

Review Committee for Descriptive Rules for Achalasia of the Esophagus
President
Hisahiro Matsubara
Former President
Nobutoshi Ando
English Edition Committee, Chairman
Nobuo Omura
Adviser
Hideyuki Kashiwagi
English Edition Committee Members
- Soji Ozawa
Surgery
- Tatsuyuki Kawano
Surgery
- Hiroyasu Makuuchi
Surgery
- Katsuhiko Iwakiri
Internal Medicine
- Motoyasu Kusano
Internal Medicine
- Ken Haruma
Internal Medicine
- Kaiyo Takubo
Pathology
- Akio Yanagisawa
Pathology
Japanese Edition Committee, Chairman
Hideyuki Kashiwagi
Contents
Descriptive Rules for Achalasia of the Esophagus
-
I.Achalasia of the Esophagus
- Definition
- Symptoms
- Diagnosis
-
3.1Diagnostic features on esophagography
-
3.2Diagnostic features on upper gastrointestinal endoscopy
-
3.3Diagnostic features on esophageal manometry
-
3.1
- Classification
-
4.1Radiographic images of the esophagus
-
4.2Endoscopy
-
4.3Esophageal manometry
-
4.4Histopathology
-
4.1
- Treatment
-
5.1Pharmacotherapy
-
5.2Endoscopic treatment
-
5.3Surgical treatment
-
5.1
-
II.Other Esophageal Motility Disorders
- Diffuse esophageal spasm (DES)
- Nutcracker esophagus
- Hypertensive LES
- Non-specific esophageal motility disorder (NEMD)
- Esophageal motility dysfunctions complicating other diseases
- Pseudoachalasia
I Achalasia of the esophagus
1. Definition
Achalasia of the esophagus is an esophageal motility disorder of unknown etiology, characterized by failure of relaxation of the lower esophageal sphincter (LES) and impaired peristaltic movement of the lower esophageal body.
2. Symptoms
Symptoms include dysphagia, regurgitation of ingested food into the oral cavity, chest pain, weight loss, and nocturnal cough.
3. Diagnosis
Useful diagnostic modalities for this disorder include: (1) esophagography; (2) upper gastrointestinal endoscopy; (3) esophageal manometry; (4) histopathologic examination of the esophageal muscle layers (in patients undergoing surgery).
3.1 Diagnostic features on esophagography
Dilatation/tortuosity of the esophagus
Retained food in the esophagus and poor emptying of barium
Smooth conical narrowing of the esophagogastric junction (bird-beak sign)
Absence or diminution of gastric air bubbles
Abnormal esophageal motility
3.2 Diagnostic features on upper gastrointestinal endoscopy
Dilatation of the esophageal lumen
Abnormal retention of food and/or liquid remnants in the esophagus
Whitish change and thickening of the esophageal mucosal surface
Functional stenosis of the esophagogastric junction (endoscope passes through the stenotic segment although the esophagogastric junction fails to be dilated by insufflation; the procedure may involve winding of tissue around the scope or leafing of tissue on scope rotation)
Abnormal contraction waves of the esophagus
3.3 Diagnostic features on esophageal manometry
Deglutitive dysrelaxation of the LES*
Disappearance of primary peristaltic waves*
Increased esophageal static pressure (higher than the intragastric pressure)
Increased LES pressure
Occurrence of simultaneous contraction waves
*Principal finding
4. Classification
4.1 Radiographic images of the esophagus
X-ray examination: a dorsoventral view is obtained with the patient in the standing position; the patient is asked to swallow a barium meal, consisting of 100 mL of 100% barium sulfate, as quickly as possible, so that radiograms can be obtained within 1 min of the swallowing. No spasmolytic agent is used.
Morphologic type
This classification is based on the radiographic features of the esophagus. This classification, subclassified into the spindle type, flask type and sigmoid type according to the conventional descriptive rules, has been extensively used over decades. However, there are no distinct pathophysiological differences between the spindle type and the flask type, and no distinction is made between these two types in the United States or Europe. As for the sigmoid type, the extent of deviation and tortuosity of the upper esophagus may also have an impact on the therapeutic outcome. Therefore, achalasia is classified into the following two types in this version of the descriptive rules.
-
i.
Straight (St) type (Fig. 1)
Modest degree of tortuosity of the longitudinal axis of the esophagus. This type includes the conventional spindle type and flask type mentioned above.
-
ii.
Sigmoid (Sg) type (Fig. 2)
Significant degree of tortuosity of the longitudinal axis of the esophagus. Pronounced rightward tortuosity of the esophagus, causing the organ to assume an L-shaped course, is specifically termed the advanced sigmoid (aSg) type (Fig. 3).
Fig. 1.

Straight (St) type
Fig. 2.
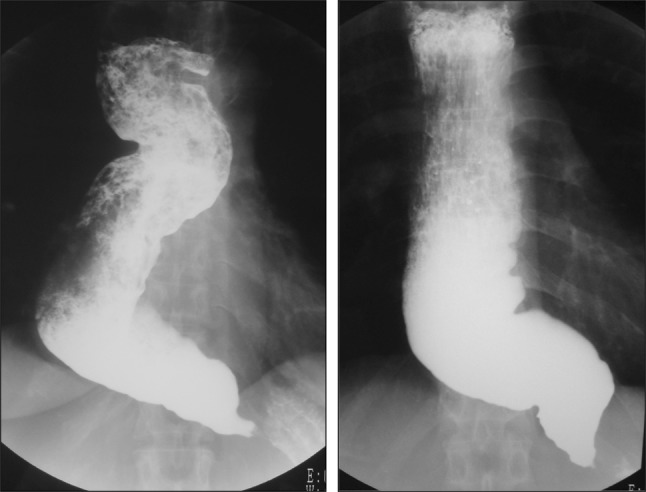
Sigmoid (Sg) type
Fig. 3.

Advanced sigmoid (aSg) type
Addendum:
The St type, Sg type, and aSg type are illustrated in Fig. 4.
Fig. 4.

Distinction among the St, Sg, and aSg types
In cases where esophageal flexion(s) is noted, a straight line should be drawn in the direction of the esophageal long axis.
In case two straight lines are drawn, a single angle will be formed by the crossing straight lines; in case three straight lines are drawn, two angles will be formed by the crossing straight lines.
The following definitions are framed in order of increasing angle, α, formed by the crossing straight lines.
When α ≥ 135°, the disorder is diagnosed as the St type.
When 90° ≤ α < 135°, the disorder is diagnosed as the Sg type.
When α < 90°, the disorder is diagnosed as the aSg type.
The angle(s) should be stated without fail.
-
(2)
Dilatation grading (Fig. 5)
Fig. 5.

Dilatation grading. Grade I d < 3.5 cm, Grade II 3.5 ≤ d < 6.0 cm, Grade III 6.0 cm ≤ d
The dilatation is classified into Grades I to III according to the maximum transverse diameter (d) of the esophagus drawn perpendicularly to the longitudinal axis.
-
i.
Grade I d < 3.5 cm
-
ii.
Grade II 3.5 ≤ d < 6.0 cm
-
iii.
Grade III 6.0 cm ≤ d
Addenda:
-
i.
Tortuosity of the upper thoracic esophagus (Fig. 6)
-
ii.
Leftward-tortuous esophagus (Fig. 7)
-
iii.
Concurrent epiphrenic diverticulum (pulsion diverticulum) (Fig. 8)
-
iv.
Concurrent carcinoma of the esophagus (location, size, and depth of invasion should be stated)
Fig. 6.

Tortuosity of the upper thoracic esophagus
Fig. 7.

Leftward tortuosity of the esophagus
Fig. 8.

Concurrent epiphrenic diverticulum
4.2 Endoscopy (Fig. 9)
Fig. 9.

Endoscopic images. Normal type (a), retained type (b), dilated type (c), and dilated-retained type (d)
Achalasia of the esophagus is classified into the following four types according to the endoscopic findings.
-
i.
Normal type: there is no obvious retention of ingested food or dilatation of the esophagus.
-
ii.
Retained type: retention of ingested food or fluid in the esophagus, but no apparent dilatation.
-
iii.
Dilated type: dilatation of the esophagus is evident, but no retained ingested food is seen in the esophagus.
-
iv.
Retained-dilated type: the esophagus is dilated with retained ingested food.
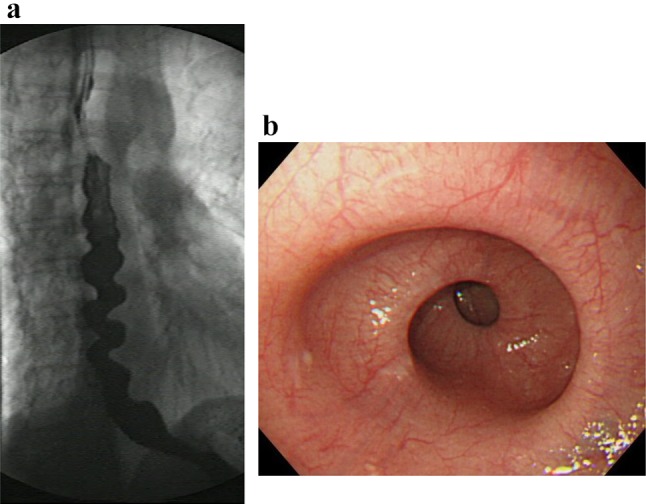
Reference findings suggestive of achalasia (Fig. 10)
Fig. 10.

Endoscopic images of the cardiac portion of the esophagus. Healthy subject (a) and a patient with achalasia (b)
In healthy subjects who inspire deeply, the lower esophagus usually opens, and an entire view of the esophageal palisade vessels becomes visible. However, in patients with achalasia, an entire view of the esophageal palisade vessels does not become visible and, in addition, rosette-like esophageal folds appear in the lower esophagus [1].
4.3 Esophageal manometry
Achalasia of the esophagus is classified into the following two types according to the findings on esophageal manometry.
-
i.
Complete type
Impaired relaxation of the LES and the absence of esophageal peristalsis in response to swallowing.
-
ii.
Incomplete type
Not meeting the above criteria.
Esophageal manometric findings in healthy subjects (Fig. 11a, b)
Fig. 11.

Esophageal high-resolution manometry findings of primary peristalsis and lower esophageal sphincter (LES) relaxation after water swallowing in healthy subject. a Manometric instrument: Trace! (Dr. G.S. Hebbard, The Royal Melbourne Hospital, Parkville, Australia). b Manometric instrument: ManoScan 360™ (Sierra Scientific Instruments Inc.)
Esophageal manometric findings in patients with achalasia (Fig. 12, b)
Impaired relaxation of the LES
Absence of esophageal peristalsis
Fig. 12.

Esophageal high-resolution manometry findings in a patient with achalasia. Manometric instrument: Trace! (Dr. G.S. Hebbard, The Royal Melbourne Hospital, Parkville, Australia)
Addendum:
i) Vigorous achalasia [2] (Fig. 13a, b)
Fig. 13.

Esophageal manometry findings in a patient with vigorous-type achalasia. Manometric instrument: ManoScan 360™ (Sierra Scientific Instruments Inc.). a Conventional method. b Esophageal high-resolution manometry
In addition to the above diagnostic criteria, when amplitude of the lower esophagus is ≥37 (30 to 40) mmHg, this condition is defined as vigorous achalasia, and when amplitude of the lower esophagus is <37 (30 to 40) mmHg, it is termed classic achalasia.
4.4 Histopathology (Figs. 14, 15)
Fig. 14.

Histopathologic photomicrographs (Grade II). a Lymphocyte accumulation in Auerbach’s plexus between the hypertrophic inner circular and outer longitudinal muscle layers. b Close-up view of a. Prominent lymphocyte infiltration and fibrosis are evident in Auerbach’s plexus. There is an evident decrease in the number of neuroganglion cells and degeneration of neuroganglion cells
Fig. 15.

Histopathologic photomicrographs (Grade III). a A smaller Auerbach’s plexus is evident in the hypertrophic inner circular and outer longitudinal layers of the tunica muscularis propria. b Close-up view of a. Fibrosis is evident in Auerbach’s plexus. Loss of neuroganglion cells and the nerve fiber network is observed
It is advisable for evaluation of the esophageal muscularis propria to be performed both on specimens from the dilated segment and narrowed segment. The tissue sampling sites must be stated. Achalasia of the esophagus is classified under the following three categories according to the ganglion cell/nerve fiber status observed on histopathology.
Grade I: practically normal ganglion cells and nerve fibers.
Grade II: diminution and degeneration of ganglion cells and nerve fibers.
Grade III: loss of ganglion cells and nerve fibers.
Addendum: note if there is any lymphocytic infiltration, etc.
5. Treatment
Calcium channel antagonists (e.g., Adalat® Capsule) and nitrates (e.g., Nitorol® Tablet) are used as drugs to relax the LES. In patients with pronounced subjective symptoms, complete relief of the symptoms can often not be obtained with pharmacotherapy alone. Currently, pharmacotherapy is generally recognized as the treatment option of choice for patients with mild disorder and for those who are not suitable candidates for endoscopic therapy or surgery, as well as for temporary relief of symptoms. The medications are also prescribed as needed in case of postoperative chest pain. Calcium antagonists are subject to off-label use in terms of national health insurance scheme.
5.2 Endoscopic treatment
(1) Dilatation therapy [11–13]
Following endoscopic insertion of a guidewire into the stomach, a balloon (usually, a 30-mm balloon) is placed at the gastroesophageal junction along the guidewire under fluoroscopic guidance; the balloon is then gradually inflated, beginning at a low pneumatic pressure level, while checking for pain until the balloon notches disappear. The pneumatic pressure is further elevated slightly to dilate the balloon while checking for pain, although excessive pressurization may be risky. The reported effectiveness rates of balloon dilatation range from 66 to 93%, hence virtually comparable to effectiveness rates of surgical treatment. However, the reported effectiveness rates of balloon dilatation in young adults (under 40 years of age) are poorly responsive to treatment. Symptoms recur in about 33% of patients at 4 to 6 years after balloon dilatation. Complications include reflux esophagitis, chest pain, fever, and perforation.
The conditions and frequency of balloon dilatation should be stated in each case of dilatation therapy.
(2) Botulinum toxin local injection therapy [14, 15]
Botulinum toxin local injection reduces in the LES pressure via inhibiting neurotransmitter release from the preganglionic cholinergic neurons. In botulinum toxin local injection therapy, 100 IU of type A botulinum toxin is injected endoscopically into the 4 quadrants of the LES. Relapse is often reported in 6–12 months. Use of botulinum toxin local injection therapy for achalasia cardia is subject to off-label use for the purpose of coverage by the national health insurance scheme in Japan.
(3) Endoscopic myotomy [16]
This procedure consists of peroral endoscopic myotomy performed on the esophageal submucosa. Use of endoscopic myotomy for the treatment of achalasia cardia is listed as off-label use for the purpose of coverage by the national health insurance scheme.
5.3 Surgical treatment [17–24]
Surgical treatment was previously performed via a laparotomy, and the procedure has recently become supplanted by a laparoscopic technique. Heller’s myotomy to relieve obstruction combined with a reflux-preventive procedure to prevent post-myotomy gastroesophageal reflux, especially the Dor technique, is widely used, with gratifying response rates of as high as about 90%.
The length of muscle layer incision, whether the short gastric arteries vessels were dissected or not, whether an esophageal bougie was inserted during the operation or not, and whether there was any intraoperative mucosal injury or not should be stated.
II Other Esophageal Motility Disorders [25−30]
1. Diffuse esophageal spasm (DES) (Figs. 16, 17, 18)
Fig. 16.

Esophageal manometry in a patient with DES by ManoScan 360™ (Sierra Scientific Instruments Inc.). a Normal peristalsis. b Simultaneous contractions
Fig. 17.

Esophageal manometry in a patient with DES by high-resolution manometry. a Normal peristalsis. b Simultaneous contractions
Fig. 18.

Radiographic appearance in a patient with DES
DES is a motility disorder characterized by occasional, persistent or repetitive abnormal contractions while peristaltic waves are usually normal, and may cause dysphagia and chest pain. One of the diagnostic criteria is that 2 or more repetitive simultaneous contractions account for 20% or more of the peristalsis on water swallow. The abnormality may be accompanied with multi-peaked contractions, elevation of the amplitude of the peristaltic waves, spontaneous contractions, and incomplete LES relaxation. Esophageal X-ray findings may include simultaneous contractions (nonperistaltic contractions), corkscrew appearance, arrest of contrast medium passage, and pocket formation.
2. Nutcracker esophagus (Figs. 19, 20)
Fig. 19.

Esophageal high-resolution manometry findings in a patient with nutcracker esophagus. Manometric instrument: Trace ! (Dr. G.S. Hebbard, The Royal Melbourne Hospital, Parkville, Australia)
Fig. 20.
X-ray (a) and endoscopic (b) images of nutcracker esophagus
Nutcracker esophagus is one of primary esophageal motility disorders. Nutcracker esophagus is defined as normal peristalsis of the esophageal body with an average distal esophageal amplitude exceeding 180 mm Hg and often has non-cardiac chest pain or dysphagia. Barium swallows are usually normal but a corkscrew-like esophagus, reminiscent of the findings of diffuse esophageal spasm (DES), is observed occasionally.
3. Hypertensive lower esophageal sphincter (Hypertensive LES)
This esophageal motility disorder is characterized by elevation of LES pressure, causing chest pain and dysphagia. A mean resting LES static pressure of ≥45 mmHg, normal relaxation of the LES, and normal peristaltic waves of the esophageal body are essential for diagnosis of this disorder.
4. Non-specific esophageal motility disorder (NEMD) (Fig. 21)
Fig. 21.

Esophageal manometric features in NEMD. Manometric instrument: INSIGHT (Sandhill Scientific Instruments Inc.)
NEMD represents a spectrum of esophageal motility abnormalities presenting with apparent esophageal manometric tests, but failing to meet the diagnostic criteria for the esophageal manometric features of achalasia, DES, nutcracker esophagus or hypertensive LES. The most common manometric finding among the esophageal motility abnormalities is the occurrence of low contraction waves with amplitudes of ≤30 mmHg or nonpropagating contractions in the lower esophagus. According to the latest classification of esophageal manometry, detection of the above manometric finding on water swallowing at a frequency of ≥30% is newly defined as ineffective esophageal motility (IEM).
5. Esophageal motility dysfunctions complicating other diseases
Esophageal motility dysfunction may be associated with collagen diseases such as scleroderma and systemic lupus erythematosus, diabetes mellitus, amyloidosis, eosinophilic esophagitis, neurodegenerative disorders such as Parkinson’s disease, and alcohol dependence.
6. Pseudoachalasia
This disorder presents with apparently achalasia-like symptoms/findings associated with malignancy, such as carcinoma of the esophagogastric junction.
References
- 1.Iwakiri K, Hoshihara Y, Kawami N, et al. The appearance of rosette-like esophageal folds(“esophageal rosette”)in the lower esophagus after a deep inspiration is a characteristic endoscopic finding of primary achalasia. J Gastroenterol. 2010;45(4):422–425. doi: 10.1007/s00535-009-0179-7. [DOI] [PubMed] [Google Scholar]
- 2.Camacho-Lobato L, Katz PO, Eveland J, et al. Vigorous achalasia: original description requires minor change. J Clin Gastroenterol. 2001;33(5):375–377. doi: 10.1097/00004836-200111000-00006. [DOI] [PubMed] [Google Scholar]
- 3.Hongo M. The effects of calcium-antagonists on lower esophageal sphincter pressure-the possibility of application of nifedipine to achalasia. J Jpn Soc Gastroenterol. 1982;79(10):1883–1891. [PubMed] [Google Scholar]
- 4.Becker BS, Burakoff R. The effect of verapamil on the lower esophageal sphincter pressure in normal subjects and in achalasia. Am J Gastroenterol. 1983;78(12):773–775. [PubMed] [Google Scholar]
- 5.Wong RK, Maydonovitch C, Garcia JE, et al. The effect of terbutaline sulfate, nitroglycerin, and aminophylline on lower esophageal sphincter pressure and radionuclide esophageal emptying in patients with achalasia. J Clin Gastroenterol. 1987;9(4):386–389. doi: 10.1097/00004836-198708000-00006. [DOI] [PubMed] [Google Scholar]
- 6.Coccia G, Borttolotti M, Michetti P, et al. Prospective clinical and manometric study comparing pneumatic dilatation and sublingual nifedipine in the treatment of oesophageal achalasia. Gut. 1991;32(6):604–606. doi: 10.1136/gut.32.6.604. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Short TP, Thomas E. An overview of the role of calcium antagonists in the treatment of achalasia and diffuse oesophageal spasm. Drug. 1992;43(2):177–184. doi: 10.2165/00003495-199243020-00004. [DOI] [PubMed] [Google Scholar]
- 8.Harasawa S. Manual for treatment of chronic diseases. Achalasia. Clinic All-Round. 1997;46:1059–1062. [Google Scholar]
- 9.Eherer AJ, Schwetz I, Hammer HF, et al. Effect of sildenafil on oesophageal motor function in healthy subjects and patients with oesophageal motor disorders. Gut. 2002;50(6):758–764. doi: 10.1136/gut.50.6.758. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Kaufman JA, Oelschlager BK. Treatment of achalasia. Curr Treat Opinions Gastroenterol. 2005;8(1):59–69. doi: 10.1007/s11938-005-0052-6. [DOI] [PubMed] [Google Scholar]
- 11.Tanaka Y, Iwakiri K, Kawami N, et al. Predictors of a better outcome of pneumatic dilatation in patients with primary achalasia. J Gastroenterol. 2010;45(2):153–158. doi: 10.1007/s00535-009-0145-4. [DOI] [PubMed] [Google Scholar]
- 12.Boeckxstaens GE, Annese V, des Varannes SB, et al. European Achalasia Trial Investigators. Pneumatic dilation versus laparoscopic Heller’s myotomy for idiopathic achalasia. N Engl J Med. 2011;364(19):1807–1816. doi: 10.1056/NEJMoa1010502. [DOI] [PubMed] [Google Scholar]
- 13.Richter JE, Boeckxstaens GE. Management of achalasia: surgery or pneumatic dilation. Gut. 2011;60(6):869–876. doi: 10.1136/gut.2010.212423. [DOI] [PubMed] [Google Scholar]
- 14.Zaninotto G, Annese V, Costantini M, et al. Randomized controlled trial of botulinum toxin versus laparoscopic Heller myotomy for esophageal achalasia. Ann Surg. 2004;239(3):364–370. doi: 10.1097/01.sla.0000114217.52941.c5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Mikaeli J, Yaghoobi M, Montazeri G, et al. Efficacy of botulinum toxin injection before pneumatic dilatation in patients with idiopathic achalasia. Dis Esophagus. 2004;17(3):213–217. doi: 10.1111/j.1442-2050.2004.00410.x. [DOI] [PubMed] [Google Scholar]
- 16.Inoue H, Minami H, Kobayashi Y, et al. Peroral endoscopic myotomy(POEM)for esophageal achalasia. Endoscopy. 2010;42(4):265–271. doi: 10.1055/s-0029-1244080. [DOI] [PubMed] [Google Scholar]
- 17.Makuuchi H, Mitomi T, Sasaki T, et al. Diagnosis and treatment for esophageal achalasia. The Japanese. J Thorac Cardiovasc Surg. 1988;36(5):737–739. [Google Scholar]
- 18.Mitomi T, Makuuchi H. Functional disorders. Surgery for esophagus. Shin Gekagaku Taikei 21, Nakayama-shoten, Tokyo, pp 353–96;1988.
- 19.Kostic S, Kjellin A, Ruth M, et al. Pneumatic dilatation or laparoscopic cardiomyotomy in the management of newly diagnosed idiopathic achalasia. Results of a randomized controlled trial. World J Surg. 2007;31(3):470–478. doi: 10.1007/s00268-006-0600-9. [DOI] [PubMed] [Google Scholar]
- 20.Lopushinsky SR, Urbach DR. Pneumatic dilatation and surgical myotomy for achalasia. JAMA. 2006;296(18):2227–2233. doi: 10.1001/jama.296.18.2227. [DOI] [PubMed] [Google Scholar]
- 21.Palanivelu C, Maheshkumar GS, Jani K, et al. Minimally invasive management of achalasia cardia: results from a single center study. JSLS. 2007;11(3):350–357. [PMC free article] [PubMed] [Google Scholar]
- 22.Wang L, Li YM, Li L. Meta-analysis of randomized and controlled treatment trials for achalasia. Dig Dis Sci. 2009;54(11):2303–2311. doi: 10.1007/s10620-008-0637-8. [DOI] [PubMed] [Google Scholar]
- 23.Zaninotto G, Costantini M, Rizzetto C, et al. Four hundred laparoscopic myotmies for esophageal achalasia: a single centre experience. Ann Surg. 2008;248(6):986–993. doi: 10.1097/SLA.0b013e3181907bdd. [DOI] [PubMed] [Google Scholar]
- 24.Jeansonne LO, White BC, Pilger KE, et al. Ten-year follow-up of laparoscopic Heller myotomy for achalasia shows durability. Surg Endosc. 2007;21(9):1498–1502. doi: 10.1007/s00464-007-9500-9. [DOI] [PubMed] [Google Scholar]
- 25.Esophageal motility testing made easy. Bremner CG, DeMeester TR, Bremner RM, Mason RJ, eds. Quality Medical Publishing, ST. Louis, Missouri, 2001.
- 26.Kusano M, Maeda M, Shimoyama Y, et al. Esophageal motor function in nonachalasia motility disorders. J Jpn Soc Gastroenterol. 2003;100(9):1095–1105. [PubMed] [Google Scholar]
- 27.Kashiwagi H, Omura N. Each argument 1. Benign diseases 2. Function and abnormal structure. Shokudogeka up-to-date, Kuwano H eds, Chugai Medical co, Tokyo, p 40–55;2010.
- 28.Clouse RE, Staiano A. Contraction abnormalities of the esophageal body in patients referred for manometry. Dig Dis Sci. 1983;28(9):784–791. doi: 10.1007/BF01296900. [DOI] [PubMed] [Google Scholar]
- 29.Kahrilas PJ, Dodds WJ, Hogan WJ. Effect of peristaltic dysfunction on esophageal volume clearance. Gastroenterology. 1988;94(1):73–80. doi: 10.1016/0016-5085(88)90612-9. [DOI] [PubMed] [Google Scholar]
- 30.Leite LP, Johnston BT, Barrett J, et al. Ineffective esophageal motility(IEM):the primary finding in patients with non-specific esophageal motility disorder. Dig Dis Sci. 1997;42(9):1859–1865. doi: 10.1023/A:1018802908358. [DOI] [PubMed] [Google Scholar]