

Abstract
Objectives:
Oestrogen deprivation has been shown to have a negative effect on connective tissue and its turnover. A link may exist between supplemental oestrogen, preservation of tendon collagen and less tendon abnormality. The aim was to determine the effects of female sex hormone supplementation (FSHS) on tendon.
Methods:
A systematic search of nine key health databases; Medline, CINAHL, EMBASE, SPORTDiscus, AUSPORT and AMI, Cochrane Library, SafetyLit and PEDro was completed (to Feb 24, 2016). The search yielded 6378 records using terms relating to hormone (oestrogen, estrogen, hormone replacement therapy, HRT, estrogen therapy, oestrogen therapy, oral contraceptive pill) and tendon. Quality assessment, data extraction and data synthesis of included papers was undertaken.
Results:
Low level of evidence for all outcomes; no positive or negative link between FSHS and molecular, mechanical and morphological tendon response outcomes, and the addition of exercise to FSHS, had minimal effects on tendon CSA.
Conclusions:
The effect of oestrogen supplementation on tendon is contradictory and inconsistent. This review suggests there is a need for further studies to understand the effects of FSHS on tendon tissue at a mechanical, morphological and molecular level.
Keywords: Hormone Replacement Therapy, Oestrogen, Oral Contraceptive Pill, Women, Tendon
Introduction
Tendinopathy is the clinical diagnosis given to a tendon causing pain and dysfunction. Tendinopathy affects active and inactive populations, from adolescents through to the elderly1, and can impact on quality of life2 and the ability to participate in pain-free activity. Rehabilitation is long, tedious and often expensive with many patients seeking multiple therapies, secondary to ineffective treatment regimens1.
Tendinopathy is usually associated with pathology within the tendon, although, pathology can be present for years3, without causing symptoms4,5. Tendon pathology is characterised by a change in cell function, increase in ground substance, disorganisation of collagen and neovascularisation6,7 evident on ultrasound or magnetic resonance imaging.
A number of risk factors for tendinopathy are associated with levels of circulating female sex hormones. Advancing age, female gender, body composition, and genetic make-up can all influence circulating sex hormone levels1,7-9 and may predispose to tendon pain. As oestrogen levels decline after menopause, collagen production can decline and tendons may become thinner10, rates of tendon pathology and the likelihood of tendon rupture increases11,12. Where oestrogen levels are higher in pre-menopausal females, the likelihood of developing lower limb tendinopathy is lower than that of age matched men4.
Body shape and fat distribution have also been associated with changes in oestrogen levels13 and tendon pathology14,15. Those with an android compared to a gynoid body shape are more likely to develop tendon pathology16. There is emerging evidence to suggest that supplemental oestrogen directly affects fibroblast proliferation17,18 and collagen synthesis19,20 and may change the susceptibility to tendinopathy. Thus, investigation of the impact of female sex hormones on tendon molecular, mechanical and morphological outcomes, and CSA area is therefore warranted.
Topical, subcutaneous and, more commonly, oral oestrogen is prescribed in both pre and post-menopausal populations, and the effect on connective tissue structures has been widely researched. It is known that supplemental oestrogen is beneficial for increasing skeletal muscle strength21, reducing fractures22, preserving bone mass23 and preventing a decline in the collagen content of skin24,25. The effect of oestrogen on collagen turnover in connective tissue varies, with studies finding an inhibiting effect17,26, no effect27 and a stimulating effect28. The reported higher rate of anterior cruciate ligament injury in women compared to men, has been attributed to the rhythmic variation of fluctuating oestrogen levels, but this remains both equivocal and controversial in the literature29,30.
Little is known about the effects of female sex hormones on tendon and it is hypothesised that the effects could be a direct and/or indirect. Tendon cells contain hormone-specific receptors and evidence suggests that tendon may be responsive to oestrogen31, directly effecting type 1 collagen upregulation and turnover19. Animal studies have also linked progesterone and high dose oestrogen with the upregulation of relaxin receptor isoforms (RXFPI and RXFP2) in tendon32. Relaxin has an effect on the extracellular matrix of tendon tissue. While animal and basic science studies have shown structural and molecular changes in response to sex hormones, it is unclear how they affect the mechanical properties of the tendon, or in turn the propensity to develop tendon pathology or pain.
Sex hormones have been reported to alter mechanical (tendon stress: failure point of the tendon measured in megapascals (MPa); strain: ∆length/length; stiffness: ∆force/length); Young’s Modulus: ∆stress/∆strain)33, molecular (tendon collagen synthesis)19,34 and morphological (tendon CSA)1 properties of human tendon. Despite the research to date, the direct and indirect effects of female sex hormone supplementation on human tendon tissue are not well understood, and it is unknown as to whether increasing or decreasing these factors are beneficial19. It is plausible that supplemental oestrogen (hormone replacement therapy: HRT) may be beneficial for preserving tendon collagen10 and reduced tendon abnormality1.
Objective
The primary aim of this review was to evaluate the effect of female sex hormone supplementation (FSHS) on tendon tissue in pre and post-menopausal women. The secondary objective was to assess, within the included studies, whether the addition of exercise to FSHS alters the mechanical, morphological and molecular response of tendon.
Data sources
Search methods and study selection
Database searches were conducted by one reviewer (CG) accessing Medline (1946 to Feb 24, 2016), CINAHL (1984 to Feb 24, 2016), EMBASE (1988 to Feb 24, 2016), all Cochrane Library databases (to Feb 24, 2016), PEDro (to Feb 24, 2016), SPORTDiscus (1937 to Feb 24, 2016), AUSPORT (1970 to Feb 24, 2016), SafetyLit (to Feb 24, 2016) and AMI (1970 to Feb 24, 2016). A subject heading and key word search was performed using two main concepts: hormone (oestrogen, estrogen, hormone replacement therapy, HRT, estrogen therapy, oestrogen therapy, oral contraceptive pill) and tendon. All references were imported into Endnote version X6 (Thomson Reuters, New York, NY, USA) and duplicate articles were deleted by one reviewer (CG). Three reviewers (CG - all, TP - L-Z and AS - A-K) independently applied the selection criteria to the titles and abstracts of the remaining studies and excluded studies that did not clearly meet the criteria. There were no disagreements between independent reviewers during this process. Full texts were obtained where the title and abstract appeared to meet the criteria or did not provide sufficient information to determine eligibility. The criteria were reapplied to all retrieved full text articles by two reviewers in consultation (CG, TP).
Citation tracking of included studies was performed using Google Scholar. A manual check of references in key articles was also performed to ensure that no relevant articles had been missed in the initial search.
Study selection
Eligibility criteria
Participants: Studies assessing pre and/or post-menopausal women were included. Studies were required to document hormonal status.
Types of Intervention: A comparison of FSHS versus no hormone supplementation (control group) was required for studies to be included in this review. Female sex hormone supplementation interventions of any frequency and duration were included in the study. Acceptable FSHS interventions included the oral contraceptive pill, transdermal oestrogen and HRT/oestradiol therapy.
Types of outcome measures
Studies must have assessed one or more of: the molecular response, morphological response or mechanical response of tendon to FSHS. Outcomes must have been evaluated in both the intervention (FSHS) group and control group. Additionally, all outcomes must have been measured at a resting state but could additionally be measured during or post-exercise. Any non-tendon outcomes, such as those relating muscle and bone, were excluded from the review. Where the same outcome was reported twice on the same cohort20,35, only the study with the most complete dataset was included20.
Study characteristics
Only full text articles published in peer-reviewed journals were included and no restrictions on language were applied to the search. Studies on the prevalence of tendon abnormality associated with FSHS were included. Case studies, case series and opinion articles were excluded due to the greater potential for bias in these types of studies36.
Data extraction
Appraisal of included studies
Due to the varying susceptibility to bias in non-randomised studies, all included papers were assessed for methodological quality by one reviewer (CG) using an observational study assessment form. This form was adapted from a quality tool employed by Siegfried et al37. The Non-Randomised Studies Methods Group of The Cochrane Collaboration has commended this quality assessment tool38. This tool was chosen as it evaluates external and internal validity (performance bias, detection bias and selection bias). Furthermore, it itemises and displays each aspect of quality assessment in its raw form for readers. Specific criteria were created to evaluate bias and confounding factors in study design – level of hormone administered, duration of HRT or oral contraceptive pill (OCP) usage prior to the study, testing procedure, baseline participant fitness/activity levels, present co-morbidities, participant weight/body mass index, the use of separate exercise and non-exercise groups to assess the impact of exercise with FSHS, and randomisation of intervention. Unlike many quality assessment tools, a summary score is not used; rather, the reader is able to evaluate the studies by each category and hence study quality validity is not compromised37.
Quality of evidence
The level of evidence for each review outcome was evaluated based on methods first described by vanTulder39 and modifed by Yusuf et al.40 due to heterogeneity of the included studies. There were five levels of evidence, with strong evidence indicating consistent findings among high quality studies, moderate evidence indicating generally consistent findings from at least one high quality study and multiple low quality studies, limited evidence indicating generally consistent results from two or more low quality studies, very limited evidence indicating results from one low quality study and conflicting evidence indicating inconsistent findings among multiple low or high quality statistically heterogeneous studies. This synthesis places weight on the quality of studies and consistency of results for each outcome.
This review defined a ‘high quality’ study was as one that randomised participants to the intervention, and fulfilled nine of the eleven other categories on the quality tool employed (Table II). A ‘low quality’ study was defined as one that did not randomise participants to the intervention and fulfilled less than nine of the eleven other categories.
Table 1.
Characteristics of included studies.
| Author | Study Type | Tendon investigated | Groups /Intervention | Population(s) | Mean (SD) Age in years | Outcomes Analysed in Review |
|---|---|---|---|---|---|---|
| Bryant et al. (47) | Cross-sectional | Achilles | 20 Users of monophasic oral contraceptive pill (MOCP) 20 No contraception (non-MOCP) |
Pre-menopausal athletic women (runners) | 28.0(4.2) 31.9(7.3) |
Achilles tendon strain Plasma oestrogen levels (pg/ml) |
| Cook et al. (1) | Cross-sectional | Achilles | 16 Users of HRT 37 Non-HRT 8 Users of HRT 24 Non-HRT |
Post-menopausal asymptomatic active women (golfers) Post-menopausal asymptomatic inactive women (golfers) |
S8.0(8.27) 61.8(6.36) 58.8(7.72) 58.9(6.87) |
Achilles tendon diameter (mm) Achilles tendon status: normal/abnormal (% abnormal) |
| Finni et al. (48) | Cross-sectional | Achilles | 14 Users of HRT 14 Non-HRT |
Post-menopausal monozygotic female twin pairs (14 pairs) | 57.2(1.8) | Achilles tendon thickness Achilles tendon CSA (cm2) Serum estradiol (pmol/L) Free estradiol (pmol/L) Estrone (pM) |
| Hansen et al. (19) | Cross-sectional | Patellar | 10 Users of ERT post hysterectomy 10 Non-users of ERT |
Post menopausal women | 61 (4) 60(4) |
Patellar tendon force maximum Serum estradiol (nmol/L) Tendon fibril size, density, tendon CSA, tendon stress, tendon strain, tendon stiffness Young’s Modulus, Tendon collagen synthesis (FSR, PINP) |
| Hansen et al. (33) | Cross-sectional | Patellar | 15 Users of oral contraceptive pill 15 Non-users of the oral contraceptive pill |
Pre menopausal athletic women (handball players) | 23.0(1.0) 22.0(1.0) |
Patellar tendon CSA (mm2), tendon fibril diameter (nm), tendon stress, strain, stiffness. Young’s Modulus Plasma oestrogen (nmol/L), LH, FSH |
| Holmes & Un. (49) | Cross-sectional | Achilles | 44 Women with Achilles tendinopathy 38 Men with Achilles tendinopathy |
Women and Men diagnosed with symptomatic Achilles Tendinopathy | Women = 51.3 Men = 49.5 |
Prevalence (%) of HRT or oral contraceptive use in people with Achilles tendinopathy |
| Hansen et al. (35) | Cross-sectional | Patellar | 11 Users of oral contraceptive pill 12 Non-users of the oral contraceptive pill |
Pre menopausal young healthy women | 24(2) 24 (4) |
Patellar tendon CSA Serum estradiol levels (nmol/L) Tendon collagen synthesis (PINP) |
| Hansen et al. (20) | Cross-sectional | Patellar | 11 Users of oral contraceptive pill 12 Non-users of the oral contraceptive pill |
Pre-menopausal young healthy women | 24(2) 24 (4) |
Patellar tendon CSA Serum estradiol levels (nmol/L) Tendon collagen synthesis (FSR) |
| Pingel et al. (34) | Randomised controlled cross over study | Patellar | Oestrogen patch applied to the patellar tendon No oestrogen patch (total of 11 participants in crossover) | Post-menopausal women | 65.0(2.0) | Serum estradiol and (nmol/L) Serum PINP(mgL-1) Whole body tendon collagen synthesis (PINP) |
N/A = not applicable, CSA = cross-sectional area, PINP = a measure for amino-terminal propeptide of type I collagen, FSR = Functional synthesis rate, HRT = Hormone Replacement Therapy, ERT = Estrogen Replacement Therapy.
Table 2.
Quality assessment and risk of bias for included studies.
| Study | External Validity | Internal Validity | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Performance | Detection | Selection bias/Control of Confounding factors | ||||||||||
| Representative | Participation rate | Direct Observation | Blinded Assessors | Method and dosage of FSHS | Duration of HRT or OC usage prior to the study indicated | non-OC users testing procedure timing described | Baseline activity or fitness levels of participants described | Participant comorbidities, or lack thereof, indicated | Partici pant weight/BMI | Randomisation of FSHS | Impact of exercise assessed with separate exercise and non-exercise groups | |
| Bryant et al. (47) | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✗ | ✓ | ✗ | ✓ |
| Cook et al. (1) | ✓ | ✗ | ✓ | ✓ | ✗ | ✓ | N/A | ✓ | ✗ | ✓ | ✗ | ✓ |
| Finni et al. (48) | ✓ | ✗ | ✓ | ✗ | ✗ | ✓ | N/A | ✓ | ✗ | ✓ | ✗ | ✓ |
| Hansen et al. (19) | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | N/A | ✓ | ✓ | ✓ | ✗ | ✗ |
| Hansen et al. (33) | ✓ | ✗ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✗ | ✗ |
| Holmes and Lin (49) | ✓ | ✓ | ✗ | ✗ | ✗ | ✗ | N/A | ✗ | ✓ | ✓ | ✗ | ✓ |
| Hansen et al. (35) | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✗ | ✗ |
| Hansen et al.(20) | ✓ | ✓ | ✓ | ✗ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✗ | ✗ |
| Pingel et al. (34) | ✓ | ✓ | ✓ | ✗ | ✓ | ✓ | N/A | ✗ | ✓ | ✓ | ✓ | ✗ |
Note: ✓ indicates the measure was adequately addressed in the study. ✗ indicates the measure was not adequately addressed in the study.
Representative: ✓ if study had pre and/or postmenopausal participants but no menopausal participants.
Participation rate: ✓ if 100% of those who were eligible to participate in the study were included in the study.
Direct Observation: ✓ if either be stated or implied.
N/A not applicable to the study.
Data extraction methods
A customised data extraction form based on the recommendations of the National Randomised Studies and Methods Group (NRSMG)41 and the Transparent Reporting of Evaluations with Non-randomised Designs (TREND) statement42, was used to guide data extraction for non-randomised studies. Information obtained included (but was not limited to) study inclusion and exclusion criteria, details of methodology, outcome measures, confounding variables and any statistical analyses. Where studies incorporated a non-exercise and active/exercise or post-exercise condition, both sets of data were included in the review.
Data synthesis
Review Manager (RevMan Version 5.2. Copenhagen: The Nordic Cochrane Centre, The Cochrane Collaboration, 2012) was used to create forest plots and calculate effect sizes via standardised mean differences and 95% confidence intervals (CI) for study outcomes. A small number of studies investigating each outcome meant that it was inappropriate to combine most of the data into a meta-analysis41,43. A meta-analysis was performed on outcomes where studies were clinically and statistically homogenous. Statistical homogeneity was determined by the I2 value44, where a value of 0% indicates no observed heterogeneity, less than 25% is considered to have low levels and a value of 100% indicates a completely heterogenous sample. For ease of analysis, ‘non-exercise leg’ data were grouped with ‘inactive’ and ‘contralateral leg’ participant data, and ‘exercise leg’ data were grouped with ‘active’ and ‘jumping leg’ participant data. Odds ratios (OR) were also calculated to determine the likelihood of tendon abnormality, where ultrasonographic abnormality was defined as “a variation in the fiber structure of the tendon evident in both the longitudinal and the transverse scans”, commonly seen “as a hypoechoic region or fusiform swelling”1. In studies where mean and confidences intervals or standard errors were published, the variance measure was converted to standard deviations to enable comparison of results across the studies1. Where studies presented results graphically, data were estimated from the graph45 and confirmed using GraphClick computer software (Arizona-Software, Version 3.0, 2008), which has been shown to be a valid and reliable tool46.
Results
Study selection
The number of references considered at each stage of the review and the reason for exclusions are shown in Figure 1. In total, 9 studies were included in the review.
Figure 1.

Flowchart of the studies included in the review.
Study characteristics
Participants across the studies ranged in number from 11 to 85 and had a mean age (SD) between 22.0 (1.0) and 65.0 (2.0) years (Table 1). All studies included in the review compared FSHS (intervention group) with no FSHS (control group). Eight of the nine cross-sectional studies were observational and participants in the intervention groups were taking FSHS prior to undertaking the study. Of these eight, four studies examined the effects of the oral contraceptive pill on tendon in pre-menopausal women20,33,35,47 and three examined the effects of oral hormone replacement therapy on tendon in post-menopausal women compared to a control group1,19,48. The remaining retrospective study investigated the prevalence of oral contraceptive and hormone replacement therapy use in a group of people with Achilles tendinopathy49. There was only one study that randomised FSHS and placebo (5 day transdermal oestrogen patch) in a post-menopausal population34.
In addition to investigating FSHS, four out of nine studies included results for non-exercise and exercise legs19,20,34,35, two reported on active and inactive groups1,48 and one on the participants’ normal jumping leg and contra-lateral leg33. Outcomes assessed varied considerably between the studies. The most commonly evaluated outcome was tendon CSA19,20,34,35,48.
Risk of bias assessment
All included studies displayed strong external validity, being representative of pre and post-menopausal populations1,19,20,33-35,47-49. Performance bias was low, with 8 out of 9 studies having stated or implied observation of the interventions. A moderate level of detection bias was present among the studies, with only five studies utilsing blinded assessors1,19,33,35,47. Selection bias varied considerably across the confounding factors incorporated into the analysis. Six out of nine studies indicated the method and dosage of hormone administration19,20,33-35,47. Three papers reported the type of hormone therapy but not the dosage level1,48,49. Seven studies recorded the duration of hormone therapy usage prior to participating in the study1,19,20,33-35,47,48. All of the studies investigating the oral contraceptive pill, identified the method of data collection and the timing of the menstrual cycle and/or pill cycle19,20,35,47. Seven out of nine studies reported baseline activity levels of included participants, which is important for determining the effects that exercise/activity levels have on tendon when combined with a hormone therapy supplement. All studies recorded the weight of included participants but only four studies identified the presence or absence of co-morbidities20,33,34,49. Four other studies provided an overarching statement of ‘healthy’ or ‘athletic’ women, assumed to indicate a lack of co-morbidites1,19,35,47. Finni et al.48 reported that their participants had no contradindications to participate in their study. In only one study, were participants randomised to receive the intervention34. Five of the eight studies19,20,33-35 used both legs of the same participant to examine the impact of resistance exercise – having an ‘exercise’ and a ‘non-exercise’ leg, rather than an ‘exercise group’ and a ‘non-exercise’ group (Table 2).
Tendon outcome analysis
Molecular/Histopathological response
Very limited evidence (one low quality study19) exists for tendon collagen fractional synthesis rate (FSR), and limited evidence (two low quality studies unable to be combined with meta-analysis19,34) for tendon PINP (a measure for amino-terminal propeptide of type I collagen synthesis50) in the post-menopausal population. Tendon collagen FSR for the non-exercise and exercise legs was greater in post-menopausal women on FSHS19. In pre-menopausal women, tendon FSR was significantly lower for the non-exercise leg for participants not taking the OCP, however no differences were found in the exercise leg. In post-menopausal women, PINP was higher and lower with hormone supplementation19,34. Very limited evidence exists for serum PINP in post-menopausal women and tendon fibril density in pre and post-menopausal women, with only one low quality study reporting on each outcome. No differences were found for serum PINP at day 2, 3 or 5 of the transdermal oestrogen patch application (Figure 2)34. Although higher in post-menopausal women, no significant differences for tendon fibril density were found in either population group19.
Figure 2.
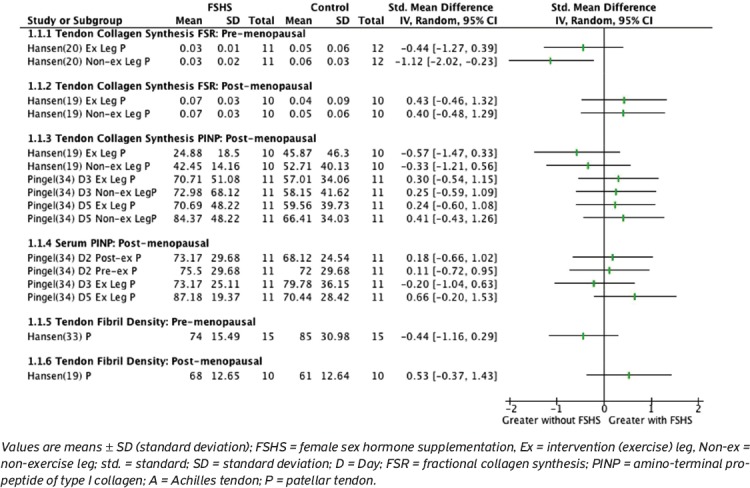
Molecular Response of tendon in pre and post-menopausal women.
Mechanical response
Very limited evidence existed for all mechanical response measures (one low quality study per outcome), except tendon strain that had conflicting evidence (two low quality studies, unable to be combined with meta-analysis). Tendon stress was lower and maximum tendon force and Young’s modulus significantly lower with FSHS in post-menopausal women19. Contrary to this, Hansen et al.33 found that with FSHS supplementation, tendon stress and Young’s Modulus was higher in the contralateral leg but lower in the jumping leg in pre-menopausal women, however none of these differences were significant. Differences in pre-menopausal tendon strain was evident with Bryant et al.47 finding lower strain with FSHS, and Hansen et al. (2013)33, found no significant difference. Bryant et al.47 reported results during two sections of the female hormone cycle – ovulation (where serum oestrogen levels are at their lowest) and menstruation (where serum oestrogen levels are at their highest). No significant differences were identified in tendon strain in post-menopausal women and tendon stiffness in pre and post-menopausal women (Figure 3).
Figure 3.
Mechanical Response of tendon in pre and post-menopausal women.
Morphological response
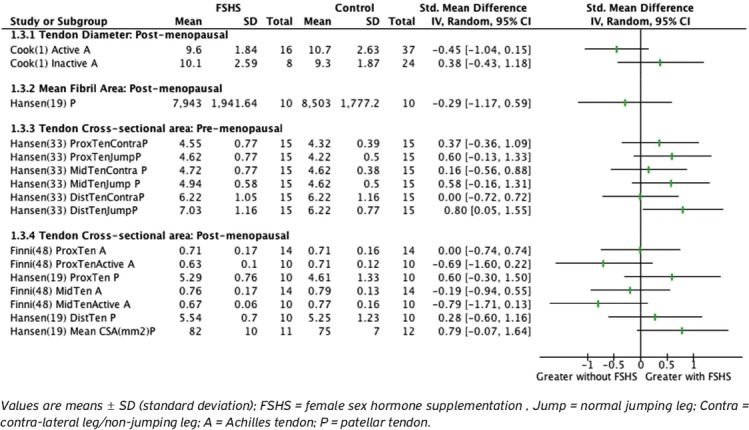
Very limited evidence existed for post-menopausal cross sectional area (middle and distal tendon), tendon diameter and mean fibril size, and pre-menopausal tendon cross sectional area (proximal, middle and distal), with only one low quality study reporting on each of these outcomes. Cook et al.1 reported that active women on HRT had less tendon abnormality than inactive women on HRT (p=0.056)1. However the odds ratio suggests no significant difference in risk of tendon abnormality (OR=0.31, 95%CI=0.08, 1.08). Inactive participants on hormone replacement therapy were more likely to have tendon abnormality (OR=5.0, 95%CI=0.91, 27.47) compared to those not on hormone replacement therapy. No significant differences were found in tendon diameter1 or mean fibril size19 across both pre and post-menopausal populations.
No significant differences were found for cross-sectional area (CSA) for the non-exercise leg at the proximal, mid and distal parts of the tendon in participants taking FSHS. Cross-sectional area of the proximal tendon of the non-exercise leg in post-menopausal women was the only outcome appropriate for meta-analysis, using a random effects model to account for the heterogeneity between studies51. With a sample size of 2419,48, there were no significant findings (degrees of freedom: df= 1.0, 95%CI -0.34 to 0.83, p=0.41). Conflicting evidence exists for post-menopausal FSHS for the proximal tendon, as indicated by a low level of statistical heterogeneity between the studies, I2=3%19,48.
For the exercise leg, pre-menopausal populations taking FSHS (OCP) had significantly higher distal CSA33. There was also higher CSA at proximal and mid parts of tendon33 however differences were not significant. In contrast, CSA was greater, but not significantly so, in a post-menopausal population48 not taking FSHS (Figure 4).
Figure 4.

Morphological response of tendon in pre and post-menopausal women.
Holmes and Lin49 reported that within their cohort of participants with Achilles tendinopathy, hormone replacement therapy was statistically associated with Achilles tendinopathy in the 60-64 year age group and for the group as a whole (50-74 years).
Discussion
This review provides a synthesis of the current literature on the effects of FSHS on tendon. Caution should be taken extrapolating these findings, as included studies were mostly observational, underpowered, and had outcomes that were difficult to interpret within the small body of literature available. Similarly, the presence of large confidence intervals in the results, decrease the likelihood of ruling in or out, any physiologically important effects. Using the vanTulder approach to assess level of evidence39, this review shows either limited, very limited or conflicting evidence for all outcomes assessed.
Although, the intention was to provide a series of meta-analyses, the range of outcomes, ages and activities across studies, made it difficult to combine data to determine the true effect of FSHS on tendon. Due to this clinical heterogeneity, only one outcome could be evaluated via meta-analysis - CSA of the proximal tendon19,48. The results suggest that FSHS has a varied effect on tendon outcomes when compared to no FSHS. Young’s modulus and maximum tendon force were lower, and tendon FSR was higher, in post-menopausal women taking FSHS19. There was a trend towards tendon PINP being higher with FSHS supplementation34, and tendon CSA being higher without FSHS under an exercise condition48, in post-menopausal women. Significantly lower FSR for the non-exercise leg was seen in pre-menopausal women20 and although not significant, there was also a trend for higher tendon CSA with FSHS in this population33. Tendon strain results varied between two studies, showing both higher and lower strain in response to FSHS in pre-menopausal women33,47. All other findings were not significant.
Effects of supplemental oestrogen
Molecular/Histopathological response
Profoundly different FSR of collagen were reported in two studies19,20, likely due to differences in sample population: pre-menopausal20 versus post-menopausal women19 and type of intervention – OCP (2 mg of oral serum oestradiol) versus ERT (30 µg ethinyl oestradiol or 35 µg ethinyl oestradiol and 0.25 mg norgestimate per day). The risk of bias was moderate in both studies. Neither study randomised the intervention20,35, and the use of blinded assessors in Hansen et al.20 was not explicit.
The outcome measures of tendon collagen synthesis (FSR and PINP) are pragmatic and clinically relevant however, whether they are an accurate measure of what occurs at the tendon tissue level is questionable. Unlike muscle, core tendon is not continuously renewed52. It has been reported that intracellular degradation of collagen accounts for up to 10-40% of newly synthesised tendon collagen53-55. Therefore measures of protein synthesis rates using stable isotopes, as reported in two of the included papers19,20, may overestimate collagen synthesis as proteins may be degraded prior to being incorporated into the extracellular matrix52. Additionally, serum measures (s-PINP) may provide a more systemic reflection of collagen synthesis that occurs in many tissues. Similarly, in a study on bone turnover, Bennell et al.56 found no association between measures of serum collagen cross-links (pyridinoline: Pyr and deoxypyridinoline: D-Pyr) in urine samples and the development of stress fractures. However, as these are measures of bone remodelling throughout the skeleton, local changes at the site of the stress fracture are possible, similar to what may occur in tendon. As a consequence, results from included studies should be reviewed with caution as these outcome measures (tendon collagen FSR and PINP, and serum PINP), may not be a true reflection of collagen synthesis in the tendon tissue.
Mechanical response
Biomechanical properties of tendon were investigated in three out of eight included studies19,33,47. Although widely researched in the literature, there is no consensus on the optimal level of tendon stiffness, stress and strain, or a method to accurately measure such properties. However, these properties are highly participant specific; may be responsive to participant age, injury history, training loads, and immobilisation57. This review found that the biomechanical properties of Young’s modulus and maximum tendon force were significantly reduced in the presence of oestrogen in post-menopausal women19. For pre-menopausal women, results for tendon stress, stiffness and Young’s modulus were inconclusive33. Bryant et al.47 reported significantly higher Achilles tendon strain in the control group compared to the OCP user group (p=0.035), however in our analysis, findings were only significant during menstruation. Articles investigating the mechanical properties of Achilles tendon highlight the large variation in methods used to quantify tendon strain and stress58-61. Thus, it is difficult to evaluate whether changes in these properties are a barrier or facilitator to tendon health.
Morphological response
Tendon diameter, mean fibril size, tendon abnormality and CSA were evaluated in this review. Neither tendon diameter nor mean fibril size was affected by FSHS. Tendon CSA was the most evaluated outcome in this review. There is debate as to whether higher or lower tendon CSA is a helpful morphological adaptation or a marker of pathology. Previous studies have shown larger tendon CSA with heavy resistance training compared to light resistance training62 and remain unchanged with prolonged endurance training63. Challenging this interpretation, is the study by Heinemeyer et al.52 that reported adult core tendon collagen renewal is extremely limited and the formation of tendon collagen occurs within the first 17 years of life52.
Prevalence of tendinopathy
Holmes and Lin49 found most of the participants in their study diagnosed with Achilles tendinopathy used FSHS. As this was a retrospective study it is unknown if those taking FSHS had other comorbidities that may have an additional impact on their Achilles tendon health. The risk of bias analysis revealed a presence of selection bias, as the baseline activity/fitness level of the included participants and the method, dosage and the duration hormone supplementation use, was unknown.
Effects of rest and exercise conditions on tendon
Several studies reported on the additional impacts of no-exercise and exercise on tendon (secondary aim) in those people taking FSHS. Different methods were used to investigate this: five studies presented results for each leg of a participant (a non-exercise/rest leg and an exercise leg)19,20,33-35; two studies divided the participants into a control (inactive) group and active group or sub-group of people1,48 and one study described their participants as active, however only reported on the primary outcome of this review. Only one significant result was found with the addition of exercise - pre-menopausal populations taking the OCP had significantly higher CSA. Thus, evidence to suggest that exercise impacted considerably on tendon morphology was not heavily substantiated.
Issues can arise when reporting on both legs of a participant, particularly if the exercise applied to one leg has systemic and/or cortical effects, resulting in changes to the contralateral leg64,65. This has been evident in animal studies where tenocyte hypercellularity and vascular proliferation have been measured in response to exercise in one limb in rabbits66. Significantly larger tenocyte numbers were reported after three and six weeks of training in both the exercised and unexercised limb. Also, an increase in vascularity and VEGF-mRNA of the tendon tissue was found. These findings were indicative of bilateral tendinosis like changes in both the exercised and non-exercised leg, suggesting it would be inappropriate to use the non-exercised limb as a control. In addition, it is believed that unilateral exercise may activate neural circuits causing plastic changes in the primary motor cortex64,65 and altering the excitability of cortical67-72 and spinal67,73-75 motor pathways to the contralateral limb. Thus, in this review, where studies have implemented unilateral strength training in combination with supplemental oestrogen19,20,34,35, the effects on the non-exercised limb may be exaggerated, and accurate interpretation of the effect of exercise with supplemental oestrogen on tendon, more difficult.
Limitations
Of the outcomes assessed in this review, many were only evaluated by 1-2 studies, meaning that a definitive effect of FSHS on each outcome could not be determined. In addition, there is a possibility of publication bias (i.e. unpublished studies with insignificant findings or small effect sizes).
It is difficult to interpret whether changes in the outcome measures described in this review represent a positive or negative change. For exercise in isolation, contradictory findings have been observed for mechanical properties such as stiffness and Young’s Modulus76. These contradictory findings highlight the difficulty of dichotomising response to FSHS as positive and negative.
Summary
This review provides no strong evidence to suggest a positive or negative link between FSHS and tendon outcomes. The overall findings of this review must be interpreted in light of methodological limitations of included studies, study heterogeneity, and the moderate risk of bias. Studies reported on tendon response outcomes relating to oral contraceptive pill supplementation20,33,35,47, oral hormone replacement therapy1,35,48 and a transdermal oestrogen patch34. Although dosage and type of hormone administered may have been defined, no attempt to standardise the dosage of oral contraceptive across study participants was made. In the randomised controlled crossover study, it was reported that a recommended dose of oestrogen replacement therapy of 50 µg/24hour patch was administered to all participants34. However, the source of such recommendation and the optimal dosage and duration of FSHS administration to affect molecular, mechanical and morphological tendon outcomes, positively or negatively are unknown. Therefore it is difficult to determine the true effect of FSHS on tendon. Only one of the nine studies randomised the hormone therapy intervention34. Risk of bias was higher in the remaining eight studies as they recruited participants who were already taking FSHS prior to the commencement of the study. As a consequence, the intervention and control groups are likely to vary on known and unknown confounding factors at baseline. The decision to take, or reasons for taking, FSHS (medical, contraceptive and life-style) potentially divides participants prior to inclusion in the studies.
Conclusions
The effect of oestrogen supplementation on tendon is contradictory and inconsistent. Few studies reported the effects of oestrogen on the molecular, mechanical and morphological responses of tendon. Most mechanical and molecular tendon response outcomes were not significantly different between FSHS and no supplementation. Although, results suggest some benefit of FSHS for higher tendon CSA in pre-menopausal women and reducing tendon abnormality in post-menopausal women, results must be viewed with caution. Included studies were mostly observational, underpowered and had outcomes that were difficult to interpret within the small body of literature available. This review suggests there is a need for further studies to understand the effects of FSHS on tendon tissue at a mechanical, morphological and molecular level.
Footnotes
The authors have no conflict of interest. Professor Cook was supported by the Australian centre for research into sports injury and its prevention, which is one of the International Research Centres for Prevention of Injury and Protection of Athlete Health supported by the International Olympic Committee (IOC). Professor Cook is a NHMRC practitioner fellow (ID 1058493).
Edited by: S. Warden
References
- 1.Cook JL, Bass SL, Black JE. Hormone therapy is associated with smaller Achilles tendon diameter in active post-menopausal women. Scandinavian Journal of Medicine and Science in Sports. 2007;17:128–32. doi: 10.1111/j.1600-0838.2006.00543.x. [DOI] [PubMed] [Google Scholar]
- 2.Rio E, Moseley L, Purdam C, et al. The pain of tendinopathy:physiological or pathophysiological? Sports Medicine. 2013 doi: 10.1007/s40279-013-0096-z. [DOI] [PubMed] [Google Scholar]
- 3.Malliaras P, Cook J. Patellar tendons with normal imaging and pain:change in imaging and pain status over a volleyball season. Clinical Journal of Sport Medicine. 2006;16:388–91. doi: 10.1097/01.jsm.0000244603.75869.af. [DOI] [PubMed] [Google Scholar]
- 4.Cook JL, Khan KM, Harcourt PR, et al. Patellar tendon ultrasonography in asymptomatic active athletes reveals hypoechoic regions:A study of 320 tendons. Clinical Journal of Sport Medicine. 1998;8:73–7. doi: 10.1097/00042752-199804000-00001. [DOI] [PubMed] [Google Scholar]
- 5.Shalaby M, Almekinders L. Patellar Tendinitis:The significance of magnetic resonance imaging findings. The American Journal of Sports Medicine. 1999;27:345–9. doi: 10.1177/03635465990270031301. [DOI] [PubMed] [Google Scholar]
- 6.Cook JL, Malliaras P, De Luca J, Ptasznik R, Morris ME, Goldie P. Neovascularization and pain in abnormal patellar tendons of active jumping athletes. Clinical Journal of Sport Medicine. 2004;14:296–9. doi: 10.1097/00042752-200409000-00008. [DOI] [PubMed] [Google Scholar]
- 7.Kountouris A, Cook J. Rehabilitation of Achilles and patellar tendinopathies. Best Practice and Research Clinical Rheumatology. 2007;21:295–316. doi: 10.1016/j.berh.2006.12.003. [DOI] [PubMed] [Google Scholar]
- 8.Knobloch K, Schreibmueller L, Kraemer R, Jagodzinski M, Vogt PM, Redeker J. Gender and eccentric training in Achilles mid-portion tendinopathy. Knee Surgery, Sports Traumatology, Arthroscopy. 2010;18:648–55. doi: 10.1007/s00167-009-1006-7. [DOI] [PubMed] [Google Scholar]
- 9.Miller BF, Hansen M, Olesen JL, et al. Tendon collagen synthesis at rest and after exercise in women. Journal of Applied Physiology. 2007;102:541–6. doi: 10.1152/japplphysiol.00797.2006. [DOI] [PubMed] [Google Scholar]
- 10.Moalli PA, Talarico LC, Sung VW, et al. Impact of menopause on collagen subtypes in the arcus tendineous fasciae pelvis. American Journal of Obstetrics and Gynecology. 2004;190:620–7. doi: 10.1016/j.ajog.2003.08.040. [DOI] [PubMed] [Google Scholar]
- 11.Kannus P, Jozsa L. Histopathological changes preceding spontaneous rupture of a tendon. Journal of Bone and Joint Surgery. 1991;17A:1507–25. [PubMed] [Google Scholar]
- 12.Maffulli N, Waterston SW, Squair J, Reaper J, Douglas S. Changing Incidence of Achilles Tendon Rupture in Scotland:A 15-Year Study. Clinical Journal of Sport Medicine. 1999;9:157–60. doi: 10.1097/00042752-199907000-00007. [DOI] [PubMed] [Google Scholar]
- 13.Bjorntorp P. The regulation of adipose tissue distribution in humans. International Journal of Obesity and Related Metabolic Disorders. 1996;20:291–302. [PubMed] [Google Scholar]
- 14.Wendelboe AM, Hegmann KT, Gren LH, Alder SC, White GL, Jr, Lyon JL. Associations between body-mass index and surgery for rotator cuff tendinitis. The Journal of Bone and Joint Surgery American Volume. 2004;86-A:743–7. doi: 10.2106/00004623-200404000-00011. [DOI] [PubMed] [Google Scholar]
- 15.Werner RA, Franzblau A, Gell N, Ulin SS, Armstrong TJ. A longitudinal study of industrial and clerical workers:predictors of upper extremity tendonitis. Journal of Occupational Rehabilitation. 2005;15:37–46. doi: 10.1007/s10926-005-0872-1. [DOI] [PubMed] [Google Scholar]
- 16.Gaida JE, Cook JL, Bass SL, Austen S, Kiss ZS. Are unilateral and bilateral patellar tendinopathy distinguished by differences in anthropometry, body composition, or muscle strength in elite female basketball players? British Journal of Sports Medicine. 2004;38:581–5. doi: 10.1136/bjsm.2003.006015. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Liu SH, Al-Shaikh RA, Panossian V, Finerman GA, Lane JM. Estrogen affects the cellular metabolism of the anterior cruciate ligament. A potential explanation for female athletic injury. The American Journal of Sports Medicine. 1997;25:704–9. doi: 10.1177/036354659702500521. [DOI] [PubMed] [Google Scholar]
- 18.Yu WD, Liu SH, Hatch JD, Panossian V, Finerman GA. Effect of estrogen on cellular metabolism of the human anterior cruciate ligament. Clinical Orthopaedics and Related Research. 1999;366:229–38. doi: 10.1097/00003086-199909000-00030. [DOI] [PubMed] [Google Scholar]
- 19.Hansen M, Kongsgaard M, Holm L, et al. Effect of estrogen on tendon collagen synthesis, tendon structural characteristics, and biomechanical properties in postmenopausal women. Journal of Applied Physiology. 2009;106:1385–93. doi: 10.1152/japplphysiol.90935.2008. [DOI] [PubMed] [Google Scholar]
- 20.Hansen M, Miller BF, Holm L, et al. Effect of administration of oral contraceptives in vivo on collagen synthesis in tendon and muscle connective tissue in young women. Journal of Applied Physiology. 2009;106:1435–43. doi: 10.1152/japplphysiol.90933.2008. [DOI] [PubMed] [Google Scholar]
- 21.Greising SM, Baltgalvis KA, Lowe DA, Warren GL. Hormone therapy and skeletal muscle strength:a meta-analysis. The journals of gerontology Series A, Biological sciences and medical sciences. 2009;64:1071–81. doi: 10.1093/gerona/glp082. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Calleja-Agius J, Brincat MP. Hormone replacement therapy post Women's Health Initiative study:where do we stand? Current Opinion in Obstetrics and Gynecology. 2008;20:513–8. doi: 10.1097/GCO.0b013e32830dfa5c. [DOI] [PubMed] [Google Scholar]
- 23.Wells G, Cranney A, Tugwell P, et al. Meta-analyses of therapies for postmenopausal osteoporosis. V. Meta-analysis of the efficacy of hormone replacement therapy in treating and preventing osteoporosis in postmenopausal women. Endocrine Reviews. 2002;23:529. doi: 10.1210/er.2001-5002. [DOI] [PubMed] [Google Scholar]
- 24.Brincat M, Kabalan S, Studd JW, Moniz CF, de Trafford J, Montgomery J. A study of the decrease of skin collagen content, skin thickness, and bone mass in the postmenopausal woman. Obstetrics and Gynecology. 1987;70:840–5. [PubMed] [Google Scholar]
- 25.Sauerbronn AV, Fonseca AM, Bagnoli VR, Saldiva PH, Pinotti JA. The effects of systemic hormonal replacement therapy on the skin of postmenopausal women. International Journal of Gynaecology and Obstetrics. 2000;68:35–41. doi: 10.1016/s0020-7292(99)00166-6. [DOI] [PubMed] [Google Scholar]
- 26.Yu WD, Panossian V, Hatch JD, Liu SH, Finerman GA. Combined effects of estrogen and progesterone on the anterior cruciate ligament. Clinical Orthopaedics and Related Research. 2001;383:268–81. doi: 10.1097/00003086-200102000-00031. [DOI] [PubMed] [Google Scholar]
- 27.Seneviratne A, Attia E, Williams RJ, Rodeo SA, Hannafin JA. The effect of estrogen on ovine anterior cruciate ligament fibroblasts:cell proliferation and collagen synthesis. The American Journal of Sports Medicine. 2004;32:1613–8. doi: 10.1177/0363546503262179. [DOI] [PubMed] [Google Scholar]
- 28.Lee CY, Liu X, Smith CL, et al. The combined regulation of estrogen and cyclic tension on fibroblast biosynthesis derived from anterior cruciate ligament. Matrix Biology. 2004;23:323–9. doi: 10.1016/j.matbio.2004.07.004. [DOI] [PubMed] [Google Scholar]
- 29.Hewett TE, Myer GD, Ford KR. Anterior cruciate ligament injuries in female athletes:Part 1, mechanisms and risk factors. The American Journal of Sports Medicine. 2006;34:299–311. doi: 10.1177/0363546505284183. [DOI] [PubMed] [Google Scholar]
- 30.Lefevre N, Bohu Y, Klouche S, Lecocq J, Herman S. Anterior cruciate ligament tear during the menstrual cycle in female recreational skiers. Orthopaedics &Traumatology:Surgery & Research. 2013;99:571–5. doi: 10.1016/j.otsr.2013.02.005. [DOI] [PubMed] [Google Scholar]
- 31.Hart DA, Archambault JM, Kydd A, Reno C, Frank CB, Herzog W. Gender and neurogenic variables in tendon biology and repetitive motion disorders. Clinical Orthopaedics and Related Research. 1998;351:44–56. [PubMed] [Google Scholar]
- 32.Dehghan F, Muniandy S, Yusof A, Salleh N. Sex-steroid regulation of relaxin receptor isoforms (RXFP1 &RXFP2) expression in the patellar tendon and lateral collateral ligament of female WKY rats. International Journal of Medical Sciences. 2014;11:180–91. doi: 10.7150/ijms.6283. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.Hansen M, Couppe C, Hansen CSE, et al. Impact of oral contraceptive use and menstrual phases on patellar tendon morphology, biochemical composition, and biomechanical properties in female athletes. Journal of Applied Physiology. 2013;114:998–1008. doi: 10.1152/japplphysiol.01255.2012. [DOI] [PubMed] [Google Scholar]
- 34.Pingel J, Langberg H, Skovgård D, et al. Effects of transdermal estrogen on collagen turnover at rest and in response to exercise in postmenopausal women. Journal of Applied Physiology. 2012;113:1040–7. doi: 10.1152/japplphysiol.01463.2011. [DOI] [PubMed] [Google Scholar]
- 35.Hansen M, Koskinen SO, Petersen SG, et al. Ethinyl oestradiol administration in women suppresses synthesis of collagen in tendon in response to exercise. Journal of Physiology (London) 2008;586:3005–16. doi: 10.1113/jphysiol.2007.147348. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36.Systematic reviews:CRD's guidance for undertaking reviews in healthcare. 2009. at www.york.ac.uk/inst/crd/pdf/Systematic_Reviews.pdf .
- 37.Siegfried N, Muller M, Deeks J, et al. HIV and male circumcision-a systematic review with assessment of the quality of studies. The Lancet Infectious Diseases. 2005;5:165–73. doi: 10.1016/S1473-3099(05)01309-5. [DOI] [PubMed] [Google Scholar]
- 38.Reeves B, Deeks J, Higgins J, Wells G. Including non-randomized studies. In: Higgins J, Green S, editors. Cochrane Handbook for Systematic Reviews of Interventions. United Kingdom: John Wiley & Sons; 2008. [Google Scholar]
- 39.van Tulder M, Furlan A, Bombardier C, Bouter L. Editorial Board of the Cochrane Collaboration Back Review G Editorial Board Cochrane C. Updated method guidelines for systematic reviews in the cochrane collaboration back review group. Spine. 2003;28:1290–9. doi: 10.1097/01.BRS.0000065484.95996.AF. [DOI] [PubMed] [Google Scholar]
- 40.Yusuf E, Kortekaas MC, Watt I, Huizinga TWJ, Kloppenburg M. Do knee abnormalities visualised on MRI explain knee pain in knee osteoarthritis? A systematic review. Annals of the Rheumatic Diseases. 2011;70:60–7. doi: 10.1136/ard.2010.131904. [DOI] [PubMed] [Google Scholar]
- 41.Cochrane Handbook for Systematic Reviews. Version 5.1.0 [updated March 2011] The Cochrane Collaboration. 2011. at http://www.cochrane-handbook.org .
- 42.Des Jarlais D, Lyles C, Crepaz N, Group T. Improving the reporting quality of nonrandomized evaluations of behavioral and public health interventions:The TREND Statement. American Journal of Public Health. 2004;94:361–6. doi: 10.2105/ajph.94.3.361. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 43.Egger M, Schneider M, Smith GD. Spurious precision? Meta-analysis of observational studies. British Medical Journal. 1998;316:140–4. doi: 10.1136/bmj.316.7125.140. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 44.Higgins JPT, Thompson SG, Deeks JJ, Altman DG. Measuring inconsistency in meta-analyses. British Medical Journal (Clinical research edition) 2003;327:557–60. doi: 10.1136/bmj.327.7414.557. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 45.Herbert RD. How to estimate treatment effects from reports of clinical trials. I:continuous outcomes. Australian Journal of Physiotherapy. 2000;46:229–35. doi: 10.1016/s0004-9514(14)60334-2. [DOI] [PubMed] [Google Scholar]
- 46.Boyle MA, Samaha AL, Rodewald AM, Hoffmann AN. Evaluation of the reliability and validity of GraphClick as a data extraction program. Computers in Human Behavior. 2013;29:1023–7. [Google Scholar]
- 47.Bryant AL, Clark RA, Bartold S, et al. Effects of estrogen on the mechanical behavior of the human Achilles tendon in vivo. Journal of Applied Physiology. 2008;105:1035–43. doi: 10.1152/japplphysiol.01281.2007. [DOI] [PubMed] [Google Scholar]
- 48.Finni T, Kovanen V, Ronkainen PH, et al. Combination of hormone replacement therapy and high physical activity is associated with differences in Achilles tendon size in monozygotic female twin pairs. Journal of Applied Physiology. 2009;106:1332–7. doi: 10.1152/japplphysiol.91439.2008. [DOI] [PubMed] [Google Scholar]
- 49.Holmes GB, Lin J. Etiologic factors associated with symptomatic achilles tendinopathy. Foot and Ankle International. 2006;27:952–9. doi: 10.1177/107110070602701115. [DOI] [PubMed] [Google Scholar]
- 50.Langberg H, Skovgaard D, Petersen LJ, Bülow J, Kjær M. Type I collagen synthesis and degradation in peritendinous tissue after exercise determined by microdialysis in humans. The Journal of Physiology. 1999;521:299–306. doi: 10.1111/j.1469-7793.1999.00299.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 51.Cooper H, Hedges L. The Handbook of Research Synthesis. New York: Russell Sage Foundation; 1994. [Google Scholar]
- 52.Heinemeier KM, Schjerling P, Heinemeier J, Magnusson SP, Kjaer M. Lack of tissue renewal in human adult Achilles tendon is revealed by nuclear bomb 14C. Federation of American Societies of Experimental Biology. 2013;27:2074–9. doi: 10.1096/fj.12-225599. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 53.Rennard SI, Stier LE, Crystal RG. Intracellular degradation of newly synthesized collagen. The Journal of Investigative Dermatology. 1982;79(Suppl.1):77s–82s. doi: 10.1111/1523-1747.ep12545844. [DOI] [PubMed] [Google Scholar]
- 54.Steinberg J. The turnover of collagen in fibroblast cultures. Journal of Cell Science. 1973;12:217. doi: 10.1242/jcs.12.1.217. [DOI] [PubMed] [Google Scholar]
- 55.Humphries S, Lu Y, Canty E, Kadler K. Active Negative Control of Collagen Fibrillogenesis in Vivo: Intracellular cleavage of the type 1 procollagen propeptides in tendon fibroblasts without intracellular fibrils. The Journal of Biological Chemistry. 2008;283:12129–35. doi: 10.1074/jbc.M708198200. [DOI] [PubMed] [Google Scholar]
- 56.Bennell KL, Malcolm SA, Brukner PD, et al. A 12-month prospective study of the relationship between stress fractures and bone turnover in athletes. Calcified Tissue International. 1998;63:80–5. doi: 10.1007/s002239900493. [DOI] [PubMed] [Google Scholar]
- 57.Hansen M, Kjaer M. Influence of sex and estrogen on musculotendinous protein turnover at rest and after exercise. Exercise and Sport Sciences Reviews. 2014;42:183–92. doi: 10.1249/JES.0000000000000026. [DOI] [PubMed] [Google Scholar]
- 58.Hunter DG, Spriggs J. Investigation into the relationship between the passive flexibility and active stiffness of the ankle plantar-flexor muscles. Clinical Biomechanics. 2000;15:600–6. doi: 10.1016/s0268-0033(00)00017-6. [DOI] [PubMed] [Google Scholar]
- 59.Shruti A, Kornelia K. Tendinopathy alters mechanical and material properties of the Achilles tendon. Journal of Applied Physiology. 2010;108:670–5. doi: 10.1152/japplphysiol.00259.2009. [DOI] [PubMed] [Google Scholar]
- 60.Arampatzis A, Monte GD, Karamanidis K. Effect of joint rotation correction when measuring elongation of the gastrocnemius medialis tendon and aponeurosis. Journal of Electromyography and Kinesiology. 2008;18:503–8. doi: 10.1016/j.jelekin.2006.12.002. [DOI] [PubMed] [Google Scholar]
- 61.Magnusson SP, Hansen P, Aagaard P, et al. Differential strain patterns of the human gastrocnemius aponeurosis and free tendon, in vivo. Acta physiologica Scandinavica. 2003;177:185–95. doi: 10.1046/j.1365-201X.2003.01048.x. [DOI] [PubMed] [Google Scholar]
- 62.Kongsgaard M, Reitelseder S, Pedersen TG, et al. Region specific patellar tendon hypertrophy in humans following resistance training. Acta Physiologica. 2007;191:111–21. doi: 10.1111/j.1748-1716.2007.01714.x. [DOI] [PubMed] [Google Scholar]
- 63.Westh E, Kongsgaard M, Bojsen-Moller J, et al. Effect of habitual exercise on the structural and mechanical properties of human tendon, in vivo, in men and women:Effect of habitual exercise on the structural and mechanical properties of human tendon. Scandinavian Journal of Medicine & Science in Sports. 2008;18:23–30. doi: 10.1111/j.1600-0838.2007.00638.x. [DOI] [PubMed] [Google Scholar]
- 64.Muellbacher W, Ziemann U, Boroojerdi B, Cohen L, Hallett M. Role of the human motor cortex in rapid motor learning. Experimental Brain Research. 2001;136:431–8. doi: 10.1007/s002210000614. [DOI] [PubMed] [Google Scholar]
- 65.Muellbacher W, Ziemann U, Wissel J. Early consolidation in human primary motor cortex. Nature. 2002;415:640–4. doi: 10.1038/nature712. [DOI] [PubMed] [Google Scholar]
- 66.Andersson G, Forsgren S, Scott A, et al. Tenocyte hypercellularity and vascular proliferation in a rabbit model of tendinopathy:contralateral effects suggest the involvement of central neuronal mechanisms. British Journal of Sports Medicine. 2011;45:399–406. doi: 10.1136/bjsm.2009.068122. [DOI] [PubMed] [Google Scholar]
- 67.Hortobagyi T TJ, Petersen NT, et al. Changes in segmental contractions and motor cortical output with contralateral muscle contractions and altered sensory inputs in human. Journal of Neurophysiology. 2003;90:2451–9. doi: 10.1152/jn.01001.2002. [DOI] [PubMed] [Google Scholar]
- 68.Muellbacher W, Facchini S, Boroojerdi B. Changes in motor cortex excitability during ipsilateral hand muscle activation in humans. Clinical Neurophysiology. 2000;111:344–9. doi: 10.1016/s1388-2457(99)00243-6. [DOI] [PubMed] [Google Scholar]
- 69.Stedman A, Davey N, Ellaway P. Facilitation of human first dorsal interosseous muscle responses to transcranial magnetic stimulation during voluntary contraction of the contralateral homonymous muscle. Muscle Nerve. 1998;21:1033–9. doi: 10.1002/(sici)1097-4598(199808)21:8<1033::aid-mus7>3.0.co;2-9. [DOI] [PubMed] [Google Scholar]
- 70.Stinear C, Walker K, Byblow W. Symmetric facilitation between motor cortices during contraction of ipsilateral hand muscles. Experimental Brain Research. 2001;139 doi: 10.1007/s002210100758. [DOI] [PubMed] [Google Scholar]
- 71.Liepert J, Dettmers C, Terborg Cea. Inhibition of ipsilateral motor cortex during phasic generation of low force. Clinical Neurophysiology. 2001;112:114–21. doi: 10.1016/s1388-2457(00)00503-4. [DOI] [PubMed] [Google Scholar]
- 72.Dettmers C, Fink G, Lemon R. Relation between cerebral activity and force in the motor areas of the human brain. Journal of Neurophysiology. 1995;74:802–15. doi: 10.1152/jn.1995.74.2.802. [DOI] [PubMed] [Google Scholar]
- 73.Carson R, Riek S, Mackey D. Excitability changes in human forearm corticospinal projections and spinal reflex pathways during rhythmic voluntary movement of the opposite limb. Journal of Physioloogy. 2004;560(Pt 3) doi: 10.1113/jphysiol.2004.069088. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 74.Sabatino M, Caravaglios G, Sardo P ea. Evidence of a contralateral motor influence on reciprocal inhibition in man. Journal of Neural Transmission Parkinson's Disease and Dementia Section. 1992;4:257–66. doi: 10.1007/BF02260074. [DOI] [PubMed] [Google Scholar]
- 75.Delwaide P, Sabatino M, Pepin J. Reinforcement of reciprocal inhibition by contralateral movements in man. Experimental Neurology. 1988;99:75–98. doi: 10.1016/0014-4886(88)90122-7. [DOI] [PubMed] [Google Scholar]
- 76.Obst SJ, Barrett RS, Newsham-West R. Immediate effect of exercise on achilles tendon properties:systematic review. Medicine and Science in Sports and Exercise. 2013;45:1534–44. doi: 10.1249/MSS.0b013e318289d821. [DOI] [PubMed] [Google Scholar]