

Progression of Alzheimer's disease (AD) is associated with accumulation of proteinaceous plaques composed of misfolded β-amyloid fibrils and oligomers, and neurofibrillary tangles consisting of hyperphosphorylated MAPT (tau) protein in the cerebral cortex (and other brain regions), leading to demyelination, neuronal cell death, central nervous system (CNS) impairment, cognitive dysfunction, and ultimately death. Numerous strategies are under investigation for tackling the molecular mechanisms underlying the disease. All of these methods, regardless of the molecular target, are dependent on the successful delivery of a therapeutic compound to the brain. Achieving this goal has been a major challenge in the development of CNS-specific therapeutics, because the blood–brain barrier (BBB), which tightly regulates the transport of molecules to the brain, prevents nearly all biotherapeutics from reaching their site of action. However, in this issue of Molecular Therapy, Kohli et al.1 show that bioencapsulated therapeutic proteins can reduce AD-related amyloid load in the brain and retina upon oral delivery.
AD, the most common cause of dementia, is currently incurable. At present, clinical intervention is limited to symptom management and palliative care. Novel therapeutics that target β-amyloid are desirable given the centrality of β-amyloid in AD pathophysiology. A handful of studies have reported successful systemic CNS delivery of macromolecular drugs. For example, Pardridge and colleagues have shown that protein therapeutics can be directed to the brain by fusing them genetically to monoclonal antibodies that recognize receptors on the BBB and thereby promote transcytosis.2 Similarly, we have recently demonstrated systemic delivery of short interfering RNAs to the brain via the use of targeted exosomes.3 In another article in this issue, Meng et al. show that chimeric peptides comprising a cationic domain and an apolipoprotein E receptor–binding sequence could mediate systemic delivery of therapeutic enzymes to the brain by simply mixing the peptide with the enzyme.4 However, all of these studies evaluated intravenous administration; if drugs are to be administered orally the additional obstacle of the gastrointestinal barrier must be crossed, adding a further layer of complexity.
Bioencapsulation of cargoes has been proposed to overcome this hurdle. This emerging technique utilizes plant cells to produce a therapeutic protein so as to take advantage of the protective plant cell wall. The latter, while shielding the protein from acids and enzymes in the stomach, is digested by gut microbes, releasing encapsulated proteins in the process. Although this approach has previously been used to achieve oral delivery of peptides, vaccine antigens and autoantigens, its potential to reach targets in the CNS has not been explored until now.5
Kohli et al. fused green fluorescent protein or myelin basic protein (MBP) via a furin-cleavable linker to the cholera toxin B subunit (CTB) and expressed the fusion proteins in plant cells. They then administered lyophilized plant extracts orally to triple-transgenic Alzheimer's disease (3×TgAD) mice, a mouse model for AD, to explore the ability of the fusion proteins to reach the brain following oral delivery.1 MBP has been shown to inhibit amyloid fibril formation via its direct binding to and degradation of amyloid by an intrinsic protease activity. These properties appear essential to the current strategy, as the authors also observed ex vivo reduction of amyloid levels not only in 3×TgAD mouse brains but also in postmortem human AD brains following exposure to the protein. Even though the authors demonstrate that CTB is required for entry of the fusion protein to neuronal cells, they note that this event seems not to be a prerequisite for the activity of MBP, which exerts its activity primarily extracellularly.6
The role of CTB in the fusion construct instead resides in its capability to bind the ganglioside receptor, thereby facilitating transcytosis across the intestinal epithelium following release of the protein drug from the bioencapsulation carrier. In a previous publication the authors showed that during transcytosis, furin (a trans-Golgi network enzyme) cleaves the fusion protein, which releases MBP into the circulation.7 However, in the current study, the authors also claim that intact CTB fusion proteins can reach the circulation, allowing for their subsequent transport across the BBB and blood–retinal barrier (BRB). This is potentially achieved by the dual function of the high-affinity GM1-binding ligand that, in addition to facilitating transcytosis across enterocytes, could also help the drug to reach brain and retinas via a similar mechanism (i.e., transcytosis across endothelial cells). Most importantly, after reaching the brain and retinas, MBP appears capable of reducing amyloid levels and aggregates in 3×TgAD mice in vivo (Figure 1).1
Figure 1.
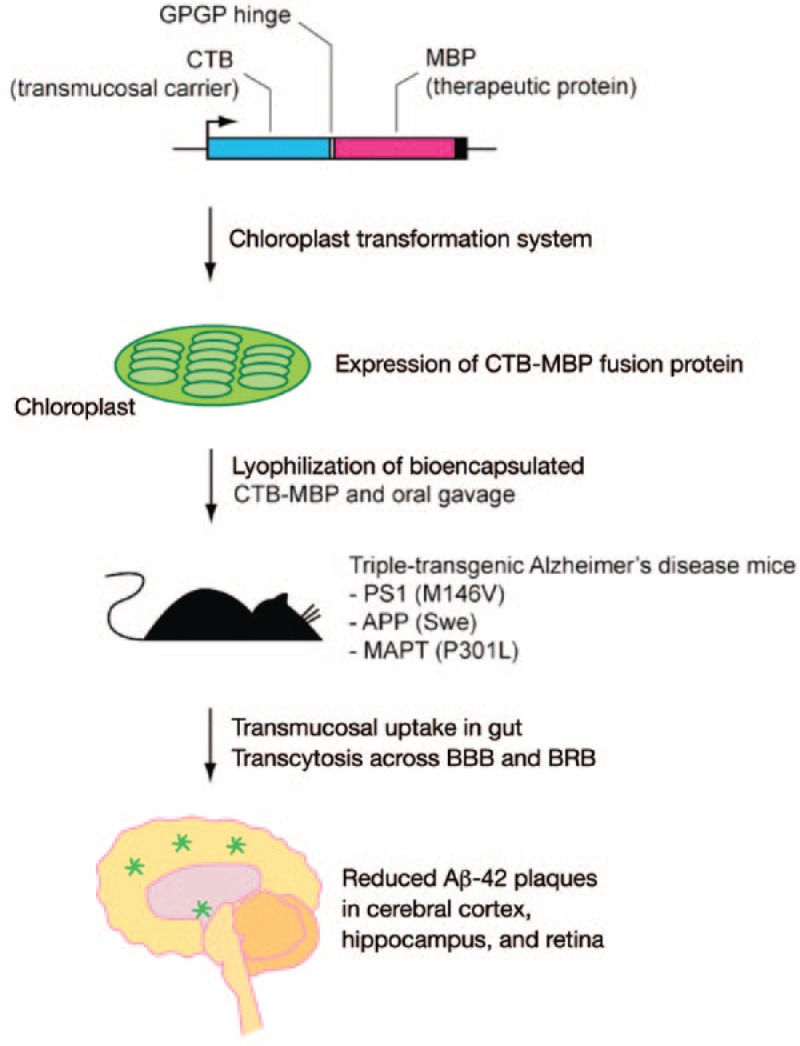
Strategy for reducing amyloid plaques in the brain and retina upon oral administration of bioencapsulated CTB-MBP fusion protein.1 Cholera toxin B subunit (CTB) and myelin basic protein (MBP) fusion protein are expressed in chloroplasts to achieve their bioencapsulation. After lyophilization, the therapeutic compound is orally administered to triple-transgenic Alzheimer's disease (3×TgAD) mice. Following transmucosal uptake in gut and transcytosis across the blood–brain barrier (BBB) and blood–retinal barrier (BRB), MBP reduces amyloid plaques in the brain and retina.
Oral administration of bioencapsulated CTB-MBP fusion protein seems to reduce the level of insoluble, high-molecular-weight β-amyloid aggregates in the hippocampus, an important hallmark of AD. This decrease is associated with a concurrent increase of soluble amyloid, consistent with the dual activity of MBP. Amyloid levels were also reduced in the retinas, leading to a lower rate of apoptosis of cells in this tissue, indicating that this strategy may also alleviate AD-related visual abnormalities.
These findings could potentially be important for the design of novel oral therapies for AD and for other CNS diseases. Even though in this study the therapeutics did not have to enter target cells to mediate their effect but could instead exert the effect within the extracellular space, it could be envisioned that appropriate fusion protein design could also allow access to intracellular targets. However, thorough mechanistic studies are required to achieve this goal; e.g., the need for cleavable linkers between the therapeutic and targeting proteins must be carefully assessed. Furthermore, even though these results appear remarkable, wider applicability of this technology for treating AD following delivery of other types of biotherapeutics (e.g., monoclonal antibodies, which have faced severe challenges) remains to be tested.
Nevertheless, bioencapsulation by expressing therapeutic proteins in plant cells to enable their oral delivery is a provocative strategy that deserves greater study. It may offer advantages over other routes of administration, such as low manufacturing costs, easy scale-up, low risk of contamination with human pathogens, facile purification, minimally stringent storage conditions, and sterile delivery.5 As Kwon et al. point out, there may be an emerging trend of trans-kingdom drug delivery. Employing plant expression systems for therapeutic proteins seems feasible, because the first plant cell system for production of human therapeutic protein (a lysosomal enzyme expressed in carrots) was recently approved by the US Food and Drug Administration (FDA).8 It should also be noted that the use of CTB as an antigen is already permitted by the FDA,9 and MBP is naturally found in the circulation, potentially allowing translational study of this technology at a rapid pace.
References
- Kohli N, Westerveld DR, Ayache AC, Verma A, Shil P, Prasad T.et al. (2014Oral delivery of bioencapsulated proteins across blood–brain and blood–retinal barriers Mol Ther 22535–546. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Pardridge WM. Drug transport across the blood–brain barrier. J Cereb Blood Flow Metab. 2012;32:1959–1972. doi: 10.1038/jcbfm.2012.126. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Alvarez-Erviti L, Seow Y, Yin H, Betts C, Lakhal S., and, Wood MJA. Delivery of siRNA to the mouse brain by systemic injection of targeted exosomes. Nat Biotechnol. 2011;29:341–345. doi: 10.1038/nbt.1807. [DOI] [PubMed] [Google Scholar]
- Meng Y, Sohar I, Sleat DE, Richardson JR, Reuhl KR, Jenkins RB.et al. (2014Effective intravenous therapy for neurodegenerative disease with a therapeutic enzyme and a peptide that mediates delivery to the brain Mol Ther 22547–553. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kwon K-C, Verma D, Singh ND, Herzog R., and, Daniell H. Oral delivery of human biopharmaceuticals, autoantigens and vaccine antigens bioencapsulated in plant cells. Adv Drug Deliv Rev. 2013;65:782–799. doi: 10.1016/j.addr.2012.10.005. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Liao MC, Ahmed M, Smith SO, Van Nostrand WE. Degradation of amyloid beta protein by purified myelin basic protein. J Biol Chem. 2009;284:28917–28925. doi: 10.1074/jbc.M109.050856. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Limaye A, Koya V, Samsam M., and, Daniell H. Receptor-mediated oral delivery of a bioencapsulated green fluorescent protein expressed in transgenic chloroplasts into the mouse circulatory system. FASEB J. 2006;20:959–961. doi: 10.1096/fj.05-5134fje. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Zimran A, Brill-Almon E, Chertkoff R, Petakov M, Blanco-Favela F, Muñoz ET.et al. (2011Pivotal trial with plant cell-expressed recombinant glucocerebrosidase, taliglucerase alfa, a novel enzyme replacement therapy for Gaucher disease Blood 1185767–5773. [DOI] [PubMed] [Google Scholar]
- Hill DR, Ford L., and, Lalloo DG. Oral cholera vaccines: use in clinical practice. Lancet Infect Dis. 2006;6:361–373. doi: 10.1016/S1473-3099(06)70494-7. [DOI] [PubMed] [Google Scholar]