

Abstract
On the basis of current evidence derived from hospital-based studies, mostly from North India, the prevalence of psoriasis in adults varies from 0.44 to 2.8%, with a much lower prevalence in children. The peak age at onset in adults is in the third and fourth decade of life, with a slight male preponderance. It is recommended that population-based large epidemiologic studies should be undertaken in different parts of the country for estimating the correct prevalence of psoriasis in general population. Chronic plaque-type psoriasis is the most common morphologic presentation of psoriasis, accounting for more than 90% of all cases. Other morphologic variants that deserve special mention include palmoplantar psoriasis, pustular psoriasis, and recalcitrant psoriasis. For epidemiologic purposes, psoriasis can be classified into early and late onset psoriasis. Psoriasis can be classified on the basis of morphology and extent of involvement into localized and widespread disease. For the purpose of clinical trials, psoriasis may be classified as mild psoriasis, moderate psoriasis, and severe psoriasis. The literature shows that there is a significant risk of psoriatic arthritis (7–48%) in patients with plaque-type psoriasis. Hence, it is recommended to evaluate for its presence by detailed history taking and clinical examination, and if necessary, by appropriate radiological investigations. Evidence on the association between plaque-type psoriasis and cardiovascular disease risk factors and ischemic heart disease isinconsistent. On the basis ofavailable evidence, it is prudent to proactively look for metabolic syndrome, dyslipidemia, and obesity, especially in patientswith severe psoriasis (Level 1+ evidence based on systematic reviews and meta-analysis). Based on the current evidence, the psoriasis area severity index appears to be the most valid and reproducible clinical severity score in the management of adult patients with plaque-type psoriasis.
Keywords: Co-morbidities, epidemiology, psoriasis, severity scoring
INTRODUCTION
Psoriasis is a chronic inflammatory immune-mediated proliferative skin disorder that predominantly involves the skin, nails, and joints. Robert Willan, the father of modern dermatology, is credited with the first detailed clinical description of psoriasis, and hence, it is also termedas Willan'slepra.[1] The association between arthritis and psoriasis was described for the first time by Alibert in 1818, and the American Rheumatology Association recognized it as a separate entity in 1964.
Epidemiology
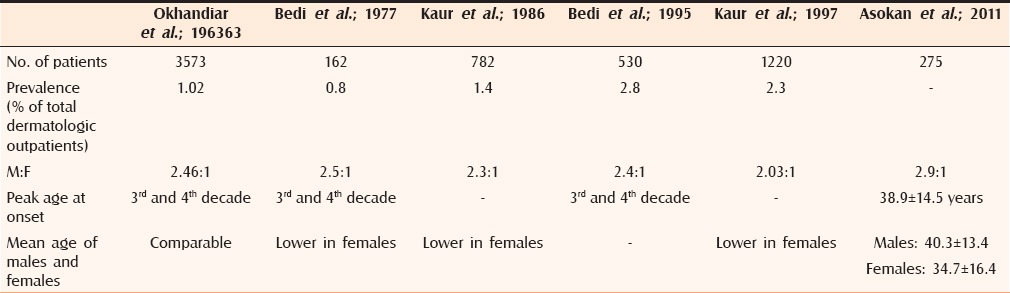
The worldwide prevalence of psoriasis is estimated to be approximately 2–3%.[2] Although the disease is known to have higher prevalence in the polar regions of the world, its burden in a tropical/subtropical country like India cannot be underestimated. In a diverse country such as India, the prevalence of psoriasis may vary from region to region due to variable environmental and genetic factors. We found only six studies, mostly in a hospital setting, from North India estimating the prevalence of disease among adult dermatologic patients [Table 1].[3,4,5,6,7,8] A higher prevalence in males has been reported with a peak age at onset is in the third and fourth decade of life.[9,10] In one of the larger studies from Northern India, point prevalence of pediatric psoriasis was estimated to be 0.0002%.[11] The peak age at onset among boys is in the 6–10 years age group compared to girls in 11–15 years age group.[12] A positive family history may be elicited in 9.8-28% of the children. The age at onset of psoriatic arthritis varies from 35 to 50 years with no sex predilection. Nearly 70% of the patients develop psoriasis before articular involvement; in another 15%, arthritis precedes the onset of psoriasis by more than 1 year, and in the remaining 15% of the cases, the two conditions occur within 12 months of each other.[13] The yearly estimated incidence and prevalence of psoriatic arthritis are, respectively, 3.0–23.1 cases/100,000 and 1–420 cases/100000 people,[14,15,16,17,18,19,20,21] with similar results in Western countries and in China. Prey et al. in their systematic review of literature concluded that psoriatic arthritis may affect upto 24% of patients with psoriasis.[14] Such data is lacking among Indian patients. In children, arthritis may precede psoriasis in 50% of cases. The mean age of onset in children is 9–10 years with female predominance.[22]
Table 1.
Epidemiologic studies of psoriasis in adults in India
DEFINITIONS, CLASSIFICATION, AND CLINICAL PRESENTATION
Psoriasis
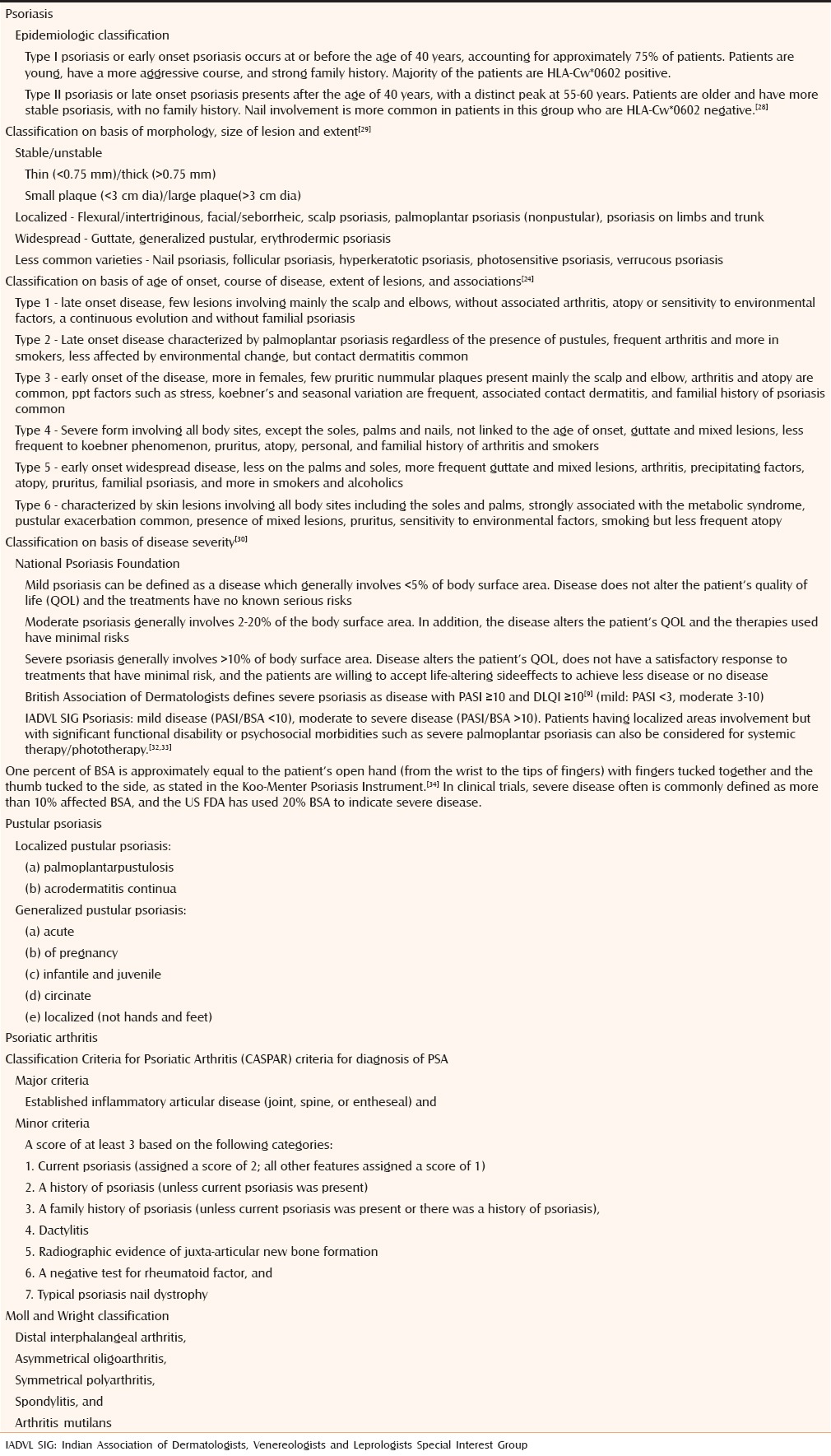
There is no clear definition or criteria proposed for the diagnosis of psoriasis as the diagnosis is essentially clinical. Based on the current understanding of its pathogenesis, psoriasis can be defined as a papulosquamous disorder characterized by disordered keratinization arising due to T cell-mediated immune dysregulaion. Epidemiologically, psoriasis has been classified into early onset and late onset psoriasis by Henseler and Christophers [Table 2].[23] Guinot et al. have recently classified psoriasis into six phenotypic types.[24]
Table 2.
Classification of psoriasis vulgaris, pustular psoriasis, and psoriatic arthritis
Psoriatic arthritis
Psoriatic arthritis belongs to the broad group of spondyloarthropathies which is characterized by its association with psoriasis and seronegativity for rheumatoid factor.[25] The most accepted classification criteria has been published in 2006 by the Classification Criteria for Psoriatic Arthritis (CASPAR) study group [Table 2].[26] CASPAR classification is easy to use enabling psoriatic arthritis to be diagnosed in the presence of rheumatoid factor and absence of psoriasis, provided typical findings of psoriatic arthritis are present. It has high sensitivity in early psoriatic arthritis, and may, therefore, be used to classify patients early in the course of disease.[27]
Pustular psoriasis
Pustular psoriasisis characterized by appearance of macroscopic sterile pustules in a patient with psoriasis. On the basis of extent of involvement, it can be classified into localized or generalized disease [Table 2].
Chronic plaque-type psoriasis is the most common morphologic variety which manifests as circumscribed, well-demarcated, erythematous plaques involving particularly the extensor aspects of elbows and knees, buttocks, scalp, and lower back. The character of scaling varies from the typical silvery-white scales to waxy yellow or orange-brown scales. Other clinical patterns of psoriasis include guttate psoriasis, unstable psoriasis, hyperkeratotic psoriasis, erythrodermic, and pustularpsoriasis, uncommon variants such asfollicular psoriasis, eczematous psoriasis, flexural psoriasis, nail psoriasis, and photosensitive psoriasis. The Medical Advisory Board of the National Psoriasis Foundation has defined mild, moderate, and severe psoriasis based largely on quality-of-life (QOL) measures, with consideration also given to proportion of body surface area affected [Table 2].[31]
As in adult psoriasis, chronic plaque psoriasis with its variants is the most frequent type in infancy and childhood. Inverse psoriasis is more common in children than inadults. In infants, the disease may manifest as diaper dermatitis. In small children and adolescents, guttate psoriasis is another distinct presentation and has been reported in up to 44% of patients.[35] Pustularpsoriasis, although rare in children, can present with certain typical morphological patterns such as annular and circinate pustular psoriasis. Annular pustular psoriasis is characterized by gyrate lesions with erythema and a collarette of scales at the periphery. Psoriatic erythroderma and psoriatic arthritis are relatively less common. International Psoriasis Council has put forward a new classification thatincludes various clinical phenotypes of psoriasis and may be relevant to clinical practitioners and researchers.[30]
Psoriatic arthritis: Clinical features
Three different clinical patterns of psoriatic arthritis can be recognized, namely, oligoarticular (≤4 involved joints) or polyarticular (≥5involved joints), peripheral disease, and axial disease with or without peripheral arthritis. Various studies have shown peripheral psoriatic arthritis to be the most frequent pattern with asymmetric knee involvement to be the most common presentation in 40% of the patients.[36] The DIP arthritis has been reported to account for 1–59% of cases in various studies, although it is not very specific for psoriatic arthritis and may be seen in other spondyloarthropathies. It is often associated with dactylitis and nail dystrophy.[37] Variables that predict the severity of disease include polyarticular involvement at the onsetincluseraised erythrocyte sedimentation rate, late onset disease, HLA-B27 positivity for psoriatic arthritis spondylitis, and presence of TNF-α-308 and TNF-β-252 gene polymorphism.[38] Nail involvement occurs in nearly 75% of psoriatic patients with arthritis. Axial psoriatic arthritis is seen in 5–36% of the patients with psoriatic arthritis; axial involvement may be in the form of sacroiliitis or limited to only one tract of the spine with or without concomitant peripheral arthritis.[39] Axial psoriatic arthritis may only affect the cervical spine with sparing of other tracts of the axial skeleton.[40] It is characterized by a better prognosis and minor functional damage compared to ankylosingspondylitis. Enthesitis represents a hallmark of the clinical spectrum of psoriatic arthritis, and it is usually defined in the presence of tenderness and swelling in an enthesis site. Plantar fasciitis and Achille’senthesitis are very common. Dactylitis or the “sausage-shaped digit”is defined as a diffuse swelling of the entire digit and is seen in 5.6–53% of reported cases.[38,39] The swelling is believed to be due to a combination of flexor tenosynovitis and interphalangeal joint synovitis. Distal extremity swelling with pitting edema is not infrequently observed in psoriatic arthritis (in nearly 21% patients). When distal edema involves the dorsum of the hand a“boxing glove”appearance is seen.
CO-MORBIDITIES ASSOCIATED WITH PSORIASIS
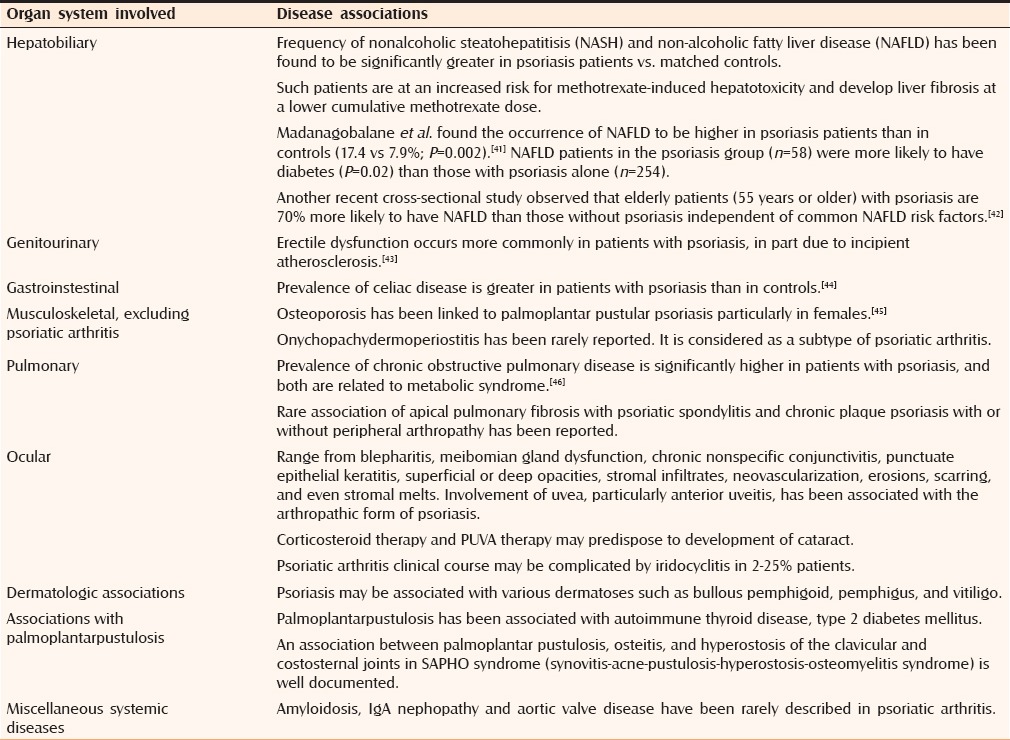
Psoriasis has been associated with numerous dermatologic and non-dermatologic diseases [Table 3].[41,42,43,44,45,46] In recent years, there has been an enormous interest on the association of psoriasis with conventional cardiovascular risk factors (e.g., metabolic syndrome, obesity, low physical activity, smoking, alcohol, lipid abnormalities, hypertension), nonconventional cardiovascular risk factors such as deranged homocysteine metabolism, cardiovascular comorbidities, and increased risk of myocardial infarction and myocardial infarction.[47,48] However, the data supporting the occurrence of such an association is not consistent. The prevalence of metabolic syndrome in the developed countries varies from 15 to 35%.[49] Two Indian studies that differed in their definition of obesity reported the prevalence of 13 and 41% in general population.[50,51] The third Indian study reported a prevalence of 11.2% for metabolic syndrome.[52]
Table 3.
Disease associations with psoriasis
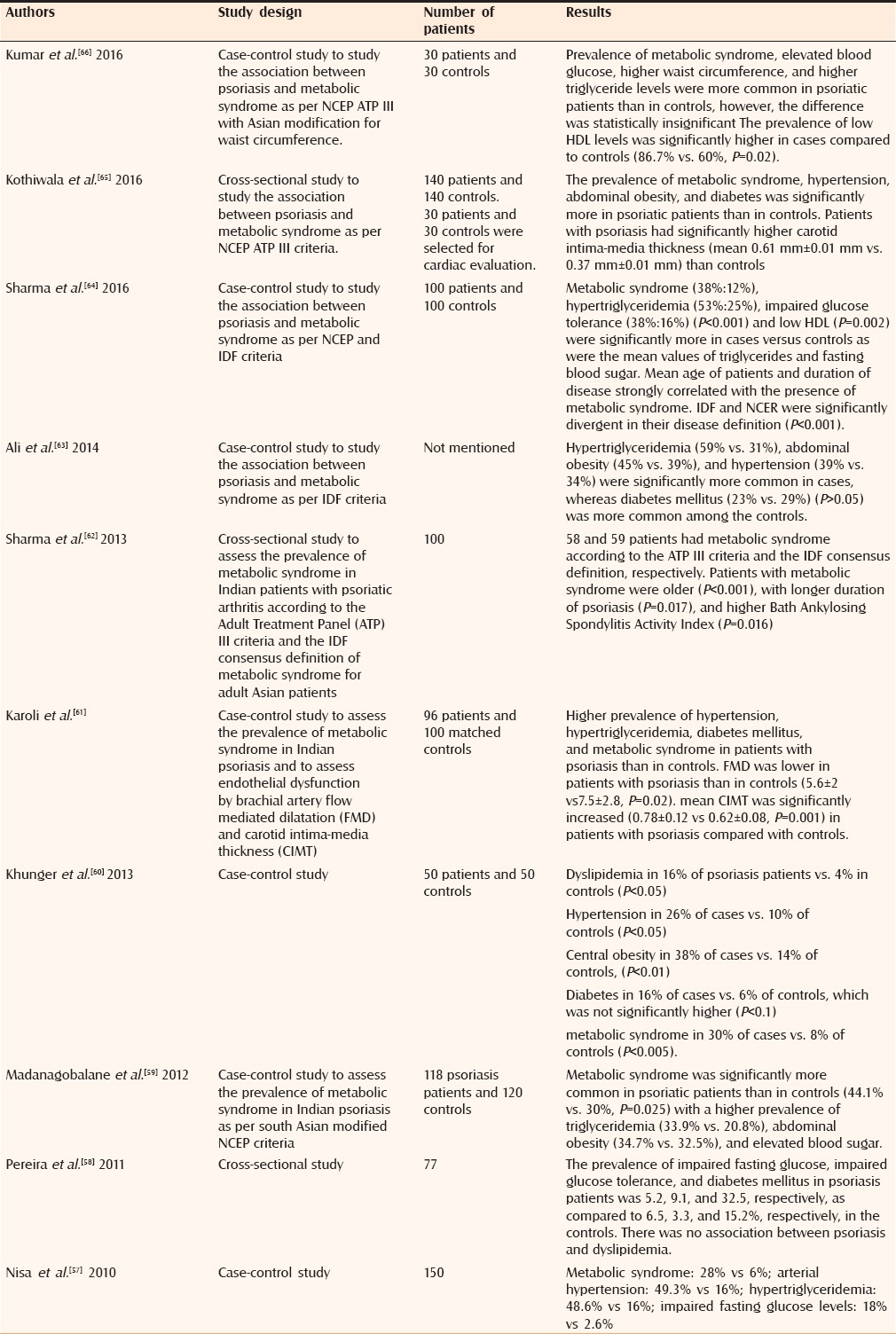
In one of the largest and well-conducted meta-analysis, it was concluded that, based on information, mostly from hospital-based studies, psoriasis is associated with cardiovascular disease and its risk factors, and not with cerebrovascular disease.[53] The association is stronger with psoriatic arthritis compared to psoriasis. However, Prey et al. in their systematic review of epidemiologic studies studying the cardiovascular risk factors in chronic plaque psoriasis concluded that there is an increased risk of obesity and metabolic syndrome in psoriasis, although no consistent results were found with hypertension, diabetes, and dyslipidemia.[48] Armstrong et al. in their systematic review alsofound similar results, especially in severe psoriasis.[54] In another recent systematic review and meta-analysis, Samarasekera et al. noted that increased cardiovascular risk was identified only in individuals with severe psoriasis (requiring systemic therapy or hospital admission).[55] They also observed that uncertainty remains about whether cardiovascular risk is directly attributable to psoriasis, as the majority of studies failed to adequately adjust for key traditional risk factors. In the landmark population-based Rotterdam study, the risk of incident cardiovascular disease was not increased in psoriasis.[56] Although, the patient population in this study was younger, smoked more, had higher diastolic blood pressure and body mass index levels compared to controls, there was no significant difference in the adjusted carotid intima-media thickness, crude and adjusted ankle-brachial index, pulse-wave velocity, and coronary artery calcium scores. Table 4 summarizes the results of Indian studies evaluating association between psoriasis and metabolic syndrome.[57,58,59,60,61,62,63,64,65,66]
Table 4.
Indian studies estimating the risk of cardiovascular disease risk factors in psoriasis
CLINICAL SCORES IN PSORIASIS
A variety of scoring systems have been used to assess the severity of plaque-type psoriasis. These include the clinical severity scores and quality of life scores, which are enumerated in Table 5. The clinical scores incorporate and grade the typical clinical features of psoriasis, i.e., erythema, scaling, infiltration, and extent of body surface area involved. Few scores, such asSPI, also include the psychosocial impact of the disease. Puzenat et al. in their systematic review identified 44 clinical severity scores, of which only 6 were correctly defined and validated.[67] Tables 6 and 7 summarize the salient features of these clinical severity scores. All scores except SAPASI are assessed by physicians. Although PASI, BSA, and PGA have been approved by FDA for use in clinical trials, all have certain pitfalls. The most widely used scale is PASI as it is the most extensively validated, however, it lacks sensitivity for mild disease and does not evaluate quality of life impairment and comorbidities. A 75% reduction in the PASI score (PASI 75) is the current benchmark of primary endpoints for most clinical trials of psoriasis. However, Carlin et al. concluded that PASI of 50 equates to a clinically meaningful improvement in psoriasis. They observed that PASI score is not linearly reflective of psoriasis severity and that an improvement in quality of life exists at PASI 50.[68] British Association of Dermatologists defined adequate response to treatment as either attainment of PASI 50 and decrease in ≥5 points in DLQI or attainment of PASI 75.[69]
Table 5.
Various clinical severity scores and quality of life impairment scores employed in assessing psoriasis severity
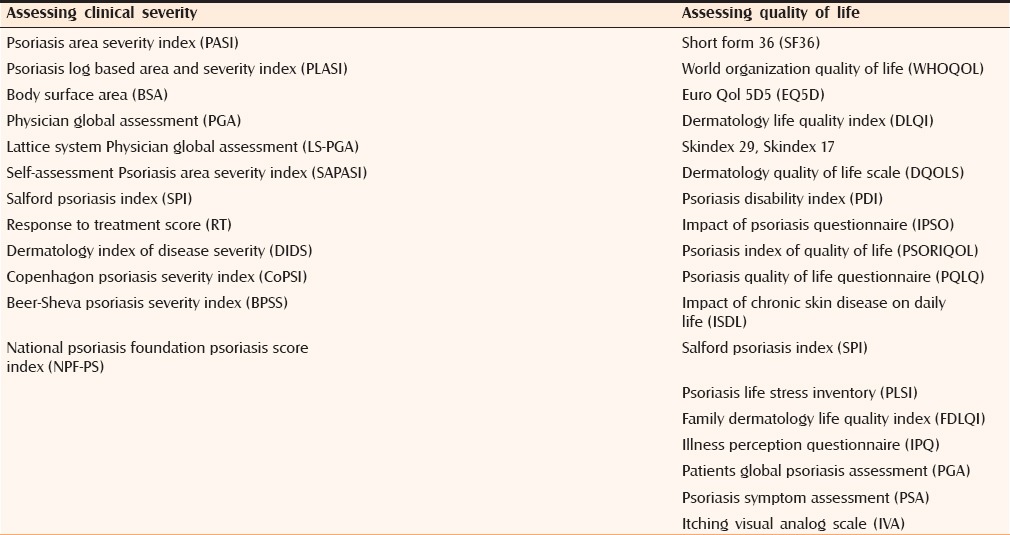
Table 6.
Salient features of clinical severity scores in psoriasis
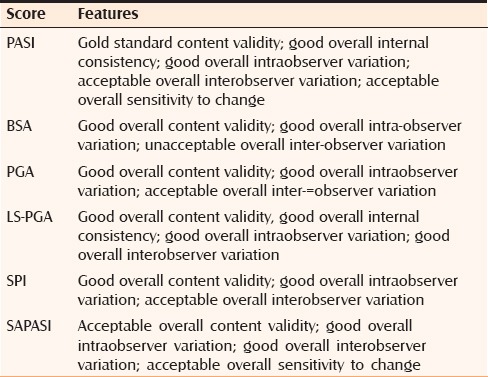
Table 7.
Salient features of quality of life impairment scores in psoriasis
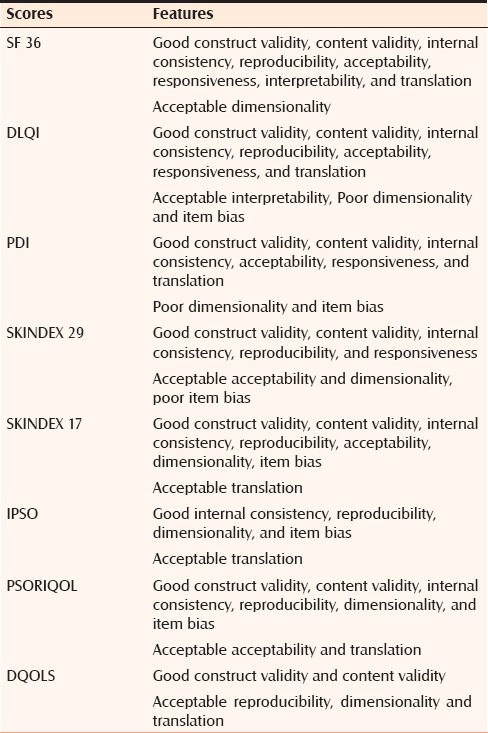
Psoriasis has a significant negative impact on patients’ health related quality of life. Lower quality of life in psoriasis patientsis due to its physical symptoms such as pruritus, scaling and joint pains, financial and psychosocial impact leading to problems of self-esteem, stigmatization, feeling of shame and embarrassment, and maladaptive coping responses. Bronsard et al. in their systematic review of quality of life scores in psoriasis identified 21 questionnaires, of which 8 satisfied the validation criteria.[70] The advantages and the shortcomings of each of these scores are summarized in Table 7. Bronsard et al. concluded that DLQI is the easiest to use in clinical trials due to its brevity and simplicity.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
REFERENCES
- 1.Glickman FS. Lepra, psora, psoriasis. J Am Acad Dermatol. 1986;14:863–6. doi: 10.1016/s0190-9622(86)70101-1. [DOI] [PubMed] [Google Scholar]
- 2.Pariser DM, Bagel J, Gelfand JM, Korman NJ, Ritchlin CT, Strober BE, et al. National Psoriasis Foundation Clinical Consensus on Disease Severity. Arch Dermatol. 2007;143:239–24. doi: 10.1001/archderm.143.2.239. [DOI] [PubMed] [Google Scholar]
- 3.Okhandiar RP, Banerjee BN. Psoriasis in the tropics: An epidemiological survey. J Indian Med Assoc. 1963;41:550–6. [PubMed] [Google Scholar]
- 4.Bedi TR. Psoriasis in north India. Geographical variations. Dermatologica. 1977;155:310–4. doi: 10.1159/000250983. [DOI] [PubMed] [Google Scholar]
- 5.Kaur I, Kumar B, Sharma VK, Kaur S. Epidemiology of psoriasis in a clinic from north India. Indian J Dermatol Venereol Leprol. 1986;52:208–12. [PubMed] [Google Scholar]
- 6.Bedi TR. Clinical profile of psoriasis in North India. Indian J Dermatol Venereol Leprol. 1995;61:202–5. [PubMed] [Google Scholar]
- 7.Kaur I, Handa S, Kumar B. Natural history of psoriasis: Astudy from the Indian subcontinent. J Dermatol. 1997;24:230–4. doi: 10.1111/j.1346-8138.1997.tb02779.x. [DOI] [PubMed] [Google Scholar]
- 8.Asokan N, Prathap P, Ajithkumar K, Betsy A, Binesh VG. Pattern of psoriasis in a tertiary care teaching hospital in south India. Indian J Dermatol. 2011;56:118–9. doi: 10.4103/0019-5154.77575. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Lal S. Clinical pattern of psoriasis in Punjab. Indian J Dermatol Venereol Leprol. 1966;35:5–12. [PubMed] [Google Scholar]
- 10.Mehta TK, Shah RN, Marquis L. A study of 300 cases of psoriasis. Indian J Dermatol Venereol Leprol. 1976;42:67–74. [PubMed] [Google Scholar]
- 11.Dogra S, Kumar B. Epidemiology of Skin Diseases in School Children: A Study from Northern India. Paed Dermatol. 2003;20:470–3. doi: 10.1111/j.1525-1470.2003.20602.x. [DOI] [PubMed] [Google Scholar]
- 12.Kumar B, Jain R, Sandhu K, Kaur I, Handa S. Epidemiology of childhood psoriasis: A study of 419 patients from northern India. Int J Dermatol. 2004;43:654–8. doi: 10.1111/j.1365-4632.2004.02182.x. [DOI] [PubMed] [Google Scholar]
- 13.Leonard DG, O’Duffy JD, Rogers RS. Prospective analysis of psoriatic arthritis in patients hospitalized for psoriasis. Mayo Clin Proc. 1978;53:511–8. [PubMed] [Google Scholar]
- 14.Prey S, Paul C, Bronsard V, Puzenat E, Gourraud PA, Aractingi S, et al. Assessment of risk of psoriatic arthritis in patients with plaque psoriasis: A systematic review of the literature. J Eur Aacd Dermatol Venereol. 2010;24:31–5. doi: 10.1111/j.1468-3083.2009.03565.x. [DOI] [PubMed] [Google Scholar]
- 15.Hukuda S, Minami M, Saito T, Mutsui H, Matsui N, Komatsubara Y, et al. Spondyloarthropathies in Japan: Nationwide questionnaire survey performed by the Japan Ankylosing Spondylitis Society. J Rheumatol. 2001;28:554–9. [PubMed] [Google Scholar]
- 16.Alamanos Y, Papadopoulos NG, Voulgari PV, Siozas C, Psychos DN, Tympanidou M, et al. Epidemiology of psoriatic arthritis in northwest Greece, 1982–2001. J Rheumatol. 2003;30:2641–4. [PubMed] [Google Scholar]
- 17.Wilson FC, Icen M, Crowson CS, McEvoy MT, Gabriel SE, Kremers HM. Time trends in epidemiology and characteristics of psoriatic arthritis over 3 decades: A population-based study. J Rheumatol. 2009;36:361–7. doi: 10.3899/jrheum.080691. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Gelfand JM, Gladman DD, Mease PJ, Smith N, Margolis DJ, Nijsten T, et al. Epidemiology of psoriatic arthritis in the population of the United States. J Am Acad Dermatol. 2005;53:573. doi: 10.1016/j.jaad.2005.03.046. [DOI] [PubMed] [Google Scholar]
- 19.Madland TM, Apalset EM, Johannessen AE, Rossebo B, Brun JG. Prevalence, disease manifestations, and treatment of psoriatic arthritis in Western Norway. J Rheumatol. 2005;32:1918–22. [PubMed] [Google Scholar]
- 20.Love TJ, Gudbjornsson B, Gudjonsson JE, Valdimarsson H. Psoratic arthritis in Reykjavik, Iceland: Prevalence, demographics, and disease course. J Rheumatol. 2007;34:2082–8. [PubMed] [Google Scholar]
- 21.Zeng QY, Chen R, Darmawan J, Xiao ZY, Chen SB, Wigley R, et al. Rheumatic diseases in China. Arthritis Res Ther. 2008;10:17. doi: 10.1186/ar2368. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Stoll ML, Lio P, Sundel RP, Nigrovic PA. Comparison of Vancouver and International League of Associations for rheumatology classification criteria for juvenile psoriatic arthritis. Arthritis Rheum. 2008;59:51–8. doi: 10.1002/art.23240. [DOI] [PubMed] [Google Scholar]
- 23.Hanseler T, Christopher E. Psoriasis of early and late onset: Characterization of two types of psoriasis vulgaris. J Am AcadDermatol. 1985;13:450–6. doi: 10.1016/s0190-9622(85)70188-0. [DOI] [PubMed] [Google Scholar]
- 24.Guinot C, Latreille J, Perrussel M, Doss N, Dubertret L French Psoriasis Group. Psoriasis: Characterization of six different clinical phenotypes. Exp Dermatol. 2009;18:712–9. doi: 10.1111/j.1600-0625.2009.00871.x. [DOI] [PubMed] [Google Scholar]
- 25.Moll JM, Wright V. Psoriatic arthritis. Semin Arthritis Rheum. 1973;3:55–78. doi: 10.1016/0049-0172(73)90035-8. [DOI] [PubMed] [Google Scholar]
- 26.Taylor W, Gladman D, Helliwell P, Marchesoni A, Mease P CASPAR study group. Classification criteria for psoriatic arthritis. Arthritis rheum. 2006;54:2665–73. doi: 10.1002/art.21972. [DOI] [PubMed] [Google Scholar]
- 27.Chandran V, Schentag CT, Gladman DD. Sensitivity of the classification of psoriatic arthritis criteria in early psoriatic arthritis. Arthritis Rheum. 2007;57:1560–3. doi: 10.1002/art.23104. [DOI] [PubMed] [Google Scholar]
- 28.Gudjonsson JE, Karason A, Runarsdottir EH, Antonsdottir AA, Hauksson VB, Jonsson HH, et al. Distinct clinical differences between HLA-Cw*0602 positive and negative psoriasis patients-An analysis of 1019 HLA-C- and HLA-B-typed patients. J Invest Dermatol. 2006;126:740–5. doi: 10.1038/sj.jid.5700118. [DOI] [PubMed] [Google Scholar]
- 29.Griffiths CE, Christophers E, Barker JN, Chalmers RJ, Chimenti S, Krueger GG, et al. A classification of psoriasis vulgaris according to phenotype. Br J Dermatol. 2007;156:258–62. doi: 10.1111/j.1365-2133.2006.07675.x. [DOI] [PubMed] [Google Scholar]
- 30.Pariser DM, Bagel J, Gelfand JM, Korman NJ, Ritchlin CT, Strober BE, et al. National Psoriasis Foundation Clinical Consensus on Disease Severity. Arch Dermatol. 2007;143:239–24. doi: 10.1001/archderm.143.2.239. [DOI] [PubMed] [Google Scholar]
- 31.Smith CH, Anstey AV, Barker JN, Burden AD, Chalmers RJ, Chandler DA, et al. British Association of Dermatologist's guidelines for biologic interventions for psoriasis 2009. Br J Dermatol. 2009;161:987–1019. doi: 10.1111/j.1365-2133.2009.09505.x. [DOI] [PubMed] [Google Scholar]
- 32.Janagond AB, Kanwar AJ, Handa S. Efficacy and safety of systemic methotrexate vs. acitretin in psoriasis patients with significant palmoplantar involvement: A prospective, randomized study. J Eur Acad Dermatol Venereol. 2013;27:e384–9. doi: 10.1111/jdv.12004. [DOI] [PubMed] [Google Scholar]
- 33.Feldman SR, Koo JY, Menter A, Bagel J. Decision points for the initiation of systemic treatment for psoriasis. J Am Acad Dermatol. 2005;53:101–7. doi: 10.1016/j.jaad.2005.03.050. [DOI] [PubMed] [Google Scholar]
- 34.Gupta SK, Singh KK, Lalit M. Comparative therapeutic evaluation of different topicals and narrow band ultraviolet B therapy combined with systemic methotrexate in the treatment of palmoplantar psoriasis. Indian J Dermatol. 2011;56:165–70. doi: 10.4103/0019-5154.80410. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.Cordoro KM. Management of Childhood Psoriasis. Adv Dermatol. 2008;24:125–69. doi: 10.1016/j.yadr.2008.09.009. [DOI] [PubMed] [Google Scholar]
- 36.Marsa S, Armadans-Gil L, Martinez M, Gallardo D, Ribera A, Lience E. Clinical, radiographic and HLA associations as markers for different patterns of psoriatic arthritis. Rheumatology. 1999;38:332–7. doi: 10.1093/rheumatology/38.4.332. [DOI] [PubMed] [Google Scholar]
- 37.Veale D, Rogers S, Fiztgerald O. Classification of clinical subsets in psoriatic arthritis. Br J Rheumatol. 1994;33:133–8. doi: 10.1093/rheumatology/33.2.133. [DOI] [PubMed] [Google Scholar]
- 38.Balding J, Kane D, Livingstone W, Mynett-Johnson L, Bresnihan B, Smith O, et al. Cytokine gene polymorphisms: Association with psoriatic arthritis susceptibility and severity. Arthritis Rheum. 2003;48:1408–13. doi: 10.1002/art.10935. [DOI] [PubMed] [Google Scholar]
- 39.Chandran V, Barrett J, Schentag CT, Farewell VT, Gladman DD. Axial psoriatic arthritis: Update on a long term prospective study. J Rheumatol. 2009;36:2744–50. doi: 10.3899/jrheum.090412. [DOI] [PubMed] [Google Scholar]
- 40.Russell EB, Hunter JB, Pearson L, McCarty DJ. Remitting, seronegative, symmetrical synovitis with pitting edema – 13 additional cases. J Rheumatol. 1990;17:633–9. [PubMed] [Google Scholar]
- 41.Madanagobalane S, Anandan S. The increased prevalence of non-alcoholic fatty liver disease in psoriatic patients: A study from South India. Australas J Dermatol. 2012;53:190–7. doi: 10.1111/j.1440-0960.2012.00905.x. [DOI] [PubMed] [Google Scholar]
- 42.van der Voort EA, Koehler EM, Dowlatshahi EA, Hofman A, Stricker BH, Janssen HL, et al. Psoriasis is independently associated with nonalcoholic fatty liver disease in patients 55 years old or older: Results from a population-based study. J Am Acad Dermatol. 2014;70(3):517–24. doi: 10.1016/j.jaad.2013.10.044. [DOI] [PubMed] [Google Scholar]
- 43.Goulding JM, Price CL, Defty CL, Hulangamuwa CS, Bader E, Ahmed I. Erectile dysfunction in patients with psoriasis: Increased prevalence, an unmet need, and a chance to intervene. Br J Dermatol. 2011;164:103–9. doi: 10.1111/j.1365-2133.2010.10077.x. [DOI] [PubMed] [Google Scholar]
- 44.Birkenfeld S, Dreiher J, Weitzman D, Cohen AD. Coeliac disease associated with psoriasis. Br J Dermatol. 2009;161:1331–4. doi: 10.1111/j.1365-2133.2009.09398.x. [DOI] [PubMed] [Google Scholar]
- 45.Dreiher J, Weitzman D, Cohen AD. Psoriasis and osteoporosis: A sex-specific association? J Invest Dermatol. 2009;129:1643–9. doi: 10.1038/jid.2008.432. [DOI] [PubMed] [Google Scholar]
- 46.Dreiher J, Weitzman D, Shapiro J, Davidovici B, Cohen AD. Psoriasis and chronic obstructive pulmonary disease: Acase-control study. Br J Dermatol. 2008;159:956–60. doi: 10.1111/j.1365-2133.2008.08749.x. [DOI] [PubMed] [Google Scholar]
- 47.Menter A, Griffiths CEM, Tebbey PW, Horn EJ, Sterry W. Exploring the association between cardiovascular and other disease-related risk factors in the psoriasis population: The need for increased understanding across the medical community. J Eur Aacd Dermatol Venereol. 2010;24:1371–7. doi: 10.1111/j.1468-3083.2010.03656.x. [DOI] [PubMed] [Google Scholar]
- 48.Prey S, Paul C, Bronsard P, Puzenat E, Gourraud PA, Aractingi S, et al. Cardiovascular risk factors in patients with plaque psoriasis: A systematic review of epidemiological studies. J Eur Aacd Dermatol Venereol. 2010;24(S):23–30. doi: 10.1111/j.1468-3083.2009.03564.x. [DOI] [PubMed] [Google Scholar]
- 49.Cameron AJ, Shaw JE, Zimmet PZ. The metabolic syndrome: Prevalence in worldwide populations. Endocrinol Metab Clin North Am. 2004;33:351–75. doi: 10.1016/j.ecl.2004.03.005. [DOI] [PubMed] [Google Scholar]
- 50.Ramachandran A, Snehalatha SC, Satyavani K, Sivasankari S, Vijay V. Metabolic syndrome in urban Asian Indian adults-Apopulation study using modified ATP III criteria. Diabetes Res Clin Pract. 2003;60:199–204. doi: 10.1016/s0168-8227(03)00060-3. [DOI] [PubMed] [Google Scholar]
- 51.Gupta A, Gupta R, Sarna M, Rastogi S, Gupta VP, Kothari K. Prevalence of diabetes, impaired fasting glucose and insulin resistance syndrome in an urban Indian population. Diabetes Res Clin Pract. 2003;61:69–76. doi: 10.1016/s0168-8227(03)00085-8. [DOI] [PubMed] [Google Scholar]
- 52.Deepa R, Shanthirani CS, Premalatha G, Sastry NG, Mohan V. Prevalence of insulin resistance syndrome in a selected south Indian population-The Chennai urban population study-7 [CUPS-7] Indian J Med Res. 2002;115:118–27. [PubMed] [Google Scholar]
- 53.Miller IM, Ellervik C, Yazdanyar S, Jemec GB. Meta-analysis of psoriasis, cardiovascular disease, and associated risk factors. J Am Acad Dermatol. 2013;69:1014–24. doi: 10.1016/j.jaad.2013.06.053. [DOI] [PubMed] [Google Scholar]
- 54.Armstrong AW, Harskamp CT, Armstrong EJ. Psoriasis and metabolicsyndrome: A systematic review and meta-analysis of observational studies. J Am AcadDermatol. 2013;68:654–62. doi: 10.1016/j.jaad.2012.08.015. [DOI] [PubMed] [Google Scholar]
- 55.Samarasekera EJ, Neilson JM, Warren RB, Parnham J, Smith CH. Incidence of cardiovascular disease in individuals with psoriasis: A systematic review and meta-analysis. J Invest Dermatol. 2013;133:2340–6. doi: 10.1038/jid.2013.149. [DOI] [PubMed] [Google Scholar]
- 56.Dowlatshahi EA, Kavousi M, Nijsten T, Ikram MA, Hofman A, Franco OH, et al. Psoriasis is not associated with atherosclerosis and incident cardiovascular events: The Rotterdam Study. J Invest Dermatol. 2013;133:2347–54. doi: 10.1038/jid.2013.131. [DOI] [PubMed] [Google Scholar]
- 57.Nisa N, Qazi MA. Prevalence of metabolic syndrome in patients with psoriasis. Indian J Dermatol Venereol Leprol. 2010;76:662–5. doi: 10.4103/0378-6323.72462. [DOI] [PubMed] [Google Scholar]
- 58.Pereira RR, Amladi ST, Varthakavi PK. A study of the prevalence of diabetes, insulin resistance, lipid abnormalities, and cardiovascular risk factors in patients with chronic plaque psoriasis. Indian J Dermatol. 2011;56:520–6. doi: 10.4103/0019-5154.87144. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 59.Madanagobalane S, Ananda S. Prevalence of metabolic syndrome in South Indian patients with psoriasis vulgaris and the relation between disease severity and metabolic syndrome: A hospital-based case-control study. Indian J Dermatol. 2012;57:353–7. doi: 10.4103/0019-5154.100474. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 60.Khunger N, Gupta D, Ramesh V. Is psoriasis a new cutaneous marker for metabolicsyndrome? A study in Indian patients. Indian J Dermatol. 2013;58:313–4. doi: 10.4103/0019-5154.113958. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 61.Karoli R, Fatima J, Shukla V, Dhillon KS, Khanduri S, Maini S, et al. A study of cardio-metabolic risk profile in patients with psoriasis. J Assoc Physicians India. 2013;61:798–803. [PubMed] [Google Scholar]
- 62.Sharma A, Gopalakrishnan D, Kumar R, Vijayvergiya R, Dogra S. Metabolicsyndrome in psoriatic arthritis patients: A cross-sectional study. Int J Rheum Dis. 2013;16:667–73. doi: 10.1111/1756-185X.12134. [DOI] [PubMed] [Google Scholar]
- 63.Ali NM, Kuruvila M, Unnikrishnan B. Psoriasis and metabolic syndrome: A case control study. Indian J Dermatol Venereol Leprol. 2014;80:255–7. doi: 10.4103/0378-6323.132257. [DOI] [PubMed] [Google Scholar]
- 64.Sharma YK, Prakash N, Gupta A. Prevalence of metabolic syndrome as per the NCEP and IDF definitions vis-a-vis severity and duration of psoriasis in a semi-urban Maharashtrian population: A case control study. Diabetes Metab Syndr. 2016 doi: 10.1016/j.dsx.2016.01.033. Epub ahead of print. [DOI] [PubMed] [Google Scholar]
- 65.Kothiwala SK, Khanna N, Tandon N, Naik N, Sharma VK, Sharma S, et al. Prevalence of metabolic syndrome and cardiovascular changes in patients with chronic plaque psoriasis and their correlation with disease severity: A hospital-based cross-sectional study. Indian J Dermatol Venereol Leprol. 2016;82:510–8. doi: 10.4103/0378-6323.183638. [DOI] [PubMed] [Google Scholar]
- 66.Praveenkumar U, Ganguly S, Ray L, Nanda SK, Kuruvila S. Prevalence of Metabolic Syndrome in Psoriasis Patients and its Relation to Disease Duration: A Hospital Based Case-Control Study. J Clin Diagn Res. 2016;10:WC01–5. doi: 10.7860/JCDR/2016/17791.7218. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 67.Puzenat E, Bronsard V, Prey S, Gourraud PA, Aractingi S, Bagot M, et al. What are the best outcome measures for assessing plaque psoriasis severity? A systematic review of the literature J Eur Aacd Dermatol Venereol. 2010;24:S10–6. doi: 10.1111/j.1468-3083.2009.03562.x. [DOI] [PubMed] [Google Scholar]
- 68.Carlin CS, Feldman SR, Krueger JG, Menter A, Krueger GG. A 50% reduction in the Psoriasis Area and Severity Index (PASI 50) is a clinically significant endpoint in the assessment of psoriasis. J Am Acad Dermatol. 2004;50:859–66. doi: 10.1016/j.jaad.2003.09.014. [DOI] [PubMed] [Google Scholar]
- 69.Smith CH, Anstey AV, Barker JN, Burden AD, Chalmers RJ, Chandler DA, et al. British Association of Dermatologist's guidelines for biologic interventions for psoriasis 2009. Br J Dermatol. 2009;161:987–1019. doi: 10.1111/j.1365-2133.2009.09505.x. [DOI] [PubMed] [Google Scholar]
- 70.Bronsard V, Paul C, Prey S, Puzenat E, Gourraud PA, Aractingi S, et al. What are the best outcome measures for assessing quality of life in plaque type psoriasis? A systematic review of the literature J Eur Aacd Dermatol Venereol. 2010;24:S17–22. doi: 10.1111/j.1468-3083.2009.03563.x. [DOI] [PubMed] [Google Scholar]