

Abstract
Repair of large ventral hernia is a challenge for even experienced surgeons, as there are large defects with large contents, often with loss of domain. The large defects were bridged by various plastic surgical procedures like myofascial flaps or free flaps with high recurrences and complications. More often, the bridging was done with artificial prosthesis, leaving the defects open. This was accomplished by either open surgery (onlay, inlay, sublay or underlay) or laparoscopic intraperitoneal onlay meshes (IPOMs). However, non-closure of the midline had adverse effects on postural maintenance, respiration, micturition, defecation and biomechanical properties, which have a profound impact on the patients’ overall physical capacity and quality of life. Component separation technique (CST) is a novel answer to the closure of midline with live, active tissues with or without the use of additional prosthesis. Though this technique was originally described in 1990, it has undergone lots of modifications like perforator preserving CST, endoscopic technique and posterior component separation. So, we present a series of 22 patients with large ventral hernia repaired using various options of component separation technique in the last 3 years.
Keywords: Component separation technique, Ventral hernia, Large ventral hernia, Posterior component separation
Introduction
Ventral hernia occurs in approximately 0.5 to 1 % of population. It can be primary or secondary to previous abdominal surgeries (incisional hernia). Two to 11 % of laparotomy wounds develop into incisional hernia [1]. Ventral hernia is repaired by closure of the defect without tension, along with reinforcement with artificial prosthesis, which can be placed on the defect (onlay) or below the defect and above the peritoneum (sublay).
Wide defects in large ventral hernia cannot be closed. Traditionally, such defects are not closed but bridged with artificial prosthesis (onlay, sublay or intraperitoneal onlay). Non-closure of defects has significant physiological derangements. We have described a new way of the closure of midline defects with component separation technique in 22 cases of ventral hernia with large defects.
Material and Methods
From January 2011 to December 2014, we repaired 22 cases of large ventral hernia using various techniques of component separation. Four patients had primary hernia without any previous abdominal surgery, while the rest of 18 cases had abdominal surgery. Eleven cases had one previous surgery (two gynaecological and nine exploratory laparotomy), and seven cases had two previous surgeries (all gynaecological). In addition, there was an attempt to repair hernia in six cases which recurred (five cases had a single attempt, while one case was repaired twice).
Technique
All patients underwent surgery under general anaesthesia along with transverse abdominis block (TAB) or epidural catheterisation for post-op analgesia. The incision was midline, excising the previous scars in redo cases. Thorough adhesiolysis was done. All the contents were dropped back in the abdomen. The size of the defect was measured in its width. It varied from 6 to 15 cm (average 9.72 cm) (Table 1). For midline approximation and closure of the defect, one of the techniques of component separation was done.
Table 1.
Results of different techniques of CST
| Sr. no. | Size of defect (in cm) | Technique of CST | Complete wound healing (in days) | Complications | Recurrence (over 1–3 years) |
|---|---|---|---|---|---|
| 1 | 9 | Anterior with onlay mesh | 15 | Nil | Nil |
| 2 | 7 | Anterior with onlay mesh | 15 | Nil | Nil |
| 3 | 9 | Anterior with onlay mesh | 15 | Nil | Nil |
| 4 | 13 | Anterior with onlay mesh | 45 | SSI grade II+ large skin necrosis | 1 year |
| 5 | 11 | Anterior with onlay mesh | 20 | Minimal skin necrosis | Nil |
| 6 | 12 | Anterior with onlay mesh | 20 | Minimal skin necrosis | Nil |
| 7 | 10 | Endoscopic with sublay mesh | 15 | Nil | Nil |
| 8 | 8 | Anterior, preservation of perforators with sublay mesh | 15 | Nil | Nil |
| 9 | 9 | Endoscopic with sublay mesh | 15 | Nil | Nil |
| 10 | 15 | Anterior, preservation of perforators with sublay mesh | 30 | SSI grade I | Nil |
| 11 | 9 | Endoscopic with sublay mesh | 15 | Nil | Nil |
| 12 | 6 | Posterior with sublay mesh | 15 | Nil | Nil |
| 13 | 9 | Posterior with sublay mesh | 15 | Nil | Nil |
| 14 | 8 | Posterior with sublay mesh | 15 | Nil | Nil |
| 15 | 7 | Anterior with sublay mesh | 14 | Nil | |
| 16 | 12 | Anterior with Sublay mesh | 30 | Minimal skin necrosis | Nil |
| 17 | 9 | Anterior with sublay mesh | 16 | Nil | Nil |
| 18 | 8 | Anterior with sublay mesh | 15 | Nil | Nil |
| 19 | 10 | Anterior with sublay mesh | 14 | Nil | Nil |
| 20 | 14 | Anterior with sublay mesh | 45 | Minimal skin necrosis | Nil |
| 21 | 11 | Anterior with sublay mesh | 15 | Nil | Nil |
| 22 | 8 | Anterior with sublay mesh | 17 | Nil | Nil |
SSI surgical site infection
Anterior Component Separation Technique
We did classical Ramirez technique [2] in 16 cases. The skin flaps were raised by about 5 cm beyond the midline, the lateral-to-lateral border of the rectus muscle (linea semilunaris), which was preoperatively marked with USG (Fig. 1).
Fig. 1.

A case of large ventral hernia with preoperative marking of linea semilunaris
The external oblique was divided into 2 cm lateral to linea semilunaris, vertically and separated from the internal oblique. This allows medialization of the rectus. The extent of division of the external oblique depends on the size of the defect. The separation was done till midline could be closed with only normal physiological tension (Fig. 2).
Fig. 2.
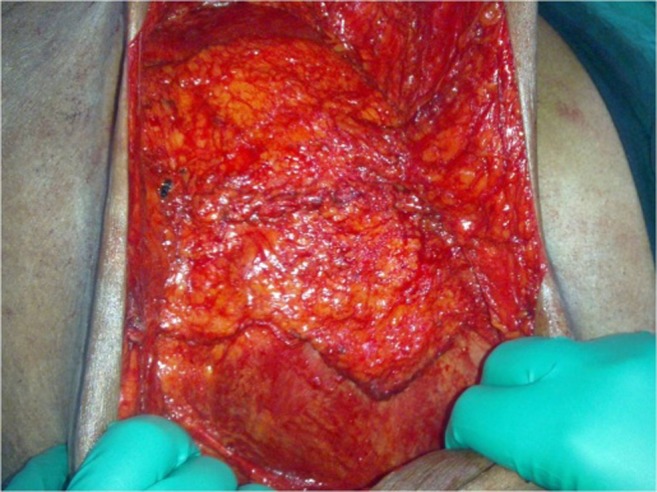
Closure of the midline after anterior CST
A light polypropylene mesh was put as an onlay in the first six cases and as a sublay in the subsequent ten cases. Sixteen-French suction drains were put in the subcutaneous plane, and the skin was closed. However, we encountered skin necrosis in some of these patients (Table 1). Skin necrosis is attributed to division of peri-umbilical perforators which get divided when skin flaps are raised.
Endoscopic Component Separation Technique
Endoscopic division of external oblique [3] was suggested to avoid raising the skin flaps which led to skin necrosis. We did an endoscopic component separation technique (CST) in the three cases. A 12-mm skin incision was made in lateral to costo-rectal angle. The wound was deepened up to the external oblique, which was split. A TDP balloon was inserted below the split external oblique and pushed towards the inguinal ligament, and the balloon was inflated with 20 to 25 puffs of air. This opens out the space showing external aponeurosis on the roof and internal oblique on the floor. The balloon was replaced with a 12-mm Hassan’s cannula, and the space was kept open with CO2 insufflation at 20 mmHg (Fig. 3).
Fig. 3.

Endoscopic component separation technique in ventral hernia repair
Another 5-mm trocar was put in the lumbar region in the space created, and the external oblique along with Scarpa’s fascia was divided with a hook cautery. The same procedure was carried out on the other side till the release allows midline closure without tension. A soft mesh was put in the retro rectal plane as a sublay. Though we could achieve midline closure without sacrificing perforators, the availability and cost of balloon were a constraint.
Perforator Preserving Anterior CST
We went back to open release, but preserving at least few peri-umbilical perforators. All these cases healed without skin necrosis.
Posterior CST
We have also done posterior component separation [4] in three cases. After initial adhesiolysis, a plane is opened between the rectus muscle and posterior rectus sheath. The posterior rectus sheath was divided 5 mm medial to linea semilunaris. A plane between the transverse abdominis and internal oblique was created along the length of incision on both sides which allows medialization of rectus. A soft mesh was then inserted as a sublay, and the midline was closed. We could manage to close the midline with 6-, 9- and 8-cm defects using this method (Table 1).
All the 22 cases had subcutaneous drains which were kept till drain dropped below 20 ml.
Results
All the 22 patients tolerated the procedure very well. Seventeen cases recovered without complications and discharged within 1 week of time. We encountered necrosis of the skin in five cases, all after anterior CST. Four cases had very minimal necrosis in the peri-umbilical area, which healed with dressings. One had a large area of necrosis which needed to be debrided, and the exposed onlay mesh was explanted. The same patient had a recurrence at 1 year (Table 1).
Discussion
Ventral hernia is a common problem. It can be primary or secondary to previous abdominal surgery. The attributing factors for ventral hernia are obesity, multiple pregnancies, smoking, chronic obstructive pulmonary disease, etc. Incisional hernia, in addition, can result from faulty surgical techniques and wound infection. About 10 % of ventral hernias undergo incarceration and need emergency surgery.
If untreated, the natural history of ventral hernias is gradual enlargement. The linea alba serves as the midline anchor for the aponeurotic insertions of the rectus sheath and oblique musculature. Disruption results in gradual enlargement of the hernia defect because of unopposed lateral contraction of the oblique musculature. This leads to widening of hernial defect and large ventral hernia.
Repair of large ventral hernia is a challenge for even experienced surgeons, as there are large defects which are difficult to close. In the earlier time, these large defects were closed using procedures like myofascial flaps or free flaps with high recurrences and complications [1]. Off late, these defects are bridged with artificial prosthesis (laparoscopic or open), but leaving the defects open.
However, non-closure of the midline had adverse effects on abdominal wall functions. Abdominal wall has many functions like protecting the abdominal viscera and supporting the spine. Besides, dynamic abdominal muscles take part in many physiological activities like coughing, micturition and defecation and are important during childbirth (parturition). The resistance of live, sensitive abdominal muscles to a distending stomach brings an end point of satiety and controls overeating.
Component separation technique (CST) is a novel answer to closure of midline with live, active tissues with or without the use of additional prosthesis. This technique was originally described in 1990 by Ramirez [2]. Lower hernia recurrence rates, restoration of dynamic abdominal wall function and improvement in back and postural abnormalities have been cited in the Western literature [5]. Major issue with this technique is wound-related complications owing to wide undermining of skin flaps. Modification by preserving peri-umbilical perforators can reduce wound-related morbidity as shown in our study and some of recent works [5]. However, there are no studies in the Indian literature on results of this technique so far.
Conclusion
Component separation technique is an effective technique for all large ventral hernias which have difficult midline closure.
Acknowledgments
Conflict of Interest
All the three authors declare that they have no conflict of interest.
References
- 1.Dan H, Shell IV, de la Torre J, Andrades P, Vasconez LO. Open repair of ventral incisional hernias. Surg Clin N Am. 2008;88:61–83. doi: 10.1016/j.suc.2007.10.008. [DOI] [PubMed] [Google Scholar]
- 2.Ramirez OM, Ruas E, Dellon AL. “Components separation” method for closure of abdominal-wall defects: an anatomic and clinical study. Plast Reconstr Surg. 1990;86:519. doi: 10.1097/00006534-199009000-00023. [DOI] [PubMed] [Google Scholar]
- 3.Maas SM, de Vries Reilingh TS, van Goor H, de Jong D, Bleichrodt RP. Endoscopically assisted “components separation technique” for the repair of complicated ventral hernias. J Am Coll Surg. 2002;194(3):388–390. doi: 10.1016/S1072-7515(01)01140-1. [DOI] [PubMed] [Google Scholar]
- 4.Novitsky YW, Elliott HL, Orenstein SB, Rosen M. Transversus abdominis muscle release: a novel approach to posterior component separation during complex abdominal wall reconstruction. JAM J Surg Nov. 2012;204(5):709–716. doi: 10.1016/j.amjsurg.2012.02.008. [DOI] [PubMed] [Google Scholar]
- 5.Nguyen V, Shestak KC. Separation of anatomic components method of abdominal wall reconstruction: clinical outcome analysis and an update of surgical modifications using the technique. Clin Plastic Surg. 2006;33:255. doi: 10.1016/j.cps.2005.12.010. [DOI] [PubMed] [Google Scholar]