

Abstract
We established a method for creation of an anatomic femoral tunnel with minimal damage to the remnant bundle in remnant-preserving anterior cruciate ligament (ACL) reconstruction. The goals of this surgical technique were to preserve the remnant bundle as much as possible, especially at the femoral insertion, and to make the tunnel at the anatomic position. The critical points are that the posterior side of the femoral footprint of the ACL is observed through the posterolateral portal using a 70° arthroscope and a femoral tunnel is made by use of an outside-in technique with remnant preservation. This technique allows for easy viewing of the posterior side of the ACL and enables performance of an anatomic ACL reconstruction.
For treatment of a torn anterior cruciate ligament (ACL), reconstruction is supposed to be the best option; however, controversy persists with regard to the best reconstructive procedures. During ACL reconstruction, a relatively thick and abundant ACL remnant could be observed in most cases.1 However, the ACL remnant is usually debrided to create the correct femoral and tibial tunnels and to decrease the risk of impingement and cyclops lesions in traditional ACL reconstruction.1-3
Good results have been reported after remnant-preserving ACL reconstruction using a transtibial technique.4,5 However, another important point to consider is an anatomic reconstruction at the footprint of the native ACL.6-10 After remnant-preserving ACL reconstruction, the position of the femoral tunnel was not satisfactory and it was supposed to be positioned slightly to the anterior side, compared with our expectation, even though good clinical results were achieved.1,4,11 Recently, the trans-portal technique has become popular with creation of the femoral tunnel at the anatomic position. However, it is also difficult to preserve the remnant bundle using this technique.12 The outside-in femoral tunnel procedure seems to be a more reliable and precise way to achieve an anatomic ACL reconstruction in addition to being helpful in preserving the remnant bundle.
It is very difficult to observe the posterior portion of the ACL femoral attachment using an anteromedial (AM) or anterolateral (AL) portal because of preservation of the remnant bundle. From this viewpoint, we established a method for creation of an anatomic femoral tunnel with minimal damage to the remnant bundle in remnant-preserving ACL reconstruction. The critical points are that the posterior side of the ACL femoral footprint is observed through the posterolateral (PL) portal using a 70° arthroscope and the femoral tunnel is made using an outside-in technique with remnant preservation.
Surgical Technique
This technical note describes the technique of a remnant-preserving anatomic ACL reconstruction with outside-in femoral drilling using a FlipCutter (Arthrex, Naples, FL). It focuses on the procedure for AM femoral tunnel formation with minimal damage to the remnant bundle (Video 1). The details are summarized in Tables 1 and 2.
Table 1.
Tips and Pearls of Technique
| 1. The PL portal should be positioned behind the lateral femoral condyle. |
| 2. A 70° arthroscope should be used. |
| 3. During reaming using a FlipCutter, an empty shaver is positioned for the removal of bone debris through the AM portal. |
| 4. Tibial reaming is performed inside the remnants. |
| 5. Passing suture is observed at the PL portal and is transferred to the anterior tibial tunnel. |
Table 2.
Pitfalls and Risks
| 1. Technical demand for PL portal formation |
| 2. Only possible technique in case of tibial stump preservation |
| 3. Possible peroneal nerve injury when portal is placed in position that is too posterior |
| 4. Possible damage to remnants during retro-reaming procedure |
A routine arthroscopic examination of the knee joint was performed using the standard AL and AM portals with a distended knee joint at the arthroscopic infusion pump. For the remnant preservation, a straight suture hook (Linvatec, Largo, FL) with No. 0 PDS (Ethicon, Somerville, NJ) was introduced through the AM portal. The sharp tip penetrated the remnants of the ACL near the proximal end, and the free end of the suture in the intercondylar notch was grasped and brought up to the AM portal. This step was repeated until 3 sutures were placed (Fig 1).
Fig 1.

For remnant preservation, 3 sutures are placed near the proximal end of the remnant ACL and the free end of the suture in the intercondylar notch is grasped and brought up to the AM portal.
For observation of the posterior aspect of the ACL femoral footprint, the arthroscope was inserted through the AM portal and reached the PL compartment through the interval between the ACL and lateral femoral condyle. By use of a transillumination technique, a PL portal was made. The 70° arthroscope was then inserted through the PL portal and advanced to reach the posterior aspect of the intercondylar notch. With this approach, the posterior margin of the ACL femoral footprint could be clearly observed (Fig 2).
Fig 2.

In a right (Rt) knee, through a PL portal, the 70° arthroscope is inserted and advanced to reach the posterior aspect of the intercondylar notch. The posterior margin of the ACL footprint can be observed.
Under visualization through the PL portal, the ACL tibial drilling guide (Linvatec) or Acufex ACL femoral guide (Smith & Nephew, Andover, MA) was introduced through the AL portal. The AM femoral tunnel is usually adjusted to 7 to 9 mm according to the graft diameter (Fig 3). The guide tip was placed at the 4- to 5-mm anterior-distal area of the posterior-proximal margin of the ACL femoral footprint. The center point of the AM tunnel usually shows good correspondence with the anterior-proximal end of the cartilage margin (Fig 4). Drilling of the AM tunnel was performed with a FlipCutter, and the aperture of the tunnel was aligned with the inner margin of the cartilage. Retro-reaming was then performed to about 30 mm of the tunnel length until the FlipCutter bottomed out on the drill sleeve. After the surgeon removed the FlipCutter by pushing it back into the joint and straightening the blade tip, a suture retriever with looped No. 1-0 Maxon (Covidien, Mansfield, MA) and No. 1-0 Prolene (Ethicon) was inserted through the femoral tunnel for the graft and remnant bundle passage with 3 PDS sutures.
Fig 3.

Gross appearance during formation of anatomic femoral tunnel in right (Rt) knee. The arthroscope is inserted through the PL portal, and the ACL tibial drilling guide (Linvatec) is introduced through the AL portal.
Fig 4.

Postoperative 3-dimensional computed tomography image. The center point of the AM tunnel usually shows good correspondence with the anterior-proximal end of the cartilage margin.
For formation of the tibial tunnel, the tibial stump of the remnant ACL insertion was carefully palpated with a probe, a small incision was made at the center of the tibial stump with scissors, and a guide pin was inserted from the proximal-medial tibial condyle to the center of the ACL tibial insertion using an ACL tibial guider with a 50° angle, with preservation of the remnant bundle. Reaming of the tibial side was also adjusted according to the graft diameter.
The TightRope device (Arthrex) was used for femoral fixation. For remnant preservation, the suture ends of the remnant tissue were simultaneously pulled past the passing suture through the tibia and out the femur (Fig 5). The button was pulled through the femur until it exited the lateral cortex, and the graft was advanced by tensioning on the TightRope shortening strands. Finally, a tie was made between the sutures of the remnant tissue and shortening strands of the TightRope.
Fig 5.
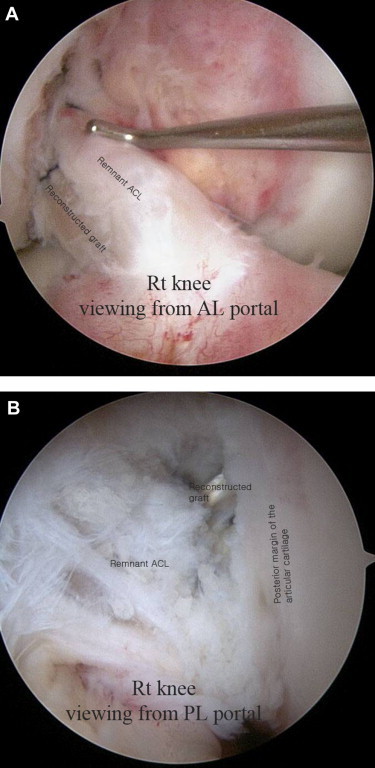
(A) In the right (Rt) knee, viewing through the AL portal, the reconstructed graft is wrapped with a preserved remnant. (B) Viewing through the PL portal, the reconstructed graft is passed at the posterior margin of the cartilage with remnant preservation.
Discussion
Most ACLs are ruptured in the proximal half,13 and most mechanoreceptors have been reported to be located in the subsynovial layer near the tibial insertion of the ACL.14-17 Therefore it seems reasonable to assume that the remnant tissue could be preserved, especially the tibial side, as a source of reinnervation if impingement and cyclops lesions can be prevented.1,4,5,18 However, during remnant preservation, using an anterior portal could interfere with restoration of the anatomic footprint because remnant tissue could be an obstacle to formation of an anatomic tunnel location.
Posterior (posteromedial, PL, and trans-septal) portals are frequently used in our practices.19-21 This technique allows for easy viewing of the posterior structures and enables performance of correct positioning of the tibial tunnel of the posterior cruciate ligament and medial meniscus posterior horn during meniscal root repair in meniscal allograft transplantation. On the basis of this background, it was thought that the posterior side of the ACL femoral footprint could be observed from the PL side using a 70° arthroscope or trans-septal portal using a 30° arthroscope. With the use of a trans-septal portal, an additional posteromedial and trans-septal portal could be made. Therefore using a PL portal was ideal.
Anatomic ACL reconstruction has been defined as the functional restoration of the ACL to its native dimensions, collagen orientation, and insertion sites, which is independent of whether a single or double bundle is used.8,9 This definition implies that exact observation of the native footprint is very important for anatomic ACL reconstruction. Usually, the anterior side of the ACL footprint is relatively easily observed through routine anterior (AM and AL) portals. However, viewing the posterior side of the ACL footprint is difficult with the use of these portals, especially during remnant-preserving ACL reconstruction. Therefore the PL or trans-septal portal could be an effective way to observe the posterior side of the ACL femoral footprint.
The outside-in femoral tunnel procedure appears to be a more reliable and precise method for achieving an anatomic ACL reconstruction, as well as being helpful in preservation of the remnant bundle.5,22-24 The TightRope device is included among cortical suspension devices and has acceptable biomechanical properties.25-27 This device is commonly used with a FlipCutter during outside-in femoral drilling; the FlipCutter has been newly devised and achieves the least invasive bone-sparing reconstructive procedures. This device allows surgeons to place the femoral socket without anatomic restrictions or femoral soft-tissue dissection. Once in the joint, the FlipCutter was used as a retrograde reamer for creation of the femoral socket from inside out.22
The advantages of this technique are direct visualization of the posterior footprint of the ACL, preservation of the remnant bundle, and then possible anatomic ACL reconstruction. However, additional PL portal formation, the need for a 70° arthroscope, and the oblique view from the PL portal could be disadvantages. Therefore, surgeons who are not accustomed to performing PL portal formation and viewing with the 70° arthroscope should use caution when performing these procedures.
In summary, by use of an outside-in technique, it is very helpful to use the PL portal with a 70° arthroscope for creation of a femoral tunnel at an anatomic position with minimal damage to the remnant bundle of the femoral attachment.
Footnotes
The authors report that they have no conflicts of interest in the authorship and publication of this article.
Supplementary data
Preoperative magnetic resonance imaging showing remnants, arthroscopic views of entire surgical procedure, and follow-up 3-dimensional computed tomography (to assess tunnel position) and magnetic resonance imaging (to assess graft status).
References
- 1.Ahn J.H., Lee Y.S., Ha H.C. Anterior cruciate ligament reconstruction with preservation of remnant bundle using hamstring autograft: Technical note. Arch Orthop Trauma Surg. 2009;129:1011–1015. doi: 10.1007/s00402-008-0597-7. [DOI] [PubMed] [Google Scholar]
- 2.Harner C.D., Giffin J.R., Dunteman R.C., Annunziata C.C., Friedman M.J. Evaluation and treatment of recurrent instability after anterior cruciate ligament reconstruction. Instr Course Lect. 2001;50:463–474. [PubMed] [Google Scholar]
- 3.Lee B.I., Min K.D., Choi H.S., Kim J.B., Kim S.T. Arthroscopic anterior cruciate ligament reconstruction with the tibial-remnant preserving technique using a hamstring graft. Arthroscopy. 2006;22:340.e1–340.e7. doi: 10.1016/j.arthro.2005.11.010. www.arthroscopyjournal.org Available online at. [DOI] [PubMed] [Google Scholar]
- 4.Ahn J.H., Lee S.H., Choi S.H., Lim T.K. Magnetic resonance imaging evaluation of anterior cruciate ligament reconstruction using quadrupled hamstring tendon autografts: Comparison of remnant bundle preservation and standard technique. Am J Sports Med. 2010;38:1768–1777. doi: 10.1177/0363546510368132. [DOI] [PubMed] [Google Scholar]
- 5.Ahn J.H., Wang J.H., Lee Y.S., Kim J.G., Kang J.H., Koh K.H. Anterior cruciate ligament reconstruction using remnant preservation and a femoral tensioning technique: Clinical and magnetic resonance imaging results. Arthroscopy. 2011;27:1079–1089. doi: 10.1016/j.arthro.2011.03.002. [DOI] [PubMed] [Google Scholar]
- 6.Fu F.H., Musahl V. Anatomic ACL reconstruction. Preface. Clin Sports Med. 2012;32:xv–xvi. doi: 10.1016/j.csm.2012.10.001. [DOI] [PubMed] [Google Scholar]
- 7.Lubowitz J.H., Akhavan S., Waterman B.R., Aalami-Harandi A., Konicek J. Technique for creating the anterior cruciate ligament femoral socket: Optimizing femoral footprint anatomic restoration using outside-in drilling. Arthroscopy. 2013;29:522–528. doi: 10.1016/j.arthro.2012.10.007. [DOI] [PubMed] [Google Scholar]
- 8.van Eck C.F., Samuelsson K., Vyas S.M., van Dijk C.N., Karlsson J., Fu F.H. Systematic review on cadaveric studies of anatomic anterior cruciate ligament reconstruction. Knee Surg Sports Traumatol Arthrosc. 2011;19(suppl 1):S101–S108. doi: 10.1007/s00167-011-1544-7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.van Eck C.F., Schreiber V.M., Mejia H.A. “Anatomic” anterior cruciate ligament reconstruction: A systematic review of surgical techniques and reporting of surgical data. Arthroscopy. 2010;26:S2–S12. doi: 10.1016/j.arthro.2010.03.005. [DOI] [PubMed] [Google Scholar]
- 10.Yasuda K., Tanabe Y., Kondo E., Kitamura N., Tohyama H. Anatomic double-bundle anterior cruciate ligament reconstruction. Arthroscopy. 2010;26:S21–S34. doi: 10.1016/j.arthro.2010.03.014. [DOI] [PubMed] [Google Scholar]
- 11.Ahn J.H., Jeong H.J., Ko C.S., Ko T.S., Kim J.H. Three-dimensional reconstruction computed tomography evaluation of tunnel location during single-bundle anterior cruciate ligament reconstruction: A comparison of transtibial and 2-incision tibial tunnel-independent techniques. Clin Orthop Surg. 2013;5:26–35. doi: 10.4055/cios.2013.5.1.26. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Sonnery-Cottet B., Chambat P. Anatomic double bundle: A new concept in anterior cruciate ligament reconstruction using the quadriceps tendon. Arthroscopy. 2006;22:1249.e1–1249.e4. doi: 10.1016/j.arthro.2006.07.042. www.arthroscopyjournal.org Available online at. [DOI] [PubMed] [Google Scholar]
- 13.Sherman M.F., Lieber L., Bonamo J.R., Podesta L., Reiter I. The long-term followup of primary anterior cruciate ligament repair. Defining a rationale for augmentation. Am J Sports Med. 1991;19:243–255. doi: 10.1177/036354659101900307. [DOI] [PubMed] [Google Scholar]
- 14.Kennedy J.C., Alexander I.J., Hayes K.C. Nerve supply of the human knee and its functional importance. Am J Sports Med. 1982;10:329–335. doi: 10.1177/036354658201000601. [DOI] [PubMed] [Google Scholar]
- 15.Krauspe R., Schmitz F., Zoller G., Drenckhahn D. Distribution of neurofilament-positive nerve fibres and sensory endings in the human anterior cruciate ligament. Arch Orthop Trauma Surg. 1995;114:194–198. doi: 10.1007/BF00444261. [DOI] [PubMed] [Google Scholar]
- 16.Schutte M.J., Dabezies E.J., Zimny M.L., Happel L.T. Neural anatomy of the human anterior cruciate ligament. J Bone Joint Surg Am. 1987;69:243–247. [PubMed] [Google Scholar]
- 17.Zimny M.L., Schutte M., Dabezies E. Mechanoreceptors in the human anterior cruciate ligament. Anat Rec. 1986;214:204–209. doi: 10.1002/ar.1092140216. [DOI] [PubMed] [Google Scholar]
- 18.Adachi N., Ochi M., Uchio Y., Sumen Y. Anterior cruciate ligament augmentation under arthroscopy. A minimum 2-year follow-up in 40 patients. Arch Orthop Trauma Surg. 2000;120:128–133. doi: 10.1007/s004020050028. [DOI] [PubMed] [Google Scholar]
- 19.Ahn J.H., Lee D.H., Lee Y.S., Wang J.H., Ha H.C. Clearing a blind spot in knee arthroscopy: Popliteal bursa. Knee Surg Sports Traumatol Arthrosc. 2008;16:549–552. doi: 10.1007/s00167-008-0488-z. [DOI] [PubMed] [Google Scholar]
- 20.Ahn J.H., Yang H.S., Jeong W.K., Koh K.H. Arthroscopic transtibial posterior cruciate ligament reconstruction with preservation of posterior cruciate ligament fibers: Clinical results of minimum 2-year follow-up. Am J Sports Med. 2006;34:194–204. doi: 10.1177/0363546505279915. [DOI] [PubMed] [Google Scholar]
- 21.Lee Y.S., Ahn J.H., Min B.H., Nha K.W. Arthroscopic loose body removal and cyst decompression using a posterior trans-septal portal in the blind spot during knee arthroscopy—Technical report. Knee. 2011;18:55–58. doi: 10.1016/j.knee.2010.01.008. [DOI] [PubMed] [Google Scholar]
- 22.Lee Y.S., Lee B.K., Chun D.I. Flipping method of a RetroButton during ACL reconstruction with outside-in femoral drilling using a FlipCutter. Orthopedics. 2012;35:861–864. doi: 10.3928/01477447-20120919-04. [DOI] [PubMed] [Google Scholar]
- 23.Lee Y.S., Lee B.K., Moon D.H., Park H.G., Kim W.S., Moon C.W. Comparison of tunnel locations of double bundle ACL reconstruction using the conventional transtibial technique with anatomic tunnel locations using a 3D CT model. Arch Orthop Trauma Surg. 2013;133:1121–1128. doi: 10.1007/s00402-013-1780-z. [DOI] [PubMed] [Google Scholar]
- 24.Lee Y.S., Sim J.A., Kwak J.H., Nam S.W., Kim K.H., Lee B.K. Comparative analysis of femoral tunnels between outside-in and transtibial double-bundle anterior cruciate ligament reconstruction: A 3-dimensional computed tomography study. Arthroscopy. 2012;28:1417–1423. doi: 10.1016/j.arthro.2012.03.017. [DOI] [PubMed] [Google Scholar]
- 25.Lee Y.S., Kim S.K., Park J.H. Double-bundle anterior cruciate ligament reconstruction using two different suspensory femoral fixation: A technical note. Knee Surg Sports Traumatol Arthrosc. 2007;15:1023–1027. doi: 10.1007/s00167-007-0336-6. [DOI] [PubMed] [Google Scholar]
- 26.Milano G., Mulas P.D., Ziranu F., Piras S., Manunta A., Fabbriciani C. Comparison between different femoral fixation devices for ACL reconstruction with doubled hamstring tendon graft: A biomechanical analysis. Arthroscopy. 2006;22:660–668. doi: 10.1016/j.arthro.2006.04.082. [DOI] [PubMed] [Google Scholar]
- 27.Kamelger F.S., Onder U., Schmoelz W., Tecklenburg K., Arora R., Fink C. Suspensory fixation of grafts in anterior cruciate ligament reconstruction: A biomechanical comparison of 3 implants. Arthroscopy. 2009;25:767–776. doi: 10.1016/j.arthro.2009.01.021. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Preoperative magnetic resonance imaging showing remnants, arthroscopic views of entire surgical procedure, and follow-up 3-dimensional computed tomography (to assess tunnel position) and magnetic resonance imaging (to assess graft status).