disease in infancy.
It is known that in infancy an osteomyelitis of the proximal femur can occur in a similar mild manner as in our case. Mohr suggests that hip joint osteomyelitis occurs relatively commonly in infants with a slow course of localized bone thickening and a tendency to spontaneous absorption and he reported such a case in which the position of contracture of the hip, pain on movement, and thickening at the upper end of the femur, led to the diagnosis of osteomyelitis involving the hip joint; in the course of about 3 months complete healing occurred without an abscess. It speaks much for the Mohr’s presumption, that the cases of acute infantile arthritis described by Drehmann developed from primary osteomyelitis of the epiphysis with secondary involvement of the joint.
Drehmann showed that subsequent deformities of the hip joint, especially pseudo-congenital luxations and coxa vara, sometimes develop as a consequence of joint infections in infancy. Preiser also previously published an observation of coxa vara with peculiarly deformed femoral head epiphysis. Even if the disease is not as directly described as arthritis deformans, the assumption as in our case 3 that the deforming arthritis is due to acute illness in infancy is consistent with the above observations.
The long interval which separates the beginning of the arthritis deformans from the acute disease in the first years of life is striking. However, this observation is not without precedent.
In Axhausen’s case we have every reason to believe that scarlet fever and diphtheria in the 6th year of life initiated the disease. A waddling gait persisted with swelling of both hips and a right thigh abscess, but the movement was good in both hips again until 20 years of age when the signs of arthritis deformans appeared in both hips.
Wollenberg even suggests that “arthritis deformans is particularly likely to occur as a sequel to long-past infections. These cases are all characterized by the long and varying intervals of time between the original disease and the onset of arthritis deformans.” In the hip Wollenberg has even observed that a case of acute inflammation of the hip joint in typhoid abdominalis, in which a limp was present for six years, but then the patient’s gait was completely normal for 14 years until the first symptoms of arthritis deformans began. Hoffa and Wollenberg reported a case of tuberculous coxitis in a 5-year old with an apparently complete cure, but 20 years later the same joint developed arthritis deformans.
In any case, we will not be able to doubt the interesting possibility that the arthritis deformans juvenilis is attributed to a hip joint infection in infancy that apparently healed without consequences.
As an example of arthritis deformans as a follow-up disease of acute hip infections the cases of Borchard can be considered which are often cited in the literature as arthritis deformans juvenilis. In their youth, Borchard’s three patients were suffering from symptoms suggestive of osteomyelitis of the hip. The condition developed into a slowly progressive chronic hip disease. Borchard found all the signs of arthritis deformans by femoral head resection, but he also found “residuals of subchondral inflammation”, “…old inflammation foci,” which caused him to come to the pathological-anatomical diagnosis of osteomyelitis and not arthritis deformans. Since Borchard certainly rejected the diagnosis of arthritis deformans, his cases have to be removed from the observation material of juvenile arthritis deformans. However, subchondral softening of the femoral head as have also been observed in arthritis deformans, and it would be unfortunate to try to reinterpret Borchard’s diagnosis of his own preparations. Borchard goes too far when he says that all cases of arthritis deformans juvenilis with non-traumatic origin can be ascribed to a “confusion with osteomyelitis, since we certainly know that there are only a few observations of traumatic juvenile arthritis deformans of the hip.” There can be no doubt that my six cases are certainly cases of juvenile arthritis deformans of the hip joint, but in only one of these cases does trauma as an etiological factor comes into question.
How shall we now consider the cases in which neither a trauma nor an infection can be established as an initiating moment, i.e. the group to which our observations on cases 2, 4, 5 and 6 belong? It is quite conceivable that in these cases of mild inflammation of the hip in infancy existed without their parents and other relatives remembering. This cannot be proven.
After all, many factors speak in favor of Wollenberg’s assumption that the group of “idiopathic juvenile arthritis deformans” that still must be distinguished will merge more and more with the various groups of secondary arthritis as we learn more.
Wollenberg considers the changes of the minor bone vessels (end artery obliterans) and venous congestion that he demonstrated as the etiologically most important pathologic finding. These changes are induced by various causes, but according to Wollenberg cause in the same way the picture of arthritis deformans by the arterial occlusion in the bone and the congestion leading to proliferation processes. The pathologists must verify this theory that the occurrence of arthritis deformans is due to various causative factors such a trauma, nervous affections, and bacterial infection. The finding of destruction within the femoral epiphysis on the X-ray images of our early stages of juvenile coxitis is at least consistent with Wollenberg’s idea.
Let us finally summarize the findings of our observations in a few sentences:
The frequency and practical importance of the juvenile arthritis deformans of the hip joint is greater than it appears from previous publications. (Six of our own cases within one year!)
In the majority of cases of coxitis deformans juvenilis, trauma cannot be considered as the etiological factor. In our cases there was no evidence for the assumption of an incongruency (Preiser) as the cause of the disease. In one of our cases the arthritis deformans was likely attributed to an acute bacterial infection of the hip joint in infancy but the first symptoms of the disease appeared only after a symptom-free interval of several years.
The first pathologic alteration in the arthritis deformans is the flattening of the epiphysis of the (femoral) head. This often leads to a characteristic cone-shaped deformation of the femoral head. The gradual increase of the height reduction of the epiphysis can be followed in serial x-rays. The x-ray certainly indicates that during the deformation of the femoral head, nutritional disturbances within the epiphysis are significantly involved leading to regions of subchondral resorption.
The movement limitations of the juvenile arthritis deformans are a direct mechanical consequence of the joint deformation. The limitations are – at least in the early stages of the disease – in different directions. The cone-shaped deformation of the femoral head causes a limitation or restriction of abduction and rotation with free flexion.
Pain is not caused by active and passive movements of the joint or by pressure. Spontaneous pain, however, occurs especially after extended walking and is often experienced in the knee. Nevertheless, there are cases of high-grade deformation without any pain.
Crepitation can only be found in a small fraction of cases.
A limp, which usually is the first symptom of the arthritis deformans juvenilis of the hip joint, is due to an insufficiency of the abductors as with congenital hip dislocation.
Diagnostic confusion of the coxitis deformans with coxa vara or tuberculous coxitis cannot be prevented.
In the currently followed cases a slow but continuous progression of pathologic changes was observed. Despite this progression, the limitation of movement and pain can resolve spontaneously at times.
Immobilizing bandages should not be used for treatment. Systematic passive mobilization and massage are advisable especially for the abductors. For cases with far advanced bony changes an operative modeling of the femoral head or a resection can be considered.
Appendix I – Case Histories
Unilateral Cases
1. Ida A., age 8.4 Parents and three siblings live and healthy. From previous diseases, especially symptoms of rickets are not reported. 7 year old child was kicked while throwing a snowball into a ditch, but was not in bed, a doctor who examined the child the day after the fall “found nothing.” Soon after, his parents noticed the child was limping. There was moderate pain in the left hip which disappeared after a few months. The child is brought because of limp. There is no pain even after prolonged walking.
Status April 26, 1909. Child is weak but shows no standing deformity of the spine. While walking and stepping on the left leg the upper body sways to the left every time. In the recumbent position both hip joints normal. Real shortening of the left leg. Anterior superior iliac spine – external malleolus right 61.4 cm, left 60.6 cm. Tip of the right trochanter almost 1 cm, left almost 2 inches above the Roser-Nélentonschen Line. No palpable deformity of region of the hip. No tenderness on pressure over the trochanter or the femoral head. Normal movements on the right. Left extension and flexion free. Adduction to 20° is possible and abduction completely abolished. When attempts at abduction the pelvis moves with it immediately. External rotation in extension is not limited, internal rotation is completely eliminated. All movements, if they are possible, are without pain or crepitus. The radiograph (Fig. 1) shows slight flattening of the femoral head in its upper and medial part. The acetabulum points directly below the center of small irregularities of the boundary line, flat prominences according to the cavity.
Fig. 1.

Case 1. 8 year-old girl. Left Hip on April 26, 1909
Status June 12, 1910 In general similar to 14 months before. The limp has not become greater, no pain, but now leg length from the anterior superior iliac spine – external malleolus right 64.2, left 63.2. On the left diseased hip joint, free flexion, abduction absent, adduction to 10° possible. In flexion, the thigh is in an approximately 30° abducted position, from which he may be abducted or adducted further. Outward rotation in flexion to 60° possible inward absent. When standing on the left leg, the right half of the pelvis drops significantly down to the inclination of the upper body on the left (positive Trendelenburg sign). X-ray image: the flattening of the head has increased in the upper portions. The height of the epiphysis of the head has decreased from 16 mm to 10 mm. In place of the spherical shape of the head, the shape has entered a truncated cone. In the epiphysis in the whole thickness of the epiphysis shows irregularly defined bright spots. This suggests the normal bone part is missing.
2. Eugene H., 11 years. Parents and four siblings healthy. The boy himself was always weak, but never seriously ill, especially not from rickets. At the age of 9 years, he often complained about pain in his right hip, and, “went lame at times.” January 1909 the parents noticed an increase of limping. The pain in the region of the right hip varies in intensity, usually only slight and but for days painfree.
Status February 1, 1909. When standing, slight left convex lumbar scoliosis. Region of the right trochanter more prominent than on the left. Left anterior superior iliac spine is lower than the right. The boy is always bent left and stretches his right knee, with left knee in extension as the right heel rises from the floor. Limping slightly. When stepping on the left leg the trunk seems to sway more each time. Lying down the right leg is adducted by 10° and with similar abduction on the left. Right heel, right malleoli, etc., are about 5 inches higher than the left. Leg length from the anterior superior iliac spine – external malleolus, right 63.5, left 64.2 cm. Right trochanter almost 1 cm above the Roser-Nélentonschen line, left the same. No palpable abnormality of the hip area.
No pain, either by pressure on the joint or on the trochanter with impact against the heel in the longitudinal direction of the leg. Movements: flexion and extension movements in the right hip joint active and passive, totally free and painless, however, abduction and abduction and rotation completely absent. Even with little shaking the pelvis immediately moves. Left has completely free movements.
X-ray (Fig. 3). The femoral head to the right shows the distinct shape of a cone or sugar loaf wide. The rounded tip of the cone is exactly opposite the center of the acetabulum. The conical shape of the head is due to the fact that the proximal epiphyseal line at the location of the head which contrast to the perfectly normal conditions on the other side. The distal location of the epiphyseal portion of the head and the femoral neck and shaft appear left and right, especially with respect to the normal angle of the femoral neck.
Fig. 3.

Case 2. 11 year-old boy. February 11, 1909
Status June 12, 1910. The boy received salt baths, but otherwise remained without treatment and has in spite of intermittent pain regularly attended school. The pain presents itself only after some time, several hours of walking, but also after prolonged sitting at school, but appears to have eased in recent months. The limp is especially noticeable when the child is tired. The status differs from the previous years only in that when lying there is adduction of the right hip to compensate for the tension on the right leg. It is now up to 20° abduction, adduction to 30°, rotation to 15° in either direction possible, flexion is still completely free. Limb length from the anterior superior iliac spine- external malleolus, right 66.0 cm, left 66.9 cm. No tenderness, no pain during motion. Pelvic brim to the prominence of the trochanter measured on both sides is the same (31 cm). When standing on the right leg, the left half of the pelvis is lower by 2–3 cm below the horizontal (positive Trendelenburg sign). Nevertheless, despite freer movements in the past few years, X-ray image (see Figs. 4 and 14) now shows severe changes in the right hip: The flattening of the femoral head in its upper sections has increased, the proximal to the epiphyseal location of the head, the epiphysis has not increased, but rather in the last few years its former height of 12 decreased to 8 mm! The epiphyseal line now shows significant irregularities with several large bright regions, suggesting bone loss. Regions of the epiphyseal plate extend into the femoral epiphysis. The femoral neck and trochanter are unchanged. Normal structural drawing clearly visible. Left hip still shows normal radiographic findings.
3. F. Ernst, 13 years. Healthy parents. Of eleven children he suffered more neck gland swelling. According to precise information from the parents, at the age of about 10 weeks, he fell ill suddenly with heavy sweating and fever. The right leg was held in the hip joint rigid. “Any attempt to stretch the legs, caused the child severe pain.” The child was born on 6 August 1898 at the Leipzig University Clinic of Surgery. In the outpatient clinic of the journal entry is found: right femoral osteomyelitis. Therapy: lead lotion. According to the parents and a splint was made. The illness lasted about 5 months after complete healing was observed in the clinic. The child, “learned to walk at the age of 2 years.” There were no noted subsequent consequences of the disease. At the age of 10 years, the boy began to limp, however, and later to complain about pain after prolonged walking in the right leg. The right-sided inguinal glands were swollen considerably. Nevertheless, the boy went to school and after the first years of life was never been treated medically. There was no history of injury.
Status June 5. 1909. Well-developed boy looking healthy. At present no subjective complaints. He occasionally complains of pain in his right leg that causes him to stop but not to participate in the running games of his friends. When standing, there is a low convex right lumbar scoliosis, lumbar lordosis very slightly greater than normal. The pelvis is tilted with the right anterior superior iliac spine lower than the left. While walking, the torso tends to sway when the right leg to the right. In a reclining position of the pelvis and both hip joints normal. Real shortening of the right leg. Leg length from anterior superior iliac spine-external malleolus, right 67.4 left 69.4 cm.
Corresponding elevation of the right trochanter. No palpable deformity of the hip joints. The right hip is a bit sensitive to pressure. Pressure on the trochanter and slight impact in the longitudinal direction of the leg are sensitive. In the right groin are fairly hard, painful lymph glands, some the size of beans. Movements: in the right hip abduction by only 25° possible, adduction, flexion from 25° through a right angle of about 100° with internal rotation in the extended position 15° and 15° external, making a total of 30°. The movements are carried out without pain and without crepitation. Left hip is all normal movements. The radiograph (Fig. 7) shows that the right femoral head has largely disappeared. As is clear from the position of the epiphyseal line on initial impression, there is an impressively flattened head, perpendicular to the larger structure to wider part of the femoral neck, just in its uppermost sections of the small remains of the head cap. The height of the head and neck of the femoral intertrochanteric line on the left side is 5 cm, it measures only 3 inches to the right. Therefore the greater trochanter and the femoral axis have shifted by 2 cm from the inside to the acetabulum. The normal upper femoral neck-shaft angle has been lost. The rest of the head is nearly in the extension of the axis of the femur. On the head can be seen lateral bone “osteophytes.” The acetabulum is flattened and widened and above (with incipient enlargement of the acetabulum). The left hip is completely normal.
Fig. 15.

Case 3 on March 16, 1910
Status June 12, 1910. The treatment has consisted of saline baths and massage of the gluteal muscles. At times, the boy had no particular cause of pain in either hip, despite the disease, but the pain in recent months had rather increased. The boy has not missed a day of school in the past year. Very slight limp. Upper body leans when stepping on the right leg to the right. When standing on two legs, the right spine is lower than the left, the upper body tilted slightly to the right (shortening of the right leg). When standing on the right leg, the left half of the pelvis drops slightly below the horizontal, while standing on the left (healthy) leg, the right half of the pelvis in the normal way, rises above the horizontal (positive Trendelenburg sign). Periphery of the right buttock reveals prominence of the trochanter, measured 34 cm, 37 cm to the left. The right gluteus region is flattened and the muscle feels flaccid compared to the left. Leg length anterior superior iliac spine – external malleolus, 71 right, left 74 cm. Right trochanter almost 5 cm, left 1½ inches above the Roser-Nélentonschen line. With heavy pressure from the front there is little tenderness in either hip.
Movements: flexion to 100° possible. With strong flexion there is about 20° from abducted position, abduction to 30°, 30° adduction possible. All movements are without pain and without crepitation. Rotation in a flexed position not possible.
One the left few restrictions of motion: abduction to 50°, abduction to 25° are possible, with free flexion. Radiograph of the right hip 15 (taken on March 16, 1910.): The deformity of the right hip joint has increased. The osteophytes on the head are larger. Between the upper osteophytes of the head and the greater trochanter seems to be developing a connection. Those, “migration of the acetabulum” has progressed by ½ inch. The left shows some irregularities in the acetabulum base which may or may not be normal.
4. Alfred R., 13 years. Other than measles, the boy has had no serious no illnesses, and in particular not rickets. Neither the mother nor the boy are aware of any injury. Three fourths years ago it was noticed that the boy, “became lame.” There is no pain. The boy takes part in all running sports, but tires quickly. He apparently felt fatigue only in the left leg.
Status March 14, 1910. Normally developed boy. When standing, when both legs are kept straight and the spine, the left heel very slightly raised so that the body burden rests largely on his right leg.
While walking on the left leg, the upper body leans slightly to the left. Supine the left hip is adducted 7°. Real shortening of the left leg by 1 cm. Distance from the anterior superior iliac spine-external malleolus, right 75.5, left 74.5 cm. Apex of the left trochanter 1 cm above the R. N. line, while that of the right is at most 0.5 cm above this line. Pressure on the trochanter, and strong impact against the heel does not hurt, the boy jumps off a table without pain. Only strong pressure on the head from the front left leg is sensitive. Movements in the right hip joint: totally free in the left hip with complete flexion and extension, but at the beginning of each active and passive flexion there is some resistance, which is then overcome. Abduction and adduction active and passive completely absent. Rotation in extension only in very small extent around 20° is possible, in a rectangular flexion rotation absent.
Fig. 16.

Case 4 on June 7, 1910
The x-ray shows the left femoral neck, trochanter, and shaft and is unchanged. Femoral neck angle is normal. Significant deformity of the femoral head. Flattening of the upper and the medial portion, which abut one another both obtuse at an approximately corresponding to the center of the head surface location at an angle. Very irregular epiphyseal line. The distance from the epiphyseal to the surface of the head measures only 8 mm. (The same measure on the healthy side of 20 mm.)
Acetabulum face flat and not very regular, small extension of the acetabulum to the top. The radiograph of the right hip joint is completely normal.
Status June 7, 1910. Findings generally unchanged. Absolutely no pain when walking, running and jumping – despite considerable deformation of the femoral head. On the left side the pronounced limping gait is very similar to that of a congenital hip dislocation. Each occurrence standing on the left foot causes the upper body to lean to the left. When standing on the left foot with the right leg raised the right hemipelvis drops down so that the anterior superior iliac spine is at least two finger-breadths lower than on the left (positive Trendelenburg sign). When standing on the right foot to the left buttock lifts in the normal way, so that the left spine is at least two fingers’ breadth higher than the right. Movements same as on March 14th. Flexion-free. Abduction absent. But compared to the previous low (7°) adduction, the leg is now adducted in adducted position by another 20°. Measurement of the circumference of both halves of the pelvis at the greatest prominence of the trochanter major results are left 37.7, right 38 cm. The right gluteal muscles appear slightly atrophic.
5. Minna G., 13 years. Parents and six younger sisters are alive and healthy. The girl has for a long time, suffered with “neck glands,” but apparently not the English disease, has learned to run over the past 1½ years. At the age of 12 years, the child began to limp with no known cause. She had suffered no injury and never missed school. Now pain is only intermittent – when the child has walked for more than half an hour – but usually the child is completely painless.
February 10, 1909. Strong, well developed child with scars on the right side of the neck arising from tuberculous lymphatic glands.
Standing: slight normal lordosis of the lumbar spine. Both spines equal. Left foot is held slightly inwardly rotated. In the lower third of both lower legs varus bowing. The gait is similar to that of a left-sided congenital hip dislocation. With each step on the left leg, the upper body leans to the left side. Lying down: Position of both legs at the hip in flexion and abduction is normal, however, the left leg at 45° flexion is rotated inward. Slight shortening of the left leg compared to the right. Anterior superior iliac spine – external malleolus, left 66 cm, 68 cm right. Left trochanter at 5.5, and right 3 cm above the R. N. line. Both trochanters are massive by palpation. No tenderness of the hip joints, no apparent atrophy of the thigh muscles. Movements: Right hip joint. Flexion and extension completely normal. Abduction to 30°, adduction to 40° possible. Rotation in extension is free but in right angle flexion only 45° is possible. The magnitude of the side opposite to the abducted leg in the air can be obtained without difficulty.
Left hip: flexion possible only to 80°, abduction absent, Adduction to 40°. Rotation (of the limb) causes rotation of the pelvis. Upon flexion of the hip, the leg is held in marked adduction. Sometimes hip movements cause loud left hip joint crepitation. The left leg is in the right lateral position, insofar as permitted by the absent abduction, are kept under misalignment of the pelvis raised against the affected side.
Radiograph of the right hip joint (Fig. 12): Head and acetabulum normal. Femoral shaft very thick. Femoral neck angle of 115°. The trochanter is markedly developed, surpassing in size and scope of the normal by 3 to 4 times and stands about ½ inch higher than the highest level of the head. Above the acetabulum directly over the trochanter appears a pit, into which the tip of the trochanter would fit with abduction of the leg.
Radiograph of the left hip joint (Fig. 11). The head shows significant flattening in its upper sections, and irregularity of its surface. The epiphyseal line can be seen, but the portion of the epiphyseal line of the head is minimal. At the lower portions of the head bone apposition has taken place. The acetabulum is completely congruent with the abnormal shape of the head so that it fits precisely. Femoral shaft is very thick and bulky. Femoral neck angle approximately 110°, but is hard to determine because of the deformity of the head. The trochanter is like one the right an abnormally bulky structure, which rises high above the head of the femur and the hip.
Status on March 21. 1910. Right hip similar to that three months previously, but on the left the following changes occurred: a little more flexion possible, up to 110°, internal rotation in extension now up to 90°. Shortening of the left leg has increased slightly. Anterior superior iliac spine-external malleolus, right now 71 cm, left 68.5 cm. Gait similar to three months earlier. Pain has not increased. Radiograph shows slight increase in irregularity in the surface of the left femoral head.
Bilateral case
6. Wilhelm P., age 9. Nine brothers and sisters live and be healthy; only a younger brother suffers from chronic otitis. The boy himself has had no illnesses except measles and suffered no injury. At the age of 8 years – about 2 months before the first visit to at the clinic, “he began to limp on his right leg.’ The pain was only intermittent after strenuous activity. Now, complaining of pain in his right knee. In his free time outside the home he plays with no complaints with his comrades.
Status October 8. 1909: Normally developed boy. Standing: left convex lumbar scoliosis Low. Right anterior superior iliac spine is significantly higher than the left. The right heel is not touching the floor when the left knee is in extension. Right gluteal fold compared to the left is clearly flattened. Slight limping gait. The upper body leans very slightly to the right when stepping on the right leg. Lying down: Right hip joint is at an angle of 14°, adduction, abduction left similar. The level of spina right anterior superior iliac spine and knee and malleoli, etc, are high compared to the left. Anterior superior iliac spine-external malleolus, right and left 64 cm. Greater trochanter on both sides ½ inch above the R. N. line. No palpable deformity of the hip joints. No tenderness on either side. Circumference of the thigh 18 cm above the patella on the right ½ inches less than the left. In both groins there are enlarged, indurated, painless lymph nodes about the size of beans. On the left, they are larger and more numerous than on the right. Movements: Right hip joint. Flexion and extension almost completely free and painless, but lacks 10° full flexion. Abduction and adduction completely absent, only a few degrees of rotational movements are possible. Left hip joint. Flexion and extension, completely free. Abduction, up to 40 degrees, adduction to 30° rotations in extension by approximately 30°. All movements painless. In abduction loud crepitation.
X-ray image from the right hip joint (Fig. 10): flattening of the femoral head and irregularity of its surface at the top and medial portions. Moderate irregularity of the inner surface of acetabulum (pathological). Femoral neck angle normal. Trochanter very small.
Fig. 10.

Same case as in Fig. 9, but right hip
X-ray image of the left hip joint (Fig. 9): Very significant deformity of the upper femur.
The location of the epiphyseal line, so the actual femoral head corresponding part is almost completely gone, however, appears at the lower and medial portions of bone apposition to have taken place. This places the head in coxa vara rolled inferiorly. If one, however, draws the femoral neck and shaft axes, it is a narrow angle.
Status June 12, 1910. Pain has not worsened, the boy still runs and plays. The boy can jump without pain from a table to the floor. He has complained only occasionally, especially at night. Still limping slightly, upper body leans on each occurrence the right foot hitting the floor. The Trochanter height on both sides is increased to 2 cm above the R. N. line. Anterior superior iliac spine-external malleolus, right 65.3, left 65. 9 cm. Adduction of the right hip is now absent. The joint remains normal, except as before the loss of abduction. Adduction to 20°. Virtually free flexion. Mobility of the left hip joint still similar to that in previous years. In abduction at any given moment a sudden loud crack. The Trendelenburg sign is very positive right. When standing on the right leg the left spine anterior spine drops significantly below the horizontal, while standing on the left leg the right spine does not drop, however, is does not rise in the normal way above the horizontal. The X-ray image of deformity has increased especially in the right femur, so that above the right femoral head there is now a pit several millimeters deep.
Appendix II – Review of the cases observed up to now, sorted by the occurrence of the first symptoms
Unilateral Cases
| Nr. | Case | Age at onset of symptoms | Etiology |
|---|---|---|---|
| 1 | Zesas, 11 year-old girl | 6 years | After inflammatory disease of the right hip |
| 2 | Eigner, Case 1, 8 year-old girl | 7 years | Minor contusion of the left hip |
| 3 | Matsuoka, 18 year-old girl | 8 years | – |
| 4 | Eigner, Case 2, 10 year-old boy | 9 years | – |
| 5 | Negroni, 9 year-old girl | 9 years | Joint arthritis |
| 6 | Eigner, Case 3, 13 year-old boy | 10 years | Acute hip joint inflammation (osteomyelitis of the femur?) at age 10 weeks |
| 7 | Hofmeister, 12 year-old boy | 11 years | – |
| 8 | Eigner, Case 4, 13 year-old boy | 12 years | – |
| 9 | Eigner, Case 5, 13 year-old girl | 12 years | – |
| 10 | Gruer-Wollenberg, 17 year-old girl | 13 years | Congenital hip dislocation |
| 11 | Fridberg, 14 year-old boy | 13 years | – |
| 12 | Maydl, 15 year-old girl | 14 years | Minor hip contusion (?) |
| 13 | Hofmeister, 15 year-old girl | 14 years | Apparently acute onset |
| 14 | G. Schmidt, 43 year-old man | 14 years | Trauma as a seven-year-old (?) |
| 15 | Immelman, 33 year-old woman | End of second decade | Trauma as a 14-year-old (?) |
| 16 | Küster-Zesas, 16 year-old boy | 15 years | Subluxation of left hip, but repositioned |
| 17 | Riedel-Cornils, 17 year-old girl | 15 years | – |
| 18 | Fridberg, 22 year-old man | 16 years | – |
| 19 | G. Schmidt, 32 year-old man | 16 years | Subluxation of left hip, but repositioned |
| 20 | Riedel-Cornils, 18 year-old man | 17 years | Minor trauma (?) |
| 21 | Negroni, 18 year-old man | 17 years | – |
| 22 | Maydl, 18 year-old man | 18 years | – |
| 23 | Immelmann, 18 year-old woman | 26 years | Minor trauma (?) |
| 24 | Hoffa and Wollenberg, 30 year-old man | 17 years | Tuberculous coxitis age 5–7 years |
| 25 | Frangenheim, 39 year-old man | 32 years | Purulent inflammation of the left gluteal region (?) |
| 26 | Preisser, 35 year-old man | 34 years or more | Congenital joint deformity (?) |
Bilateral Cases
| Nr. | Case | Age at onset of symptoms | Etiology |
|---|---|---|---|
| 1 | Eigner, case 6, 8 year-old boy | 7 years | – |
| 2 | Okada, 17 year-old man | 7 years | “Infantalism” (?) |
| 3 | Guhl, 36 year-old woman | 7 years | – |
| 4 | v. Brunn, 12 year-old girl | 9 years | Minor trauma (?) |
| 5 | Hesse, 32 year-old woman | 10 years | – |
| 6 | Bibergeil, 14 year-old girl | 11 years | Minor trauma |
| 7 | Negroni, 13 year-old girl | 13 years | – |
| 8 | v. Brunn, 23 year-old woman | 16 years | – |
| 9 | Frangenheim, 17 year-old man | 17 years | Trauma (?) |
| 10 | Axhausen, 35 year-old man | 20 years | Scarlet fever and diphtheria at age 6 with painful swelling both hips |
| 11 | Kuliga, 41 year-old woman | 28 years | – |
| 12 | Wollenberg, 35 year-old woman | 30 years | Arthritis associated with abdominal typhus at age 12 |
Note. In the above chart are not listed a case of Oberst in which the findings at the hip joint were not indicated more precisely, two cases of Okada in which the diagnosis was not proven, three cases of Borchardt in which the author himself recognized the disease as arthritis deformans but as osteomyelitis.
Footnotes
Only Matsuoka reported about an 18 year old Japanese girl who after eight years of age gradually had almost all the major joints of her body affected. The radiographs showed marked deformity of the joints, particularly in the hip and shoulder. The stiffening of the joints was based on these shape changes, not on the fusion of the articulating bones. Swelling of the periarticular connective tissues and joint effusions were not observed. Everything indicates that the label that Matsuoka applied one case, “arthritis deformans juvenilis” is indeed correct and that it was not a primary chronic rheumatism. We should not eliminate such Matsuoka’s case as ‘not pure’, as did Bibergeil, but we must consider it as a rare exception and accept the rule that in osteoarthritis deformans epiphysis of the hip joint, the other joints of the body are not affected at the same time.
Regarding the second case of Schmidt, I can only agree to Bibergeil (Journal for Orthopedic Surgery Volume 25, pp. 199). In Maydl's case 2 I cannot consider the trauma – the patient slipped on a piece of coal and two days later developed pain – as the probable cause. What miners in a coal mine would not ever slip on a piece of coal?
I use the name of coxa vara in a traditional way to refer to all cases in which the femoral neck angle is reduced. As is well known, Sprengel and Kempf, recently reserved the term coxa vara for the cases of traumatic epiphyseal slipping and called all other cases in which a reduction of the femoral neck angle is observed a coxae adducta.
The age refers to that at the time of the last examination.
Editor’s Note: The translation of this article was performed by Drs. Dieter Rosenbaum of the University of Münster and Richard Brand.
Richard A. Brand MD (✉) Clinical Orthopaedics and Related Research, 1600 Spruce Street, Philadelphia, PA 19103, USA e-mail: dick.brand@clinorthop.org
References
- 1.Alsberg, Anatomische und klinische Betrachtungen über Coxa vara. Zeitschr. f. Orthopäd. Chirurgie. Vol. 6.
- 2.Axhausen, Klinische und histologische Beiträge zur Kenntnis d. juvenilen Arthritis deformans coxae. Charité-Annalen. 1909, Nr. 33, P. 414.
- 3.Bibergeil, Gibt es eine Osteoarthritis deformans coxae juvenilis idiopathica? Zeitschr. f. Orthopäd. Chirurgie Vol. 25, P. 184.
- 4.Borchard, Zur Frage der deformierenden Entzfindung (Arthritis deformans) des Hüftgelenks bei jugendlichen lndividuen. Deutsche Zeitschr. f. Chirurgie Vol. 85, P. 74.
- 5.v. Brunn, Über die juvenile Osteoarthritis deformans des Hüftgelenks. Beiträge z. klin. Chirurgie Vol. 40, P. 651.
- 6.P. Cornils, Über Gelenkresektion bei Arthritis deformans und Hallux valg. Inaug.-Dissert. Jena 1890 P. 18, Fall 2.
- 7.Engel, Anleitung zur Beurteilung d. Leichenbefunde. Wien 1846, P. 237. (vgl. Wollenberg 1910, P. 33).
- 8.Frangenheim, Zur Pathologie der Osteoarthritis deformans juvenilis des Hüftgelenks. Bruns’ Beitr. zur klin. Chirurgie Vol. 65, P. 19.
- 9.Fridberg, Coxa vara adolesc, and Osteoarthritis deform, coxe. The amer. journ. of orthoped. surgey (sic). July 1905, Vol. 3. Riedingers Archiv f. Orthopädie 1908, P. 96.
- 10.Guhl, Ein durch Osteoarthritis deformans juvenilis trichterförmig verengtes Becken. Hegars Beitr. z. Geburtsh. u. Gyn. 1906, Vol. 11, P. 155.
- 11.Hesse, Arthritis deformans juvenilis coxae. Mitt. a. d. Grenzgeb. Vol. 15, P. 345.
- 12.Hoffa, Diskussion z. Vortrag Immelmann in d. Freien chir. Vereinigung, 22. X. 1906. Deutsche med. Wochenschr. 1907, P. 204.
- 13.Hoffa und Wollenberg, Arthritis deformans und sogenannter chronischer Gelenkrheumatismus. Stuttgart 1908, Enke.
- 14.Hofmeisters Fälle, referiert von Zesas 1909.
- 15.Immelmann, Osteoarthritis deformans coxae juvenilis. Freie Vereinig. d. Chir. Berlin 23 . X. 1906. Deutsche med. Wochenschr. 1907, Nr. 5 and 6,
- 16.Küttner. Münchn. med. Wochenschr. 1906, P. 1891.
- 17.Matsuoka, Über die Osteoarthritis deformans juvenilis. Deutsche Zeitschr. f. Chirurgie 1908, Vol. 96, P. 302.
- 18.Maydl, Coxa vara und Arthritis deformans coxae. Wiener klin. Rundschau 1897, Nr. 10–12.
- 19.H. Mohr, Über Osteomyelitis im Säuglingsalter. Med. klin. Wochenschr. 1905, Nr. 7.
- 20.Negroni, Dell’ osteoarthrite deformante giovanile dell anca. Arch. Di ortopedia 1905, Nr. 3 (ref. Zentralbl. f. Chirurgie).
- 21.Oberst, Die Diagnose der Hüftgelenkserkrankungen. Zeitschr. f. ärztl. Fortbildung 1908, Vol. 5, Nr. 17.
- 22.T. Okada, Über infantile Formen der Arthritis deformans. Riedingers Archiv f. Orthopädie usw., Vol. 8, P. 126.
- 23.Preiser, Über die Arthritis deformans coxae ihre Beziehungen zur Roser-Né1atonschen Linie und über s. Trochanterhochstand Hüftgesunder infolge anormaler Pfannenstellung. Deutsche Zeitschr. f. Chirurgie Vol. 89, P. 540.
- 24.Preiser, Pathol. Gelenkflächeninkongruenz. Zentralbl. f. Chirurgie 1908.
- 25.Preiser, Ein Fall yon sogenannter idiopathischer juveniler Osteoarthritis deformans coxae. Deutsche Zeitschr. f. Chirurgie Vol. 89, P. 613.
- 26.Preiser, Über die praktische Bedeutung einer anatomischen und habituell funktionellen Gelenkflächeninkongruenz. Fortschr. a. d. Gebiete d. Röntgenstrahlen Vol. 12, P. 1552.
- 27.Preiser, Über Deformitäten nach Gelenkentzündungen des Säuglingsalters. Zeitschr. f. orthopäd. Chirurgie Vol. 21, Issue 1–3.
- 28.Preiser, Über pathologische Gelenkflächeninkongruenz als Ursache der Arthritis deformans. Verhandlgn. d. Naturforscherverslg. 1908.
- 29.Trendelenburg, Über den Gang bei angeborener Hüftgelenksluxation. Deutsche med. Wochenschr. 1895, Nr. 2.
- 30.Georg Schmidt, Die Kontusion der Knorpelfuge des Schenkelkopfes und ihre Folgezustände (Coxa vara, Coxitis deformans). Mikulicz-Gedenkband. Mitt. a. d. Grenzgeb. d. inn. Medizin u. Chirurgie 1907.
- 31.Walkhoff. Verhandlungen d. Deutschen Patholog. Gesellschaft 1905.
- 32.Wollenberg, Arthritis deformans und sogenannter chronischer Gelenkrheumatismus. Stuttgart Enke 1908.
- 33.Wollenberg, Ätiologie der Arthritis deformans. Stuttgart Enke 1910.
- 34.Zesas DG. Über Resektion des Hüftgelenks bei Arthritis deformans. Deutsche Zeitschr. f. Chirurgie. 1888;27:586. doi: 10.1007/BF02832031. [DOI] [Google Scholar]
- 35.Zesas, Über die juvenile Osteoarthritis deformans coxae. Arch. f. Orthopädie, Mechanotherapie u. Unfallchirurgie 1909, Vol. 7, Issue 2 and 3.
- 36.Zesas, Nachtrag zu dem Aufsatze: Über die juvenile Osteoarthritis deformans coxae. Riedingers Archiv f. Orthopädie 1910, Vol. 8, P. 139.
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.