

Abstract
Context
Spiritual care (SC) from medical practitioners is infrequent at the end of life (EOL) despite national standards.
Objectives
The study aimed to describe nurses' and physicians' desire to provide SC to terminally ill patients and assess 11 potential SC barriers.
Methods
This was a survey-based, multisite study conducted from October 2008 through January 2009. All eligible oncology nurses and physicians at four Boston academic centers were approached for study participation; 339 nurses and physicians participated (response rate = 63%).
Results
Most nurses and physicians desire to provide SC within the setting of terminal illness (74% vs. 60%, respectively; P = 0.002); however, 40% of nurses/physicians provide SC less often than they desire. The most highly endorsed barriers were “lack of private space” for nurses and “lack of time” for physicians, but neither was associated with actual SC provision. Barriers that predicted less frequent SC for all medical professionals included inadequate training (nurses: odds ratio [OR] = 0.28, 95% confidence interval [CI] = 0.12–0.73, P = 0.01; physicians: OR = 0.49, 95% CI = 0.25–0.95, P = 0.04), “not my professional role” (nurses: OR = 0.21, 95% CI = 0.07–0.61, P = 0.004; physicians: OR = 0.35, 95% CI = 0.17–0.72, P = 0.004), and “power inequity with patient” (nurses: OR = 0.33, 95% CI = 0.12–0.87, P = 0.03; physicians: OR = 0.41, 95% CI = 0.21–0.78, P = 0.007). A minority of nurses and physicians (21% and 49%, P = 0.003, respectively) did not desire SC training. Those less likely to desire SC training reported lower self-ratings of spirituality (nurses: OR = 5.00, 95% CI = 1.82–12.50, P = 0.002; physicians: OR = 3.33, 95% CI = 1.82–5.88, P < 0.001) and male gender (physicians: OR = 3.03, 95% CI = 1.67–5.56, P < 0.001).
Conclusion
SC training is suggested to be critical to the provision of SC in accordance with national care quality standards.
Keywords: Palliative care, religion, spirituality, spiritual care, hidden curriculum
Introduction
Spiritual care (SC) of patients at the end of life (EOL) has been identified as a core domain by the World Health Organization,1 the National Consensus Project on Quality Palliative Care (NCPQPC),2 and highlighted as an EOL priority by the Joint Commission.3 The NCPQPC outlines the importance of an interdisciplinary medical team assessing patients' spiritual, religious, and existential dimensions of care and addressing spiritual needs.2 Likewise, the Joint Commission requires health care institutions to provide quantifiable measures demonstrating “care and services that accommodate[s] patient's… spiritual EOL needs” and staff education concerning the unique needs of patients at the EOL.3 These standards are grounded in an evidence base that outlines the importance of religion/spirituality (R/S) within an EOL experience4 and the prominent spiritual needs encountered during life-threatening illness.5–7 National and international guidelines also are based on prospective studies that have found associations between medical team spiritual support and 1) patient quality of life,4,8,9 2) decreased aggressive care at the EOL,8 and 3) significantly higher costs when SC is absent.10
Although community clergy and hospital chaplains hold a central role in providing SC, the role of medical professionals is less clear. Consequently, empirical data grounding medical professional SC provision is needed. Despite palliative care guidelines1–3 and research supporting the importance of its inclusion in EOL care, prior studies indicate that 6–26% of patients receive SC from their medical teams, revealing a gap between extant policies and current practice.11–13 This gap does not appear to be primarily related to a lack of perceived importance of EOL SC by patients or clinicians as most patients, nurses, and physicians in an EOL care setting agree that R/S ought to be addressed by medical professionals.13,14 Rather, barriers appear to be operating to limit SC provision despite a frequent awareness of its importance. Hence, to advance a holistic approach to palliative care provision that includes patient R/S, an understanding of medical professional barriers to SC provision is required. However, data exploring such barriers are limited. In studies of self-reported barriers to SC provision, reasons cited by nurses and physicians for infrequent SC provision include insufficient time to discuss R/S and personal discomfort with R/S.14–17 Although illuminating as to potential barriers at play, these studies do not examine the relationship of these barriers to actual SC provision to patients. Furthermore, there are other putative barriers that require investigation, such as the asymmetry between the U.S. population and medical professionals in religious characteristics, including religious affiliation and self-reported religiosity and spirituality;13,18 these factors may prompt medical professionals to avoid R/S issues, rather than risk creating discomfort or offense.14,19,20 By understanding these barriers to SC, steps can be identified in how to best overcome them and facilitate the provision of SC to patients. Hence, critical to advancing SC as a central dimension of EOL care in accordance with national care quality standards2,3 is an understanding of what factors limit actual provision of SC to patients at the EOL.
The Religion and Spirituality in Cancer Care study was designed to measure perceptions of SC barriers from the viewpoints of nurses and physicians caring for terminally ill patients. The study investigated three hypotheses, namely 1) nurses and physicians desire to provide SC to terminally ill patients, but 2) encounter multiple barriers that limit its provision, and 3) medical professional demographic and R/S characteristics would influence perceptions of SC barriers and their desire to receive SC training.
Methods
Sample
Enrollment ran from October 2008 through January 2009, and oncology nurses and physicians were eligible if they cared for patients with incurable cancer. Practitioners were from four Boston (U.S.) academic centers, namely Beth Israel Deaconess Medical Center, Boston University Medical Center, Brigham and Women's Hospital, and Dana-Farber Cancer Institute.
Protocol
Nurses and physicians were identified by collecting e-mail information from departmental databases, and were invited to participate via an e-mail containing a link to an online survey. All participants provided informed consent according to protocols approved by each site's human subjects committee (implied consent for nurses/physicians based on all elements of consent included in the survey introduction). Respondents received a $10 gift card for participation. Of 537 nurses and physicians contacted, 339 responded (response rate = 63%; 59% among physicians, 72% among nurses). Eight practitioners indicated that they did not provide care to incurable cancer patients, and nine did not finish the questionnaire, yielding 322 respondents (95% of 339, 204 physicians and 118 nurses).
The survey defined for participants the terms religion, spirituality, and SC, and included eight specific SC examples based on the literature2,21 (see Table 1 for definitions).
Table 1. Religion and Spirituality Cancer Care Survey Definitions, Questions, and Response Options.
| Definitions | |
|---|---|
| Spirituality | |
| Spirituality is a search for and/or a connection to what is divine or sacred (e.g., God or a higher power). | |
| Religion | |
| Religion is a tradition of spiritual beliefs and practices shared by a group of people. | |
| Spiritual care | |
| Spiritual care from doctors or nurses is care that supports a patient's spiritual health. | |
| It not clear what are the best ways (if at all) that doctors and nurses should give spiritual care. Some possible types of spiritual care include a doctor or nurse: | |
| 1. Asking about a patient's religious/spiritual background to be aware of whether or not it is important to them. | |
| 2. Encouraging a patient's spiritual activities or beliefs that are helpful to them. For example, a doctor or nurse saying to a patient: “I'm so glad that your faith gives you strength during this difficult time.” | |
| Or | |
| 3. Asking questions that invite patients to talk about spiritual matters if they want to. For example, a doctor or nurse asking, “What helps you find meaning during this difficult time?” | |
| Survey category | Response options |
| Religious/spiritual characteristics | |
| To what extent do you consider yourself a religious person? | Very religious |
| Moderately religious | |
| Slightly religious | |
| Not religious at all | |
| To what extent do you consider yourself a spiritual person? | Very spiritual |
| Moderately spiritual | |
| Slightly spiritual | |
| Not spiritual at all | |
| Please indicate the religious tradition that most closely describes you: | Catholic |
| Protestant | |
| Jewish | |
| Muslim | |
| Buddhist | |
| Hindu | |
| No religious tradition | |
| Other (please specify) | |
| Please indicate the degree to which you agree with the following statement: “My religious/spiritual beliefs influence my practice of medicine.” | Strongly agree |
| Agree | |
| Neutral | |
| Disagree | |
| Strongly disagree | |
| Frequency of spiritual care | |
| How often do you offer any type of spiritual care during the course of your relationship with an advanced, incurable cancer patient? | Never |
| Rarely | |
| Seldom | |
| Occasionally | |
| How often do you desire to offer any type of spiritual during the course of your relationship with an advanced, incurable cancer patient | Frequently |
| Almost always | |
| Always | |
| Think back to the past three advanced, incurable cancer patients you saw. To how many of those patients have you provided any type of spiritual care during the course of their treatment? | None |
| 1 Patient | |
| 2 Patients | |
| 3 Patients | |
| Barriers to spiritual care | |
| Below is a list of reasons spiritual care might not be performed even when ideally it would be performed. How significant are each of the following factors in limiting you from providing spiritual care? | Not significant |
| Slightly significant | |
| Moderately significant | |
| Very significant | |
| |
| Spiritual care training | |
| Have you ever received training in providing any type of spiritual care? | Yes |
| Would you desire further training in how to appropriately provide spiritual care to your patients? | No |
Measures
Sample Characteristics
Practitioner demographic information was self-reported including age, gender, race, field of oncology, and years of practice.
Religiousness/Spirituality
Table 1 provides information on the survey instrument. Practitioners reported religiousness and spirituality using items from the validated Multidimensional Measure of Religiousness and Spirituality.22 Also assessed were religious affiliation, religious service attendance,22 and intrinsic religiosity (the degree to which religiousness permeates daily life).18
Desire to Provide SC and Actual Frequency
Practitioners were asked on seven-point scales, from “never” to “always”: “How often do you DESIRE to offer any type of SC to advanced, incurable cancer patients?” and “How often do you offer any type of SC during the course of your relationship with an advanced, incurable cancer patient?” A quantitative assessment of actual SC provision was determined by nurses and physicians reporting—after reviewing the eight SC examples—on their SC provision to the last three patients with advanced cancer seen in clinic. For each of these three patients, practitioners indicated whether or not they had provided any form of SC at any point during the patient's care.
Medical Professional Barriers to SC
Items assessing 11 SC barriers were developed by an expert panel and piloted among oncology nurses and physicians. Participants were asked: “Below is a list of reasons SC might NOT be performed even when IDEALLY it would be performed. How significant are each of the following factors in limiting you from providing spiritual care?” Response options included “not significant,” “slightly significant,” “moderately significant,” and “very significant.” In exploratory analysis, item ratings were summed to generate an overall SC barrier score (range 11–44) measuring a cumulative effect of the 11 barriers.
Medical Professional Desire to Receive SC Training
Practitioners answered “yes/no” to SC training: “Would you desire further training in how to appropriately provide SC to your patients?”
Statistical Analysis
Chi-squared tests were used to compare demographic information between nurses and physicians. Chi-squared tests also were used to compare nurse and physician perceptions of SC frequency, desire to provide SC, and SC barriers.
Univariate (UVA) and multivariate (MVA) linear and logistic regression analyses were used to identify predictors of SC barrier ratings for nurses and physicians, predictors of actual SC provision for nurses and physicians, and predictors of lack of desire for future SC training. The MVAs included nurse/MD professional characteristics and R/S variables (religiousness, spirituality religious tradition, and intrinsic religiosity).
All reported P-values are two sided and considered significant when P-value is lower than 0.05. Statistical analyses were performed with R v. 2.13.1 (Wirtschaftsuniversität Wien, Vienna, Austria).
Results
Sample Characteristics
Sample characteristics are reported in Table 2. Nurses and physicians differed in R/S characteristics. Although nurses were most likely to be Catholic, physicians were most likely to be Jewish. Nurses were more religious (P = 0.02) and spiritual than physicians (P < 0.001).
Table 2. Sample Characteristics of Oncology Nurses and Physicians Who Care for Patients With Advanced Cancer, N=322.
| Characteristics | Nurses, n (%) (N = 118) | Physicians, n (%) (N = 204) | P-valuea |
|---|---|---|---|
| Female gender | 116 (98) | 88 (42) | <0.001 |
| Age (yrs), mean (SD) | 46 (9.1) | 41 (9.8) | <0.001 |
| Race/ethnicityb,c | |||
| White | 108 (94) | 154 (77) | <0.001 |
| Black | 2 (2) | 4 (2) | |
| Asian, Indian, Pacific Islander | 2 (2) | 35 (17) | |
| Hispanic | 1 (1) | 3 (2) | |
| Other | 1 (1) | 5 (2) | |
| Field of oncology | |||
| Medical | 91 (77) | 113 (54) | <0.001 |
| Radiation | 13 (11) | 46 (22) | |
| Surgical | 9 (8) | 34 (16) | |
| Palliative care | 5 (4) | 16 (8) | |
| Years in practiceb | |||
| Resident or fellow | – | 67 (33) | <0.001 |
| 1–5 | 24 (20) | 38 (17) | |
| 6–10 | 24 (20) | 35 (17) | |
| 11–15 | 15 (13) | 23 (11) | |
| 16–20 | 12 (10) | 20 (10) | |
| 21+ | 43 (36) | 26 (12) | |
| Religiousnessb,d | |||
| Not at all religious | 29 (26) | 62 (31) | 0.02 |
| Slightly religious | 33 (30) | 66 (33) | |
| Moderately religious | 43 (38) | 54 (27) | |
| Very religious | 7 (6) | 17 (9) | |
| Spiritualityb,d | |||
| Not at all spiritual | 6 (5) | 30 (15) | <0.001 |
| Slightly spiritual | 18 (16) | 57 (29) | |
| Moderately spiritual | 58 (52) | 75 (38) | |
| Very spiritual | 30 (27) | 37 (19) | |
| Religious traditionb | |||
| Catholic | 70 (63) | 47 (24) | <0.001 |
| Protestant | 17 (15) | 45 (23) | |
| Jewish | 6 (5) | 51 (26) | |
| Muslim | 0 (0) | 2 (1) | |
| Hindu | 2 (2) | 11 (6) | |
| Buddhist | 0 (0) | 3 (2) | |
| No religious tradition | 6 (5) | 22 (11) | |
| Other | 11 (10) | 18 (9) | |
| Intrinsic religiositye | |||
| Strongly disagree | 31 (28) | 51 (25.6) | 0.827 |
| Somewhat disagree | 11 (10) | 22 (11.1) | |
| Neutral | 26 (23) | 45 (22.6) | |
| Somewhat agree | 30 (27) | 47 (23.6) | |
| Strongly agree | 14 (12) | 34 (17.1) |
P-values based on Chi-squared test for categorical data. Age based on F-statistic from ANOVA.
Categories missing 5% or more of responses. Category percentages not adding to 100 are because of rounding.
Refused to answer: two nurses and five physicians.
In combining religiosity and spirituality, nurses were more likely to rate themselves as “moderately” or “very” spiritual and “not at all” or “slightly” religious (38%) in contrast to physicians (25%, P < 0.001). Physicians were more likely to rate themselves as “not at all” or “slightly” religious and spiritual (39%), in contrast to nurses (18%, P < 0.001).
Intrinsic religiosity is the degree to which one's religiousness permeates one's daily life, including one's vocation. It was assessed based on a question from a national study of physicians:16 “Please indicate the degree to which you agree with the following statement: My religious/spiritual beliefs influence my practice of medicine,” and was measured on a five-point scale from “strongly agree” to “strongly disagree” and within analyses dichotomized to “strongly agree/somewhat agree” vs. “neutral/somewhat disagree/strongly disagree.”
Desire to Provide SC and Actual Frequency
Most nurses and physicians desire to at least “occasionally” provide SC when caring for patients with a terminal illness (74% vs. 60%, respectively; P = 0.002). Fig. 1 illustrates nurses' and physicians' desire to provide SC compared with descriptive assessments of SC frequency (SC frequency has been previously reported13). A large minority of nurses and physicians provided SC less frequently than desired (39% and 41%, respectively), whereas a small minority (9% and 9.5%, respectively) provided SC more frequently than desired. There was a significant difference between desire to provide SC and reported provision among nurses (P < 0.001) and physicians (P < 0.001).
Fig. 1.
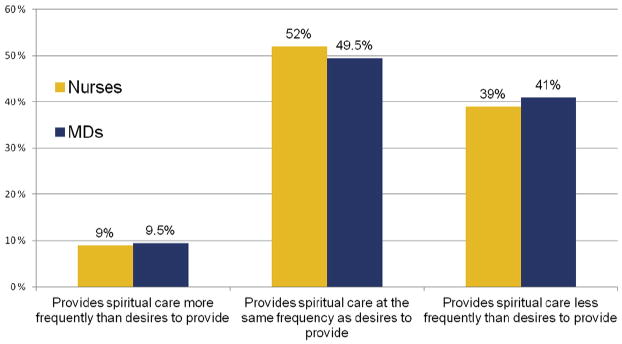
Comparison of nurses' (n = 113) and physicians' (n = 200) desire to provide spiritual care and self-reported frequency of spiritual care provision. On seven-point Likert scales, medical professionals were asked, “How often do you desire to offer any type of spiritual care during the course of your relationship with an advanced, incurable cancer patient?” Nurse/physician responses included: “never” (8%/11%), “rarely” (6%/11%), “seldom” (13%/16%), “occasionally” (34%/20%), “frequently” (18%/23%), “almost always” (11%/8%), and “always” (9%/3%). Nurses and physicians were also asked, “How often do you offer any type of spiritual care during the course of your relationship with an advanced, incurable cancer patient?” Responses are previously published.13
SC Barriers
Table 3 provides nurse and physician perceptions of barriers to providing SC to patients with advanced cancer. On combining nurses and physicians, the most frequently endorsed barriers considered “moderately” or “very significant” included lack of time (72%), inadequate training (61%), lack of privacy (52%), and SC better offered by others (50%). Nurses and physicians significantly differed as professional caregivers concerning how private space, professional roles, and power differences influenced their SC provision (Table 3).
Table 3. Nurse (N = 112)a and Physician (N = 195)b Perceptions of Barriers to Providing Spiritual Care to Patients With Advanced Cancer.
| Rank | Orderc | Nurse Barriers, n (%)d | Physician Barriers, n (%)e | P-valueb |
|---|---|---|---|---|
| #1 | Not enough time | 79 (71) | 142 (73) | 0.39 |
| #2 | Lack of private space to discuss these matters with my patients | 83 (74) | 76 (39) | <0.001 |
| #3 | I have not received adequate training | 67 (60) | 121 (62) | 0.94 |
| #4 | I believe that spiritual care is better done by others on the health care team | 35 (31) | 120 (62) | <0.001 |
| #5 | I am worried that patients will feel uncomfortable | 50 (45) | 86 (44) | 0.12 |
| #6 | I feel uncomfortable engaging these issues with patients whose religious/spiritual beliefs may differ from my own | 37 (33) | 94 (48) | 0.04 |
| #7 | I am personally uncomfortable discussing spiritual issues | 37 (33) | 91 (47) | 0.03 |
| #8 | I do not believe it is my professional role to engage patient spirituality | 26 (23) | 87 (45) | <0.001 |
| #9 | I am worried that the power inequity between patient and (nurse/doctor) makes spiritual care inappropriate | 27 (24) | 84 (43) | <0.001 |
| #10 | Religion/spirituality is not important to me personally | 23 (21) | 54 (28) | 0.40 |
| #11 | I do not believe cancer patients want spiritual care from (nurses/doctors) | 16 (14) | 39 (20) | 0.04 |
Sample size reduced from 118, with six respondents with missing data.
Sample size reduced from 204, with nine respondents with missing data.
Rank order combines nurse and physician responses on most highly endorsed barriers to spiritual care.
Responses dichotomized to not significant (not/slightly significant) vs. significant (moderately/very significant).
P-values based on Chi-squared test.
Predictors of SC Infrequency
The MVAs examining the relationship of reported barriers to actual SC practices by nurses and physicians are shown in Table 4. In MVA models predicting lack of SC provision to patients recently seen in clinic, significant barriers experienced by both nurses and physicians included inadequate training, a belief that SC is not part of the medical professional's role, and worry that the power inequity between patient and clinician makes SC inappropriate.
Table 4. Multivariable Predictors of Barriers Hindering Actual Spiritual Care Provision by Nurses and Physicians to Patients With Advanced Cancera.
| Nurses | Physicians | |||||
|---|---|---|---|---|---|---|
|
|
|
|||||
| Parameters | Odds Ratiob | 95% CI | P-valuec | Odds Ratiob | 95% CI | P-valuec |
| Not enough time | 0.73 | 0.29–10.85 | 0.51 | 10.72 | 0.82–3.62 | 0.15 |
| Lack of private space to discuss these matters with my patients | 0.88 | 0.34–2.25 | 0.79 | 0.93 | 0.46–1.91 | 0.85 |
| I have not received adequate training | 0.25 | 0.09–0.67 | 0.006 | 0.49 | 0.25–0.98 | 0.04 |
| I believe that spiritual care is better done by others on the health care team | 0.31 | 0.13–0.77 | 0.01 | 0.68 | 0.34–1.35 | 0.27 |
| I am worried that patients will feel uncomfortable | 0.65 | 0.28–1.50 | 0.31 | 0.35 | 0.18–0.70 | 0.003 |
| I feel uncomfortable engaging these issues with patients whose religious/spiritual beliefs may differ from my own | 0.20 | 0.07–0.56 | 0.002 | 0.51 | 0.26–1.00 | 0.049 |
| I am personally uncomfortable discussing spiritual issues | 0.46 | 0.18–1.12 | 0.09 | 0.27 | 0.14–0.54 | <0.001 |
| I do not believe it is my professional role to engage patient spirituality | 0.21 | 0.07–0.61 | 0.004 | 0.37 | 0.18–0.75 | 0.006 |
| I am worried that the power inequity between patient and (nurse/physician) makes spiritual care inappropriate | 0.32 | 0.12–0.85 | 0.02 | 0.39 | 0.20–0.76 | 0.006 |
| Religion/spirituality is not important to me personally | 0.52 | 0.17–1.596 | 0.25 | 1.10 | 0.47–2.61 | 0.83 |
| I do not believe cancer patients want spiritual care from (nurses/physicians) | 0.62 | 0.20–1.97 | 0.42 | 0.25 | 0.11–0.61 | 0.002 |
Provision of spiritual care defined as any vs. no provision of spiritual care during the course of a nurse or physicians' relationship with the last three advanced cancer patients seen in clinic. Frequency of spiritual care provision has been previously published.12
Multivariable analysis controlled for gender, race (white vs. non-white), years of medical practice (>11 years vs. 11+years), religiousness (“not at all/slightly religious” vs. “moderately/very religious”), spirituality (“not at all/slightly spiritual” vs. “moderately/very spiritual”), religious tradition (Christian vs. non-Christian), and intrinsic religiosity (strong disagree-neutral vs. agree/strongly agree), and religious service attendance (one to three times per month or less vs. one to three times per month or more).
P<0.05 considered significant (bolded values).
Personal and Professional Characteristics and SC Barriers
The MVAs assessed physician and nurse characteristics and their relationship to overall SC barriers scores (score of 11 SC barrier ratings, higher scores indicating greater perceived barriers to SC). In MVA assessing nurse perceptions of SC barriers at the EOL, only lower spirituality predicted higher ratings of SC barriers (β̂ = 3.44, P = 0.038). In MVA assessing physician barriers, predictors of increased perceptions of SC barriers included female gender (β̂ = 5.56, P = 0.02), years practiced more than 11 years (β̂ = 5.1, P = 0.001), non-Christian religious denomination (β̂ = 3.51, P = 0.03), and lack of SC training (β̂ = 3.01, P = 0.04).
A minority of nurses and physicians (21% and 49%, respectively, P = 0.003) said that they did not desire future training in SC. In MVA models predicting nurse lack of desire for SC training, only lower spirituality (odds ratio [OR] = 5.00, 95% confidence interval [CI] = 1.82–12.50, P = 0.002) was significantly associated with lack of desire for SC training. Physician predictors for lack of desire for SC training include lower spirituality (OR = 3.33, 95% CI = 1.82–5.88, P < 0.001), practicing for more than 11 years (OR = 2.00, 95% CI = 1.09–3.57, P = 0.02), low intrinsic religiosity (OR = 1.92, 95% CI = 1.09–3.45, P = 0.02), and male gender (OR = 3.03, 95% CI = 1.67–5.56, P < 0.001).
Discussion
This study investigated three hypotheses related to the potential role of barriers inhibiting the provision of SC by medical professionals to patients with advanced cancer. First, the hypothesis that most medical professionals desire to provide SC to terminally ill patients was supported in light of the finding that most nurses (74%) and physicians (60%) desire to provide SC to their advanced cancer patients. In addition, a large minority of nurses (39%) and physicians (41%) provide SC less often than desired (Fig. 1). Second, the hypothesis that medical professionals experience multiple barriers that limit provision of SC was substantiated by the multiple barriers identified as limiting SC provision, with the most frequently identified barriers for nurses and physicians being lack of time and inadequate training (Table 3). Notable differences between nurses and physicians also were found: most nurses who said that they lack private space to provide SC and most physicians who agreed that “SC is better done by others.” We also found distinctions between perceived barriers and those actually associated with SC provision. Lack of SC training was the only barrier that was endorsed by most nurses and physicians (Table 3) and found in MVA to be associated with less frequent SC by both nurses (OR = 0.25, P = 0.006) and physicians (OR = 0.49, P = 0.04). Surprisingly, the barriers thought by most medical professionals to significantly limit SC (i.e., insufficient time and lack of private space) were not associated with actual SC provision. Third, multivariate analysis upheld the hypothesis that personal and professional characteristics among medical professionals were associated with increased perceptions of SC barriers and decreased desire to receive SC training. In summary, SC barriers are widely recognized by medical professionals, associated with less frequent SC provision, and intensified by personal and professional characteristics.
This study highlights the importance of SC training for nurses and physicians as the primary means to complement SC provided by clergy and chaplains, and incorporate SC into the care of patients facing serious illness in accordance with national care quality standards.2,3 Lack of training was the only barrier endorsed by most nurses and physicians and found in MVA to be associated with less frequent SC provision to patients. The SC training also holds potential to address other identified critical barriers to SC provision, for example, by increasing clinician awareness of their SC role and the role of critical SC providers (e.g., chaplains) and by developing strategies that assist a patient-centered approach to SC that does not compromise patient autonomy. Furthermore, SC training has the potential to also address other identified barriers to SC provision at the EOL. The SC training can be crafted to specifically address SC discomfort among medical professionals by enabling their own reflection on personal R/S views (including the lack thereof) and by providing general SC competencies across various R/S traditions.23 The potential for SC training to powerfully influence provision of SC at the EOL is highlighted by a previous report indicating that medical professionals who had previously received SC training had a seven- to 11-fold greater odds of providing SC to their patients with advanced cancer, after adjusting for personal and professional confounders.13
Notably, although most nurses (79%) and physicians (51%) would like to receive SC training, only 12–20% have prior training.13,17 In addition, this study indicates that nurse and physician desire to receive SC training is influenced by personal characteristics. Nurses with lower self-reported spirituality had a fivefold reduced odds of desiring SC training in comparison with more spiritual nurses. Likewise, several characteristics (lower spirituality, male gender, 11+ years in practice, and low intrinsic religiosity) predicted physician lack of desire for SC training. Hence, the gap between national guidelines and current practices11–13 will likely remain unaltered until SC training becomes standardized within routine medical curricula24,25 for all professional staff caring for patients at the EOL. Training in SC provision would assist those nurses and physicians who desire to provide SC more frequently than actual practice (Fig. 1) by providing an educational foundation needed to overcome barriers to SC.14 Likewise, those who are pre-disposed to not seek SC training because of personal characteristics would be equipped to recognize patients' R/S needs; draw on other SC providers within the medical team; and, therefore, use a more patient-centered approach to care at the EOL.23 Although the Joint Commission already requires staff education concerning the unique needs of patients at the EOL, including patient R/S,3 this study indicates that where this requirement is fulfilled, the frequency of SC at the EOL would significantly increase.
In addition, this study underscores a distinction between barriers perceived as obstacles to SC but not associated with SC frequency and those barriers that measurably limit SC provision. This distinction is important to locate how national quality standards may be more widely disseminated in the medical care of the terminally ill. Our study points to three barriers associated with less frequent SC, held in common by nurses and physicians: 1) SC is not part of one's professional role, 2) worry that power inequities render SC an inappropriate medical activity, and 3) lack of training. Engagement of these specific barriers may be critical to narrow the gap between national guidelines2,3 and clinical practice.13,14 Notably, although insufficient time and private space are widely considered to impede SC,15–17 these barriers were not associated with SC frequency, suggesting that although these issues may be important to address as felt barriers for clinicians, they are not central barriers to SC provision. This study also dispels another popular misconception that medical professionals do not value R/S on a professional level. A significant majority desire to provide SC in an EOL cancer context, and Fig. 1 illustrates how a large subset of medical professionals desire to provide SC on a more frequent basis.18
Key barriers are tied to basic conceptual questions related to the relationship of medical practice and R/S. Those who contend that medicine and R/S should remain separate have appealed primarily to ethical arguments that R/S falls outside professional boundaries, risks patient autonomy, and requires extensive training.19,20,26,27 From this viewpoint, barriers limiting SC are not to be overcome per se but serve as the very groundwork justifying a necessary separation. However, as evidence has accumulated to demonstrate the central relevance of patient R/S to the experience of serious illness,4–7 including being major determinants of patient quality of life and medical care at the EOL, these ethical arguments for separation are being remolded to critical issues to be considered in providing SC in a patient-centered fashion at the EOL. This transformation is reflected in the presence of international/national SC guidelines1–3 highlighting both the central relevance of SC within palliative care and the necessity for a patient-centered approach to SC that does not impose R/S views and/or violate professional roles. This is likewise reflected within this study's elucidation of how medical professionals conceptualize the relationship of spirituality and medicine. First, most medical professionals hold at least an occasional desire to provide SC to terminally ill patients, including 40% who desire to provide SC more often than they actually practice. Second, most desire to receive future training. Both points indicate that medical professionals understand their own professional role to overlap with their patients' EOL spiritual needs. We also have previously reported that most terminally ill patients, nurses, and physicians agree that spiritual support from medical professionals is important, appropriate, and positively beneficial to patients and the patient-clinician relationship.6,13,14,28 Indeed, the Religion and Spirituality in Cancer Care study provides a snapshot of how most conceptualize the relationship of EOL medical care and R/S in an integrated manner.6,13,14,28,29
Limitations of this study include that, although the response rates for nurses and physicians were high, selection bias is still possible. Furthermore, participants surveyed were from a single, U.S. urban region. However, given this region's lower national averages of R/S,30 findings likely underestimate desire for SC in the EOL setting. Finally, the generalizability of these findings to other diseases or stages of illness remains unclear.
Conclusion
Nurses and physicians frequently desire to provide SC at the EOL but also encounter barriers to its provision. This study points toward SC training as the critical next step to narrow the gap between national care quality standards2,3 and the current infrequent practice of SC at the EOL.13 Evidence-based SC training holds promise to advance SC competency and practice among medical professionals and to improve patient well-being4,8,9 and medical care quality at the EOL.8,10
Acknowledgments
This research was supported in part by an American Society of Clinical Oncology Young Investigator Award and Career Development Award (T. A. B.), a HealthCare Chaplaincy award (T. A. B.), Templeton Foundation Awards (M. J. B. and T. J. V.), and a University of Chicago Program in Religion and Medicine Faculty Scholars Award (M. J. B.). None of the authors have relationships with any entities having financial interest in this topic.
References
- 1.World Health Organization. Palliative care: Symptom management and end of life care. [Accessed May 1, 2013];Integrated management of adolescent and adult illness. 2004 Available from http://www.who.int/hiv/pub/imai/genericpalliativecare082004.pdf.
- 2.National Consensus Project. Clinical practice guidelines for quality palliative care. 2nd. Pittsburgh, PA: National Consensus Project; 2013. [Google Scholar]
- 3.The Joint Commission. Spirituality, religion, beliefs, and cultural diversity. JCAHO's Standards/Elements of Performance Manual for Hospitals E-dition. 2013 PC. 02.02.13. [Google Scholar]
- 4.Steinhauser KE, Christakis NA, Clipp EC, et al. Factors considered important at the end of life by patients, family, physicians, and other care providers. JAMA. 2000;284:2476–2482. doi: 10.1001/jama.284.19.2476. [DOI] [PubMed] [Google Scholar]
- 5.Alcorn SR, Balboni MJ, Prigerson HG, et al. “If God wanted me yesterday, I wouldn't be here today”: religious and spiritual themes in patients' experiences of advanced cancer. J Palliat Med. 2010;13:581–588. doi: 10.1089/jpm.2009.0343. [DOI] [PubMed] [Google Scholar]
- 6.Winkelman WD, Lauderdale K, Balboni MJ, et al. The relationship of spiritual concerns to the quality of life of advanced cancer patients: preliminary findings. J Palliat Med. 2011;14:1022–1028. doi: 10.1089/jpm.2010.0536. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Delgado-Guay MO, Hui D, Parsons HA, et al. Spirituality, religiosity, and spiritual pain in advanced cancer patients. J Pain Symptom Manage. 2011;41:986–994. doi: 10.1016/j.jpainsymman.2010.09.017. [DOI] [PubMed] [Google Scholar]
- 8.Balboni TA, Paulk ME, Balboni MJ, et al. Provision of spiritual care to patients with advanced cancer: associations with medical care and quality of life near death. J Clin Oncol. 2010;28:445–452. doi: 10.1200/JCO.2009.24.8005. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Brady MJ, Peterman AH, Fitchett G, Mo M, Cella D. A case for including spirituality in quality of life measurement in oncology. Psychooncology. 1999;8:417–428. doi: 10.1002/(sici)1099-1611(199909/10)8:5<417::aid-pon398>3.0.co;2-4. [DOI] [PubMed] [Google Scholar]
- 10.Balboni T, Balboni M, Paulk ME, et al. Support of cancer patients' spiritual needs and associations with medical care costs at the end of life. Cancer. 2011;117:5383–5391. doi: 10.1002/cncr.26221. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Astrow AB, Wexler A, Texeira K, He MK, Sulmasy DP. Is failure to meet spiritual needs associated with cancer patients' perceptions of quality of care and their satisfaction with care? J Clin Oncol. 2007;25:5753–5757. doi: 10.1200/JCO.2007.12.4362. [DOI] [PubMed] [Google Scholar]
- 12.Balboni TA, Vanderwerker LC, Block SD, et al. Religiousness and spiritual support among advanced cancer patients and associations with end-of-life treatment preferences and quality of life. J Clin Oncol. 2007;25:555–560. doi: 10.1200/JCO.2006.07.9046. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Balboni MJ, Sullivan A, Amobi A, et al. Why is spiritual care infrequent at the end of life? Spiritual care perceptions among patients, nurses, and physicians and the role of training. J Clin Oncol. 2013;31:461–467. doi: 10.1200/JCO.2012.44.6443. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Phelps AC, Lauderdale KE, Alcorn S, et al. Addressing spirituality within the care of patients at the end of life: perspectives of patients with advanced cancer, oncologists, and oncology nurses. J Clin Oncol. 2012;30:2538–2544. doi: 10.1200/JCO.2011.40.3766. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Curlin FA, Lawrence RE, Odell S, et al. Religion, spirituality, and medicine: psychiatrists' and other physicians' differing observations, interpretations, and clinical approaches. Am J Psychiatry. 2007;164:1825–1831. doi: 10.1176/appi.ajp.2007.06122088. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Ronaldson S, Hayes L, Aggar C, Green J, Carey M. Spirituality and spiritual caring: nurses' perspectives and practice in palliative and acute care environments. J Clin Nurs. 2012;21:2126–2135. doi: 10.1111/j.1365-2702.2012.04180.x. [DOI] [PubMed] [Google Scholar]
- 17.Ramondetta LM, Sun C, Surbone A, et al. Surprising results regarding MASCC members' beliefs about spiritual care. Support Care Cancer. 2013;21:2991–2998. doi: 10.1007/s00520-013-1863-y. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Curlin FA, Lantos JD, Roach CJ, Sellergren SA, Chin MH. Religious characteristics of U.S. physicians: a national survey. J Gen Intern Med. 2005;20:629–634. doi: 10.1111/j.1525-1497.2005.0119.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Sloan RP, Bagiella E, VandeCreek L, et al. Should physicians prescribe religious activities? N Engl J Med. 2000;342:1913–1916. doi: 10.1056/NEJM200006223422513. [DOI] [PubMed] [Google Scholar]
- 20.Lawrence RJ. The witches' brew of spirituality and medicine. Ann Behav Med. 2002;24:74–76. doi: 10.1207/S15324796ABM2401_09. [DOI] [PubMed] [Google Scholar]
- 21.Lo B, Kates LW, Ruston D, et al. Responding to requests regarding prayer and religious ceremonies by patients near the end of life and their families. J Palliat Med. 2003;6:409–415. doi: 10.1089/109662103322144727. [DOI] [PubMed] [Google Scholar]
- 22.Fetzer Institute. Multidimensional measurement of religiousness/spirituality for use in health research: A report of the Fetzer Institute/National Institute on Aging Working Group. Kalamazoo, MI: Fetzer Institute; 2003. [Google Scholar]
- 23.Puchalski C, Ferrell B, Virani R, et al. Improving the quality of spiritual care as a dimension of palliative care: the report of the Consensus Conference. J Palliat Med. 2009;12:885–904. doi: 10.1089/jpm.2009.0142. [DOI] [PubMed] [Google Scholar]
- 24.Koenig HG, Hooten EG, Lindsay-Calkins E, Meador KG. Spirituality in medical school curricula: findings from a national survey. Int J Psychiatry Med. 2010;40:391–398. doi: 10.2190/PM.40.4.c. [DOI] [PubMed] [Google Scholar]
- 25.Rasinski KA, Kalad YG, Yoon JD, Curlin FA. An assessment of US physicians' training in religion, spirituality, and medicine. Med Teach. 2011;33:944–945. doi: 10.3109/0142159X.2011.588976. [DOI] [PubMed] [Google Scholar]
- 26.Sloan RP, Bagiella E, Powell T. Religion, spirituality, and medicine. Lancet. 1999;353:664–667. doi: 10.1016/s0140-6736(98)07376-0. [DOI] [PubMed] [Google Scholar]
- 27.Post SG, Puchalski CM, Larson DB. Physicians and patient spirituality: professional boundaries, competency, and ethics. Ann Intern Med. 2000;132:578–583. doi: 10.7326/0003-4819-132-7-200004040-00010. [DOI] [PubMed] [Google Scholar]
- 28.Balboni MJ, Babar A, Dillinger J, et al. “It depends”: viewpoints of patients, physicians, and nurses on patient-practitioner prayer in the setting of advanced cancer. J Pain Symptom Manage. 2011;41:836–847. doi: 10.1016/j.jpainsymman.2010.07.008. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Vallurupalli M, Lauderdale K, Balboni MJ, et al. The role of spirituality and religious coping in the quality of life of patients with advanced cancer receiving palliative radiation therapy. J Support Oncol. 2012;10:81–87. doi: 10.1016/j.suponc.2011.09.003. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Pew Forum on Religion & Public Life. U S religions landscape survey. Washington, DC: Pew Research Center; 2008. [Accessed December 4, 2013]. Available from http://religions.pewforum.org/pdf/report-religious-landscape-study-full.pdf. [Google Scholar]