

Abstract
Background
A number of randomized controlled trials (RCTs) have investigated the role of perioperative corticosteroids in rhinoplasty. Each of these trials however has an insufficient sample sizes to reach definitive conclusions and detect harms. Three recent reviews have analyzed edema and ecchymosis outcomes following rhinoplasty; each arrived at a different conclusion and recommendation.
Objective
To estimate the effectiveness of systemic perioperative corticosteroid treatment compared to placebo for clinical outcomes in rhinoplasty using a methodologically rigorous meta-analysis.
Methods
Electronic databases were searched without language restriction. Included trials were randomized controlled trials of systemic perioperative corticosteroid treatment vs placebo in rhinoplasty evaluating at least one of: edema, ecchymosis, bleeding, cosmetic outcome, and patient satisfaction. The Cochrane risk of bias tool was applied to included trials, and the quality of evidence for each outcome was assessed using the GRADE approach.
Results
Analyses included 336 patients from eight trials. Perioperative corticosteroids reduced the worst edema (SMD: −1.03, 95%CI −1.30 to −0.76, P < .001) and ecchymosis (SMD: −0.78, 95%CI −1.09 to 0.47, P < .001) after rhinoplasty. At one day postoperative, a single dose of perioperative corticosteroid reduced edema (SMD −1.15, 95%CI −1.42 to −0.87, P < .001) and ecchymosis (SMD −0.79, 95%CI −1.05 to −0.52, P < .001). No clinical benefit in edema or ecchymosis was found seven days postoperatively, nor did intraoperative bleeding increase.
Conclusions
There is high quality evidence to support perioperative systemic corticosteroid treatment in rhinoplasty to reduce short-term edema and ecchymosis without increased intraoperative bleeding. These findings are not present at seven days. For future trials, we suggest evaluation of patient satisfaction, and correlation with long-term cosmetic outcome.
Level of Evidence: 2

Rhinoplasty is challenging due to variable nasal anatomy prohibiting a standardized procedure.1 Patient satisfaction rates are lower2 compared to other cosmetic procedures. Given the forces required to reshape the nose, complications involving the skin and soft tissues occur in 10% of procedures.3 Postoperative edema and eccyhmosis are both patient-important and surgeon-important. To patients, these soft tissue effects (edema, ecchymosis) are obvious in the early postoperative period.3 To surgeons, these complications are purported to impact final aesthetic outcome.4
Perioperative administration of systemic corticosteroids (steroids) was introduced to facial surgery to reduce postoperative edema and improve skin flap survival.5-7 Steroids limit vascular permeability, providing anti-inflammatory properties.8 Intravenous steroids have a half-life of 72 hours, with benefit reported seven days postoperatively.9 Steroids however, are anecdotally reported to increase intraoperative bleeding.10 Further, known systemic risks are associated with short term treatment,4 most notably avascular necrosis.1
Early corticosteroid reports were followed by large series reporting subjective diminished edema in rhinoplasty and other facial surgical patients, without adverse events.11-13 However, case series lack control groups, are subject to bias, and do not allow causal inferences. Several RCTs have investigated the role of steroids in rhinoplasty.8-11,14-21 Long-term outcomes are unclear.
A survey in the United Kingdom revealed that 24% of cosmetic surgeons reported administration of preoperative corticosteroids in rhinoplasty.1 Of these surgeons, approximately half (54%) administer a single perioperative dose of dexamethasone (8 mg). Only 12% of respondents administer steroids for one or more days postoperatively.
Three recent published reviews on this topic provide discordant conclusions. Hatef et al3 pooled data and reported a seven-day reduction in edema and ecchymosis. Youssef et al22 pooled data and concluded no benefit to edema after the third postoperative day. Pulikkotil et al4 qualitatively reviewed the literature, and concluded edema and ecchymosis reduction are transient and risks of steroid administration outweigh benefits. Given how common rhinoplasty procedures are, the authors conducted this systematic review and meta-analysis to resolve conflicting conclusions generated by prior reviews, using the most rigorous current methods in meta-analysis research. The objective of this meta-analysis is to determine the effect of perioperative steroids on postoperative edema, ecchymosis, patient satisfaction, and cosmetic outcome in patients undergoing rhinoplasty.
METHODS
Personnel
None of the authors has a conflict of interest in any of the products, devices, or drugs mentioned in this manuscript.
Trial Eligibility
This review included RCTs comparing systemic perioperative steroid treatment to placebo or no treatment among adults undergoing primary rhinoplasty for any indication. Outcomes were edema, ecchymosis, intraoperative bleeding, cosmetic outcome, and patient satisfaction. Trials in any language were eligible.
Data Sources
Electronic search strategy was reviewed with a health science research librarian, last updated 1 April 2013: MEDLINE (1946-present), EMBASE (1980 to 2013), and Cochrane Register for Randomized Controlled Trials (2013, Issue 4) (a document containing the MEDLINE and EMBASE search strategies can be viewed as Supplementary Material at www.aestheticsurgeryjournal.com). Gray literature review included bibliographies of included trials and systematic reviews, trials in progress (ClinicalTrials.gov, Controlled-Trials.com), and conference proceedings for the past three years (AAPS, ASPS, CSPS, IPRAS, EURAPS).
Trial Selection
Two reviewers (CJC and SHV) independently screened titles and abstracts in duplicate. Relevant reports were retrieved. The same two reviewers screened full text reports in duplicate, using a standardized electronic eligibility form. Disagreements were resolved through discussion. Cohen’s unweighted kappa was calculated for full- ext agreement on inclusion.
Data Extraction and Quality Assessment
One reviewer (CJC) extracted trial, patient, treatment, and outcome characteristics from all eligible full- ext reports using electronic forms with a data dictionary designed a priori. Data were checked by a second reviewer (SHV). The Cochrane risk of bias tool was applied in duplicate by the same two reviewers to assess the following RCT quality and methodological safeguards: randomization sequence generation, allocation concealment, blinding of subjects, research personnel and outcome assessment, incomplete outcome data, selective reporting, and other bias, including trial funding.23 The Grading of Recommendations Assessment, Development and Evaluation (GRADE) approach24 was applied independently in duplicate by the same two reviewers to rate the quality of evidence for each outcome. RCT outcomes began as high-quality, and were downgraded by one level for specific factors defined a priori25: risk of bias (blinding), inconsistency (unexplained heterogeneity), imprecision (optimal information size, sensitivity analyses), publication bias, and indirectness. In cases where uncertain terms such as double-blind were employed, risk of bias assessment was guided by Akl et al’s26 algorithm.
Data Synthesis and Analysis
Data were analyzed in Review Manager 5.2.27 Analysis employed pooled standardized mean differences (SMD) with 95% confidence intervals. Clinical heterogeneity was incorporated into a random effects model. In extracting outcomes from included RCTs, data were measured from graphs if necessary. If upper and lower eyelid outcomes were reported separately, results were averaged. Missing standard deviations (SD) were calculated from existing data; if unable to calculate, the highest reported SD from another trial for each outcome was used as the most conservative estimate. If trials randomized patients to multiple steroid groups vs a single control group, steroid groups were combined for a single pair-wise comparison.28 For subgroup analyses where steroid groups were divided within a trial, the control group was split to avoid double-counting these subjects and creating a unit-of-analysis error.28 Steroid equivalency was established a priori where Dexamethasone 8 mg equals Betamethasone 8-10 mg, and Methylprednisolone 45-50 mg.
Minimal clinically important differences (MCID) for outcomes were not identified in the literature review. Therefore, the results were interpreted with Cohen’s effect size. Standardized mean differences were calculated, where a small effect size was >0.2, medium >0.5 and large >0.8.29 Optimal information size was calculated to determine if each analysis was adequately powered. GRADEpro was employed to summarize findings.30 Sources of clinical heterogeneity were identified a priori in a survey1: dosage of corticosteroid (baseline dexamethasone 8-10 mg vs higher) and length of treatment (perioperative only vs continued postoperatively). We hypothesized multiple days of treatment and higher doses would demonstrate a larger treatment effect. Heterogeneity was explored with the I2 statistic31 to investigate inconsistency in trial outcomes; outcomes with I2 over 40% were explored with subgroup analyses. To assess publication bias, funnel plots were analyzed if at least ten trials were found; analyses lack power with fewer trials.31
RESULTS
Search criteria identified 190 potentially relevant citations; 12 citations were selected for full text review. Eight trials were eligible for inclusion (Figure 1).8-10,15-17,19,20 Four trials were excluded (Table 1).14,18,32,33 Unweighted kappa for inter-rater agreement was 1.0. Five trials reported edema and/or ecchymosis separately for upper and lower eyelids.8,15-17,19 Standard deviation was calculated from other data reported in one trial.8 Edema and ecchymosis data were extrapolated from graphs in two trials.15,16 Standard deviations were missing in two trials.15,16 Data from Koc et al20 could only be pooled for the variable of intraoperative bleeding; mean edema and ecchymosis could not be calculated from data reported.
Figure 1.
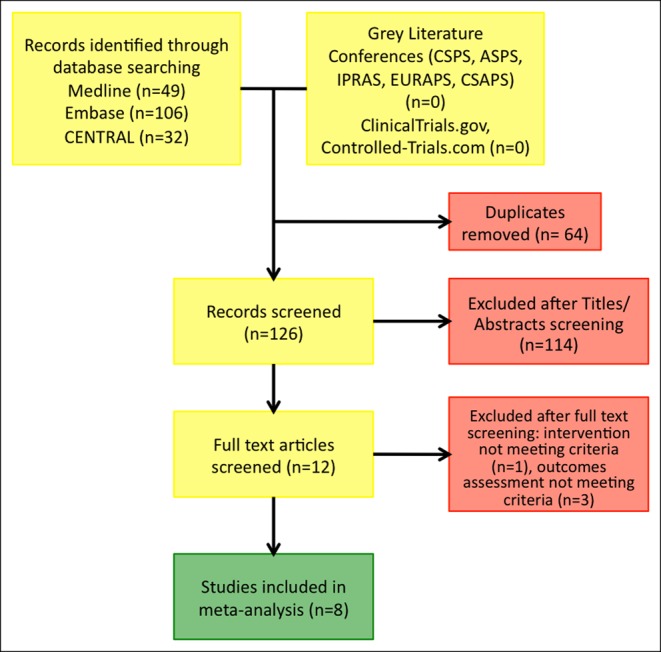
Flow diagram of search and study selection.
Table 1.
Excluded Trial Characteristics
| Trial | Reason for exclusion |
|---|---|
| Alajmi et al, 200933 | Edema and ecchymosis combined on a single three point scale |
| Berinstein et al, 199814 | Edema measured radiologically on CT scan |
| Racic et al, 200032 | Timing of outcome assessment not reported |
| Totonchi et al, 200718 | Number of patients in each arm not reported |
Characteristics
Trial characteristics8-10,15-17,19,20 are listed in Table 2, patient characteristics in Table 3, and treatment and outcome characteristics in Table 4.
Table 2.
Included Trial Characteristics
| Trial | Country | Duration | Blinding | Surgeon expertise | Protocol registration | Sponsorship/conflict of interest |
|---|---|---|---|---|---|---|
| Griffies et al, 198910 | USA | 1986-1987 | Patient, surgeon | PGY 4/5 residents | No | No |
| Hoffmann et al, 19918 | USA | NR | Patient, surgeon | Performed or supervised by 1 staff | No | No |
| Kara et al, 199915 | Turkey | NR | Patient, surgeon | 1 of 2 Staff surgeons | No | No |
| Kargi et al, 200316 | Turkey | 2000-2002 | Patient, surgeon | 1 of 3 Staff surgeons | No | No |
| Gurlek et al, 20069 | Turkey | NR | Patients, surgeon, observers | Single staff surgeon | No | No |
| Ozdel et al, 200619 | Turkey | NR | Patient, surgeon | NR | No | No |
| Gurlek et al, 200917 | Turkey | NR | Double-blind | Single staff surgeon | No | No |
| Koc et al, 201120 | Turkey | NR | Patient, surgeon | NR | No | No |
NR, not reported.
Table 3.
Patient Characteristics
| Trial | Treatment (n) | Control (n) | Age range | Rhinoplasty | Splint |
|---|---|---|---|---|---|
| Griffies et al, 198910 | 16 | 14 | 18-45 | Osteotomies | External with packing |
| Hoffmann et al, 19918 | 34 | 25 | 15-70 | 20 open, 29 closed | NR |
| Kara et al, 199915 | 38 | 17 | NR | Open and closed, all with osteotomies | Packing |
| Kargi et al, 200316 | 50 | 10 | NR | Closed | Packing |
| Gurlek et al, 20069 | 24 | 8 | 22-30 | Open, osteotomies | External cast |
| Ozdel et al, 200619 | 15 | 15 | NR | Open and closed, all with osteotomies | Packing |
| Gurlek et al, 200917 | 32 | 8 | 19-35 | Open, osteotomies | External cast and internal splints |
| Koc et al, 201120 | 30 | 10 | NR | Osteotomies | External cast and internal splints |
NR, not reported.
Table 4.
Trial Intervention and Outcome Characteristics
| Trial | Perioperative steroid | Postoperative steroid | Outcomes used | Follow-up | Outcome assessor |
|---|---|---|---|---|---|
| Griffies et al, 198910 | IMMEDIATE PREOP: Dexamethasone 10 mg IV | No | Edema, ecchymosis | 1 day | Surgeon |
| Hoffmann et al, 19918 | INTRAOP: Dexamethasone 10 mg IV | In all (n = 34), 5 day taper, 50 mg prednisone by 10 mg daily | Edema, ecchymosis | 1,4,7 days | 2 blinded residents/fellows or staff, may have been operating surgeons |
| Kara et al, 199915 | IMMEDIATE PREOP or IMMEDIATE POSTOP: dexamethasone 10 mg IV | No | Edema, ecchymosis, blood loss | Daily 1-9 days | 2 surgeons |
| Kargi et al, 200316 | PREOP, IMMEDIATE PREOP or POSTOP: dexamethasone 8 mg | In 2 groups, (n = 20), dexamethasone 8 mg×2 days | Edema, ecchymosis, blood loss | 2,5,7,10 days | NR |
| Gurlek et al, 20069 | IMMEDIATE PREOP: betamethasone 8 mg, dexamethasone 8 mg, methylprednisolone 40 mg | In 2 groups (n = 12) same as peri ×3 days | Edema, ecchymosis | 1,3,7 days | Blinded observers |
| Ozdel et al, 200619 | IMMEDIATE PREOP: Dexamethasone 10 mg IV | No | Edema, ecchymosis, blood loss | 1,2 days | Another physician unaware of what was administered |
| Gurlek et al, 200917 | IMMEDIATE PREOP: methylprednisolone 250 mg (2 groups) methylprednisolone 500 mg (2 groups) | In 2 groups (n = 16), 250 and 500 mg daily×3 days | Edema, ecchymosis | 1,3,7 days | Blinded observers |
| Koc et al, 201120 | IMMEDIATE PREOP: 1 mg/kg methylprednisolone IV, 3 mg/kg methylprednisolone IV | No | Blood loss | Intraop | 3 independent observers |
NR, not reported.
Bias
Risk of bias categories for the included trials are summarized in Table 5. There were too few trials to analyze publication bias with a funnel plot.
Table 5.
Risk of Bias Characteristics for All Included Trials
| Griffies et al, 198910 | Hoffmann et al, 19918 | Kara et al, 199915 | Kargi et al, 200316 | Gurlek et al, 20069 | Ozdel et al, 200619 | Gurlek et al, 200917 | Koc et al, 201120 | |
|---|---|---|---|---|---|---|---|---|
| Random sequence generation (selection bias) | Unclear | Unclear | Unclear | Unclear | Unclear | Unclear | Unclear | Unclear |
| Allocation concealment (selection bias) | Unclear | Unclear | Unclear | Unclear | Unclear | Unclear | Unclear | Unclear |
| Blinding of participants and personnel (performance bias) | Low | Low | Low | Low | Low | Low | Low | Low |
| Blinding of outcome assessment (detection bias) | Low | Low | Low | Low | Low | Low | Low | Low |
| Incomplete outcome data (attrition bias) | Low | Unclear | Unclear | Unclear | Unclear | Unclear | Unclear | Low |
| Selective reporting (reporting bias) | Unclear | Unclear | Unclear | Unclear | Unclear | Unclear | Unclear | Unclear |
| Other bias | Low | Low | Low | Low | Low | Low | Low | Low |
Low, low risk of bias; Unclear, unclear risk of bias.
Worst Edema and Ecchymosis
The most severe (worst) edema and ecchymosis experienced by patients in the postoperative period were reported for 296 patients in seven trials.8-10,15-17,19 The worst scores were determined by the highest scale outcome measure for both edema and ecchymosis reported in the trial. Timing of worst outcome ranged from postoperative days one to three.
Perioperative steroids demonstrated a statistically significant reduction in worst edema, SMD: −1.03, 95%CI: −1.30 to −0.76, P < .001(Figure 2). This is a medium effect size. Perioperative steroids demonstrated a statistically significant reduction in worst ecchymosis, SMD: −0.78, 95%CI: −1.09 to −0.47, P < .001(Figure 3). This is a medium effect size. Results favor perioperative steroids to decrease the worst postoperative edema and ecchymosis patient’s experience. Quality for these outcomes is high.
Figure 2.

Most severe postoperative edema for corticosteroids vs placebo.
Figure 3.

Most severe postoperative ecchymosis for corticosteroids vs placebo.
Day 1 Edema and Eccyhmosis
Edema and ecchymosis at day one postoperatively were reported for 296 patients from seven trials.8-10,15-17,19
Perioperative steroids demonstrated a statistically significant reduction in edema at one day postoperatively, SMD: −1.15, 95%CI: −1.42 to −0.87, P < .001(Figure 4). This is a large effect size. Perioperative steroids demonstrated a statistically significant reduction in ecchymosis at day one postoperatively, SMD: −0.79, 95%CI: −1.05 to −0.52, P < .001(Figure 5). This is a medium effect size. Results favor perioperative steroids to decrease edema and ecchymosis at day one postoperatively. Quality for both outcomes is high.
Figure 4.

Day 1 postoperative edema for corticosteroids vs placebo.
Figure 5.

Day 1 postoperative ecchymosis for corticosteroids vs placebo.
Day 7 Edema and Ecchymosis
Edema and ecchymosis at day seven postoperatively were reported for 236 patients from five trials.8,9,15-17 In the study by Gürlek et al,17 high dose steroids (equivalent to dexamethasone 45 and 90 mg) were administered.
At the lowest end of the confidence interval, perioperative steroids demonstrated a small but statistically significant reduction in edema at day seven postoperatively, SMD: −0.60, 95%CI: −1.14 to −0.05, P = .03. However, I2 = 65% may represent substantial heterogeneity; the results of a subgroup analysis of perioperative only vs perioperative and a postoperative oral course are found in Figure 6. Perioperative administration alone demonstrated a clinically very small, but statistically significant reduction in edema at day seven postoperatively, SMD: −0.50, 95%CI: −0.96 to −0.04, P = .03, I2 = 0%. Conversely, postoperative continued steroid administration demonstrated no significant edema reduction, SMD: −0.66, 95%CI: −1.66 to 0.33, P = .19, I2 = 81%.
Figure 6.

Day 7 postoperative edema for corticosteroids vs placebo, subgroup analysis.
Perioperative steroids demonstrated no reduction in ecchymosis at day seven postoperatively, SMD: −0.29, 95%CI: −0.80 to 0.22, P = .26. Optimal information size was not met, indicating the pooled analysis was underpowered. I2 = 78% represents considerable heterogeneity. The results of a subgroup analysis of perioperative only vs perioperative and a postoperative oral course are found in Figure 7. Neither subgroup demonstrates a reduction in ecchymosis at day seven postoperatively. Overall, results do not favor perioperative steroids for edema or ecchymosis at day seven postoperatively. Addition of a postoperative oral course did not change results. Quality for this outcome is low.
Figure 7.

Day 7 postoperative ecchymosis for corticosteroids vs placebo, subgroup analysis.
Intraoperative Bleeding
Intraoperative bleeding was reported for 155 patients from three trials.15,16,20 Perioperative steroids did not demonstrate a difference in intraoperative bleeding, SMD: −0.25, 95%CI: −0.60 to 0.10, P = .16 (Figure 8). Overall, results do not support increased intra-operative bleeding as a harm of perioperative steroid treatment. Quality for this outcome is moderate.
Figure 8.

Intraoperative bleeding for corticosteroids vs placebo.
Cosmetic Outcome and Patient Satisfaction
No study reported these outcomes.
DISCUSSION
Summary of Main Results
Outcomes from eight RCTs are illustrated with the GRADE profile framework (Table 6). Results support a single systemic perioperative administration of steroids (dexamethasone 8 mg or equivalent) to reduce the worst edema and ecchymosis patients experience postoperatively, and edema and ecchymosis at day one postoperatively. Converting SMDs for each outcome to a standard 4-point scale, steroids reduce edema and ecchymosis by approximately 1 point at worst and at day one vs no treatment. We believe this is a clinically important difference; a difference a patient would notice as effective.
Table 6.
GRADE Quality Assessment for Each Outcome Reported in Meta-analysis
| Quality assessment |
No of Patients |
Effect |
Quality | Importance | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| No. of studies | Study design | Risk of bias | Inconsistency | Indirectness | Imprecision | Other considerations | Perioperative corticosteroids | Rhinoplasty | Relative (95% CI) | Absolute (95% CI) | ||
| Edema at Worst (follow up: 1-3 days; assessed with: 0-4 point scale) | ||||||||||||
| 7 | Randomized trials | Not seriousa | Not seriousf | Not serioush | Not seriousb | Noneh | 199 | 97 | - | SMD 1.03 lower (1.3 lower to 0.76 lower) | ⨁⨁⨁⨁ HIGH | IMPORTANT |
| Ecchymosis at Worst (follow up: 1-3 days; assessed with: 0-4 point scale) | ||||||||||||
| 7 | Randomized trials | Not seriousa | Not seriousf | Not serioush | Not seriousb | Noneh | 199 | 97 | - | SMD 0.78 lower (1.09 lower to 0.47 lower) | ⨁⨁⨁⨁ HIGH | IMPORTANT |
| Edema Day 1 (follow up: 1 days; assessed with: 0-4 point scale) | ||||||||||||
| 7 | Randomized trials | Not seriousa | Not seriousf | Not serioush | Not seriousb | Strong associationi | 199 | 97 | - | SMD 1.15 lower (1.42 lower to 0.87 lower) | ⨁⨁⨁⨁ HIGH | NOT IMPORTANT |
| Ecchymosis Day 1 (follow up: 1 days; assessed with: 0-4 point scale) | ||||||||||||
| 7 | Randomized trials | Not seriousa | Not seriousf | Not serioush | Not seriousb | Noneh | 199 | 97 | - | SMD 0.79 lower (1.05 lower to 0.52 lower) | ⨁⨁⨁⨁ HIGH | NOT IMPORTANT |
| Edema Day 7 (follow up: 7 days; assessed with: 0-4 point scale) | ||||||||||||
| 5 | Randomized trials | Not seriousa | Seriousd | Not serioush | Seriousc,e | Noneh | 168 | 68 | - | SMD 0.6 lower (1.14 lower to 0.05 lower) | ⨁⨁◯◯ LOW | IMPORTANT |
| Ecchymosis Day 7 (follow up: 7 days; assessed with: 0-4 point scale) | ||||||||||||
| 5 | Randomized trials | Not seriousa | Seriousd | Not serioush | Seriousc,e | Noneh | 168 | 68 | - | SMD 0.29 lower (0.8 lower to 0.22 higher) | ⨁⨁◯◯ LOW | IMPORTANT |
| Bleeding Intraoperative (assessed with: mL blood loss) | ||||||||||||
| 3 | Randomized trials | Not seriousa | Not serious | Not serioush | Seriousb,e | Noneh | 88 | 67 | - | SMD 0.25 lower (0.6 lower to 0.1 higher) | ⨁⨁⨁◯ MODERATE | NOT IMPORTANT |
MD, mean difference; RR, relative risk. aRandomization sequence generation, allocation concealment, and specific LTFU are not reported (authors were contacted unsuccessfully). All are likely reporting issues. bOptimal information size is met. cOptimal information size is NOT met. dConsiderable heterogeneity no explained by subgroup analyses. eClinical action differs at the upper and lower ends of the confidence interval. fResults are robust to upper and lower limits of imputing SDs. gFunnel plot would be under powered to detect asymmetry. hPatients and interventions reflect clinical practice, comparisons are direct. iLarge effect size, 0.87 at lower limit of 95%CI.
Heterogeneity (variation between studies) was limited in the short term and likely inconsequential; outcomes were precise and consistent, increasing our confidence in the results. The steroid doses administered in included RCTs were consistent with those employed in clinical practice, increasing our confidence in their clinical applicability.1 Quality of these outcomes was judged to be high, with confidence in medium to large effect size in short term outcomes.
Analyses at day seven postoperative demonstrated no consistent reduction in edema and ecchymosis, decreasing our confidence in concluding that steroids confer longer-term benefit. Fewer outcomes are reported at this time point; pooled analyses are underpowered. Considerable variability was encountered between studies (heterogeneity) for both edema and ecchymosis which was not explained by our planned subgroup analyses. Pooled outcomes are imprecise; the 95% confidence interval straddles the no effect line. These factors further decrease our confidence in concluding steroids still confer benefit at day seven. Edema and ecchymosis at day seven following a single perioperative steroid consistently demonstrate a statistically significant, but clinically insignificant reduction. Practically, patients are unlikely to notice a small effect size, translating into a benefit of less than 0.5 points on a standard 4-point scale for edema and ecchymosis. Moreover, results were consistent at day seven when a postoperative course of oral steroids was employed. There was no consistent evidence for benefit of a postoperative oral steroid course.
Systemic steroid treatment is not without risk. Authors cite potential hypothalamic-pituitary-adrenal axis suppression,17,19 and mood changes.1 Half of patients presenting with femoral head avascular necrosis have a history of systemic steroid administration.34
Gürlek et al17 was the only trial that employed high steroid doses, randomizing patients to the equivalent of dexamethasone 45 mg or 90 mg daily, for three days. While Gürlek et al was not powered to detect rare harms (ie, avascular necrosis), surgeons must consider potential side effects of high dose steroids.1 In our meta-analysis, we found steroids are not associated with an increase in intraoperative bleeding. The findings are consistent, although imprecise. Anecdotal reports of increased bleeding10 with perioperative steroid treatment are not confirmed by this review.
While we found edema and ecchymosis are reduced at worst, this result may not be clinically important. Unless perioperative steroids confer long-term benefit, patients may not recognize the improvement. The literature does not demonstrate that edema and ecchymosis at worst to be a surrogate of final cosmetic outcome. The ultimate effect of steroids on important rhinoplasty outcomes, such as patient satisfaction and final cosmesis are unknown.
Overall, the trials pooled in this review had an acceptable methodological quality, with however signs of poor reporting. This is similar to the overall trials published in plastic surgery.35 Randomization sequence generation and allocation concealment, for example, were not reported in any trial. Loss to follow-up was not specifically reported in six studies. Evidence was not downgraded for risk of bias since a reporting issue could not be ruled out.36
Agreements and Disagreements With Other Reviews
Two prior reviews on this topic pooled data. Hatef et al3 concluded perioperative steroids reduced edema and ecchymosis at days one and seven postoperatively, and concluded postoperative administration was superior to perioperative alone. Our meta-analysis only agrees with Hatef et al’s conclusions at day one. Youssef et al22 concluded steroids reduced edema at days one and three postoperatively, with no difference at day seven. Our meta-analysis agrees with their conclusion regarding these outcomes. Neither review included complications. Each review included data from four studies, however the four studies were not consistent. Hatef et al made a number of assumptions in pooling data without performing sensitivity analyses to test robustness, and ignored clinical heterogeneity in outcomes at day seven. Both Hatef et al and Youssef et al inappropriately analyzed studies with multiple treatment groups, leading to duplicity of data in analyses. Neither review performed steps in duplicate. Our review performed an exhaustive search of the existing literature. Further, we tested statistical assumptions and performed sensitivity analyses where missing data were imputed. Our review considered the clinical significance of very small, but statistically significant outcomes.
Pulikkottil et al4 performed a systematic review of corticosteroids in cosmetic surgery. The search was rigorous and selection was performed in duplicate. Twelve studies of various methodologies were described qualitatively; data were not pooled, but studies were accurately described as heterogeneous. Authors concluded benefits were transient, and potentially clinically relevant to patients. They cite balancing this possible transient benefit vs known rare risks. Our meta-analysis agrees with their analysis, however we employed rigorous methodological solutions to pool existing trials. The Cochrane Risk of Bias tool and GRADE approach were employed to assess the evidence for each outcome. Each element of decision making in generating conclusions was systematic and transparent to the reader.
Potential Biases in this Systematic Review
Reviewers assumed steroids were equivalent after dose adjustment, and pooled studies accordingly. It remains possible one steroid type confers greater benefit than others; alternatively, there may be a class effect where outcomes are unrelated to dose or individual steroid type.
Randomization sequence generation, allocation concealment, and loss to follow-up were not consistently reported. Multiple attempts to contact authors for clarification were unsuccessful. Reviewers did not downgrade for risk of bias, given that there was no definitive evidence of bias in these methodological steps. These concerns may reflect reporting issues, where these steps were not reported, but may have been employed.
CONCLUSIONS
Implications for Practice
There is high quality evidence that a single dose of systemic perioperative corticosteroids reduce edema and ecchymosis at day one, and when these symptoms are most severe (worst) following rhinoplasty. Outcomes at day one reflect a single perioperative dose equivalent to dexamethasone 8 mg intravenous. Outcomes at day seven demonstrate small and clinically insignificant reductions in edema and ecchymosis; the data are too imprecise and inconsistent to conclude benefit. The addition of a postoperative oral steroid course did not change results. Long-term cosmetic outcome and patient satisfaction are unavailable. There is moderate quality evidence that steroid treatment is not associated with increased intraoperative bleeding. Studies do not report systemic harms. The administration of high dose steroid (dexamethasone 45-90 mg) is limited to one small trial, and harms are unknown.
Perioperative steroid treatment remains an option for patients undergoing rhinoplasty to reduce short-term soft tissue side effects. Given the lack of long-term cosmetic and systemic harm outcomes, surgeon and patient preferences should be considered in decision-making.
Implications for Research
This review underscores the need for a large RCT testing perioperative corticosteroids in rhinoplasty, powered to determine whether there is any reduction in edema and ecchymosis at day seven (patient important), and the impact on final cosmetic outcome and patient satisfaction (patient and surgeon important) at one year.10 Potential harms would be better captured by a trial with more patients, and longer follow-up than currently exists in the literature.
Supplementary Material
This article contains supplementary material (including a video discussion between Dr. Felmont Eaves, EBM Hub Co-editor for Aesthetic Surgery Journal, and the authors) located online at www.aestheticsurgeryjournal.com.
Disclosures
The authors declared no potential conflicts of interest with respect to the research, authorship, and publication of this article.
Funding
Dr Coroneos has received the following academic grants to fund research fellowship training: 1) The Canadian Institutes of Health Research Master’s Award: Frederick Banting and Charles Best Award; 2) The Father Sean O’Sullivan Research Centre Award, St. Joseph’s Healthcare, Hamilton, Ontario, Canada; and 3) The Juravinski Surgical Fellowship, Department of Surgery, McMaster University, Hamilton, Ontario, Canada. The other authors received no financial support for the research, authorship, and publication of this article.
Supplementary Material
REFERENCES
- 1. Ofo E, Singh A, Marais J. Steroids in rhinoplasty: a survey of current UK otolaryngologists’ practice. J Laryngol Otol. 2006;1202:108-112. [DOI] [PubMed] [Google Scholar]
- 2. Constantian MB. What motivates secondary rhinoplasty? A study of 150 consecutive patients. Plast Reconstr Surg. 2012;1303:667-678. [DOI] [PubMed] [Google Scholar]
- 3. Hatef DA, Ellsworth WA, Allen JN, Bullocks JM, Hollier LH, Stal S. Perioperative steroids for minimizing edema and ecchymosis after rhinoplasty: a meta-analysis. Aesthet Surg J. 2011;316:648-657. [DOI] [PubMed] [Google Scholar]
- 4. Pulikkottil BJ, Dauwe P, Daniali L, Rohrich RJ. Corticosteroid use in cosmetic plastic surgery. Plast Reconstr Surg. 2013;1323:352e-360e. [DOI] [PubMed] [Google Scholar]
- 5. Habal MB, Powell RD. Experimental facial edema: treatment with methylprednisolone. J Surg Res. 1978;245:353-358. [DOI] [PubMed] [Google Scholar]
- 6. Schmidt JH, Caffee HH. The efficacy of methylprednisolone in reducing flap edema. Plast Reconstr Surg. 1990;866:1148-1151. [DOI] [PubMed] [Google Scholar]
- 7. Goldman IB, Freeman J, Bloom S. The effect of cortogen in rhinoplasty. Eye Ear Nose Throat Mon. 1952;3110:548-550. [PubMed] [Google Scholar]
- 8. Hoffmann DF, Cook TA, Quatela VC, Wang TD, Brownrigg PJ, Brummett RE. Steroids and rhinoplasty. A double-blind study. Arch Otolaryngol Head Neck Surg. 1991;1179:990-993; discussion 994. [DOI] [PubMed] [Google Scholar]
- 9. Gurlek A, Fariz A, Aydogan H, Ersoz-Ozturk A, Eren AT. Effects of different corticosteroids on edema and ecchymosis in open rhinoplasty. Aesthetic Plast Surg. 2006;302:150-154. [DOI] [PubMed] [Google Scholar]
- 10. Griffies WS, Kennedy K, Gasser C, Fankhauser C, Taylor R. Steroids in rhinoplasty. Laryngoscope. 1989;9911:1161-1164. [DOI] [PubMed] [Google Scholar]
- 11. Kittel H, Masing H. Corticosteroid therapy in rhinoplasty. Rhinology. 1976;144:163-166. [PubMed] [Google Scholar]
- 12. Wing LW. Tobispray in nasal surgery. Med J Aust. 1977;120:751-752. [DOI] [PubMed] [Google Scholar]
- 13. Habal MB. Prevention of postoperative facial edema with steroids after facial surgery. Aesthetic Plast Surg. 1985;92:69-71. [DOI] [PubMed] [Google Scholar]
- 14. Berinstein TH, Bane SM, Cupp CL, DeMarco JK, Hunsaker DH. Steroid use in rhinoplasty: an objective assessment of postoperative edema. Ear Nose Throat J. 1998;771:40-43. [PubMed] [Google Scholar]
- 15. Kara CO, Gökalan I. Effects of single-dose steroid usage on edema, ecchymosis, and intraoperative bleeding in rhinoplasty. Plast Reconstr Surg. 1999;1047:2213-2218. [DOI] [PubMed] [Google Scholar]
- 16. Kargi E, Hoşnuter M, Babucçu O, Altunkaya H, Altinyazar C. Effect of steroids on edema, ecchymosis, and intraoperative bleeding in rhinoplasty. Ann Plast Surg. 2003;516:570-574. [DOI] [PubMed] [Google Scholar]
- 17. Gürlek A, Fariz A, Aydoğan H, Ersöz-Oztürk A, Evans GRD. Effects of high dose corticosteroids in open rhinoplasty. J Plast Reconstr Aesthet Surg. 2009;625:650-655. [DOI] [PubMed] [Google Scholar]
- 18. Totonchi A, Guyuron B. A randomized, controlled comparison between arnica and steroids in the management of postrhinoplasty ecchymosis and edema. Plast Reconstr Surg. 2007;1201:271-274. [DOI] [PubMed] [Google Scholar]
- 19. Ozdel O, Kara CO, Kara IG, Sevinc D, Oguzhanoglu NK, Topuz B. Does corticosteroid usage in rhinoplasty cause mood changes? Adv Ther. 2006;235:809-816. [DOI] [PubMed] [Google Scholar]
- 20. Koc S, Gürbüzler L, Yaman H et al. The effectiveness of steroids for edema, ecchymosis, and intraoperative bleeding in rhinoplasty. Am J Rhinol Allergy. 2011;252:e95-e98. [DOI] [PubMed] [Google Scholar]
- 21. Xu F, Zeng W, Mao X, Fan G-K. The efficacy of melilotus extract in the management of postoperative ecchymosis and edema after simultaneous rhinoplasty and blepharoplasty. Aesthetic Plast Surg. 2008;324:599-603. [DOI] [PubMed] [Google Scholar]
- 22. Youssef TA, Elibiary H, Amish KF. Role of steroids in reducing postoperative edema in rhinoplasty: a meta-analytic study. Eur Arch Otorhinolaryngol. 2013;2704:1189-1193. [DOI] [PubMed] [Google Scholar]
- 23. Guyatt GH, Oxman AD, Montori V et al. GRADE guidelines: 5. Rating the quality of evidence--publication bias. J Clin Epidemiol. 2011;6412:1277-1282. [DOI] [PubMed] [Google Scholar]
- 24. Guyatt GH, Oxman AD, Kunz R, Vist GE, Falck-Ytter Y, Schünemann HJ. What is “quality of evidence” and why is it important to clinicians? BMJ. 2008;3367651:995-998. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25. Fallah A, Akl EA, Ebrahim S et al. Anterior cervical discectomy with arthroplasty versus arthrodesis for single-level cervical spondylosis: a systematic review and meta-analysis. PLoS One. 2012;78:e43407. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26. Akl EA, Sun X, Busse JW et al. Specific instructions for estimating unclearly reported blinding status in randomized trials were reliable and valid. J Clin Epidemiol. 2012;653:262-267. [DOI] [PubMed] [Google Scholar]
- 27. Review Manager (RevMan) [Computer program]. Version 5.3. Copenhagen: The Nordic Cochrane Centre, The Cochrane Collaboration, 2014. [Google Scholar]
- 28. Higgins J, Deeks JJ, Altman D. How to include multiple groups from one study. In:Higgins J, Green S, eds. Cochrane Handbook for Systematic Reviews of Interventions. West Sussex: Wiley Online Library; 2008:16.5.4. [Google Scholar]
- 29. Cohen J. Statistical Power Analysis for the Behavioral Sciences. 2nd ed Hillsdale, NJ: Lawrence Erlbaum Associates; 1988. [Google Scholar]
- 30. Brozek J, Oxman A, Schünemann H. GRADEpro. [Computer program on www.gradepro.org]. Version 0.4.8, McMaster University, 2014. http://tech.cochrane.org/revman/other-resources/gradepro/about-gradepro. Acessed February 13, 2014.
- 31. Higgins JPT, Thompson SG, Deeks JJ, Altman DG. Measuring inconsistency in meta-analyses. BMJ. 2003;3277414:557-560. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32. Racic G, Matulic J, Karelovic D, Bojic L, Ognjenovic M, Matulic Z. The effects of preoperative steroids in the reconstruction of the nasal pyramide. Medica Jadertina. 2000;301:73-80. [Google Scholar]
- 33. Alajmi MA, Al-Abdulhadi KA, Al-Noumas HS, Kavitha G. Results of intravenous steroid injection on reduction of postoperative edema in rhinoplasty. Indian J Otolaryngol Head Neck Surg. 2009;614:266-269.doi:10.1007/s12070-009-0080-y [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34. Fukushima W, Fujioka M, Kubo T, Tamakoshi A, Nagai M, Hirota Y. Nationwide epidemiologic survey of idiopathic osteonecrosis of the femoral head. Clin Orthop Relat Res. 2010;46810:2715-2724.doi:10.1007/s11999-010-1292-x [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35. Voineskos S. Plastic Surgical Randomized Controlled Trials: Challenges and Opportunities for Evidence-Based Plastic Surgery, A Systematic Scoping Review. M.Sc. Thesis Hamilton, Ontario, Canada: Health Research Methodology, McMaster University, 2013. [Google Scholar]
- 36. Devereaux PJ, Choi PT-L, El-Dika S et al. An observational study found that authors of randomized controlled trials frequently use concealment of randomization and blinding, despite the failure to report these methods. J Clin Epidemiol. 2004;5712:1232-1236. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.