

Abstract
Hypothesis
Drilling on the incus produces intracochlear pressure changes comparable to pressures created by high-intensity acoustic stimuli.
Background
New-onset sensorineural hearing loss (SNHL) following mastoid surgery can occur secondary to inadvertent drilling on the ossicular chain. To investigate this, we test the hypothesis that high sound pressure levels are generated when a high-speed drill contacts the incus.
Methods
Human cadaveric heads underwent mastoidectomy, and fiber-optic sensors were placed in scala tympani and vestibuli to measure intracochlear pressures (PIC). Stapes velocities (Vstap) were measured using single-axis laser Doppler vibrometry. PIC and Vstap were measured while drilling on the incus. Four-millimeter diamond and cutting burrs were used at drill speeds of 20k, 50k, and 80k RPM.
Results
No differences in peak equivalent ear canal noise exposures (134–165 dB SPL) were seen between drill speeds or burr types. Root-mean-square PIC amplitude calculated in third-octave bandwidths around 0.5, 1, 2, 4, and 8 kHz revealed equivalent ear canal (EAC) pressures up to 110–112 dB SPL. A statistically significant trend toward increasing noise exposure with decreasing drill speed was seen. No significant differences were noted between burr types. Calculations of equivalent EAC pressure from Vstap were significantly higher at 101–116 dB SPL.
Conclusion
Our results suggest that incidental drilling on the ossicular chain can generate PIC comparable to high-intensity acoustic stimulation. Drill speed, but not burr type, significantly affected the magnitude of PIC. Inadvertent drilling on the ossicular chain produces intense cochlear stimulation that could cause SNHL.
Keywords: Acoustic trauma, iatrogenic hearing loss, ossicular chain, surgical drill, intracochlear pressures
Introduction
While a frequent aim of middle ear surgery is to preserve or restore normal hearing, one of the significant risks of these procedures is diminished cochlear sensitivity. New onset worsening of bone conduction thresholds on postoperative evaluation confirms sensorineural changes, and incidence of this type of loss has been estimated to occur in 1.2–4.5% of cases1–4. Several iatrogenic etiologies may result in acoustic trauma and contribute to postoperative hearing loss, including excessively forceful manipulation of the ossicular chain, development of perilymphatic fistula, drill-generated noise exposure, and incidental drilling on the ossicular chain5.
Studies of drill-generated noise from tympanomastoidectomy have documented widely varying levels of acoustic exposure, depending upon method of measurement. Sound level meter (SLM) estimates are as high as 118 dBA6, probe tube microphone measurements are recorded up to 131 dB SPL7, and calculations from accelerometer transfer functions estimate up to 105 dB SPL8. Though these estimates of noise level fall within the range for limiting exposure per Occupational Safety and Health Administration [OSHA] guidelines9, it remains unclear how much of the acoustic energy is transmitted to the cochlea. Some investigators have suggested that the energy transmitted is less than measured levels given lack of permanent injury to the contralateral cochlea with assumed negligible interaural attenuation10–14; however, this assumption does not take into account studies showing higher levels of intracranial attenuation15–17, which may suggest that the ipsilateral cochlea is potentially subject to higher, damaging noise levels.
Few studies have attempted to estimate noise exposure from incidental drill contact with the ossicular chain. Both case studies in human subjects and controlled experimentation in animals have demonstrated changes in hearing sensitivity after known incidental or intentional drilling on the ossicular chain, though the exact exposure levels are unknown in most cases18–23. Estimates determined from laser Doppler vibrometry (LDV) measurements on the stapes during drilling in cadaveric specimens suggest peak levels of 125 dB SPL, with the highest noise levels generated by larger diameter and cutting burrs24.
The published literature available provides only indirect estimation of cochlear exposure from drill noise via LDV measurements of stapes velocity24,25, accelerometer or record player pick-up8,21,26–28, or microphone/SLM measurements6,7,29–33. To the best of our knowledge, no direct characterization of cochlear exposure from incidental drilling on the ossicular chain with intracochlear pressure measurements has been made to date. To overcome this knowledge gap, here we investigate intracochlear pressure recordings in cadaveric human temporal bones made during intentional drilling on the incus.
Methods
Data was collected and analyzed from seven ears in fresh-frozen whole or hemi-sectioned cadaveric heads. All specimens were reported to have no known history of middle ear disease or surgery and confirmed to have intact temporal bones prior to investigation (M.D. Global, Aurora, CO, USA). The use of cadaveric human tissue was in compliance with the University of Colorado Anschutz Medical Campus Institutional Biosafety Committee and Review Board (COMIRB EXEMPT #14-1464).
Temporal Bone Preparation
Cadaveric specimens were prepared as previously described by our laboratory34–40, similar to methods employed by other groups41,42. Prior to surgical preparation, frozen cadaveric specimens were thawed and inspected to rule out temporal bone, external, or middle ear injury or disease. A canal-wall-up mastoidectomy with an extended facial recess approach was performed to allow access to the cochlea for placement of pressure probes. Preparation also included a wide exposure of the epitympanum to provide good visualization of the incus. The specimens were acoustically isolated from other testing equipment via suspension by a Mayfield Clamp (Integra Lifesciences Corp., Plainsboro, NJ, U.S.A.). The cochlear promontory was thinned near the oval and round windows, and cochleostomies into the scala tympani (ST) and scala vestibuli (SV) were created using a fine pick under a droplet of water. Fiber-optic pressure sensors (FOP-M260-ENCAP, FISO Inc., Quebec, QC, Canada) were inserted using micromanipulators (David Kopf Instruments, Trujunga, CA, U.S.A.) and sealed in place with alginate dental impression material (Jeltrate; Dentsply International Inc., York, PA, U.S.A.).
Drilling Noise Measurements
All experiments were performed in a double-walled sound-attenuating chamber (IAC Inc., Bronx, NY, U.S.A.). Prior to drilling on the ossicular chain, baseline measurements of intracochlear pressure and stapes velocity were made as an additional step in verification of normal middle ear function. One specimen was excluded due to abnormally high pressure in scala tympani, suggesting possible damage to the basilar membrane. Generation of sound stimuli and recording of responses was performed as described previously34–37. One-second tone pips ranging from 250–6000 Hz ramped on and off with one half (5 ms) of a Hanning window were presented to the specimens. Stimuli were digitally generated, driven by an external sound card (Hammerfall Multiface II, RME, Haimhausen, Germany), amplified with one channel of a stereo amplifier (TDT SA1), and presented via a closed-field magnetic speaker (MF1; Tucker-Davis Technologies Inc., Alachua, FL, U.S.A.) coupled to the ear canal with a foam earplug altered to accommodate flexible speaker and microphone tubing. The sound intensity in the ear canal was measured with a probe-tube microphone (type 4182; Bruel & Kjær, Nærum, Denmark).
Out-of-plane velocity of the stapes (VStap) was measured with a single-axis LDV (OFV-534 & OFV-5000; Polytec Inc., Irvine, CA) mounted to a dissecting microscope (Carl Zeiss AG, Oberkochen, Germany). Microscopic retro-reflective glass beads (P-RETRO 45–63 μm dia., Polytec Inc., Irvine, CA, U.S.A.) were placed on the stapes for measurement43,44.
For experimental measurements, a high-speed electric drill (Anspach EMAX2; DePuy Synthes, Solothurn, Switzerland) equipped with 4-mm burrs was used. The experimenter held the surgical drill in place, such that the edge of the burr maintained light contact with the body and short process of the incus for the duration of the recording. The drill was kept in place for 5–10 seconds, during which time intracochlear pressures (PIC) and VStap, were recorded. Both extra course diamond ball (S-4DX, DePuy Synthes, Solothurn, Switzerland) and cutting fluted ball (S-4B-G1, DePuy Synthes, Solothurn, Switzerland) burrs were used. The drill was operated at three speeds: 20kHz, 50 kHz, and 80kHz. The burrs and speeds were used in random order, varying between specimens, in order to counterbalance and unbias the experimental design.
Data Acquisition and Analysis
Input from the LDV and pressure sensors were simultaneously captured via the sound card analog inputs. The magnitude of the LDV signal was adjusted using a cosine correction (1/cos(θ)) based on an estimate of the difference in angle between the primary axis of the stapes and the orientation of the LDV laser (usually ~45°)44. Signals acquired were band-pass filtered between 15–15000 Hz with a second order Butterworth filter.
Baseline temporal bone measurements are shown as transfer functions, which consist of measured signal output normalized to sound pressure in the ear canal for each frequency, representing system gain. In order to estimate the SPL in the external auditory canal (EAC) that would have elicited an intracochlear pressure matching the measured pressure, we generated a 128-tap finite impulse response filter from the inverse of the mean acoustic transfer function for each signal observed previously in healthy human temporal bones36,41 using the Matlab function fir2. Both the raw pressure changes measured directly and the estimates of the equivalent ear canal SPL are valuable to consider; the raw pressures are the actual changes in fluid pressure observed during recordings and depict the real intracochlear fluid environment, while the estimated EAC pressures give the raw data context by describing the equivalent SPL of a sound in the EAC that would be required to generate a similar cochlear pressure response. Taken together, these measures are a useful means of quantifying cochlear pressures. Differential pressure (PDiff) is calculated as the difference in pressures between scala vestibuli and scala tympani and represents the driving force for auditory transduction. Responses were only analyzed for recordings with a signal to noise ratio greater than 6 dB, and SNR was higher than 10 dB for the majority of the recordings.
Noise level estimates from drilling on the incus were analyzed in two ways. To investigate maximum pressure exposure, the absolute peak pressures were found in each recording using the findpeaks function in Matlab (R2014b; The Mathworks, Inc., Natick, MA, U.S.A.). Peaks were only assessed if peaks occurred within 10 ms of one another in both scalae to avoid inclusion of artifacts. To investigate average noise levels across time and frequency, the mean pressure changes and stapes velocities were calculated as root-mean-square (RMS) averages in third-octave bandwidths around 500, 1000, 2000, 4000, and 8000 Hz.
Statistical analyses were completed using functions in the Statistics and Machine Learning toolbox in Matlab. Differences in pressures across drill type/speed and measurement locations (PSV, PST, or PDiff) were assessed with an n-way analysis of variance (ANOVA – the anovan function), and post hoc testing performed with a Tukey–Kramer HSD (honest significant difference) test (the multcompare function). Statistical comparisons are assessed at the α = 0.05 level unless otherwise specified.
Results
Acoustic Closed-field Transfer Functions
Stapes velocity (VStap) and intracochlear pressures (PIC) were assessed before drilling on the incus to verify the condition of each temporal bone. Closed-field acoustic transfer function magnitudes (HStap=VStap/PEAC, HSV=PSV/PEAC, HST=PST/PEAC, HDiff=PDiff/PEAC) for the six included specimens are shown in Figure 1. Responses were overlain onto the 95% CI for HStap44, and the mean standard deviation of responses observed for HSV and HST reported previously by Nakajima et al41. Responses collected from the presented specimens were consistent with previous reports34–37.
Figure 1.

Baseline VStap, PSV, PST, and PDiff transfer function magnitudes to air conducted stimuli. Response magnitudes recorded from six specimens are shown normalized to the SPL recorded in the ear canal (PEAC). Responses are superimposed onto the 95% CI and range of responses (gray bands) observed previously41,44.
Estimated Equivalent Pressure Induced by Drilling on the Incus
An example of the data recorded while drilling on the ossicular chain are shown in Figure 2, with stapes velocities (VStap) and intracochlear pressures (PSV, PST, and PDiff) shown in the tracings from top to bottom. The intracochlear pressures can be directly related to sound pressure in the ear canal via the acoustic transfer function. Figure 3A illustrates how the transfer function is derived for pressures in each scala; after an intracochlear response is measured for a known stimulus, the gain in cochlear pressure relative to the EAC pressure at each frequency generates the transfer function for the respective scala. The transfer functions are subsequently used to generate scala-specific filters that can be used to estimate an equivalent ear canal SPL based on the scala pressure, as illustrated in Figure 3B. Results for this analysis are similar to previous observations35. The estimated EAC SPL results in little difference between raw pressures and estimated EAC SPL for PST (due to low gain from the PST/PEAC transfer function) and lower estimated EAC SPL in PSV and PDiff (due to the ear canal resonance and middle ear gain observable in the PSV/PEAC and PDiff/PEAC transfer functions).
Figure 2.

Example recording during drilling on the incus in a single specimen. VStap, PSV, PST, and PDiff shown in the tracings from top to bottom, with amplitudes autoscaled to the figure to facilitate visual comparison between channels.
Figure 3.

Schematic of methods for deriving estimated equivalent ear canal pressure from intracochlear pressures. Intracochlear pressures resulting from acoustic pure-tone stimulation are compared with measured sound pressures in the ear canal to calculate scala-specific transfer functions (A). A 128-tap finite impulse response filter is derived from this transfer function and used to estimate equivalent ear canal pressure for any arbitrary intracochlear pressures measured while drilling on the incus (B).
Prior to drilling on the incus, a recording was made in each specimen while the drill was running and sitting inside the mastoid cavity but without contacting the ossicles or surrounding bone. These measurements showed a raw RMS pressure of between 0.126–0.399 Pa, which corresponded to an equivalent ear canal pressure of 70–76 dB SPL.
Peak Pressures Induced by Drilling on the Incus
Figure 4 shows a summary of the absolute maximum peak pressures observed in all recordings in all specimens, in all drilling conditions tested. Figure 4A shows the unfiltered recorded raw pressures while the maximum peak pressures in estimated EAC SPL are illustrated in Figure 4B. Estimated EAC pressures recorded during drilling on the incus ranged from 134–165 dB SPL – levels comparable in magnitude to high intensity acoustic stimuli.
Figure 4.

Summary of peak sound pressure levels observed in all specimens during all drilling conditions. Unfiltered peak intracochlear pressure measurements (A) and estimated EAC pressures (B) are shown for each pressure recording as a function of drilling condition. Box plots represent the median +/−25% of the range of pressures observed, whiskers show the full range of the estimated distribution, and +’s mark outliers.
Peak pressures served as the dependent variable and drilling conditions (drill speed and burr type) acted as independent variables for a two-way ANOVA for both unfiltered and estimated EAC SPL conditions. No significant differences were noted in either peak raw pressures or estimated EAC pressures for burr type or drill speed (F<0.6, p>0.6). A one-way ANOVA across stimulus conditions revealed a significant effect of pressure probe location (scala vestibuli, scala tympani, or differential pressure) in both raw (F=7.22, p=0.0013) and estimated EAC (F=30.74, p≪0.0001) pressures. Post hoc Tukey honest significant difference (hsd) pairwise comparisons showed significantly higher pressure in scala vestibuli than both scala tympani (p≪0.0001) and differential pressure (p≪0.0001) in raw pressure data and higher pressure in scala tympani than both scala vestibuli (p≪0.0001) and differential pressure (p≪0.0001) in estimated equivalent EAC pressures.
Average Pressures Induced by Drilling on the Incus
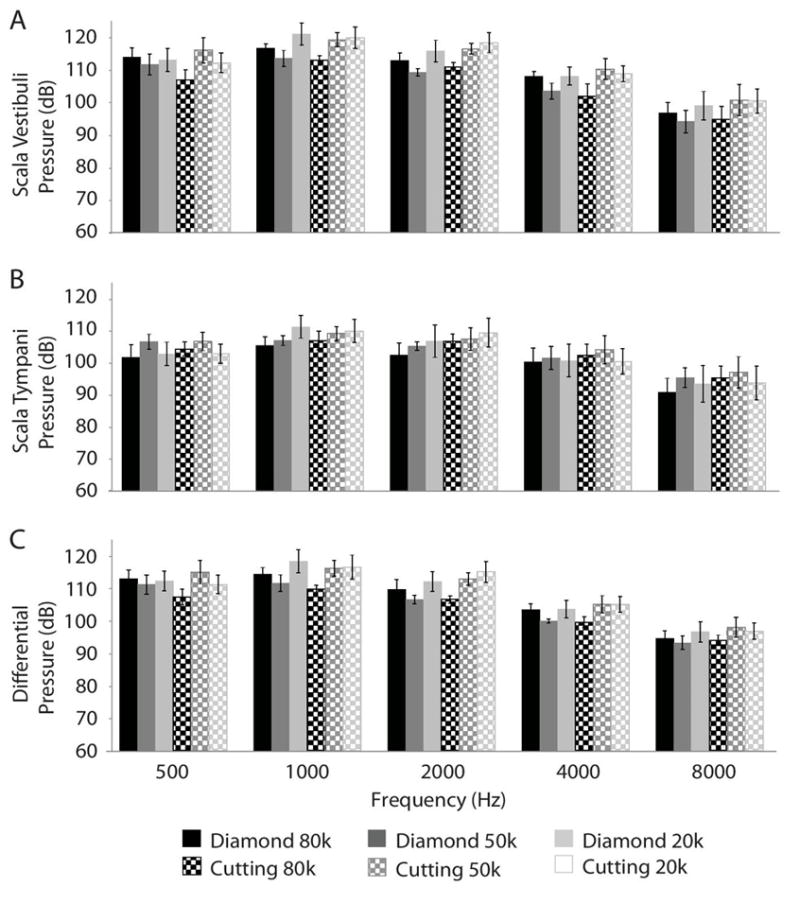
Figure 5 summarizes average pressure calculations for PSV, PST, and PDiff in raw pressure data, and Figure 6 summarizes PSV, PST, PDiff, and VStap in estimated equivalent SPL. Grey bars show the mean noise exposure for each corresponding drill speed and burr type combination in PSV (5A and 6A), PST (5B and 6B), PDiff (5C and 6C), and VStap (6D), with solid bars indicating use of the diamond burr, checkered bars indicating the cutting burr, and increasing dark shade corresponding with increasing drill speed. Error bars indicate the standard error of the mean (SEM) for each data set.
Figure 5.
Average equivalent noise in raw pressure for all specimens by drilling conditions. Mean PIC and VStap were calculated as root-mean-square (RMS) averages in third-octave bandwidths around 500, 1000, 2000, 4000, and 8000 Hz. Grey bars show the mean noise exposure for each corresponding drill speed and burr type combination in PSV (5A), PST (5B), and PDiff (5C), with solid bars indicating use of the diamond burr, checkered bars indicating the cutting burr, and increasing dark shade corresponding with increasing drill speed. Error bars indicate the SEM for each data set.
Figure 6.

Average equivalent noise in estimated ear canal sound pressures level (dB SPL Eq) for all specimens by drilling conditions. Mean PIC and VStap were calculated as root-mean-square (RMS) averages in third-octave bandwidths around 500, 1000, 2000, 4000, and 8000 Hz. Grey bars show the mean noise exposure for each corresponding drill speed and burr type combination in PSV (6A), PST (6B), PDiff (6C), and VStap (6D), with solid bars indicating use of the diamond burr, checkered bars indicating the cutting burr, and increasing dark shade corresponding with increasing drill speed. Error bars indicate the SEM for each data set.
Several trends are immediately apparent in the dataset. Equivalent ear canal pressure calculated from stapes velocity transfer function is estimated to be about 10–15 dB higher than corresponding estimates from PIC transfer functions. There does not appear to be difference in average pressure across frequency by burr type, though there appears to be a trend towards increasing pressure with decreasing drill speed.
A three-way ANOVA was performed with mean pressure as the dependent variable, and burr type, drill speed, and frequency as independent variables in both unfiltered pressures and estimated EAC SPL. For the raw pressures, results reveal a main effect of frequency (F=63.55; p≪0.0001), drill speed (F=5.21; p=0.0058) and the interaction between drill speed and burr type (F=4.79, p=0.0087), but not burr type (F=1.76; p=0.1858), nor the remaining interactions (Freq*Type: F=0.5, p=0.7377; Freq*Speed: F=0.72, p=0.6783). Table 1 contains post hoc Tukey hsd pairwise comparisons for RMS raw pressure by frequency pairs. Additionally, hsd showed significantly lower raw pressure with a drill speed of 80kHz compared with 20kHz (p=0.0039).
Table 1.
Posthoc Tukey honest-significant difference (hsd) pairwaise comparisons for RMS raw pressure by frequency pairs
| Frequency | Frequency | Lower limit 95% CI for true mean difference | Difference between estimated group means | Upper limit 95% CI for true mean difference | p-value |
|---|---|---|---|---|---|
| 500 | 1000 | −7.3223 | −3.9765 | −0.6307 | 0.0104* |
| 500 | 2000 | −4.2262 | −0.8804 | 2.4653 | 0.9525 |
| 500 | 4000 | 2.3148 | 5.6605 | 9.0063 | ≪0.0001* |
| 500 | 8000 | 10.2132 | 13.5590 | 16.9047 | ≪0.0001* |
| 1000 | 2000 | −0.2497 | 3.0961 | 6.4418 | 0.0853 |
| 1000 | 4000 | 6.2913 | 9.6370 | 12.9828 | ≪0.0001* |
| 1000 | 8000 | 14.1897 | 17.5355 | 20.8812 | ≪0.0001* |
| 2000 | 4000 | 3.1952 | 6.5409 | 9.8867 | ≪0.0001* |
| 2000 | 8000 | 11.0936 | 14.4394 | 17.7852 | ≪0.0001* |
| 4000 | 8000 | 4.5527 | 7.8985 | 11.2442 | ≪0.0001* |
For the estimated EAC SPL, results also reveal a main effect of frequency (F=9.07; p≪0.0001), drill speed (F=6.13; p=0.0023) and the interaction between drill speed and burr type (F=8.69, p=0.0002), but neither burr type (F=1.03; p=0.3099) nor the remaining interactions (F<.75, p>0.6). Post hoc Tukey hsd pairwise comparisons for frequency are shown in Table 2. Additionally, Pot hoc Tukey hsd showed significantly lower raw pressure with a drill speed of 80kHz compared with 20kHz (p=0.0014).
Table 2.
Posthoc Tukey honest-significant difference (hsd) pairwaise comparisons for RMS estimated ear canal pressure by frequency pairs
| Frequency | Frequency | Lower limit 95% CI for true mean difference | Difference between estimated group means | Upper limit 95% CI for true mean difference | p-value |
|---|---|---|---|---|---|
| 500 | 1000 | −3.8072 | −0.6745 | 2.4581 | 0.9770 |
| 500 | 2000 | −0.6059 | 2.5268 | 5.6595 | 0.1795 |
| 500 | 4000 | −0.6718 | 2.4609 | 5.5936 | 0.2020 |
| 500 | 8000 | 2.6012 | 5.7339 | 8.8666 | ≪0.0001* |
| 1000 | 2000 | 0.0687 | 3.2013 | 6.3340 | 0.0423* |
| 1000 | 4000 | 0.0028 | 3.1354 | 6.2681 | 0.0497* |
| 1000 | 8000 | 3.2758 | 6.4085 | 9.5411 | ≪0.0001* |
| 2000 | 4000 | −3.1986 | −0.0659 | 3.0668 | 1.0000 |
| 2000 | 8000 | 0.0744 | 3.2071 | 6.3398 | 0.0417* |
| 4000 | 8000 | 0.1403 | 3.2730 | 6.4057 | 0.0354* |
A one-way ANOVA across stimulus conditions revealed a significant effect of pressure probe location in both raw (F=22.99, p≪0.0001) and estimated EAC (F=67.15, p≪0.0001) pressures. Post hoc Tukey hsd pairwise comparisons showed significantly lower pressure in scala tympani than both scala vestibuli (p≪0.0001) and stapes velocity (p≪0.0001) and significantly higher pressure in scala vestibuli than differential pressure (p=0.0498) in raw pressure data and significantly higher pressure in stapes velocities than scala tympani (p=0.0135) scala vestibuli (p≪0.0001), and differential pressure (p≪0.0001) in estimated equivalent EAC pressures. For EAC SPL, scala tympani estimates were also significantly higher than both scala vestibuli (p≪0.0001) and differential pressure (p≪0.0001).
Discussion
Our results suggest that incidental drilling on the ossicular chain can generate intracochlear pressures comparable to high-intensity acoustic stimulation. Estimated peak equivalent ear canal pressure ranged from 134 to 165 dB SPL, with no difference in pressure noted between burr type or drill speed. Average PIC amplitude revealed equivalent EAC pressures up to 115 dB SPL, with significantly higher noise exposures associated with lower drill speeds. While there was a significant effect of the interaction between burr type and drill speed, there was no significant independent effect of burr type on noise exposure estimates.
Our data also demonstrated decreasing RMS energy with increasing frequency of drill-induced pressure changes. Though few studies have examined the effect of frequency content of noise on hearing loss45, it has been demonstrated that temporary threshold shifts increase with increased exposure frequency up to 2–6 kHz46,47. The lower high-frequency content of noise from drilling seen in our data suggest that the effect on hearing loss may be less than for noises with containing predominantly higher frequencies, though this would be difficult to predict.
To the best of our knowledge, no previous reports of intracochlear pressures measured during manipulation of the ossicular chain exist; however, a number of studies have used other indirect techniques to estimate cochlear noise exposure from incidental drill contact with the ossicular chain.
Stapes displacements characterized by laser Doppler vibrometry have been used to estimate equivalent noise exposure levels resulting from drilling on the incus short process. The equivalent noise levels generated ranged from 93 to 125 dB SPL, with cutting burrs generating more noise than size-matched diamond burrs and increasing energy with increasing frequency24. Prior to availability of LDV technology, one investigation employed a magnetic pick-up from a record player positioned on the inner surface of the stapes footplate to characterize displacement resulting from drilling on various locations along the ossicular chain. Transfer functions determined from prior measures of footplate displacement estimated noise levels to be over 130 dB SPL21.
Animal studies have confirmed that iatrogenic drilling on the ossicular chain can cause changes in cochlear sensitivity. In one investigation, guinea pigs underwent drill-induced injury to the body of the incus, which resulted in an immediate threshold shift in electrocochleography20. In another study, bone-conducted signals were used to elicit intraoperative electrocochleography (ECoG) in guinea pigs immediately after drilling on the incudomalleal complex. Several animals demonstrated significant post-manipulation threshold shifts18.
Several variables have been found to affect drill-generated noise levels in ear surgery. Regardless of methods used for estimation, noise levels have been shown to be higher with larger sized burrs24,27. The relationship between drill speed and noise exposure has been harder to characterize and no reliable pattern has been identified27, though our results suggest that lower speeds result in increased noise exposure. Most studies conclude that more noise is generated by cutting burrs than diamond burrs21,24,27,29,30; however, in contrast to expectation, not all studies have found an effect of burr type7, and results presented here contrast with the literature. While a cutting burr held firmly against the incus has the potential to generate large displacements as the flute edge hits against the bone, a lighter contact may generate smaller intermittent peaks in PIC, as seen in one study utilizing SLM to characterize drill noise29. The diamond drill with its irregular but comparatively flatter surface may generate a more constant change in PIC, potentially resulting in higher average noise exposures compared with the cutting burr when the drill is held in lighter contact with the incus.
Estimation of Equivalent Noise Exposure
The body of literature that attempts to quantify cochlear noise exposure from manipulation of the ossicular chain relies on acoustic transfer functions in order to estimate equivalent ear canal sound pressure levels. Transfer functions are generated by measuring the response of a system to a known stimulus; in this case, we use acoustic stimuli and characterize the response of the external, middle, and inner ears utilizing intracochlear pressure. We are then able to use the resulting transfer function to essentially reverse calculate an estimate of the intensity of acoustic stimulus that would be required to generate a given pressure measurement. While this method provides an estimate of the acoustic stimulus that would be required to elicit a similar response in both PIC and VStap, the estimate will always be somewhat inaccurate as manipulating the ossicular chain is a fundamentally different mode of providing input energy to the cochlea.
As mentioned above, the acoustic transfer function may fail to account for any additional energy transfer that may result from a non-acoustic energy source. The surgical drill may provide additional stimulation via bone conduction from drilling on other areas of the temporal bone, such as the attic or incus buttress. The drill also generates acoustic energy that may be propagated via air conduction through the middle ear and result in direct stimulation of the round window, potentially explaining higher PST than expected from acoustic stimulation alone. Additionally, the well-described vibrational modes of the stapes footplate to air-conducted stimuli48 may be altered by direct mechanical stimulation, possibly resulting in frequency-dependent variation in cochlear input energy. Furthermore, a single-axis LDV measurement cannot capture these complex stapes vibration modes, particularly for non piston-like and rocking motion known to occur at higher frequencies41,48, thus potentially underestimating the effective input to the cochlea. Stapes velocity measured at a single point, as in our experiments, do not account for these different sources of energy transfer. Contrastingly, higher than expected estimates derived from LDV measurements are also possible. Direct manipulation of the ossicular chain may result in large changes to stapes motion, but all of this energy may not be directly transferred to the cochlea given the abnormal axis of motion resulting from this method of stimulation. This could result in larger than expected estimates derived from laser Doppler measurements of stapes displacement during the direct manipulation of the ossicular chain, which may explain the difference between exposure estimates derived from stapes velocities and those calculated from intracochlear pressures.
The higher EAC SPL estimates of drill noise from the VStap measurements relative to the somewhat smaller EAC estimates based on cochlear pressure measurements in our data is consistent with this. The difference in stimulus type may account for the discrepancy noted between estimates of ear canal pressure derived from PIC and LDV measurements, as well as slightly higher than expected equivalent pressure calculated from PST. These facts present a challenge to the interpretation of data, as we cannot describe how any additional input sources affect the magnitude of the individual cochlear pressures or the driving pressure. Thus, data presented here should be interpreted with caution, as we may potentially be under- or over-estimating the equivalent noise exposures.
Mechanism of Damage from Ultrasonic Noise Exposure
Another issue to consider is the mechanism for energy transfer when utilizing high-speed drills to stimulate the inner ear. The lowest settings in most operative drills are 10–20 kHz, which represents the very upper range of acoustic sensitivity for humans, and higher speeds peak near 80 kHz, which is well above the limit for audibility. Exposure to ultrasonic noise has been documented as a risk factor for development of high frequency sensorineural hearing loss49,50. Lower frequency energy is likely transmitted in subharmonic distortions as evidenced by the high level of energy measured at the standard audiometric frequencies in this study. Exposure to signals including both audible high frequency and ultrasonic stimuli may create an overlap of energy in the inner ear, potentiating the damage of high intensity exposure of either stimulus alone50.
Limitations
Despite the fact that this investigation represents the first description of intracochlear pressure changes resulting from manipulation of the ossicular chain, several limitations in our methodology limit the ability to generalize results from this study. Although full cephali represent a more complete model than isolated temporal bones, we recognize that cadaveric specimen may be subject to post-mortem degradation. Homeostatic regulation of intracochlear pressure via the cochlear aqueduct is not possible and pressure changes from physiologic baseline cannot be verified. Additionally, we chose to run the otologic drill in the hands of the researcher, rather than suspended or fixed externally. While we prefer this method for its closer approximation of “real-world” exposure, we appreciate that this provides a source of additional variability to our dataset.
Conclusions
Incidental drilling on the ossicular chain during middle ear surgery is known to have the potential to cause sensorineural hearing loss. Data presented here have demonstrated that pressure changes in the cochlea resulting from drilling on the incus may be of sufficiently high amplitude to cause cochlear injury. Our data contrast with previous studies suggesting that cutting burrs generate higher levels of exposure than diamond burrs and may suggest an inverse relationship between drill speed and noise exposure, though additional data is needed to further investigate this association. Given the risk for iatrogenic acoustic trauma from inadvertent manipulation of the ossicular chain, this study underscores the importance of avoiding contact of the surgical drill with the ossicular chain in temporal bone surgery.
Acknowledgments
Funding:
RMBH was funded by NIH NIDCD T32 DC-012280.
Footnotes
Conflict of Interest Statement:
No potential conflict of interest was reported by the authors.
References
- 1.Tos M, Lau T, Plate S. Sensorineural hearing loss following chronic ear surgery. Ann Otol Rhinol Laryngol. 1984;93(4 Pt 1):403–409. doi: 10.1177/000348948409300424. [DOI] [PubMed] [Google Scholar]
- 2.Smyth G. Sensorineural hearing loss in chronic ear surgery. Ann Otol. 1977;86:3–8. doi: 10.1177/000348947708600102. [DOI] [PubMed] [Google Scholar]
- 3.Palva T, Kärjä J, Palva A. Immediate and short-term complications of chronic ear surgery. Arch Otolaryngol. 1976;102(3):137–139. doi: 10.1001/archotol.1976.00780080059004. [DOI] [PubMed] [Google Scholar]
- 4.Palva T, Kärjä J, Palva A. High-tone sensorineural losses following chronic ear surgery. Arch Otolaryngol. 1973;98(3):176–178. doi: 10.1001/archotol.1973.00780020184008. [DOI] [PubMed] [Google Scholar]
- 5.Schick B, Dlugaiczyk J. Surgery of the ear and the lateral skull base: pitfalls and complications. GMS Curr Top Otorhinolaryngol Head Neck Surg. 2013;12:Doc05. doi: 10.3205/cto000097. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Michaelides EM, Kartush JM. Implications of sound levels generated by otologic devices. Otolaryngol Head Neck Surg. 2001;125:361–363. doi: 10.1067/mhn.2001.118956. [DOI] [PubMed] [Google Scholar]
- 7.Yin X, Strömberg A-K, Duan M. Evaluation of the noise generated by otological electrical drills and suction during cadaver surgery. Acta Otolaryngol. 2011;131(11):1132–1135. doi: 10.3109/00016489.2011.600725. [DOI] [PubMed] [Google Scholar]
- 8.Kylén P, Arlinger S. Drill-generated noise levels in ear surgery. Acta Otolaryngol. 1976;82(5–6):402–409. doi: 10.3109/00016487609120925. [DOI] [PubMed] [Google Scholar]
- 9.Occuptional Safety Health Administration OSHA. Occupational Noise Exposure. 1926.52. :2105. https://www.osha.gov/pls/oshaweb.
- 10.Abtahi SH, Fazel A, Rogha M, Nilforoush M, Solooki R. Effect of drill-induced noise on hearing in non-operated ear. Adv Biomed Res. 2016;5(1):87. doi: 10.4103/2277-9175.182218. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Baradaranfar MH, Shahbazian H, Behniafard N, et al. The effect of drill-generated noise in the contralateral healthy ear following mastoid surgery: The emphasis on hearing threshold recovery time. Noise Health. 2015;17(77):209–215. doi: 10.4103/1463-1741.160691. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.da Cruz MJ, Fagan P, Atlas M, McNeill C. Drill-induced hearing loss in the nonoperated ear. Otolaryngol Head Neck Surg. 1997;117(5):555–558. doi: 10.1016/s0194-5998(97)70030-5. [DOI] [PubMed] [Google Scholar]
- 13.Man A, Winerman I. Does drill noise during mastoid surgery affect the contralateral ear? Am J Otol. 1985;6(4):334–335. [PubMed] [Google Scholar]
- 14.Shenoy VS, Vanka S, Rao RA, Prasad V, Kamath PM, Bhat J. Effect of mastoid drilling on the distortion product otoacoustic emissions in the non operated ear. Am J Otolaryngol. 2015;36(6):832–836. doi: 10.1016/j.amjoto.2015.07.013. [DOI] [PubMed] [Google Scholar]
- 15.Reinfeldt S, Stenfelt S, Håkansson B. Estimation of bone conduction skull transmission by hearing thresholds and ear-canal sound pressure. Hearing Research. 2013;299:19–28. doi: 10.1016/j.heares.2013.01.023. [DOI] [PubMed] [Google Scholar]
- 16.Snapp HA, Morgenstein KE, Telischi FF, Angeli S. Transcranial Attenuation in Patients with Single-Sided Deafness. Audiol Neurootol. 2016;21(4):237–243. doi: 10.1159/000447044. [DOI] [PubMed] [Google Scholar]
- 17.Stenfelt S. Transcranial attenuation of bone-conducted sound when stimulation is at the mastoid and at the bone conduction hearing aid position. Otol Neurotol. 2012;33(2):105–114. doi: 10.1097/MAO.0b013e31823e28ab. [DOI] [PubMed] [Google Scholar]
- 18.Bergin MJ, Bird PA, Vlajkovic SM, Thorne PR. High frequency bone conduction auditory evoked potentials in the guinea pig: Assessing cochlear injury after ossicular chain manipulation. Hearing Research. 2015;330(Part A):147–154. doi: 10.1016/j.heares.2015.10.009. [DOI] [PubMed] [Google Scholar]
- 19.El-Hennawi DM, El-Deen MHB, Abou-Halawa AS, Nadeem HS, Ahmed MR. Efficacy of intratympanic methylprednisolone acetate in treatment of drill-induced sensorineural hearing loss in guinea pigs. J Laryngol Otol. 2005;119(1):2–7. doi: 10.1258/0022215053222815. [DOI] [PubMed] [Google Scholar]
- 20.Gjuric M, Schneider W, Buhr W, Wolf SR, Wigand ME. Experimental sensorineural hearing loss following drill-induced ossicular chain injury. Acta Otolaryngol. 1997;117(4):497–500. doi: 10.3109/00016489709113427. [DOI] [PubMed] [Google Scholar]
- 21.Helms J. Acoustic trauma from the bone cutting burr. J Laryngol Otol. 1976;90(12):1143–1149. doi: 10.1017/s0022215100083225. [DOI] [PubMed] [Google Scholar]
- 22.Schuknecht HF, Tonndorf J. Acoustic trauma of the cochlea from ear surgery. The Laryngoscope. 1960;70:479–505. doi: 10.1288/00005537-196004000-00011. [DOI] [PubMed] [Google Scholar]
- 23.Schneider W, Gjuric M, Katalinic A, Buhr W, Wolf SR. The value of methylprednisolone in the treatment of an experimental sensorineural hearing loss following drill-induced ossicular chain injury: a randomized, blinded study in guinea-pigs. Acta Otolaryngol. 1998;118(1):52–55. doi: 10.1080/00016489850155125. [DOI] [PubMed] [Google Scholar]
- 24.Jiang D, Bibas A, Santuli C, Donnelly N, Jeronimidis G, O’Connor AF. Equivalent noise level generated by drilling onto the ossicular chain as measured by laser Doppler vibrometry: a temporal bone study. The Laryngoscope. 2007;117(6):1040–1045. doi: 10.1097/MLG.0b013e3180459a10. [DOI] [PubMed] [Google Scholar]
- 25.Eze N, Jiang D, Fitzgerald O’Connor A. Inner ear energy exposure while drilling a cochleostomy. Acta Otolaryngol. 2014;134(11):1109–1113. doi: 10.3109/00016489.2014.914245. [DOI] [PubMed] [Google Scholar]
- 26.Hilmi OJ, Mckee RH, Abel EW, Spielmann PM, Hussain SSM. Do high-speed drills generate high-frequency noise in mastoid surgery? Otol Neurotol. 2012;33(1):2–5. doi: 10.1097/MAO.0b013e31823c8f0d. [DOI] [PubMed] [Google Scholar]
- 27.Kylén P, Stjernvall JE, Arlinger S. Variables affecting the drill-generated noise levels in ear surgery. Acta Otolaryngol. 1977;84(3–4):252–259. doi: 10.3109/00016487709123964. [DOI] [PubMed] [Google Scholar]
- 28.Paulsen K, Vietor K. Measurement of sound transmitted through the body while drilling and grinding isolated petrous temporal bone (author’s transl) Arch Otorhinolaryngol. 1975;209(3):159–168. doi: 10.1007/BF00453771. [DOI] [PubMed] [Google Scholar]
- 29.Dalchow CV, Hagemeier KC, Muenscher A, Knecht R, Kameier F. Investigation of noise levels generated by otologic drills. Eur Arch Otorhinolaryngol. 2013;270(2):505–510. doi: 10.1007/s00405-012-2012-9. [DOI] [PubMed] [Google Scholar]
- 30.Parkin JL, Wood GS, Wood RD, McCandless GA. Drill- and suction-generated noise in mastoid surgery. Arch Otolaryngol. 1980;106(2):92–96. doi: 10.1001/archotol.1980.00790260024008. [DOI] [PubMed] [Google Scholar]
- 31.Pau HW, Just T, Bornitz M, Lasurashvilli N, Zahnert T. Noise exposure of the inner ear during drilling a cochleostomy for cochlear implantation. The Laryngoscope. 2007;117(3):535–540. doi: 10.1097/MLG.0b013e31802f4169. [DOI] [PubMed] [Google Scholar]
- 32.Shine NP, O’Sullivan PG, Connell J, Rulikowski P, Barrett J. Digital spectral analysis of the drill-bone acoustic interface during temporal bone dissection: a qualitative cadaveric pilot study. Otol Neurotol. 2006;27(5):728–733. doi: 10.1097/01.mao.0000226295.34542.07. [DOI] [PubMed] [Google Scholar]
- 33.Yu H, Tong B, Zhang Q, Zhu W, Duan M. Drill-induced noise level during cochleostomy. Acta Otolaryngol. 2014;134(9):000–000. doi: 10.3109/00016489.2014.927591. [DOI] [PubMed] [Google Scholar]
- 34.Banakis Hartl RM, Mattingly JK, Greene NT, Jenkins HA, Cass SP, Tollin DJ. A Preliminary Investigation of the Air-Bone Gap: Changes in Intracochlear Sound Pressure With Air- and Bone-conducted Stimuli After Cochlear Implantation. Otol Neurotol. 2016;37(9):1291–1299. doi: 10.1097/MAO.0000000000001184. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.Greene NT, Mattingly JK, Banakis Hartl RM, Tollin DJ, Cass SP. Intracochlear Pressure Transients During Cochlear Implant Electrode Insertion. Otol Neurotol. 2016;37:1541–1548. doi: 10.1097/MAO.0000000000001232. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36.Greene NT, Mattingly JK, Jenkins HA, Tollin DJ, Easter JR, Cass SP. Cochlear Implant Electrode Effect on Sound Energy Transfer Within the Cochlea During Acoustic Stimulation. Otol Neurotol. 2015;36(9):1554–1561. doi: 10.1097/MAO.0000000000000838. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37.Mattingly JK, Greene NT, Jenkins HA, Tollin DJ, Easter JR, Cass SP. Effects of Skin Thickness on Cochlear Input Signal Using Transcutaneous Bone Conduction Implants. Otol Neurotol. 2015;36(8):1403–1411. doi: 10.1097/MAO.0000000000000814. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 38.Deveze A, Koka K, Tringali S, Jenkins HA, Tollin DJ. Techniques to improve the efficiency of a middle ear implant: effect of different methods of coupling to the ossicular chain. Otol Neurotol. 2013;34(1):158–166. doi: 10.1097/MAO.0b013e3182785261. [DOI] [PubMed] [Google Scholar]
- 39.Deveze A, Koka K, Tringali S, Jenkins HA, Tollin DJ. Active middle ear implant application in case of stapes fixation: a temporal bone study. Otol Neurotol. 2010;31(7):1027–1034. doi: 10.1097/MAO.0b013e3181edb6d1. [DOI] [PubMed] [Google Scholar]
- 40.Tringali S, Koka K, Deveze A, Holland NJ, Jenkins HA, Tollin DJ. Round window membrane implantation with an active middle ear implant: a study of the effects on the performance of round window exposure and transducer tip diameter in human cadaveric temporal bones. Audiol Neurootol. 2010;15(5):291–302. doi: 10.1159/000283006. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 41.Nakajima HH, Dong W, Olson ES, Merchant SN, Ravicz ME, Rosowski JJ. Differential intracochlear sound pressure measurements in normal human temporal bones. J Assoc Res Otolaryngol. 2009;10(1):23–36. doi: 10.1007/s10162-008-0150-y. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 42.Olson ES. Observing middle and inner ear mechanics with novel intracochlear pressure sensors. J Acoust Soc Am. 1998;103(6):3445–3463. doi: 10.1121/1.423083. [DOI] [PubMed] [Google Scholar]
- 43.Stenfelt S, Goode RL. Transmission properties of bone conducted sound: measurements in cadaver heads. J Acoust Soc Am. 2005;118(4):2373–2391. doi: 10.1121/1.2005847. [DOI] [PubMed] [Google Scholar]
- 44.Rosowski JJ, Chien W, Ravicz ME, Merchant SN. Testing a method for quantifying the output of implantable middle ear hearing devices. Audiol Neurootol. 2007;12(4):265–276. doi: 10.1159/000101474. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 45.Mahendra Prashanth KV, Venugopalachar S. The possible influence of noise frequency components on the health of exposed industrial workers--a review. Noise Health. 2011;13(50):16–25. doi: 10.4103/1463-1741.73996. [DOI] [PubMed] [Google Scholar]
- 46.Miller JD. Effects of noise on people. J Acoust Soc Am. 1974;56(3):729–764. doi: 10.1121/1.1903322. [DOI] [PubMed] [Google Scholar]
- 47.Elliott DN, Fraser WR. Foundations of Modern Auditory Theory. Academic Press Inc; 1970. Fatigue and Adaptation; pp. 115–155. [Google Scholar]
- 48.Heiland KE, Goode RL, Asai M, Huber AM. A human temporal bone study of stapes footplate movement. Am J Otol. 1999;20(1):81–86. [PubMed] [Google Scholar]
- 49.Maccà I, Scapellato ML, Carrieri M, Maso S, Trevisan A, Bartolucci GB. High-frequency hearing thresholds: effects of age, occupational ultrasound and noise exposure. Int Arch Occup Environ Health. 2015;88(2):197–211. doi: 10.1007/s00420-014-0951-8. [DOI] [PubMed] [Google Scholar]
- 50.Smagowska B, Pawlaczyk-Łuszczyńska M. Effects of ultrasonic noise on the human body-a bibliographic review. Int J Occup Saf Ergon. 2013;19(2):195–202. doi: 10.1080/10803548.2013.11076978. [DOI] [PubMed] [Google Scholar]