

Abstract
Background
Median overall survival for patients with metastatic soft tissue sarcoma is 12 to 16 months. Olaratumab is a human anti–platelet-derived growth factor receptor α monoclonal antibody which has antitumour activity in human sarcoma xenografts.
Methods
We conducted an open-label phase 1b, randomised, phase 2 study of doxorubicin ± olaratumab in patients with unresectable/metastatic soft tissue sarcoma. The phase 1b primary endpoint was safety; the phase 2 primary endpoint was progression-free survival using a two-sided alpha level of 0·2 and statistical power of 0·8. This study was registered with ClinicalTrials.gov, number NCT01185964.
Findings
Fifteen patients were enrolled and treated with olaratumab+doxorubicin in the phase 1b portion; 133 patients were randomised (66 to olaratumab+doxorubicin; 67 to doxorubicin) in the phase 2 portion, 129 of whom (97%) received at least one dose of study treatment (64 olaratumab+doxorubicin; 65 doxorubicin). Median progression-free survival in phase 2 was 6·6 months (95% confidence interval [CI], 4·1–8·3) with olaratumab+doxorubicin and 4·1 months (95% CI, 2·8–5·4) with doxorubicin (stratified hazard ratio [HR], 0·672; 95% CI, 0·442–1·021; p=0·0615). Median overall survival was 26·5 months (95% CI, 20·9–31·7) with olaratumab+doxorubicin and 14·7 months (95% CI, 9·2–17·1) with doxorubicin (stratified HR, 0·463; 95% CI, 0·301–0·710; p=0·0003). Adverse events more frequent with olaratumab+doxorubicin vs doxorubicin alone included neutropenia (38 [59%] vs 25 [39%]), mucositis (34 [53%] vs 23 [35%]), nausea (47 [73%] vs 34 [52%]), vomiting (29 [45%] vs 12 [19%]), and diarrhea (22 [34%] vs 15 [23%]). Febrile neutropenia of grade ≥3 was similar in both groups (olaratumab plus doxorubicin 8 (13%) vs doxorubicin 9 (14%).
Interpretation
This study of olaratumab with doxorubicin in patients with advanced soft tissue sarcoma met its predefined primary endpoint for progression-free survival and achieved a highly significant improvement of 11·8 months in median overall survival (P=0·0003; HR 0·46).
Funding
Eli Lilly and Company.
Keywords: soft tissue sarcoma, olaratumab, monoclonal antibody, doxorubicin
Introduction
Soft tissue sarcoma is a rare and diverse group of solid tumours originating from mesenchymal precursors1,2. They account for approximately 1% of all new adult malignancies.2,3 Doxorubicin, either alone or in combination, remains a standard of care. However, survival for treated patients with metastatic disease is only 12 to 16 months, and the two-year survival rate is approximately 30%.4,5 Few, if any, novel therapies or chemotherapy combinations have been able to improve these poor outcomes3–5; consequently, soft tissue sarcoma represents an important unmet medical need.
Platelet-derived growth factor (PDGF)/PDGF receptor (PDGFR) signaling plays a significant role in mesenchymal biology, including mesenchymal stem cell differentiation, growth, and angiogenesis.6,7 The PDGF/PDGFR signaling pathway is also involved in cancer through aberrant cellular signaling and has been implicated in modulating the tumour/stromal microenvironment and facilitating metastases in numerous malignancies.8,9
Olaratumab is a recombinant human immunoglobulin G subclass 1 (IgG1) monoclonal antibody that specifically binds PDGFRα, blocking PDGF-AA, -BB, and -CC binding and receptor activation.10 Preclinical studies of olaratumab alone10 or in combination with doxorubicin11 have demonstrated antitumour activity in human sarcoma xenograft models. Based on these preclinical data and the rationale for disrupting PDGF/PDGFR signaling in sarcoma cells and the tumour/stromal microenvironment, we performed a phase 1b/randomised phase 2 study, evaluating the safety and efficacy of adding olaratumab to doxorubicin in patients with advanced soft tissue sarcoma.
Methods
Patients and Methods
Patients were enrolled at 16 clinical sites in the United States. For both the phase 1b and 2 portions of the study, eligible patients were ≥18 years of age and had a histologically confirmed diagnosis of locally advanced or metastatic soft tissue sarcoma not previously treated with an anthracycline, an Eastern Cooperative Oncology Group (ECOG) performance status of 0 to 2, and available tumour tissue to determine PDGFRα expression by immunohistochemistry. The phase 1b primary endpoint was safety. The phase 2 primary endpoint was progression-free survival; secondary endpoints included overall survival, objective response rate, safety, and pharmacokinetics (Methods section, Supplementary Appendix).
In the phase 1b portion of the study, patients received olaratumab (15 mg/kg) intravenously on day 1 and day 8 plus doxorubicin (75 mg/m2) on day 1 of each 21-day cycle for up to 8 cycles. After 8 cycles of the combination, in the absence of disease progression or unacceptable toxicities, patients were allowed to receive olaratumab monotherapy until disease progression. During cycles 5 through 8, dexrazoxane was allowed on day 1 of each cycle to reduce the potential for doxorubicin-related cardiotoxicity. The phase 1b portion was closed to enrolment once ten patients had received study treatment for two cycles.
Randomisation
In the open-label phase 2 portion of the study, patients were randomly assigned in a 1:1 ratio to receive olaratumab plus doxorubicin (as described in the phase 1b portion) or doxorubicin alone (75 mg/m2) on day 1 of each 21-day cycle for up to 8 cycles (Methods section, Supplementary Appendix). Dexrazoxane was allowed in both treatment groups during cycles 5 through 8 of doxorubicin. After completion of 8 cycles of doxorubicin, patients in the olaratumab+doxorubicin group could receive olaratumab monotherapy until disease progression, and patients in the doxorubicin group were observed and could receive olaratumab monotherapy after documented disease progression.
Randomisation was dynamic and used the minimization randomisation technique12 to balance patients by ECOG performance status (0–1 vs 2), histological tumour type (leiomyosarcoma vs synovial sarcoma vs other), immunohistochemical PDGFR expression (positive vs negative), and previous lines of treatment (0 vs ≥1 line of therapy) (Methods section, Supplementary Appendix).
Tumour response was assessed every 6 weeks according to the Response Evaluation Criteria in Solid Tumours, version 1·113 (Methods section, Supplementary Appendix). Survival was assessed every 2 months until study completion. Blood samples were collected for pharmacokinetic and immunogenic analyses. Safety was assessed for all patients who received at least one dose of study treatment. Adverse events and clinical laboratory toxicity were graded according to the National Cancer Institute Common Terminology Criteria for Adverse Events, version 4·0. Cardiac function was monitored by echocardiography or multigated acquisition scanning before treatment start and before treatment at cycles 5 and 7.
PDGFRα Assessment
PDGFR expression was assessed by immunohistochemistry at a central academic laboratory before enrolment (phase 1b) or randomisation (phase 2) (Methods section, Supplementary Appendix). After the study was completed, the randomisation assay was found to recognize both PDGFRα and β, so an additional PDGFRα-specific assay was developed and used for all post-hoc efficacy analyses.
Statistical Analysis
The Phase 1b part of the trial was intended to provide an initial look at safety outcomes relative to dosage and exposure in a small number of patients. For this purpose, a pragmatic decision to enroll 10–15 patients was made without formal statistical considerations. The phase 2 planned sample size was 130 patients, which assumed a 50% improvement in median progression-free survival (hazard ratio [HR], 0·67) for the olaratumab+doxorubicin group, a statistical power of 80%, and a two-sided significance level of 0·20. A planned interim analysis of the primary endpoint was performed with a nominal alpha spend of 0·0001, resulting in a final nominal adjusted alpha level of 0·1999 (two-sided).
The efficacy analyses were performed in the randomisation patient population (intention-to-treat population). The safety analyses were performed in the population of patients who received at least one dose of study treatment (safety population).
Study Oversight
The protocol was approved by the institutional review board at each participating center. The study was conducted in accordance with the Declaration of Helsinki and the International Conference on Harmonisation Guidelines for Good Clinical Practice. All patients provided written informed consent to participate.
Role of the funding source
The study was designed by the sponsor, Eli Lilly and Company, with input from sarcoma experts, and data were collected by Eli Lilly and Company. The data were analysed in collaboration with the academic authors. All authors vouch for the accuracy and completeness of the data and analyses reported and for the fidelity of the study to the study protocol. All authors had final responsibility for the decision to submit for publication. The first author prepared the initial draft of the manuscript with editorial assistance, and all authors contributed to subsequent drafts. The protocol is available at http://www.thelancet.com/.
Results
Study Population
From 6 October 2010 through 14 January 2013, 15 patients were enrolled and treated in the phase 1b portion of the study (figure S1), and 133 patients were randomised (66 to olaratumab+doxorubicin; 67 to doxorubicin) in the phase 2 portion, 129 of whom (97%) received at least one dose of study treatment (64 in the olaratumab+doxorubicin group; 65 in the doxorubicin group) (figure 1). Baseline characteristics (tables 1,2, and S1) were balanced except for slightly more women in the combination arm.
Figure 1. Enrollment and Outcomes in Phase 2.
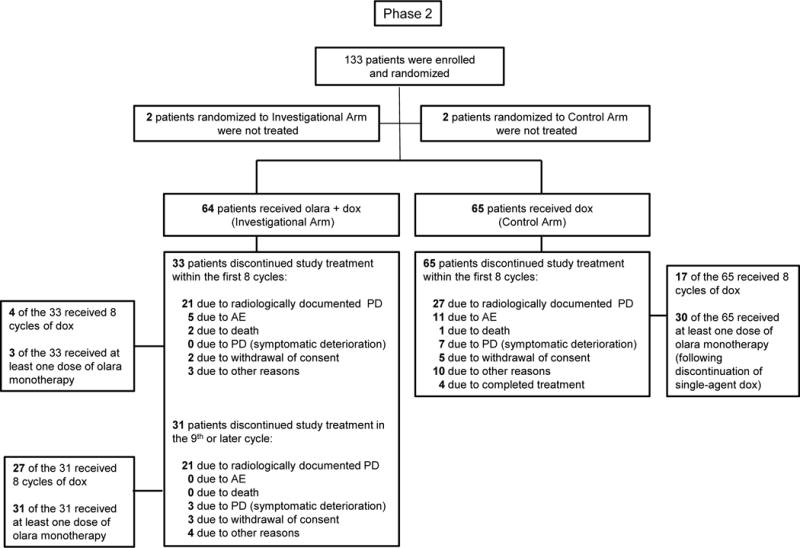
Control arm = doxorubicin; investigational arm = olaratumab + doxorubicin; olara = olaratumab
Data cut-off date: 16 May 2015.
Table 1.
Characteristics of Patients in Phase 2 at Baseline (Intention-to-Treat Population).
| Characteristic | Olaratumab + Doxorubicin (N=66) |
Doxorubicin (N=67) |
|---|---|---|
| Age—y | ||
| Median (range) | 58·5 (22–85) | 58·0 (29–86) |
| Sex—no. (%) | ||
| Male | 26 (39·4%) | 33 (49·3%) |
| Female | 40 (60·6%) | 34 (50·7%) |
| Race—no. (%) | ||
| White | 55 (83·3%) | 60 (89·6%) |
| Black | 6 (9·1%) | 5 (7·5%) |
| Asian | 2 (3·0%) | 2 (3·0%) |
| Native Hawaiian or other Pacific Islander | 1 (1·5%) | 0 |
| Other | 2 (3·0%) | 0 |
| Ethnicity—no. (%) | ||
| Hispanic or Latino | 6 (9·1%) | 2 (3·0%) |
| Not Hispanic or Latino | 60 (90·9%) | 64 (95·5%) |
| Missing | 0 | 1 (1·5%) |
| ECOG performance status—no. (%) | ||
| 0–1 | 62 (93·9%) | 63 (94·0%) |
| 2 | 4 (6·1%) | 4 (6·0%) |
| PDGFRα status—no. (%)a | ||
| Stratification assay | ||
| Positive | 58 (87·9%) | 59 (88·1%) |
| Negative | 8 (12·1%) | 8 (11·9%) |
| Exploratory assay (post hoc)b | ||
| Positive | 18 (32·7%) | 19 (33·9%) |
| Negative | 37 (67·3%) | 37 (66·1%) |
| Histological type—no. (%) | ||
| Leiomyosarcoma | 24 (36·4%) | 27 (40·3%) |
| Non-leiomyosarcomac | 42 (63·6%) | 40 (59·7%) |
| Previous treatments—no. (%) | ||
| 0 | 27 (40·9%) | 31 (46·3%) |
| ≥ 1 | 39 (59·1%) | 36 (53·7%) |
Abbreviations: ECOG = Eastern Cooperative Oncology Group performance status; PDGFRα = platelet-derived growth factor receptor
PDGFRα-positive status was defined as a staining result of 2+ or greater. The results from stratification assay results were used to stratify randomization.
“Positive” corresponds to weak intensity membranous staining comprising greater than 30% of the tumour and/or moderate to strong intensity membranous staining comprising greater than 5% of the tumour, and “negative” corresponds to staining that does not meet these requirements.
See Table S1 for a complete summary of disease by histological type, including “Other” subcategories.
Table 2.
| Histological type—no. (%) | Olaratumab + Doxorubicin (N=66) |
Doxorubicin (N=67) |
|---|---|---|
| Leiomyosarcoma | 24 (36·4%) | 27 (40·3%) |
| Undifferentiated pleomorphic sarcoma | 10 (15·2%) | 14 (20·9%) |
| Liposarcoma | 8 (12·1%) | 15 (22·4%) |
| Angiosarcoma | 4 (6·1%) | 3 (4·5%) |
| Synovial sarcoma | 1 (1·5%) | 2 (3·0%) |
| Neurofibrosarcoma | 1 (1·5%) | 0 |
| Fibrosarcoma | 1 (1·5%) | 0 |
| Othera | 17 (25·8%) | 6 (9·0%) |
See Table S1 for a complete summary of disease by histological type, including “Other” subcategories.
Progression-free Survival
Final analysis of the phase 2 primary endpoint of progression-free survival based on investigator assessment was performed after 103 events. The median progression-free survival was 6·6 months (95% confidence interval [CI], 4·1–8·3; interquartile range [IQR], 2·7–10·2) with olaratumab+doxorubicin and 4·1 months (95% CI, 2·8–5·4; IQR, 1·6–7·4) with doxorubicin (figure 2A; table S2). This improvement in favor of olaratumab+doxorubicin met the protocol-defined significance level of 0·1999 for final progression-free survival (stratified HR, 0·672; 95% CI, 0·442–1·021; p=0·0615). A blinded independent retrospective review of the radiologic scans (figure S2) showed a comparable HR (0·670; 95% CI, 0·04–1·12; p=0·1208) and a median progression-free survival of 8·2 months (95% CI, 5·5–9·8; IQR, 3·0–11·6) with olaratumab+doxorubicin and 4·4 months (95% CI, 3·1–7·4; IQR, 1·5–8·6) with doxorubicin. The 3-month and 6-month progression-free survival rates are provided in supplementary table S2.
Figure 2. Survival Endpoints in Phase 2.

Panels A and B show the Kaplan-Meier curves for the investigator assessment of progression-free survival and overall survival for the olaratumab + doxorubicin versus doxorubicin groups in the intention-to-treat population. CI denotes confidence interval, and HR denotes hazard ratio.*In Panel A the independent assessment of progression-free survival is included as an insert for comparison.
Objective Response Rate
The objective response rate was 18·2% (95% CI, 9·8–29·6) with olaratumab+doxorubicin and 11·9% (95% CI, 5·3–22·2) with doxorubicin (p=0·3421) (table S3). The objective response rate for the independent assessment was 18·2% (95% CI, 29·6–29·8) with olaratumab+doxorubicin and 7·5% (95% CI, 2·5–16·6) with doxorubicin (p=0·0740) (table S3). The disease control rate and median duration of response are provided in supplementary table S3.
Overall Survival
Final analysis of overall survival was performed per protocol after 91 deaths, approximately 70% of the intention-to-treat population. The median overall survival was 26·5 months (95% CI, 20·9–31·7; IQR, 13·8 to not evaluable) with olaratumab+doxorubicin and 14·7 months (95% CI, 9·2–17·1; IQR, 5·5–26·0) with doxorubicin (figure 2B). This difference of 11·8 months represented a statistically significant improvement in median overall survival (stratified HR, 0·46; 95% CI, 0·30–0·71; p=0·0003) and was consistent across the subgroup stratification factors including histological tumour type (leiomysarcoma vs non-leiomyosarcoma), number of lines of previous treatment (0 vs ≥1), and PDGFRα status (figure 3). More than 65% of patients in each of the two treatment groups received subsequent therapy after disease progression (table 3 and table S4). Sensitivity analyses for overall survival are shown in tables S5 and S6.
Figure 3. Forest Plot of Overall Survival Hazard Ratios for Potentially Prognostic Factors.

Forest plot of overall survival with hazard ratios (HR) and 95% confidence intervals (CI) for several subgroups that could potentially influence the overall survival treatment effect (phase 2, intention-to-treat population). Duration of disease is the time from date of histology/pathology confirmation of soft tissue sarcoma to date of informed consent. ECOG denotes Eastern Cooperative Oncology Group, PDGFRα denotes platelet-derived growth factor receptor alpha, and WBC denotes white blood cell.
Table 3.
Post-Treatment Anticancer Therapies Received (Phase 2).
| Post-treatment regimen, no. regimens | Olaratumab + Doxorubicin (N=66) |
Doxorubicina (N=67) |
|---|---|---|
| Any treatment | 44 (66·7) | 33 (49·3) |
| 1 | 18 (27·3) | 16 (23·9) |
| 2 | 12 (18·2) | 10 (14·9) |
| 3 | 9 (13·6) | 2 (3·0) |
| 4 | 1 (1·5) | 1 (1·5) |
| >4 | 4 (6·1) | 4 (6·0) |
Olaratumab monotherapy was not counted as a regimen for patients on the doxobicin arm, who elected to receive olaratumab monotherapy upon disease progression during doxorubicin therapy.
Pharmacokinetics and Exposure-response Analysis
Olaratumab serum concentration levels were available from 92 patients. Olaratumab mean maximum serum concentration (Cmax) reached 284 μg/mL (geometric coefficient of variation in % [CV%], 23∙3) and 293 μg/mL (CV%, 30∙5) after the first and second doses and returned to a mean trough serum concentration (Cmin) of 66∙5 μg/mL (CV%, 40∙4) at the end of the cycle (table S7). Steady state was reached during cycle 3; mean steady state Cmax and Cmin ranged from 419 μg/mL (CV%, 26∙2) through 487 μg/mL (CV%, 33∙0) and from 123 μg/mL (CV%, 31∙2) through 156 μg/mL (CV%, 38∙0) across cycles 4 through 9. Individual apparent terminal elimination half-life estimates of 6∙67 days and 14∙4 days were obtained during cycle 3 (table S8). Olaratumab serum levels observed in patients randomised to the doxorubicin group, who received olaratumab monotherapy after disease progression, were similar to those observed in patients in the olaratumab+doxorubicin group (table S7) Exposure-response analyses indicated that patients in the upper quartiles of olaratumab serum exposure showed a greater improvement in progression-free survival and overall survival, regardless of the pharmacokinetic endpoint considered (Cmin at the end of cycle 1, or average serum concentration throughout the treatment duration) (figures S3 and S4, tables S9 and S10).
Treatment Exposure
The median number of doxorubicin infusions was 7 (range, 1 to 8; IQR, 3 to 8) with a median cumulative dose level of 487∙6 mg/m2 (IQR, 221.7–598.8) in the olaratumab+doxorubicin group (table S11) and 4 infusions (range, 1 to 8; IQR, 2 to 8) with a median cumulative dose level of 299∙6 mg/m2 (IQR, 150.1–494.7) in the doxorubicin group. The median number of olaratumab infusions in the olaratumab+doxorubicin group was 16∙5 (range, 1∙0 to 83∙0, IQR 6 to 25.5) (table S12). The most common reason for discontinuation from study therapy in both groups was progression of disease (figure 1). The most common adverse event leading to patient discontinuation of doxorubicin was ejection-fraction decrease: 3 patients (5%) with olaratumab+doxorubicin and 4 patients (6%) with doxorubicin; the most common adverse event leading to discontinuation of olaratumab was infusion-related reaction: 2 patients (3%). In the olaratumab+doxorubicin group, 34 (53%) of 64 patients ended the olaratumab-doxorubicin combination therapy and received one or more cycles of olaratumab monotherapy (median, 9 infusions; range, 2 to 68; IQR 4 to 24; median, 4.5 cycles; IQR, 2 to 12) (Table S12). In the doxorubicin group, 30 (46%) of 65 patients opted to receive olaratumab monotherapy after disease progression and received a median of 4 infusions (range, 1 to 81; IQR, 4 to 8; median, 2 cycles; IQR, 2 to 4) (Table S12).
Adverse Events
Treatment-emergent adverse events are summarized in table S13 (phase 1b) and table 4 (phase 2). The most common treatment-emergent adverse events with olaratumab+doxorubicin in the phase 2 portion were nausea (n = 47 [73%]), fatigue (44 [69%]), neutropenia (38 [59%]), and mucositis (34 [53%]); and with doxorubicin, fatigue (45 [69%]), nausea (34 [52%]), alopecia (26 [40%]), and neutropenia (25 [39%]) (table 4).
Table 4.
Adverse Events (Phase 2).a
| Olaratumab + Doxorubicin (N=64) |
Doxorubicin (N=65) |
|||||
|---|---|---|---|---|---|---|
|
|
||||||
| Event | Any Grade | Grade 3 | Grade ≥4 | Any Grade | Grade 3 | Grade ≥4 |
| Any adverse event—no. of patients (%)b | 63 (98·4%) | 24 (37·5%) | 27 (42·2%) | 64 (98·5%) | 25 (38·5%) | 20 (30·8%) |
| Nausea | 47 (73·4%) | 1 (1·6%) | 0 | 34 (52·3%) | 2 (3·1%) | 0 |
| Fatiguec | 44 (68·8%) | 6 (9·4%) | 0 | 45 (69·2%) | 2 (3·1%) | 0 |
| Neutropeniad,e | 37 (57.8%) | 12 (18·8%) | 22 (34.4%) | 23 (35.4%) | 5 (7·7%) | 16 (24.6%) |
| Mucositisf | 34 (53·1%) | 2 (3·1%) | 0 | 23 (35·4%) | 3 (4·6%) | 0 |
| Alopecia | 33 (51·6%) | 0 | 0 | 26 (40·0%) | 0 | 0 |
| Vomiting | 29 (45·3%) | 0 | 0 | 12 (18·5%) | 0 | 0 |
| Anemiag | 26 (40·6%) | 8 (12·5%) | 0 | 24 (36·9%) | 6 (9·2%) | 0 |
| Leukopeniah,e | 26 (40.6%) | 14 (21.9%) | 9 (14.1%) | 12 (18.5%) | 5 (7.7%) | 6 (9.2%) |
| Constipation | 22 (34·4%) | 0 | 0 | 21 (32·3%) | 1 (1·5%) | 0 |
| Diarrhea | 22 (34·4%) | 2 (3·1%) | 0 | 15 (23·1%) | 0 | 0 |
| Decreased appetite | 20 (31·3%) | 1 (1·6%) | 0 | 13 (20·0%) | 0 | 0 |
| Abdominal paini | 15 (23·4%) | 2 (3·1%) | 0 | 9 (13·8%) | 0 | 0 |
| Pyrexia | 15 (23·4%) | 0 | 0 | 12 (18·5%) | 0 | 0 |
| Musculoskeletal painj | 41 (64·1%) | * | * | 16 (24·6%) | ** | ** |
| Febrile neutropeniak | 8 (12·5%) | 7 (10·9%) | 1 (1·6%) | 9 (13·8%) | 9 (13·8%) | 0 |
| Infections and infestationsk,l | 27 (42·2%) | 5 (7·8%) | 0 | 27 (41·5%) | 4 (6·2%) | 3 (4·6%) |
| Infusion-related reactionk,m | 8 (12·5%) | 0 | 2 (3·1%) | 0 | 0 | 0 |
| Treatment-related adverse event—no. of patients (%) | 63 (98·4%) | 18 (28·1%) | 25 (39·1%) | 63 (96·9%) | 19 (29·2%) | 17 (26·2%) |
| Adverse event leading to discontinuation of treatment—no. of patients (%) | 8 (12·5%) | 1 (1·6%) | 3 (4·7) | 12 (18·5) | 3 (4·6) | 5(7·7) |
| Serious adverse event—no. of patients (%) | ||||||
| Any event | 27 (42·2%) | 20 (31·3%) | 7 (10·9%) | 25 (38·5%) | 14 (21·5%) | 8 (12·3%) |
| Treatment-related event | 14 (21·9%) | 8 (12·5%) | 6 (9·4%) | 17 (26·2%) | 11 (16·9%) | 5 (7·7%) |
| Cardiac Dysfunctionn,o | 15 (23·4%) | 1 (1·6%) | 0 | 11 (16·9) | 0 | 0 |
| Oedema peripheral | 10 (15·6%) | 0 | 0 | 7 (10·8%) | 0 | 0 |
| Ejection fraction decreased | 5 (7·8%) | 1 (1·6%) | 0 | 4 (6·2%) | 0 | 0 |
| Congestive cardiac failure | 1 (1·6%) | 1 (1·6%) | 0 | 0 | 0 | 0 |
| Hepatojugular reflux | 1 (1·6%) | 0 | 0 | 0 | 0 | 0 |
| Jugular vein distension | 1 (1·6%) | 0 | 0 | 0 | 0 | 0 |
| Left ventricular dysfunction | 1 (1·6%) | 0 | 0 | 0 | 0 | 0 |
| Cardiac Dysfunction (excluding peripheral oedema)p | 5 (7·8%) | 1 (1·6%) | 0 | 4 (6·2%) | 0 | 0 |
| LVEF (lowest post-baseline) | ||||||
| Nq | 51 | 32 | ||||
| LVEF <50% | 6 (11·8%) | 3 (9·4%) | ||||
Abbreviations: LVEF = left ventricular ejection fraction
Adverse events and clinical laboratory toxicity were graded according to the National Cancer Institute Common Terminology Criteria for Adverse Events, version 4.0.
The adverse events listed here were reported in at least 15% of patients in the olaratumab + doxorubicin group, except as noted in footnote k. Included are individual preferred terms from the Medical Dictionary for Regulatory Activities [MedDRA] and certain consolidated terms combining clinically synonymous MedDRA preferred terms.
Consolidated term comprising the following preferred terms: fatigue, asthenia.
Consolidated term comprising the following preferred terms: neutropenia, neutrophil count decreased.
Some patients reported both neutropenia and leukopenia.
Consolidated term comprising the following preferred terms: mucosal inflammation, oropharyngeal pain, stomatitis.
Consolidated term comprising the following preferred terms: anemia, hemoglobin decreased.
Consolidated term comprising the following preferred terms: leukopenia, white blood cell count decreased.
Consolidated term comprising the following preferred terms: abdominal pain upper, abdominal pain, abdominal pain lower.
Preferred terms reported were: arthralgia, back pain, spasms, musculoskeletal chest pain, myalgia, pain in extremity.
These events are included here because they were considered clinically important.
Includes all preferred terms within the MedDRA system organ class of Infections and Infestations.
Consolidated term comprising the following preferred terms (from AESI): hypersensitivity, infusion-related reaction, face edema.
Includes individual preferred terms from the Medical Dictionary for Regulatory Activities (MedDRA).
Some patients reported more than one cardiac dysfunction event term.
No patients with reported AE of peripheral oedema had any reported AEs to suggest cardiac dysfunction.
Number of patients assessed at baseline and at least one post-baseline time point.
No. of patients (%) for musculoskeletal pain was 5 (7.8) for grade ≥3 in the olaratumab+doxorubicin group.
No. of patients (%) for musculoskeletal pain was 1 (1.5) for grade ≥3 in the doxorubicin group.
Treatment-related adverse events of grade 3 or higher and serious adverse events of grade 3 or higher were more frequent with olaratumab+doxorubicin than doxorubicin (43 [67%] vs 36 [55%] and 27 [42%] vs 22 [34%]) (table 4). Fatigue and neutropenia of grade 3 or higher were more frequent with olaratumab+doxorubicin (6 [9%] and 35 [55%]) than with doxorubicin (2 [3%] and 22 [34%]). However, the incidence of febrile neutropenia was similar in both groups: olaratumab+ doxorubicin (8 [13%]) vs doxorubicin (9 [14%]). The percentage of patients who discontinued treatment because of an adverse event was lower with olaratumab+doxorubicin than with doxorubicin (8 [13%] vs 12 [19%]).
Of the 129 treated patients in the phase 2 portion of the study, 39 (61%) in the olaratumab+doxorubicin group and 51 (79%) in the doxorubicin group had died at the time of data cutoff. In the olaratumab+doxorubicin group, death was attributed to disease progression in 38 patients and an unknown cause in one patient. In the doxorubicin group, death was attributed to disease progression in 44 patients, adverse events in six patients (aspirational pneumonia, respiratory failure, sepsis, septic shock, and small bowel obstruction), and an unknown cause in one patient. Doxorubicin-related toxicities (neutropenia, mucositis, nausea, vomiting, and diarrhea) were more frequent in patients treated with the combination but did not result in an increased number of febrile neutropenia events, hospitalisations (table S14), treatment discontinuations, or deaths.
The incidence of cardiac dysfunction (consolidated term comprised of peripheral edema, ejection fraction decreased, congestive cardiac failure, hepatojugular reflux, jugular vein distention and left ventricular dysfunction; any grade) was 23% (15 patients) with olaratumab+doxorubicin and 17% (11 patients) with doxorubicin (table 4). Excluding the patients with peripheral edema (none reported other adverse events to suggest cardiac dysfunction), the total incidence of cardiac dysfunction was 8% (5 patients) with olaratumab+doxorubicin and 6% (4 patients) with doxorubicin. Changes in left ventricular ejection fraction from baseline are summarized in table 4.
Immunogenicity
Eighty-five patients were evaluable for the presence or absence of antidrug antibodies. The overall incidence of treatment-emergent antidrug antibodies was 6% (5 of 85) (table S15); no effect of immunogenicity on safety or pharmacokinetics was observed.
PDGFRα Assessment and Outcomes Comparison
Analysis of PDGFRα-expression showed that 88% (doxorubicin+olaratumab) and 88% (doxorubicin) of tumours were PDGFRα-positive (Table 1). However, this assay was subsequently found to have poor specificity for PDGFRα, also detecting PDGFRβ, precluding meaningful data analysis. Reanalysis of study tumour samples with an assay with better specificity for PDGFRα demonstrated that 33% (doxorubicin+olaratumab) and 34% (doxorubicin) of tumours were positive for PDGFRα, consistent with a recent study.14 The interaction effect between PDGFRα expression (positive or negative) and treatment was not significant for either overall or progression-free survival (interaction p-values 0·3209 and 0·5924).
Discussion
The combination of olaratumab plus doxorubicin improved both progression-free and overall survival compared with the standard-of-care doxorubicin in patients with advanced soft tissue sarcoma. Analyses of pretreatment, concomitant, and posttreatment factors revealed no consistent imbalances that could have meaningfully affected the robustness of the study results. Treatment arms were well-balanced for line of treatment, performance status, and prognostic factors implicated in soft tissue sarcoma.15 Although the rate of discontinuation because of adverse events was higher in the control arm, most were considered serious adverse events, and single-agent doxorubicin performed as expected from historical data.4,16–18 A sensitivity analysis of patients discontinuing study treatment because of adverse events or symptomatic progressive disease within the first 8 cycles, or patients completing fewer than 4 cycles of doxorubicin, showed hazard ratios similar to the overall study, making these factors an unlikely source of bias for the observed overall survival results. The number of poststudy lines of treatment were relatively well balanced on both arms with modest imbalances in some chemotherapeutic agents. Sensitivity analysis censoring patients at the start of any new anti-cancer treatment or upon starting select chemotherapeutic agents showed hazard ratios similar to the overall study. It also should be noted that none of these agents have been demonstrated to improve median overall survival in the broad soft tissue sarcoma population. Lastly, the early separation of the overall survival curves is consistent with an effect of the combination rather than confounding post treatment factors.
The magnitude of improvement observed in median overall survival with olaratumab and doxorubicin (80%; 11·8 months) was greater than that observed in progression-free survival (61%; 2·5 months). This finding suggests that the inhibitory effect of olaratumab on tumour and stromal PDGFRα signaling may persist beyond the immediate treatment period. While tumour PDGFRα expression alone did not correlate with outcome, tumour samples available for study were a heterogeneous mixture of archival primary and metastatic tumours. Ongoing and future work will explore both tumour and stromal expression of PDGFRα and related ligands and more fully characterize immunohistochemical criteria for PDGFRα positivity.
Our findings are particularly notable given the limited progress in improving median overall survival in patients with advanced soft tissue sarcoma. Most patients are treated with traditional regimens of doxorubicin or doxorubicin in combination with ifosfamide; however, the prognosis for patients with metastatic disease remains poor as the efficacy of these and other treatment options are limited. In a recent phase 3 study by the European Organisation for Treatment of Cancer Soft Tissue and Bone Sarcoma Group, doxorubicin plus high-dose ifosfamide improved progression-free survival and response rates over doxorubicin alone.4 These important palliative outcomes were achieved at the expense of greater drug toxicity and without an improvement in median overall survival over doxorubicin alone (14·3 vs 12·8 months, respectively [HR, 0·83; P=0·076]). Other recent combination and novel-agent studies also did not show improvement in overall survival over doxorubicin alone,5,17,19–22 reinforcing the challenging nature of improving outcomes in advanced soft tissue sarcoma.
In conclusion, this study of olaratumab in combination with doxorubicin met its predefined, statistical, primary endpoint for progression-free survival and achieved a highly statistically significant improvement of 11·8 months in median overall survival over doxorubicin alone. Importantly, the improvement in median overall survival was achieved without an increase in serious toxicity, despite a higher cumulative exposure to doxorubicin. Although the rate of some doxorubicin-associated toxicities such as neutropenia and mucositis were higher in the combination arm, this did not lead to a higher rate of febrile neutropenia, infection, hospitalisation, or treatment-related mortality. Altogether, the pronounced survival benefit, along with an acceptable safety profile including cardiac safety, represents a positive benefit-risk profile for olaratumab+doxorubicin in the treatment of patients with soft tissue sarcoma.
Supplementary Material
Panel: Research in context.
Evidence before this study
A detailed PubMed search was performed in English to identify all randomized trials involving single agent doxorubicin from 1980 to February 25, 2016. The terms utilized in the search included: “soft tissue”, “sarcoma”, “doxorubicin”, “randomized”, and “trial”. We identified 19 randomized phase 2 or phase 3 clinical trials, none of which showed an overall survival advantage of single agent or combination therapy over doxorubicin alone.
Added value of this study
Our study is the first randomized study to show increased survival for patients with soft tissue sarcoma treated with an agent added to doxorubicin therapy. In our study, the combination of olaratumab plus doxorubicin improved both progression-free and overall survival compared with the standard of care doxorubicin in patients with advanced soft tissue sarcoma. The improvement of 11.8 months in median overall survival is highly significant, suggesting a potential paradigm shift in our treatment.
Implications of all the available evidence
The magnitude of improvement observed in median overall survival with olaratumab and doxorubicin was 80% (11·8 months) and that in progression-free survival was 61% (2·5 months), suggesting that the inhibitory effect of olaratumab on tumour and stromal PDGFRα signaling may persist beyond the immediate treatment period. These clinical results are being confirmed in a large international randomized phase 3 study. Further refinement of the understanding of PDGFRα in the context of tumour and stroma is currently a focus of ongoing investigations.
Acknowledgments
This study was funded by Eli Lilly and Company. We thank Patrick Peterson, Eli Lilly and Company, for statistical assistance and Joseph Giaconia, INC Research, for writing assistance.
Abbreviations
- CI
confidence interval
- Cmax
maximum serum concentration
- Cmin
trough serum concentration
- ECOG
Eastern Cooperative Oncology Group
- HR
hazard ratio
- LVEF
left ventricular ejection fraction
- MedDRA
Medical Dictionary for Regulatory Activities
- PDGF
platelet-derived growth factor
- PDGFR
platelet-derived growth factor receptor
- PDGFRα
platelet-derived growth factor receptor α
Footnotes
Disclosures Qin, Shahir, Cronier, Ilaria, and Conti are employees of Eli Lilly and Company. Cosaert (C) and Shah (S) were employees of ImClone Systems (now Eli Lilly and Company) during study design (C,S), conduct (C,S), and analysis (C).
Contributors
AQ was involved in the study design and led the statistical analyses. WDT, RLJ, BAVT, BC, ADE, DA, MA, MMC, MBL, GP, MRH, GDS, and GKS were involved in data collection. DMC led the pharmacokinetic analyses. All authors were involved in the interpretation of the data. WDT wrote the first draft of the manuscript, and all authors contributed to subsequent drafts.
Declaration of interests
WDT reports personal fees from Eli Lilly and Company, Advaxis, Ariad, Boehringer Ingelheim, EMD Serono, Daiichi Sankyo, Morphotek, and Plexxikon. RLJ has received a grant(s) from ImClone. BAVT served on an advisory board for Eli Lilly and Company. BC reports personal fees from Eli Lilly and Company, Amgen, Astella, Genentech, and BMS. DA has received a grant(s) from Eli Lilly and Company. MA reports personal fees from EMD Serono, Janssen, and Novartis. GP reports personal fees from Bristol-Myers Squibb. GDS was an employee of Novartis during the conduct of the study. AQ, AS, DMC, RI, IC are employees of and stockholders in Eli Lilly and Company. JC was an employee of Eli Lilly and Company during the conduct of the study. ADE, MMC, MBL, MRH, and GKS declare no competing interests.
References
- 1.D’Angelo SP, Tap WD, Schwartz GK, Carvajal RD. Sarcoma immunotherapy: past approaches and future directions. Sarcoma. 2014;2014:391967. doi: 10.1155/2014/391967. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Sharma S, Takyar S, Manson SC, Powell S, Penel N. Efficacy and safety of pharmacological interventions in second- or later-line treatment of patients with advanced soft tissue sarcoma: a systemic review. BMC Cancer. 2013;13:385. doi: 10.1186/1471-2407-13-385. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Singer S, Demetri GD, Baldini EH, Fletcher CD. Management of soft-tissue sarcomas: an overview and update. Lancet Oncol. 2000;1:75–85. doi: 10.1016/s1470-2045(00)00016-4. [DOI] [PubMed] [Google Scholar]
- 4.Judson I, Verweij J, Gelderblom H, et al. Doxorubicin alone versus intensified doxorubicin plus ifosfamide for first-line treatment of advanced or metastatic soft-tissue sarcoma: a randomised controlled phase 3 trial. Lancet Oncol. 2014;15:415–23. doi: 10.1016/S1470-2045(14)70063-4. [DOI] [PubMed] [Google Scholar]
- 5.Ryan CW, Schoffski P, Merimsky O, et al. PICASSO 3: a phase 3 international randomized double blind placebo-controlled study of doxorubicin plus palifosfamide vs. doxorubicin plus placebo for patients in first-line for metastatic soft tissue sarcoma. Eur J Cancer. 2013;49(suppl 2):S876. abstract 3802. [Google Scholar]
- 6.Ng F, Boucher S, Koh S, et al. PDGF, TGF-beta, and FGF signaling is important for differentiation and growth of mesenchymal stem cells (MSCs): transcriptional profiling can identify markers and signaling pathways important in differentiation of MSCs into adipogenic, chondrogenic, and osteogenic lineages. Blood. 2008;112:295–307. doi: 10.1182/blood-2007-07-103697. [DOI] [PubMed] [Google Scholar]
- 7.Chen CY1, Liu SH1, Chen CY1, Chen PC1, Chen CP2. Human placenta-derived multipotent mesenchymal stromal cells involved in placental angiogenesis via the PDGF-BB and STAT3 pathways. Biol Reprod. 2015;93:103. doi: 10.1095/biolreprod.115.131250. [DOI] [PubMed] [Google Scholar]
- 8.Paulsson J, Ehnman M, Östman A. PDGF receptors in tumour biology: prognostic and predictive potential. Future Oncol. 2014;10:1695–708. doi: 10.2217/fon.14.83. [DOI] [PubMed] [Google Scholar]
- 9.Ostman A, Heldin CH. Involvement of platelet-derived growth factor in disease: development of specific antagonists. Adv Cancer Res. 2001;80:1–38. doi: 10.1016/s0065-230x(01)80010-5. [DOI] [PubMed] [Google Scholar]
- 10.Loizos N, Xu Y, Huber J, et al. Targeting the platelet-derived growth factor receptor alpha with a neutralizing human monoclonal antibody inhibits the growth of tumour xenografts: implications as a potential therapeutic target. Mol Cancer Ther. 2005;4:369–79. doi: 10.1158/1535-7163.MCT-04-0114. [DOI] [PubMed] [Google Scholar]
- 11.Tonra J, Deevi D, Carrick F, et al. Enhanced antitumour activity of anti-platelet derived growth factor receptor alpha antibody, IMC-3G3, in combination with doxorubicin against a human soft-tissue sarcoma xenograft model. Presented at the AACR-NCI-EORTC Molecular Targets and Cancer Therapeutics International Conference; Philadelphia PA. November 14–18, 2005; Poster A67. [Google Scholar]
- 12.Pocock SJ, Simon R. Sequential treatment assignment with balancing for prognostic factors in the controlled clinical trial. Biometrics. 1975;31:103–15. [PubMed] [Google Scholar]
- 13.Eisenhauer EA, Therasse P, Bogaerts J, et al. New response evaluation criteria in solid tumours: revised RECIST guideline (version 1.1) Eur J Cancer. 2009;45:228–47. doi: 10.1016/j.ejca.2008.10.026. [DOI] [PubMed] [Google Scholar]
- 14.Movva S, Wen W, Chen W, et al. Multi-platform profiling of over 2000 sarcomas: identification of biomarkers and novel therapeutic targets. Oncotarget. 2015;6:12234–47. doi: 10.18632/oncotarget.3498. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.O’Sullivan B, Pisters PW. Staging and prognostic factor evaluation in soft tissue sarcoma. Surg Oncol Clin N Am. 2003;12:333–53. doi: 10.1016/s1055-3207(03)00011-5. [DOI] [PubMed] [Google Scholar]
- 16.Bramwell VH, Anderson D, Charette ML. Doxorubicin-based chemotherapy for the palliative treatment of adult patients with locally advanced or metastatic soft-tissue sarcoma: a meta-analysis and clinical practice guideline. Sarcoma. 2000;4(3):103–12. doi: 10.1080/13577140020008066. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Lorigan P, Verweij J, Papai Z, et al. Phase III trial of two investigational schedules of ifosfamide compared with standard-dose doxorubicin in advanced or metastatic soft tissue sarcoma: a European Organisation for Research and Treatment of Cancer Soft Tissue and Bone Sarcoma Group Study. J Clin Oncol. 2007;25:3144–50. doi: 10.1200/JCO.2006.09.7717. [DOI] [PubMed] [Google Scholar]
- 18.Riedel RF. Systemic therapy for advanced soft tissue sarcomas: highlighting novel therapies and treatment approaches. Cancer. 2012 Mar 15;118(6):1474–85. doi: 10.1002/cncr.26415. Epub 2011 Aug 11. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Bui-Nguyen B, Ray-Coquard I, Chevreau C, et al. High-dose chemotherapy consolidation for chemosensitive advanced soft tissue sarcoma patients: an open-label, randomized controlled trial. Ann Oncol. 2012;23:777–84. doi: 10.1093/annonc/mdr282. [DOI] [PubMed] [Google Scholar]
- 20.Chawla SP, Papai Z, Mukhametshina G, et al. First-line aldoxorubicin vs doxorubicin in metastatic or locally advanced unresectable soft-tissue sarcoma: a phase 2b randomized clinical trial. JAMA Oncol. 2015:1–9. doi: 10.1001/jamaoncol.2015.3101. [DOI] [PubMed] [Google Scholar]
- 21.Fayette J, Penel N, Chevreau C, et al. Phase III trial of standard versus dose-intensified doxorubicin, ifosfamide and dacarbazine (MAID) in the first-line treatment of metastatic and locally advanced soft tissue sarcoma. Invest New Drugs. 2009;27:482–9. doi: 10.1007/s10637-008-9217-1. [DOI] [PubMed] [Google Scholar]
- 22.Le Cesne A, Judson I, Crowther D, et al. Randomized phase III study comparing conventional-dose doxorubicin plus ifosfamide versus high-dose doxorubicin plus ifosfamide plus recombinant human granulocyte-macrophage colony-stimulating factor in advanced soft tissue sarcomas: a trial of the European Organization for Research and Treatment of Cancer/Soft Tissue and Bone Sarcoma Group. J Clin Oncol. 2000;18:2676–84. doi: 10.1200/JCO.2000.18.14.2676. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.