

Abstract
Congenital abnormalities of the optic disc are not so rare. The etiology for the most of them is unknown. Visual acuity of affected eye may be minimally or severely affected, depending on the extent of lesion. All of these conditions can be unilateral or bilateral. Chíldren who have unilateral optic disc abnormalities generally present during the preschool years with sensory esotropia. Visual acuity may be unaffected like in optic disc pit, optic disc drusen, fibre medullares, ect. However, during the evolution they may cause a decrease in visual acuity like serous retinal detachment in optic disc pit, atrophy or subretinal neovascularisation in optic disc drusen. Some of them like fibre medullares needs only a good diagnose and they do not have any evolution. Fluorescein angiography and ultrasonography may be crucial diagnostic procedures to discover some of them, like optic disc drusen. Optic disc abnormalities may be associated with other congenital disorders of the eye and often central nervous system malformations. Secondary they may be associated retinal detachment, retinochisis, macular edema, choroid neovascularisation and lipid exudation. Some of these conditions may be found on routine ophthalmologic exam such as optic disc drusen and fibre medullares and often are diagnostically problem.
The aim of our study was to present some of our cases with different optic disc abnormalities such as fibre medullares, optic disc coloboma, hypoplasio disci, optic disc drusen and optic disc pit.
Keywords: ischemic stroke, risk factors, sex
INTRODUCTION
The most of the congenital fundus abnormalities are caused by interruptions in the orderly development of the eye. The earliest recognizable structure associated with optic disc is primitive epithelial papilla. At or about the 17 mm stage, nerve fibers’ grow from the retinal ganglion cells thought the primitive epithelial papilla into the optic stalk, and the optic nerve is thus formed (1). Congenital abnormalities of the optic disc are not so rare. The etiology for the most of them is unknown. Visual acuity of affected eye may be minimally or severely affected, depending on the extent of lesion (2). They may be associated with other congenital disorders of the eye and often central nervous system malformations. Secondary they may be associated retinal detachment, retinochisis, macular edema, choroidal neovascularisation and lipid exudation (3, 4, and 5). Some of these conditions may be found on routine ophthalmologic exam such as optic disc drusen and fibre medullares and often are diagnostically problem. The aim of our study was to present different abnormalities of optic disc diagnostic approach and affection on visual acuity.
MATERIAL AND METHODS
During the period from 2006 until 2010, in 22 patients diagnosis of structural changes of optic disc has been made on department for retinal disorders and Children Ophthalmology on Eye Clinic Centre Niš, Serbia. Ophthalmologic exam of all patients obtained: visual acuity, biomicroscopy of anterior segment, applanation tonometry, indirect ophthalmoscopy, refractometry. Patients were examined in mydriasis. Visual acuity was taken by Snellen sings or in small children by pictures. All of them have been have been exam on fundus camera, and in all necessary cases the flourescein angiography has been obtain. Photo fundus images have been taken by digital fundus camera. In some cases for diagnostically verification of condition A and B scan ultrasonography. Visual field has been done in some cases also.
RESULTS
Between 22 examined patients, 11 were male and 11 female. The age, in the moment of diagnose, was between 3 years to 56 years of life. The time of diagnose dependent on visual acuity (Table 1.), type of structure changes of optic disc and extension of lesson. Optic disc pits are involved with retinal detachment and reduced visual acuity, in all patients with this anomaly (Table 1.) (Figure 1, 2). Morning glory syndrome and hypoplasio of optic disc is also followed with low visual acuity (Table 1.) (Figure 3, 4). While, patients with optic disc drusen and fibre medullares were with good visual acuity (Figure 5, 6). Visual acuity is depending on extent of lesion in patients with optic disc coloboma (Figure 7).
TABLE 1.
Visual acuity in patients with different optic disc abnormalities by Snellens chart

FIGURE 1.

Optic disc pit on both eyes
FIGURE 2.

Optic disc pit
a) optic disc pit
b) retinal detachment
FIGURE 3.

Morning glory syndrome
FIGURE 4.

Hypoplasio of optic disc
a) Colour photography of fundus
b) Golden ring sign
FIGURE 5.

Optic disc drusen
FIGURE 6.

Fibre medullares
a) Monocular involvement color fundus photography
b) Bilateral involvement color fundus photography
c) Bilateral involvement color fundus photography
d) and e) autofluorescence
FIGURE 7.

Optic disc Coloboma
a) optic disc coloboma
b) retinochoroidal coloboma
Optic disc pit was present on bout eyes in one patient (Figure 1). Bilateral involvement was also present in case of optic disc drusen in all diagnosed patients, as well as patients with fibrae medulares (Figure 1, 6b, 6c). Autofluorescence proved diagnose of optic disc drusen and fibre medullares (Figure 5 b, 6d, 6e). B scan ultrasonography detected small optic disc in patients with hypoplasio, as well as optic disc drusen, defect of the ocular bulb wall in patient with retinohoroidal coloboma and optic disc pit (Figure 8, 9, 10). Axial length was 17,8 mm in patient with hypoplasio of optic disc (Table 2).
FIGURE 8.

Ultrasound Β scan optic disc pit
FIGURE 9.

Ultrasound Β scan optic disc drusen
FIGURE 10.
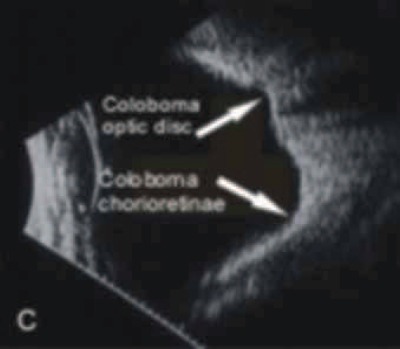
Ultrasound B.scan of optic disc coloboma and retinochoroidal coloboma
TABLE 2.
Axial lenght

DISCUSSION
Congenital abnormalities of the optic disc are not so rare. The etiology for the most of them is unknown. Visual acuity of affected eye may be minimally or severely affected, depending on the extent of lesion (1, 2, 3, 4).
All of these conditions can be unilateral or bilateral. They may be associated with other congenital disorders of the eye and often central nervous system malformations. Some of these conditions may be found on routine ophthalmologic exam such as optic disc drusen and fibre medullares and often are diagnostically problem. All optic disc abnormalities have their specific features as follows.
Optic disc pit
Congenital pits of the optic nerve head appear as a round or oval localized depressions within the optic disc. The condition is caused by an occlusion defect in the embryonic ventral fissure of the optic nerve (1, 5). Over one-half are positioned temporally on the nerve head, while about one-third are located more centrally on the disc(8,9). Optic pits range in size from 0,1 to 0,7 disc diameters along their widest dimensions and may be as deep as 25D, although the mean depth is about 5 D (4, 8). In colour, the pits may be grey (60%), yellow (30%), or black (10%). The border maybe rose as a result of pigment changes. The base of the pit may to pulsate. Bilateral involvement is seen in about 15% of patients (Figure 1). In those with unilateral pits, the optic disc itself is larger in the affected eye. There is usually one pit per optic disc although two or three occasionally occur (8). Petersen first realized the association between congenital optic pits and serous retinal detachment (7). The serous retinal detachment is usually confined to the macular region and rarely exceeds 1,5mm in height. About 40% of pits reported have been noted to have such a non-rhegmatogenous detachment. The great majority of detachments are seen in eyes with temporally located pits, and the mean age at onset is about 30 years (9). In about 25% of eyes with a detachment a lamellar or full-thickness macular hole will develop. Approximately one-third of these eyes have subretinal precipitates on the outer surface of the detached retina (5, 8). The etiology of the subretinal fluid is contra verse (5, 6, 7, 8).
Optic Disc Drusen
Drusen of the optic disc consist of hyaline bodies, are often partly calcified, and are located anterior to the lamina cribrosa. They develop due to an abnormal intracellular metabolism with calcification of the mitochondria (10). Drusen are bilateral in 69-73% of cases. They are probably already present at birth and are first clinically observed at the age of six (3). They may be associated with acqured diseases (hypertension, vessel occlusion, chorioretinitis) or with hereditary degenerative diseases (phacomatoses). Visual field defect are non-specific (Figure 11). Reduction of visual acuity as result of growth of the drusen, with pressure on the axons may occur (11). A narrow scleral canal, a prominent optic disc, and possibly dilatated capillaries are clinically visible. Hemorrhage on the edge of the optic disc occurs in 14% and shunt vessels in 7% of cases. Rarely, juxtapapillary subretinal hemorrhage occurs. The long-term prognosis is relatively good.
FIGURE 11.

Visual field Analyzer
Fibre Medullares
The condition is caused by myelinaed axons of the retinal ganglion cells in the optic nerve and and retina areas. Myelinisation occasionally extends past the lamina cribrosa along the nerve fibres of the optic nerve head and the sensory retina (12, 13). This development anomaly is found in less than 1%. It is bilateral in 20 % of cases, and the men are more often affected than women. In our patients, two were women and three men. The myelin sheaths surrounding the nerve fibres of the optic disc and retina have an opaque white appearance. Small areas of myelinated nerve fibres remote from optic disc are less frequent finding. The myelinated nerve fibres show discrete hypofluorescence due to blockage of choroidal fluorescence (13, 14, 15).
Hypoplasio
Typically, a hypoplastic optic disc appears small and pale. It is partially or totally surrounded by a yellow white ring that may be variably pigmented. Unilateral and bilateral involvement occurs with almost equal frequency (16). Visual acuity in involved eyes may range from normal to no light perception (Table 1). Strabismus is often seen in unilateral cases but in bilateral cases, eyes have a pendular nystagmus due to poor visual acuity. B -scan ultrasonography can demonstrate a small optic nerve. Systemic abnormalities associated with hypoplasia include anencephaly and hydranencephaly and an entity known as septo-optic dysplasia (De Morsier) (7). Some prenatal insults have been linked to optic disc hypoplasia development(17). In two of our patients maternal or gestation, diabetes was proved and in one infection of cytomegalovirus has been detected.
Optic disc coloboma
Colobomas are congenital or acquired notches, fissures, or defects that are found in the eye. Most commonly, they are congenital and occurs secondary to fautaly closure of the embryonic fissure. The optic nerve alone may be involved, or, more often, the anomaly may be of the retinochoroidal variety. Isolated optic disc coloboma appears as excavation within the nerve head and can range up to 25D in depth and 0,9 disc diameters across. They may be unilateral or bilateral. Visual acuity is minimally or severally affected, depending upon the extent of the lesion (18, 19). Retinochoroidal colobomas are glistering white or yellow defects with distinct borders that occurs inferior or inferonasal to the optic disc (Figure 5). Anteriorly, the defect can extend as far as the iris and produce an inferonasal gap. Colobomas may be associated with systemic abnormalities (18). Among the ocular abnormalities associated with colobomas is retinal detachment rhegmatogenous or non-rhegmatogenous. In our patients, coloboma of optic disc was present at the same time with retinal coloboma without affecting anterior segment. Ultrasound finding is presented as posterior staphyloma (B scan) (Figure 9.) and enlarged ocular bulb (A scan) (Table 2). No systemic abnormalities were detected.
Morning glory disc anomaly
The morning glory disc anomaly is a congenital excavation of the posterior globe that involves the optic disc. Embryological, morning glory disc anomaly may result from an anomalous; funnel shaped expansion of the disc portion of the optic stalk, which causes the opening of the lumen into the cavity of the optic vesicle to be abnormally large. The distal portion of the stalk does not obliterate the space within the fissure because of the increased dimensions of this space (5, 10, 19). The feature of morning glory disc anomaly is typically. An elevated annular zone surrounds the disc with irregular areas of pigmentation. A white tuft of glial tissue overlies the centre of the disc. The retinal blood vessels arise from the periphery of the disc (Figure 3).
CONCLUSION
Optic disc abnormalities are not rare condition.
All of these conditions can be unilateral or bilateral.
Visual acuity may be unaffected like in optic disc pit, optic disc drusen, fibre medullares, ect. But during the evolution they may cause a decision in visual acuity like serous retinal detachment in optic disc pit, atrophy or subretinal neovascularisation in optic disc drusen. Some of them like fibre medullares needs only a good diagnose and they do not have any evolution.
Fluorescein angiography and ultrasonography may be crucial diagnostic procedures to discover some of them.
It also should be aware that prolonged detachments of retina result in irreversible degenerative changes so laser or vitrectomy procedures should be considered.
REFERENCES
- 1.Azar N.F, Davis EA. Embryology of the eye. In: Yanoff M, Ducker JS, editors. Ophthalmology. second ed. Mosby; 2004. pp. 22–27. [Google Scholar]
- 2.Pulifiato C, Hee M, Schuman JS, Fujimoto JG. Diseases of Optic nerve in: Optical chocherence tomography of ocular diseases. Elsever; 2007. pp. 372–373. [Google Scholar]
- 3.Jandreck C. Optic nerve head anomalies. In: Heimann H, Kellner U, Foester HM, editors. Atlas of Fundus Angiography. Stuttgart. New York: Thieme; 2006. pp. 166–169. [Google Scholar]
- 4.Brodsky MC. Congenital optic Disc Anomalities. In: Yanoff M, Ducker JS, editors. Ophthalmology. second ed. Mosby; 2004. pp. 1255–1258. [Google Scholar]
- 5.Milenković S, Jaković N. Optic disc pit -Atipical optic disc coloboma. Medical Investigations. 2002;36(3):29–33. [Google Scholar]
- 6.Milenković S, Jaković N, Stefanović I. Subretinalna neovascularisation with optic disc drusen. Medical Investigations. 2002;36(1) 2:49–55. [Google Scholar]
- 7.Brown GC, Brown MM. Coexistent Optic Nerve and Macular Abnormalities. In: Yanoff M, Ducker JS, editors. Ophthalmology. second ed. Mosby; 2004. pp. 963–967. [Google Scholar]
- 8.Brown GS, Shieds JA, Goldberg RE. Congenital Pits of the Optic Nerve Head II. Clinical studies in humans. Ophthalmology. 1980;87:51–65. doi: 10.1016/s0161-6420(80)35278-0. [DOI] [PubMed] [Google Scholar]
- 9.Alimanović-Halilović E, Ibišević M. Congenital optic disc excavatio. Med. Arh. 2007;61(4):260–261. [PubMed] [Google Scholar]
- 10.Auw-Headrich C, Staubach F, Witchel H. Optic disc drusen. Surv. Ophtahalmol. 2002;47:515–532. doi: 10.1016/s0039-6257(02)00357-0. [DOI] [PubMed] [Google Scholar]
- 11.Lee AG, Zimmerman B. The rate of visual field loss in optic nerve head drusen. Am. J. Ophthalmol. 2005;139(6):1062–1066. doi: 10.1016/j.ajo.2005.01.020. [DOI] [PubMed] [Google Scholar]
- 12.Heimann H, Kellner U, Foester HM. Disorders of the Optic Nerve Head in Atlas of Fundus Angiography. Stuttgart, New York: Thieme; 2006. pp. 166–169. [Google Scholar]
- 13.Niemeijer M, Abramoff MD, Van Ginneken B. Fast detecting of the optic disc and fovea in color fundus photographs. Medical Imaging. 2009;28(5):775–785. doi: 10.1109/TMI.2008.2012029. [DOI] [PubMed] [Google Scholar]
- 14.Hornby SJ, Adolph S, Gilbert CE, Dandon CE, Foster A. Visual acuity in children with coloboma: clinical features and new phenotype classification system. Ophthalmology. 2000;107:511–520. doi: 10.1016/s0161-6420(99)00140-2. [DOI] [PubMed] [Google Scholar]
- 15.Moradian S, Karim S. Unilateral myelinated retinal nerve fiber layer associated with axial myopia, amblyopia and strabismus. J. Ophthal. Vision Res. 2009;4(4):264–265. [PMC free article] [PubMed] [Google Scholar]
- 16.May CR. Fibre Medullares in the Retina of the RD Mouse: A Case Report. Current Eye Research. 2009;34:411–413. doi: 10.1080/02713680902825507. [DOI] [PubMed] [Google Scholar]
- 17.Strömland K, Pinazo Duran MD. Ophthalmic Involvement in the Fetal Alcohol Syndrome: Clinical and Animal Model Studies. Alcohol & Alcoholism. 2002;37(1):2–8. doi: 10.1093/alcalc/37.1.2. [DOI] [PubMed] [Google Scholar]
- 18.Duton GN. Congenital disorders of the optic nerve: excavation and hypoplasia. Eye. 2004;18:1038–1048. doi: 10.1038/sj.eye.6701545. [DOI] [PubMed] [Google Scholar]
- 19.Presudovs K, Weisinger HS. Pseudoduolications of the optic nerve head. Optometry. 2000;71(9):586–590. [PubMed] [Google Scholar]