

Abstract
Breast cancer screening remains a subject of intense and, at times, passionate debate. Mammography has long been the mainstay of breast cancer detection and is the only screening test proven to reduce mortality. Although it remains the gold standard of breast cancer screening, there is increasing awareness of subpopulations of women for whom mammography has reduced sensitivity. Mammography has also undergone increased scrutiny for false positives and excessive biopsies, which increase radiation dose, cost and patient anxiety. In response to these challenges, new technologies for breast cancer screening have been developed, including; low dose mammography; contrast enhanced mammography, tomosynthesis, automated whole breast ultrasound, molecular imaging and MRI. Here we examine some of the current controversies and promising new technologies that may improve detection of breast cancer both in the general population and in high-risk groups, such as women with dense breasts. We propose that optimal breast cancer screening will ultimately require a personalized approach based on metrics of cancer risk with selective application of specific screening technologies best suited to the individual’s age, risk, and breast density.
Introduction
It is generally accepted that early detection of breast cancer increases the probability of cure and mammography has been shown to reduce breast cancer mortality in population-based screening programs (1). However, mammography has limitations, and some investigators propose the benefits do not always outweigh the risks. The sensitivity of mammography is highly variable, ranging from 98% in women with fatty breast parenchyma, to 36% in women with dense breasts (2, 3). Thus, women who undergo annual mammography may still present with cancers found only on physical exam. False positive rates in breast cancer screening are also a significant limitation as high callback rates and unnecessary biopsies increase cost, radiation dose, and patient anxiety. Concern for long-term sequelae of radiation exposure remains, as recent studies suggest mammography may actually contribute to an increased incidence of breast cancer in certain high-risk populations (4). These concerns understandably may decrease compliance with screening recommendations (5).
More successful breast cancer screening requires increased sensitivity and specificity, ideally, limiting both financial cost and radiation burden. Some of this may be obtained through new technological development. However, we propose that optimal patient care will ultimately require a new paradigm with adoption of patient-specific screening strategies tailored to risk assessment based on family history, age, genetic profiles, and breast density. The goal in this approach is development of personalized imaging algorithms that maximize specificity and sensitivity while minimizing cost and radiation exposure. In this article we discuss both current practices and imaging techniques that may be combined in novel ways to achieve optimal, personalized imaging strategies for detecting breast cancer.
Screening Mammography Recommendations
Controversies surrounding mammography and breast cancer screening have led to uncertainty about optimal screening strategies. In 2009, the United States Preventive Services Task Force (USPSTF), a panel of health care professionals that reviews published research and makes recommendations about preventive health care, issued revised mammography guidelines. These included the recommendation for screening mammograms every two years beginning at age 50 for women at average risk of breast cancer. They recommended against routine screening mammograms before age 50. This recommendation ignited an ongoing, often passionate, debate regarding optimal screening strategies.
At present, the USPSTF is the only group or consensus panel in the United States that recommends screening to begin at age 50 (Table 1). Most such groups recommend breast cancer screening to begin at age 40 and women with a first-degree relative diagnosed with breast cancer should begin annual mammography 10 years prior to the age of diagnosis of that relative (6).
Table 1.
Screening mammography guidelines from major consensus groups and organizations in the United States
| Begin Screening Interval (years) | Age (years) | |
|---|---|---|
| American Cancer Society | 40 | 1 |
| National Cancer Institute | 40 | 1 to 2 |
| American Medical Association | 40 | 1 to 2 |
| American College of Surgeons | 40 | 1 |
| American College of Physicians | 40 | 1 to 2 |
| American College of Radiology | 40 | 1 |
| American College of Obstetrics and Gynecology | 40 | 1 |
| United States Preventive Services Task Force. | 50 | 2 |
Limitations of Mammography and the Need for an Adjunctive Screening Tool
There is clear evidence that mammography detects early breast cancers and that screening large populations reduces mortality. However, mammography is an imperfect screening tool. The sensitivity of mammography is inversely proportional to breast density (7). Among women with heterogeneously dense or extremely dense breast parenchyma, full field digital mammography (FFDM) has been shown to be more sensitive than film-screen mammography (8). Unfortunately, the sensitivity of both digital and analog mammography remains low in women with dense breast parenchyma (2, 3), limiting its usefulness in high-risk younger women.
Radiation Risks and Low Dose Mammography
While the absorbed radiation dose received by the breast during mammography represents a relatively small component of the lifetime-accumulated dose from medical imaging and other sources, the popular press and medical literature frequently raise concerns regarding the radiation risks from mammography. According to the National Research Council of the National Academies Biologic Effects of Ionizing Radiation (BEIR) VII study; the average mean glandular dose (MGD) from digital mammography is 3.7 mGy. This is estimated to have a lifetime attributable risk of fatal breast cancer of 1.3 per 100,000 women aged 40 years at exposure and less than one case per 1,000,000 women aged 80 years at exposure (9). It has also been estimated that for the same cohort, 292 lives would be saved as a result of annual screening (10). While this favorable risk-benefit ratio seems clear, many women and physicians remain concerned.
Strategies are being investigated to lower radiation dose and alleviate patient fears without compromising cancer detection. Spectral imaging or photon counting is a promising new technology in digital mammography aimed at lowering the MGD to the breast. The image is acquired by a scanning method that utilizes a multi slit collimator, eliminating 97% of scattered radiation, significantly lowering the absorbed dose (11). The direct capture of individual x-rays occurs without the analog-to-digital conversion steps, increasing efficiency. Recently the FDA approved a low dose photon counting mammography unit in the United States, which delivers approximately half the dose of standard FFDM (12). This device is popular in Europe and the image quality has been judged acceptable in preliminary investigations (13).
Contrast Enhanced Mammography
A major advantage of MRI in detection of breast cancer is its ability to detect and evaluate blood flow in breast masses. Recent studies have shown that contrast enhanced digital mammography can also image blood flow using temporal subtraction and dual energy subtraction (14–16). This technique requires injection of an iodinated contrast agent and the sensitivity for tumor detection has ranged from 78–92% (14–17). Recent literature has demonstrated that the addition of contrast enhanced mammography to standard mammography and ultrasound in a diagnostic setting improves reader sensitivity from 71% to 78% and improved reader performance when compared with mammography and ultrasound alone (17). In 2011, the FDA approved a contrast enhanced digital mammography in the United States as an adjunct to standard mammographic views (Figure 1). This technology is currently under evaluation at several mammography centers in Europe and Japan.
Figure 1.

49 year-old female with palpable mass, left breast. (a.) Cranio-caudal (CC) and medio-lateral oblique (MLO) low energy mammographic views demonstrate a focal asymmetry in the left central breast with adjacent biopsy clip (arrows). Contrast enhanced mammography in the CC (c.) and MLO (d.) projections demonstrate multiple enhancing masses in the left lower inner quadrant extending to the nipple (arrows). Ultrasound guided core biopsy confirmed the presence of multifocal invasive mammary carcinoma with lobular features. Images courtesy of Dr. Maxine S. Jochelson, MD., Director of Radiology Breast and Imaging Center, Memorial Sloan Kettering Cancer Center and Associate Professor of Radiology, Weill Medical College of Cornell University.
Digital Breast Tomosynthesis
Overlapping breast tissue in standard mammography can conceal important features of malignancy and is a frequent cause of false positive findings. Digital breast tomosynthesis is an imaging technique designed to eliminate the pitfalls of overlapping tissue (Figure 2). It has the potential to lower recall rates on screening mammography and reduce false negative examinations due to dense breast tissue. Tomosynthesis produces tomographic “slices” of an entire tissue volume, similar to a CT scan, using a single acquisition. The radiation exposure for tomosynthesis remains a potential limitation as the MGD varies from approximately 1.5–4 mGy per acquisition (18), (19), (20). The entire radiation dose for the exam depends on whether the exam is a one-view or two-view technique and whether or not it is combined with a standard mammogram. Although there are conflicting reports; the “average breast” that undergoes tomosynthesis is reported to receive a MGD approximately 8% higher than standard digital mammography (21).
Figure 2.

35-year old female with a palpable mass above the left nipple. (a.) CC and (b.) MLO mammographic views show heterogeneously dense breasts and subtle architectural distortion in the left upper outer quadrant (arrows). Tomographic slices in the CC (c.) & MLO (d.) projections demonstrate a 1.6 cm spiculated mass in the left upper outer quadrant (arrows). Subsequent mastectomy showed grade III invasive ductal carcinoma (IDC). Images reprinted with permission. Courtesy of Dr. Linda R.N. Greer, M.D., Medical Director and Radiologist, Breast Health & Research Center, John C. Lincoln Health Network in Phoenix, Arizona.
A potential limitation of tomosynthesis is decreased sensitivity for detection of micro-calcifications. Tomosynthesis is currently FDA approved as an adjunct to standard mammography, and does not replace it. There is promise that, in this adjunct capacity, tomosynthesis can increase specificity in mammographically detected masses.
Automated Breast Density
A number of studies have demonstrated that women with dense breast tissue have a four to six fold increased risk of breast cancer (22, 23) (24). Increased breast density also decreases the sensitivity of the mammogram and may limit the potential for early detection (25–27).
The American College of Radiology (ACR) Breast Imaging Reporting and Data System (BI-RADS) classification describes four categories of breast tissue density and instructs radiologists to include this density information in the medical report. At the present time, this classification is a primarily subjective estimate of quartiles from almost entirely fat, to extremely dense. There is marked inter observer variability between radiologists (28, 29), raising concern for integrating this information into clinical use.
Automated, objective, volumetric density measurements may have the potential to provide, reproducible risk metrics that can be integrated into a personalized breast cancer risk assessments (30). There is several commercially available software solutions that can be incorporated seamlessly into the mammography work flow and “automate” the calculation of breast density through an algorithm that utilizes volumetric parameters. If automated breast density measurements are determined to be accurate and reproducible, baseline and serial breast cancer risk estimates could potentially be used to advise individual patients on optimal frequency and type of screening studies.
Breast Density Legislation
There has been significant legislative activity surrounding the issue of breast density and the limited sensitivity of mammography screening in women with dense breasts. In 2009, Connecticut passed a law requiring radiologists to inform women of their breast density in the plain language report they receive after their mammogram, and advise them of alternate screening options (i.e. screening breast ultrasound and MRI).
Texas, Virginia, New York and Utah subsequently passed similar laws requiring radiologists to notify patients of their breast density. At the time of this writing, there is legislation pending on this issue in at least 11 more states and a similar bill has been introduced in the United States House of Representatives. This legislation will put important knowledge in the hands of the patient regarding their breast density and open the door for conversations between women and their physicians regarding additional screening options.
Automated Whole-Breast Ultrasound System (AWBUS)
Sonography is widely available, inexpensive, requires no contrast injection, does not use ionizing radiation, and is well tolerated by patients. However, scanning with hand-held transducers has provided little practical benefit in the detection of cancers due to the poor conspicuity of some cancers and the significant operator time and experience necessary for a high quality screening breast ultrasound. The variability in technologist skill and experience has made standardization of examinations nearly impossible.
However, hand held screening breast ultrasound in high-risk women has been shown to detect more cancers than mammography alone. Unfortunately, it also resulted in more recalled exams, biopsies and recommendations for short interval follow up than mammography alone. The rate of biopsy following screening ultrasound was 5%, with a positive predictive value (PPV) of 11%. Furthermore, generalization of these results is limited since all study participants were at elevated risk with over half having a personal history of breast cancer (31).
Two-dimensional AWBUS is a promising technology that aims to standardize the screening examination and produce a consistently high quality examination to improve the conspicuity of cancers. The study is typically performed with robotic guidance of a standard ultrasound probe over the entirety of both breasts followed by cine presentation of closely spaced images in the axial plane (Figure 3a) or reconstruction of the images to present a series of images in the coronal plane (Figure 3b) (32). AWBUS as an adjunct to mammography has shown similar malignancy detection rates as those with hand held ultrasound, 3.6 per 1,000, with a higher PPV of 38% (33).
Figure 3.
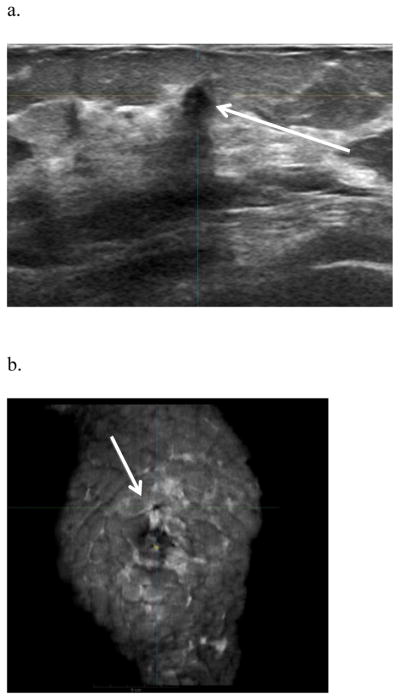
55 year-old female with dense breast parenchyma and normal screening mammogram, who underwent automated whole breast screening ultrasound. (a) Axial sonographic image from the right breast at 12 o’clock shows a 10 mm irregular hypoechoic mass with angular margins and posterior acoustic shadowing (arrow). (b.) Coronal reformatted image from a screening AWBUS demonstrates a 10 mm hypoechoic mass at 12 o’clock in the right breast (arrow). Ultrasound guided core biopsy showed IDC. Images courtesy of U-Systems, Inc. Sunnyvale, California.
High Risk Screening and Magnetic Resonance Imaging
Women at high risk for breast cancer may benefit from supplemental screening with MRI and it is recommended as an adjunct to mammography in selected high-risk patients (Figure 4) (34). There are several risk prediction models available for clinical use; such as the Gail model (35), Claus model (36), BRCAPRO (37), and Tyrer-Cuzick (38) models. An online risk assessment tool utilizing the Gail model is available on the American Cancer Society website; http://www.cancer.gov/bcrisktool/about-tool.aspx. Accessed on November 4, 2012.
Figure 4.

33 year-old female with known BRCA 2 mutation. (a.) CC and (b.) MLO mammographic views of the left breast demonstrate heterogeneously dense breast parenchyma and no identifiable masses, calcifications or other abnormality. c.) Axial contrast enhanced MRI subtraction sequences with kinetic overlay (d.) demonstrate a 1.5 cm rapidly enhancing irregular mass (arrow) with irregular margins and adjacent clumped ductal enhancement measuring up to 8.0 cm in greatest dimension. Ultrasound guided biopsy and subsequent mastectomy showed multi-centric grade III IDC with high-grade ductal carcinoma in situ (DCIS).
MRI has superior sensitivity to mammography and ultrasound in the detection of invasive cancer and has been shown to be cost effective in some high-risk groups (39–41). Recent data reports an additional 14.7 cancers per 1000 women detected when MRI is used as a supplement to mammography and whole breast ultrasound (31). However, there is no data to show a reduction in mortality from breast cancer as a result of MRI screening, and it is often criticized for decreased specificity, prompting biopsy or follow up imaging.
The American Cancer Society guidelines (Table 2a & b) for MRI as an adjunct to annual screening mammography recommends MRI for women who are first-degree relatives of BRCA carriers but have not undergone BRCA testing themselves, and women with a life-time risk that is 20–25% or greater than that of the average woman, as defined by risk prediction models (34). Some centers offer mammography and breast MRI at the same time, while others advocate staggering these examinations by 6 months, optimizing the time interval between imaging the breasts in one modality or another.
Table 2.
American Cancer Society Recommendations for Annual Supplemental MRI Screening
| a.) High Risk women for whom annual MRI is recommended |
| BRCA1 or BRCA2 gene mutations |
| First-degree relative with BRCA1 or BRCA2 mutation who have not been tested |
| Lifetime risk of breast cancer or 20–25% |
| History of radiation therapy to the chest between the ages of 10–30 years |
| Li-Fraumeni, Cowden or Bannayan-Riley-Ruvalcaba syndrome |
| b.) Women at Moderately Increased Risk who Should Talk to their Doctors About the Benefits and Limitations of MRI screening as an Adjunct to Mammography |
| Lifetime risk of breast cancer of 15–20% |
| Personal history of breast cancer ductal carcinoma in situ |
| History of lobular carcinoma in situ, atypical ductal hyperplasia, or atypical lobular hyperplasia at biopsy |
| Extremely dense or unevenly dense breasts |
Molecular Imaging
Positron emission mammography (PEM) and breast-specific gamma imaging (BSGI) use molecular imaging to increase specificity in cancer detection by demonstrating increased metabolic activity. Both of these techniques have high positive predictive values and low negative predictive values. BSGI uses a gamma radiation detector under the breast with mild compression to acquire images after intravenous administration of technetium 99m (99mTc) sestamibi (Figure 5). PEM uses paired radiation detectors to detect coincident gamma rays after the intravenous administration of fluorine 18 fluordeoxyglucose (FDG). These modalities are not currently suitable for screening, because each study results in whole body radiation equivalent to 20–30 mammograms (42). Their application is primarily in staging women with a diagnosis of cancer. Increasingly, however, FDG PET is used to evaluate response to therapy, or detect post treatment recurrence.
Figure 5.

78 year-old female with history of right lumpectomy and radiation therapy for invasive lobular carcinoma four years prior presents with increasing heaviness to the right breast after recent trauma. a.) CC and (b.) MLO mammographic views of the right breast demonstrate post lumpectomy changes with stable skin thickening, unchanged since the prior study. BSGI in the CC (c.) and (d.) MLO views demonstrate multiple areas of increased radiotracer uptake (presented as white on black) consistent with multifocal metabolically active disease. Subsequent mastectomy confirmed multi-centric invasive lobular carcinoma. Images courtesy of Dr. Michael Portillo, M.D., Susan Cheek Needler Breast Centers, Morton Plant Mease Healthcare, Clearwater, Florida.
Personalized Screening Strategies
Current screening strategies are clearly limited by the intra-population heterogeneity of breast cancer appearance, normal breast densities, and individual risk factors. Additional concerns include the financial cost of screening, the potential hazards of radiation exposure, and the medical, psychological, and financial burden of both false positive and false negative studies. We propose that new technologies in both imaging and risk assessment require re-thinking of the typical screening paradigm in which a single strategy is applied to all individuals in a population.
In other words, it seems clear that optimal breast cancer screening must be increasingly tailored to an individual’s risk and optimized through strategic, patient-specific application of available technology. Advances in breast imaging modalities, breast cancer risk assessment, breast density and a patient’s own views about the risks and benefits of screening should be carefully integrated into a personalized screening strategy. This paradigm differs from traditional guidelines in which all women are similarly screened with either annual or biennial mammograms, beginning at the age of 40 or 50.
Risk stratification tools are improving as our knowledge of the pathogenesis of breast cancer deepens. Commercially available risk stratification kits combine traditional risk models, such as the Gail Model, with DNA analysis; evaluating genetic mutations associated with breast cancer, separate from BRCA1 and BRCA2 mutations. This type of technology may aid in the evolution of personalized screening strategies as women obtain a more accurate estimate of their individual risk through risk assessment tools, genetic testing and clinical characteristics such as breast density.
These risk assessment tools along with the patient’s age, breast density, and personal preferences could then be integrated to develop an optimal screening program. For example; a 52-year old woman with heterogeneously dense breasts, highly concerned about radiation dose, may benefit from annual low dose mammography and automated whole breast ultrasound. A 65-year old woman with dense breasts concerned about false positives and excessive biopsies may prefer annual mammography combined with tomosynthesis. A-43 year old woman with heterogeneously dense breasts who has undergone DNA risk stratification and found to be “high-risk,” may choose annual mammography and tomosynthesis alternating with breast MRI every 6 months.
Personalized screening strategies are not an entirely novel concept. Women with BRCA1 or BRCA2 mutations, already participate in a form of personalized screening, with many women opting for annual mammography and breast MRI, often alternating at 6-month intervals. As technology further evolves and we are able to more accurately identify high-risk women, we will likely see evolution of personalized approaches to breast cancer screening, ranging from highly intricate to annual or perhaps biennial screening in low risk groups.
Summary
For many years, mammography has been the sole imaging test recommended for breast cancer screening, and remains the only test proven to reduce breast cancer-related mortality (1). However, the widespread application of mammography in population-based screening remains controversial, owing to decreased sensitivity in women with dense breast parenchyma, radiation concerns, and a high rate of false positive studies.
Breast imagers are adapting to these challenges with the development of new technologies. Low dose mammography can reduce radiation risk to the breast. Contrast enhanced mammography can evaluate blood flow in the breast, similar to MRI. Tomosynthesis produces multiple mammographic slices through the breast, similar to CT, and has significant potential to lower recall rates and increase specificity.
Both whole breast ultrasound and MRI have been shown to detect additional cancers in certain high-risk populations and will likely be increasingly used in screening women with dense breasts. However, a decrease in mortality has not been proven (31). Molecular imaging in the form of BSGI and PEM of the breast is widely available, although, due to relatively large whole-body radiation doses, not currently suitable for annual screening.
While these advances are encouraging, it is improbable that any of the new technologies will replace mammography for population-based screening programs, since all have significant limitations (Table 3). Furthermore, given the heterogeneity of the human population, a “perfect” imaging technology for breast cancer screening will likely never be found. In fact, because of this heterogeneity, the very concept of “one strategy fits all” population-based screening may be outmoded. The increasing ability to perform molecular, clinical, and tissue based risk assessments for an individual patient has opened new opportunities for patient-based screening strategies. Ultimately, optimal breast cancer screening will likely require a personalized approach that integrates patient-specific and age-dependent metrics of cancer risk with selective application of specific screening technologies best suited to the individual’s age, risk, and breast density.
Table 3.
Strengths and Limitations of Breast Imaging Modalities
| Modality | Strengths | Limitations | Screening |
|---|---|---|---|
| Spectral or photon counting low dose mammography | Approximate 40%
 in dose in dose |
Limited literature | Yes |
| CE Mammography | Outlines Vascularity in the breast | Limited data in screening Contrast injection | Adjunct |
| Tomosynthesis |
 Specificity Specificity |
Radiation |
Adjunct |
| AWBUS |
Sensitivity |
Specificity |
Adjunct |
|
False Positives | |||
| MRI |
Sensitivity |
Specificity |
Adjunct |
|
False Positives | |||
|
Cost Contrast Injection | |||
| BSGI |
Specificity |
Radiation |
No |
| PEM |
Specificity |
Radiation |
No |
CE, Contrast Enhanced
AWBUS, Automated whole breast ultrasound system
MRI, Magnetic resonance imaging
BSGI, Breast specific gamma imaging
PEM, positron emission mammography
References
- 1.Kuhl CK, Kuhn W, Schild H. Management of women at high risk for breast cancer: new imaging beyond mammography. Breast. 2005;14(6):480–6. doi: 10.1016/j.breast.2005.08.005. [DOI] [PubMed] [Google Scholar]
- 2.Kolb TM, Lichy J, Newhouse JH. Comparison of the performance of screening mammography, physical examination, and breast US and evaluation of factors that influence them: an analysis of 27,825 patient evaluations. Radiology. 2002;225(1):165–75. doi: 10.1148/radiol.2251011667. [DOI] [PubMed] [Google Scholar]
- 3.Mendelson G, Aronow WS. Underutilization of measurement of serum low-density lipoprotein cholesterol levels and of lipid-lowering therapy in older patients with manifest atherosclerotic disease. Journal of the American Geriatrics Society. 1998;46(9):1128–31. doi: 10.1111/j.1532-5415.1998.tb06652.x. [DOI] [PubMed] [Google Scholar]
- 4.Pijpe A, Andrieu N, Easton DF, et al. Exposure to diagnostic radiation and risk of breast cancer among carriers of BRCA1/2 mutations: retrospective cohort study (GENE-RAD-RISK) BMJ. 2012;345:e5660. doi: 10.1136/bmj.e5660. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Aro AR, de Koning HJ, Absetz P, Schreck M. Two distinct groups of non-attenders in an organized mammography screening program. Breast cancer research and treatment. 2001;70(2):145–53. doi: 10.1023/a:1012939228916. [DOI] [PubMed] [Google Scholar]
- 6.Dershaw DD. Mammographic screening of the high-risk woman. American journal of surgery. 2000;180(4):288–9. doi: 10.1016/s0002-9610(00)00463-3. [DOI] [PubMed] [Google Scholar]
- 7.Carney PA, Miglioretti DL, Yankaskas BC, et al. Individual and combined effects of age, breast density, and hormone replacement therapy use on the accuracy of screening mammography. Annals of internal medicine. 2003;138(3):168–75. doi: 10.7326/0003-4819-138-3-200302040-00008. [DOI] [PubMed] [Google Scholar]
- 8.Nelson HD, Tyne K, Naik A, et al. Screening for breast cancer: an update for the U.S. Preventive Services Task Force. Annals of internal medicine. 2009;151(10):727–37. W237–42. doi: 10.1059/0003-4819-151-10-200911170-00009. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Academies. NRCotN. Health Risks from exposure to low levels of ionizing radiation: BEIR VII, phase 2-Committee to Assess Health Risks from Exposure to Low Levels of Ionizing Radiation. Washington, DC: National Academies Press; 2006. [PubMed] [Google Scholar]
- 10.Feig SA, Hendrick RE. Radiation risk from screening mammography of women aged 40–49 years. Journal of the National Cancer Institute Monographs. 1997;(22):119–24. doi: 10.1093/jncimono/1997.22.119. [DOI] [PubMed] [Google Scholar]
- 11.Aslund M, Cederstrom B, Lundqvist M, Danielsson M. Scatter rejection in multislit digital mammography. Medical physics. 2006;33(4):933–40. doi: 10.1118/1.2179122. [DOI] [PubMed] [Google Scholar]
- 12.Baldelli P, McCullagh J, Phelan N, Flanagan F. Comprehensive dose survey of breast screening in Ireland. Radiation protection dosimetry. 2011;145(1):52–60. doi: 10.1093/rpd/ncq375. [DOI] [PubMed] [Google Scholar]
- 13.Cole EB, Toledano AY, Lundqvist M, Pisano ED. Comparison of radiologist performance with photon-counting full-field digital mammography to conventional full-field digital mammography. Academic radiology. 2012;19(8):916–22. doi: 10.1016/j.acra.2012.03.005. [DOI] [PubMed] [Google Scholar]
- 14.Lewin JM, Isaacs PK, Vance V, Larke FJ. Dual-energy contrast-enhanced digital subtraction mammography: feasibility. Radiology. 2003;229(1):261–8. doi: 10.1148/radiol.2291021276. [DOI] [PubMed] [Google Scholar]
- 15.Dromain C, Balleyguier C, Muller S, et al. Evaluation of tumor angiogenesis of breast carcinoma using contrast-enhanced digital mammography. AJR American journal of roentgenology. 2006;187(5):W528–37. doi: 10.2214/AJR.05.1944. [DOI] [PubMed] [Google Scholar]
- 16.Jong RA, Yaffe MJ, Skarpathiotakis M, et al. Contrast-enhanced digital mammography: initial clinical experience. Radiology. 2003;228(3):842–50. doi: 10.1148/radiol.2283020961. [DOI] [PubMed] [Google Scholar]
- 17.Dromain C, Thibault F, Diekmann F, et al. Dual-energy contrast-enhanced digital mammography: initial clinical results of a multireader, multicase study. Breast cancer research: BCR. 2012;14(3):R94. doi: 10.1186/bcr3210. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Dobbins JT., 3rd Tomosynthesis imaging: at a translational crossroads. Medical physics. 2009;36(6):1956–67. doi: 10.1118/1.3120285. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Dobbins JT, 3rd, Godfrey DJ. Digital x-ray tomosynthesis: current state of the art and clinical potential. Physics in medicine and biology. 2003;48(19):R65–106. doi: 10.1088/0031-9155/48/19/r01. [DOI] [PubMed] [Google Scholar]
- 20.Poplack SP, Tosteson TD, Kogel CA, Nagy HM. Digital breast tomosynthesis: initial experience in 98 women with abnormal digital screening mammography. AJR American journal of roentgenology. 2007;189(3):616–23. doi: 10.2214/AJR.07.2231. [DOI] [PubMed] [Google Scholar]
- 21.Feng SS, Sechopoulos I. Clinical digital breast tomosynthesis system: dosimetric characterization. Radiology. 2012;263(1):35–42. doi: 10.1148/radiol.11111789. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Harvey JA, Bovbjerg VE. Quantitative assessment of mammographic breast density: relationship with breast cancer risk. Radiology. 2004;230(1):29–41. doi: 10.1148/radiol.2301020870. [DOI] [PubMed] [Google Scholar]
- 23.McCormack VA, dos Santos Silva I. Breast density and parenchymal patterns as markers of breast cancer risk: a meta-analysis. Cancer epidemiology, biomarkers & prevention: a publication of the American Association for Cancer Research, cosponsored by the American Society of Preventive Oncology. 2006;15(6):1159–69. doi: 10.1158/1055-9965.EPI-06-0034. [DOI] [PubMed] [Google Scholar]
- 24.Boyd NF, Guo H, Martin LJ, et al. Mammographic density and the risk and detection of breast cancer. The New England journal of medicine. 2007;356(3):227–36. doi: 10.1056/NEJMoa062790. [DOI] [PubMed] [Google Scholar]
- 25.van Gils CH, Otten JD, Verbeek AL, Hendriks JH. Mammographic breast density and risk of breast cancer: masking bias or causality? European journal of epidemiology. 1998;14(4):315–20. doi: 10.1023/a:1007423824675. [DOI] [PubMed] [Google Scholar]
- 26.Whitehead J, Carlile T, Kopecky KJ, et al. Wolfe mammographic parenchymal patterns. A study of the masking hypothesis of Egan and Mosteller. Cancer. 1985;56(6):1280–6. doi: 10.1002/1097-0142(19850915)56:6<1280::aid-cncr2820560610>3.0.co;2-8. [DOI] [PubMed] [Google Scholar]
- 27.Sala E, Warren R, McCann J, et al. Mammographic parenchymal patterns and mode of detection: implications for the breast screening programme. Journal of medical screening. 1998;5(4):207–12. doi: 10.1136/jms.5.4.207. [DOI] [PubMed] [Google Scholar]
- 28.Berg WA, Campassi C, Langenberg P, Sexton MJ. Breast Imaging Reporting and Data System: inter- and intraobserver variability in feature analysis and final assessment. AJR American journal of roentgenology. 2000;174(6):1769–77. doi: 10.2214/ajr.174.6.1741769. [DOI] [PubMed] [Google Scholar]
- 29.Ooms EA, Zonderland HM, Eijkemans MJ, et al. Mammography: interobserver variability in breast density assessment. Breast. 2007;16(6):568–76. doi: 10.1016/j.breast.2007.04.007. [DOI] [PubMed] [Google Scholar]
- 30.Heine JJ, Fowler EE, Flowers CI. Full field digital mammography and breast density: comparison of calibrated and noncalibrated measurements. Academic radiology. 2011;18(11):1430–6. doi: 10.1016/j.acra.2011.07.011. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Berg WA, Zhang Z, Lehrer D, et al. Detection of breast cancer with addition of annual screening ultrasound or a single screening MRI to mammography in women with elevated breast cancer risk. JAMA: the journal of the American Medical Association. 2012;307(13):1394–404. doi: 10.1001/jama.2012.388. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.Kelly KM, Richwald GA. Automated whole-breast ultrasound: advancing the performance of breast cancer screening. Seminars in ultrasound, CT, and MR. 2011;32(4):273–80. doi: 10.1053/j.sult.2011.02.004. [DOI] [PubMed] [Google Scholar]
- 33.Kelly KM, Dean J, Comulada WS, Lee SJ. Breast cancer detection using automated whole breast ultrasound and mammography in radiographically dense breasts. European radiology. 2010;20(3):734–42. doi: 10.1007/s00330-009-1588-y. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34.Saslow D, Boetes C, Burke W, et al. American Cancer Society guidelines for breast screening with MRI as an adjunct to mammography. CA: a cancer journal for clinicians. 2007;57(2):75–89. doi: 10.3322/canjclin.57.2.75. [DOI] [PubMed] [Google Scholar]
- 35.Gail MH, Brinton LA, Byar DP, et al. Projecting individualized probabilities of developing breast cancer for white females who are being examined annually. Journal of the National Cancer Institute. 1989;81(24):1879–86. doi: 10.1093/jnci/81.24.1879. [DOI] [PubMed] [Google Scholar]
- 36.Claus EB, Risch N, Thompson WD. Autosomal dominant inheritance of early-onset breast cancer. Implications for risk prediction. Cancer. 1994;73(3):643–51. doi: 10.1002/1097-0142(19940201)73:3<643::aid-cncr2820730323>3.0.co;2-5. [DOI] [PubMed] [Google Scholar]
- 37.Berry DA, Iversen ES, Jr, Gudbjartsson DF, et al. BRCAPRO validation, sensitivity of genetic testing of BRCA1/BRCA2, and prevalence of other breast cancer susceptibility genes. Journal of clinical oncology: official journal of the American Society of Clinical Oncology. 2002;20(11):2701–12. doi: 10.1200/JCO.2002.05.121. [DOI] [PubMed] [Google Scholar]
- 38.Tyrer J, Duffy SW, Cuzick J. A breast cancer prediction model incorporating familial and personal risk factors. Statistics in medicine. 2004;23(7):1111–30. doi: 10.1002/sim.1668. [DOI] [PubMed] [Google Scholar]
- 39.Taneja C, Edelsberg J, Weycker D, et al. Cost effectiveness of breast cancer screening with contrast-enhanced MRI in high-risk women. Journal of the American College of Radiology: JACR. 2009;6(3):171–9. doi: 10.1016/j.jacr.2008.10.003. [DOI] [PubMed] [Google Scholar]
- 40.Plevritis SK, Kurian AW, Sigal BM, et al. Cost-effectiveness of screening BRCA1/2 mutation carriers with breast magnetic resonance imaging. JAMA: the journal of the American Medical Association. 2006;295(20):2374–84. doi: 10.1001/jama.295.20.2374. [DOI] [PubMed] [Google Scholar]
- 41.Kriege M, Brekelmans CT, Boetes C, et al. Efficacy of MRI and mammography for breast-cancer screening in women with a familial or genetic predisposition. The New England journal of medicine. 2004;351(5):427–37. doi: 10.1056/NEJMoa031759. [DOI] [PubMed] [Google Scholar]
- 42.Hendrick RE. Radiation doses and cancer risks from breast imaging studies. Radiology. 2010;257(1):246–53. doi: 10.1148/radiol.10100570. [DOI] [PubMed] [Google Scholar]