

Abstract
Parkinson's disease is a neurodegenerative disorder classically characterized by motor symptoms. Among them, hypomimia affects facial expressiveness and social communication and has a highly negative impact on patients' and relatives' quality of life. Patients also frequently experience nonmotor symptoms, including emotional‐processing impairments, leading to difficulty in recognizing emotions from faces. Aside from its theoretical importance, understanding the disruption of facial emotion recognition in PD is crucial for improving quality of life for both patients and caregivers, as this impairment is associated with heightened interpersonal difficulties. However, studies assessing abilities in recognizing facial emotions in PD still report contradictory outcomes. The origins of this inconsistency are unclear, and several questions (regarding the role of dopamine replacement therapy or the possible consequences of hypomimia) remain unanswered. We therefore undertook a fresh review of relevant articles focusing on facial emotion recognition in PD to deepen current understanding of this nonmotor feature, exploring multiple significant potential confounding factors, both clinical and methodological, and discussing probable pathophysiological mechanisms. This led us to examine recent proposals about the role of basal ganglia‐based circuits in emotion and to consider the involvement of facial mimicry in this deficit from the perspective of embodied simulation theory. We believe our findings will inform clinical practice and increase fundamental knowledge, particularly in relation to potential embodied emotion impairment in PD. © 2018 The Authors. Movement Disorders published by Wiley Periodicals, Inc. on behalf of International Parkinson and Movement Disorder Society.
Keywords: facial emotion recognition, Parkinson's disease, basal ganglia, dopamine, embodied simulation
The original description characterizing Parkinson's disease (PD) by motor symptoms1, 2 has been updated because patients also experience cognitive and psychiatric symptoms,3, 4, 5, 6, 7 including emotional impairments. These lead to difficulties in describing bodily sensations, physiological arousal and feelings, expressing emotions, and identifying others' emotions from prosody and facial expression.8, 9, 10 Facial emotion recognition (FER) is one of the most basic aspects of emotional functioning and one of the most critical components of social behaviors. Aside from its theoretical importance, understanding FER disruption in PD is crucial for improving quality of life for both patients and caregivers. However, studies assessing FER in PD still report contradictory results. Although 2 reviews and 1 meta‐analysis revealed an FER deficit in PD and outlined potential biasing factors,9, 11, 12 the origins of this inconsistency are unclear, and several questions remain unanswered. For instance, what is the actual effect of dopaminergic medication on FER in PD? Does hypomimia affect FER in accordance with embodied simulation theory? From a more methodological perspective, are the tasks currently used sensitive enough to reveal impairments among patients? In short, we know that FER is impaired in PD but do not have sufficient information to fully understand the underlying mechanisms.
Building on a previous work,9 we therefore undertook a fresh review of FER in PD to enhance current understanding of this nonmotor feature while exploring significant potential confounding factors. Regarding probable pathophysiological mechanisms subtending impaired FER in PD, we looked at recent considerations about the role of basal ganglia‐based circuits in emotion. We also reconsidered hypotheses about embodied simulation that merit further research, despite being mentioned in early studies. We end by discussing the clinic and social consequences of emotional dysfunctions in PD.
Methods
We conducted a detailed search of the literature to extend previous reviews.9, 11, 12 We searched PubMed and Web of Science services with the following key words: Parkinson's disease, emotion recognition, facial expression, and decoding. We also hand‐searched relevant journals and examined the references of retrieved articles. Articles were restricted to the English language and published between January 1983 and July 2016. This yielded 167 eligible articles. Some publications were excluded (eg, reviews, studies related to deep‐brain stimulation, articles focused on emotion production/experience). A total of 59 articles reporting 97 comparisons between PD patients and healthy controls (HCs) during FER tasks were included. For each experiment, we checked whether significant differences between patients and HCs were highlighted and whether the presence of an emotion‐specific deficit was investigated. We also looked at which errors were made by participants during the experiment to characterize the deficit in detail. Subsequently, we considered the impact of multiple confounding factors. We did not attempt to provide an exhaustive report on the substantial differences across experiments enrolling heterogeneous samples, which may explain inconsistent results but make comparisons across studies well nigh impossible. Rather, we discussed the factors that may play a role in FER impairment in PD and should be taken into account in future studies.
Facial Emotion Recognition in PD
Overview of Performances
Table 1 provides an overview of the reviewed studies. For each experiment, it indicates (1) the FER task used, (2) whether patients' performance were significantly lower than that of HCs, (3) whether the deficit depended on the emotion, and (4) quantitative information about the number of experiments highlighting an FER deficit in PD for both overall performance and each specific emotion. Table 2 shows the different task types identified and which aspects of FER in PD are subject to a deficit. The quantitative summary in Table 1 should be considered with care, given that percentage rates reflecting the presence of a deficit for each emotion are based on the number of experiments in which authors examined FER as a function of the emotion displayed, when participants were exposed to that expression. Moreover, it is based on a qualitative review. See Gray and Tickle‐Degnen12 for an estimation of the deficit magnitude.
Table 1.
Overview of performance on FER tasks (1 of 3)
| Task | Deficit | Anger | Disgust | Fear | Sadness | Surprise | Happiness | Neutral | |
|---|---|---|---|---|---|---|---|---|---|
| Scott et al, 1984a | MATCH | + | ? | ? | ? | ? | ? | ? | ? |
| Beatty et al, 1989 | ID | + | + | + | + | + | + | + | + |
| Blonder et al, 1989 | ID | + | + | + | + | + | + | + | |
| Blonder et al, 1989 | MATCH | + | ? | ? | ? | ? | ? | ? | ? |
| Borod et al, 1990 | ID | − | −? | −? | −? | −? | −? | −? | −? |
| Borod et al, 1990 | DISCRI | − | −? | −? | −? | −? | −? | ||
| Caekebeke et al, 1991b | DESCRI | − | −? | −? | −? | −? | −? | ||
| Dewick et al, 1991c | MATCH | − | − | − | − | ||||
| Madeley et al, 1995c | MATCH | − | −? | −? | −? | ||||
| Madeley et al, 1995 | ID | + | + | + | − | − | − | ||
| Haeske‐Dewick, 1996c | MATCH | − | −? | −? | −? | ||||
| Jacobs et al, 1995 | DISCRI | + | ? | ? | ? | ? | ? | ? | ? |
| Jacobs et al, 1995 | MATCH | − | − | − | − | − | − | ||
| Jacobs et al, 1995 | IMAG | + | − | + | + | − | |||
| Jacobs et al, 1995 | DESCRI | + | − | + | + | ||||
| Breitenstein et al, 1998 (1) | ID | − | − | − | − | − | − | ||
| Breitenstein et al, 1998 (1) | MATCH | − | − | − | − | − | − | ||
| Breitenstein et al, 1998 (1) | DISCRI | − | − | − | − | − | − | ||
| Breitenstein et al, 1998 (1) | NAME | − | − | − | − | − | − | ||
| Breitenstein et al, 1998 (2) | ID | + | + | + | + | + | + | ||
| Breitenstein et al, 1998 (2) | MATCH | + | + | + | + | + | + | ||
| Breitenstein et al, 1998 (2) | DISCRI | + | + | + | + | + | + | ||
| Breitenstein et al, 1998 (2) | NAME | + | + | + | + | + | + | ||
| Adolphs et al, 1998 | INT | − | − | − | − | − | − | − | − |
| St Clair et al, 1998 | ID | − | ? | ? | ? | ? | ? | ? | ? |
| Kan et al, 2002 | ID | + | − | + | + | − | − | ||
| Tessitore et al, 2002 | MATCH | − | −? | −? | |||||
| Yip et al, 2003 (1) | ID | + | +? | +? | +? | +? | +? | +? | |
| Yip et al, 2003 (1) | DISCRI | − | −? | −? | −? | −? | −? | −? | |
| Yip et al, 2003 (2) | ID | + | +? | +? | +? | +? | +? | +? | |
| Yip et al, 2003 (2) | DISCRI | + | +? | +? | +? | +? | +? | +? | |
| Sprengelmeyer et al, 2003 (1) | ID | + | + | + | + | + | − | − | |
| Sprengelmeyer et al, 2003 (1) | HEXA | + | + | − | + | − | − | − | |
| Sprengelmeyer et al, 2003 (2) | ID | + | + | + | + | − | − | ||
| Sprengelmeyer et al, 2003 (2) | HEXA | − | − | − | − | − | − | − | |
| Dujardin et al, 2004 (1) | ID | + | + | + | + | ||||
| Dujardin et al, 2004 (2) | INT | + | + | + | + | ||||
| Yoshimura et al, 2005 | SCREEN | − | −? | −? | −? | ||||
| Pell and Leonard, 2005 | ID | − | − | − | − | − | − | ||
| Pell and Leonard, 2005 | DISCRI | − | ? | ? | ? | ? | ? | ? | ? |
| Pell & Leonard, 2005 (1) | ID | − | − | − | − | − | − | ||
| Pell & Leonard, 2005 (2) | INT | + | + | − | + | − | − | ||
| Suzuki et al, 2006 | ID | − | − | − | − | − | − | − | |
| Suzuki et al, 2006 | HEXA | − | − | − | − | − | − | − | |
| Suzuki et al, 2006d | INT | + | − | + | − | − | − | − | |
| Lachenal‐Chevallet et al, 2006 | ID | + | − | + | + | − | |||
| Lawrence et al, 2007 | ID | + | + | − | − | − | − | − | |
| Ariatti et al, 2008 | ID | + | − | − | + | + | − | ||
| Ariatti et al, 2008 | MATCH | + | +? | +? | +? | +? | +? | ||
| Clark et al, 2008 | ID | + | + | − | − | − | + | − | − |
| Martins et al, 2008 | ID | + | + | + | − | − | − | ||
| Delaveau et al, 2009e | MATCH | − | − | − | |||||
| Ibarretxe‐Bilbao et al, 2009 | ID | + | + | + | + | + | + | − | |
| Assogna et al, 2010 | ID | + | − | + | − | − | − | − | + |
| Cohen et al, 2010 | ID | − | −? | −? | −? | −? | −? | ||
| Paulmann and Pell, 2010f | ID | + | + | + | + | + | + | + | + |
| Clark et al, 2010 | ID | + | + | − | − | − | + | − | − |
| Martinez‐Corral et al, 2010 (1) | ID | − | −? | −? | −? | −? | −? | −? | |
| Martinez‐Corral et al, 2010 (2) | ID | + | − | − | + | + | − | − | |
| Narme et al, 2011 | ID | + | + | − | + | − | − | ||
| Herrera et al, 2011 | ID | + | +? | +? | +? | +? | +? | +? | |
| Wieser et al, 2012 | ID | − | − | − | − | − | − | ||
| Baggio et al, 2012 | ID | + | + | + | + | + | − | − | |
| Buxton et al, 2012g | ID | + | − | + | − | + | + | + | − |
| Ventura et al, 2012h | ID | − | − | − | − | − | − | − | − |
| Ventura et al, 2012h | DISCRI | − | −? | −? | −? | −? | −? | ||
| Ventura et al, 2012h | MATCH | − | −? | −? | −? | −? | −? | ||
| Garcia‐Rodriguez et al, 2012 (1) | ID | − | −? | −? | −? | −? | −? | −? | |
| Garcia‐Rodriguez et al, 2012 (2) | ID | + | +? | +? | +? | +? | +? | +? | |
| Saenz et al, 2013 | ID | + | + | + | − | ||||
| Narme et al, 2013 | ID | + | − | − | + | + | − | + | |
| Alonso‐Recio et al, 2013 | ID | + | + | + | + | + | + | ||
| Alonso‐Recio et al, 2013 | DISCRI | − | −? | −? | −? | −? | −? | ||
| Hipp et al, 2014 | ID | + | − | − | + | − | − | − | |
| Alonso‐Recio et al, 2014a | DISCRI | + | +? | +? | +? | +? | +? | ||
| Alonso‐Recio et al, 2014b (1) | ID | + | + | + | + | + | + | ||
| Alonso‐Recio et al, 2014b (2) | DISCRI | + | + | + | + | + | + | ||
| Marneweck and Hammond, 2014i | DISCRI | + | + | ||||||
| Marneweck et al, 2014 (1) | DISCRI | + | + | + | + | + | |||
| Marneweck et al, 2014 (2) | DISCRI | + | + | + | + | + | |||
| Marneweck et al, 2014 (3) | DISCRI | + | +? | +? | +? | +? | +? | +? | |
| Marneweck et al, 2014 (4) | ID | + | +? | +? | +? | +? | +? | +? | |
| Wabnegger et al, 2015 (1) | ID | − | − | − | − | − | |||
| Wabnegger et al, 2015 (2) | INT | + | − | − | + | + | |||
| Laskowska et al, 2015j | EIS‐F | + | +? | +? | +? | +? | +? | +? | |
| Enrici et al, 2015 | ID | + | + | + | + | + | + | + | |
| McIntosh et al, 2015 | ID | + | − | + | + | − | − | − | + |
| Ricciardi et al, 2015 | ID | + | − | − | − | − | + | − | |
| Ille et al, 2016 (1) | ID | − | − | − | − | ||||
| Ille et al, 2016 (2) | INT | + | − | − | + | ||||
| Pietschnig et al, 2016 | ID | + | − | − | − | − | − | ||
| Albuquerque et al, 2016 | ID | − | − | − | − | − | − | − | − |
| Albuquerque et al, 2016 | DISCRI | − | − | − | − | − | − | − | − |
| Wagenbreth et al, 2016 | ID | + | + | + | + | − | |||
| Lin et al, 2016 (1) | ID | + | − | − | + | − | |||
| Lin et al, 2016 (2) | ID | + | + | − | + | + | |||
| Argaud et al, 2016k | ID | + | − | + | + | ||||
| Quantitative summary: | n = 97 | 64% | 44% | 47% | 54% | 51% | 30% | 27% | 42% |
Task: type of task used by the authors (see Table 2 for details). Deficit: “was the performance of patients with PD significantly lower than that of healthy controls?” A plus sign in a dark‐shaded box indicates “yes, a facial emotion recognition deficit was highlighted according to a global score” (ie, whatever the displayed emotion). A minus sign in a white box indicates “no, there was no group difference.” When the authors investigated the groups' performance as a function of the displayed emotion, the same symbols are used in the boxes corresponding to the specific emotions: a plus sign in a dark‐shaded box indicates that the deficit affected this specific emotion, whereas a minus sign in a white box indicates that recognition of this specific emotion was spared. On the contrary, when the authors only examined the groups' performance according to an overall score encompassing all the emotions, these signs are followed by a question mark. Question marks on their own mean that no information is available about the emotions displayed in the study. When the box relating to a specific emotion is empty, it means that the latter was not manipulated in the experiment. Quantitative summary: the percentage of the experiments we reviewed (n = 97) that highlighted a facial emotion recognition deficit in PD (general or specific) is indicated in the “Deficit” column. Likewise, for each specific emotion, we indicate the percentage of experiments that specifically showed that the emotion recognition deficit affected that emotion in particular (ie, when the authors submitted this emotion to the participant and examined the performance of recognition according to this emotion).
In Scott et al (1984), participants were required first to describe a target facial emotion, then to match it with an affective sentence.
Caekebe et al (1991) also exposed participants to contempt (no group difference).
In Dewick et al (1991), Madeley et al.(1995), and Haeske‐Dewick (1996), participants were required to choose which facial expression in a pair of photographs of the same person's face expressing different emotions matched a printed label. Breitenstein et al (1998) assessed FER among patients who met the criteria for (1) stage I or (2) stage II PD according to the Hoehn and Yahr classification system. Yip et al (2003) assessed FER (1) among patients with right‐sided PD classified as stage I or II according to Hoehn and Yahr staging and (2) among patients with bilateral PD classified as stages II‐V. Sprengelmeyer et al (2003) assessed FER (1) among patients in the early stages of the disease (mean score ± SD, 1.7 ± 0.5 on the Hoehn and Yahr scale) who had not yet received dopaminergic medication and (2) among patients in the more advanced stages (mean score ± SD, 2.6 ± 0.9 on the Hoehn and Yahr scale) under dopamine replacement therapy. Dujardin et al (2004) used a facial emotion rating task. The authors analyzed participants' performance (1) in terms of the percentage of accurately identified expressions, where an expression was deemed to have been accurately identified if the emotion scale eliciting the highest intensity rating corresponded to the target emotion and (2) according to intensity scores. Pell and Leonard (2005) also used a facial emotion rating task. The authors investigated participants' performance based on both (1) intensity ratings and (2) correlations between the intensity ratings that each patient assigned to a target face and the set of mean ratings assigned to that stimulus by HCs. This latter method did not allow the authors to run direct comparisons between groups but still highlighted deviations from normal patterns of sensitivity among patients for specific emotions.
Suzuki et al (2006) highlighted a specific FER deficit for disgust in PD during a facial emotion rating task, using a refined assessment method based on item response theory.
Delaveau et al (2009) conducted a study in which patients with PD and HCs were scanned both with and without levodopa medication. Regarding accuracy (correct responses), there were no differences between the groups (patients versus controls) or between pharmacological states (levodopa versus placebo) within these groups. The same data are presented in Delaveau et al (2010).
Paulmann and Pell (2010) highlighted a negative impact of PD on the recognition of emotions conveyed through different channels (lexical semantic/prosody/facial expressions), either in isolation (unimodal) or in various combinations (bi‐ or multimodal emotion cues), with no significant effect of the communication channel. Martinez‐Corral et al (2010) assessed FER among patients with PD (1) without and (2) with apathy.
Buxton et al (2012) examined FER abilities at 3 levels of difficulty (easy, moderate, and difficult). The authors highlighted deficits in the recognition of facial expressions of happiness at the moderate and difficult levels, disgust and surprise at the moderate level only, and sadness at the difficult level only. Patients had no difficulty identifying prototypical facial emotions (easy level).
Ventura et al (2012) analyzed participants' performance on an identification task and a discrimination task, based on a single composite score. In Garcia‐Rodriguez et al (2012), the FER abilities of de novo patients with PD were tested under 2 conditions: (1) a simple identification task and (2) the same identification task concurrent with a secondary task (the Corsi Blocks tapping). Alonso‐Recio et al (2014a) assessed FER abilities in PD during a one‐back procedure: participants were required to indicate whether the current stimulus matched the one shown from one step earlier in a sequenced presentation of stimuli. They highlighted a deficit among the patients that was more pronounced in patients with higher disease severity according to the CISI‐PD scale. In another study, Alonso‐Recio et al (2014b) adapted a Stroop task to assess FER in PD taking into account inhibition abilities with an emotional version (ie, participants were required to identify the emotion portrayed on the presented face while ignoring the incongruent or congruent superimposed emotion category name) and a nonemotional version (traditional color‐word Stroop task). They showed that patients were impaired in the emotional Stroop task but not in the traditional Stroop task; Likewise, to take into account the visual search abilities, the authors adapted the “face in the crowd” test with an emotional (ie, participants were required to decide whether the 24 faces showed the same emotion or whether any displayed a different one) and a nonemotional version. Here again, they showed that PD patients were impaired in the emotional version of the task but not in the classic version, the nonemotional task.
Marneweck and Hammond (2014) used 2 FER tasks in which participants were required to discriminate between neutral and angry faces. In one, they had to indicate whether the face expressed anger or neutrality by clicking the appropriate button. In the other, angry and neutral faces appeared successively on the screen, and participants were required to indicate the interval (first or second) containing the angry face. In both cases, the patients' performance was lower than that of HCs. Marneweck et al (2014) used discrimination tasks in which participants were required to discriminate between (1) facial emotions and neutral faces, (2) facial expressions of the same emotion at different levels of intensity, and (3) 2 facial expressions of the same emotion and a different one. Wabnegger et al (2015) and Ille et al (2016) used a facial emotion rating task. They assessed participants' performance (1) according to an index reflecting the response accuracy and (2) based on intensity ratings of the target emotion only.
Laskowska et al (2015) chose to use the Emotional Intelligence Scale‐Faces (EIS‐F), a more ecologically valid task featuring a mixture of basic and complex emotions (eg, tenderness, admiration, pride, disappointment, feeling of superiority, etc.). The authors based their analyses on signal detection theory, measuring decision‐making strategy (response bias) and accuracy of stimulus detection (sensitivity) to determine whether the FER deficit in PD results from a decision‐making impairment or from impaired sensory processes. In Lin et al (2016), 2 groups of patients were required to identify the valence (positive versus negative) of facial expressions: (1) patients with low motor dysfunction (<35 on UPDRS III; mean, 24; SD, mean, 48.73; SD, 14.58).
As in Dujardin et al. (2004), Argaud et al (2016) used a facial emotion rating task and analyzed participants' performance in terms of decoding accuracy, considering an expression to be accurately identified if the emotion scale receiving the highest intensity rating corresponded to the target emotion.
Table 2.
Description of the different types of tasks used in the literature and their conclusions regarding the presence of an FER deficit in PD
| Task | Instructions | n | Deficit | |
|---|---|---|---|---|
| ID | Identification task | Participants were required to select the appropriate label for a given emotional expression. | 53 | 39 |
| DISCRI | Discrimination task | Participants were required to determine whether the faces displayed simultaneously expressed the same or a different emotion. | 16 | 9 |
| MATCH | Matching task | Participants were required to match a target facial expression with another facial expression and/or an affective prosodic sentence expressing the same emotion. | 12 | 4 |
| NAME | Naming task | Participants were required to name the emotion displayed by the facial expression. | 2 | 1 |
| IMAG | Imagery task | Participants were required to imagine a target facial emotion and to answer yes/no questions about the physical characteristics of that expression (eg, “Are the eyebrows drawn together?”). | 1 | 1 |
| DESCRI | Description task | Participants were required to answer yes/no questions about the physical characteristics of a displayed facial emotion (this task was designed as a perceptual control task for the imagery task). | 2 | 1 |
| INT | Intensity rating task | Participants were required to assess the emotions portrayed and their intensity on visual analog scales ranging from “not at all” (ie, emotion absent from the expression) to “intensively expressed”. | 6 | 5 |
| HEXA | Emotion hexagon task | The emotion hexagon task is an identification task using morphed facial expressions that combines 2 closely related emotions (ie, the stimuli are morphed across a continua that lies around a hexagon: happiness‐surprise‐fear‐sadness‐disgust‐anger‐happiness). | 3 | 1 |
| SCREEN | Screening task | Participants were required to press a button as soon as they perceived a target facial emotion. | 1 | 0 |
| EIS‐F | Emotional Intelligence Scale‐ Faces | Participants were required to indicate which emotions were expressed by a given facial expression and which were not, choosing between “shown”, “not shown” and, as a last resort, “hard to say”. | 1 | 1 |
n: Number of studies that used this type of task out of a total of 97 reviewed experiments; Deficit: studies using the corresponding type of task highlighted a FER deficit in PD according to a global score.
Impaired or Intact FER?
Although a nonnegligible number of authors failed to find any difference between patients and HCs, most of the studies investigating FER in PD highlighted lower performance among patients (Table 1). This is congruent with the meta‐analysis by Gray and Tickle‐Degnen.12 Two years earlier, Clark and collaborators13 also underlined the deleterious impact of this deficit on patients' social relationships, highlighting a negative correlation between their FER difficulties and their level of interpersonal distress.
Is the Deficit Specific or General?
It is quite difficult to know if PD selectively impairs the recognition of specific emotions or leads to an overall deficit. Indeed, about 30% of the reviewed studies did not examine its effect on the recognition of specific emotions but calculated an overall score encompassing all the displayed emotions.4, 14, 15, 16, 17, 18, 19, 20, 21, 22, 23, 24, 25, 26, 27, 28, 29 Moreover, authors did not manipulate the same set of stimuli, and some only used a small subset.23, 30, 31, 32, 33, 34, 35 At last, some authors who explicitly investigated the recognition of specific emotions showed that although recognition was impaired for all the emotions they tested, some were more poorly recognized than others.24, 32, 34, 36, 37, 38, 39 Like Gray and Tickle‐Degnen,12 we noted that FER deficit in PD affected all the basic emotions but was greater for negative emotions (64% of studies highlighted a global deficit, 44% for anger, 27% for happiness; Table 1). This could echo the subcortical pathway involving the pulvinar, the amygdala, and the striatum, which may lead to a coarse but fast visual information processing.40, 41 Indeed, because of its evolutionary relevance, this preserved route may induce a preattentive and autonomic bias toward threatening stimuli like angry faces.42, 43 However, experimental data failed to fully support this “angry faces advantage” (whereby angry faces are detected more quickly than others). Some even supported the reverse “happy faces advantage”44 (see Ceiling Effect and Task Sensitivity section). In addition, there are several important caveats. First, these results were based on the subset of studies reporting participants' performance as a function of emotion. Second, Gray and Tickle‐Degnen12 chose to pool data across modalities (face/voice). Third, we should bear in mind the greater diversity of negative as opposed to positive emotions in the literature. Surprise is ambiguous (pleasant, unpleasant, astonishment). Classifying it as a positive emotion is difficult without context. Therefore, of the 6 so‐called basic emotions, there is only 1 prototypical and easily recognizable positive. Hence, the negative‐emotion‐specific FER deficit in PD is not so obvious. Future studies should shed light on this point by using a larger set of emotions including more than one positive affect.
What About the Errors Made?
Some authors conducted a deeper investigation of FER deficit in PD by examining the errors made. In an identification task, for instance, participants made an error if they did not select the appropriate label for a given expression. Instead of just counting this item as a misidentified expression, it can be quite more interesting to go further and examine the erroneous label. Did participants make an aberrant error (happiness versus sadness) or instead confuse 2 closely related emotions (surprise versus fear)? Only 5 studies reported this information.23, 30, 45, 46, 47 Three of them23, 46, 47 simply stated that patients and HCs made the same kind of errors. The two others30, 45 statistically confirmed the presence of similar confusion patterns in PD patients and HCs. In Assogna et al,45 patients mixed up negative emotions and assigned a neutral state to expressions they failed to recognize. In Argaud et al,30 the most confusing emotion whatever the group was surprise.
Discrepancies in Results
Several confounding factors have been put forward to explain discrepancies in results. Some concern methodological aspects (study design, group size, instructions), stimuli (intensity, dynamism, emotion), task type and sensitivity, and analyses (categorical analyses based on rates of correct answers, continuous analyses based on intensity ratings, effect of emotion, covariables). Others could be linked to participants' sociodemographic features (age, sex, personality) and/or patients' clinical characteristics (disease severity, nonmotor symptoms, medication). In the following sections, we review evidence for the potential role of some of the most relevant factors when studying FER in PD.
Methodological Aspects
Stimuli
Although we are usually exposed to dynamic expressions in real‐life situations, very few studies investigating FER in PD used dynamic stimuli.30, 48, 49, 50 Because emotions are defined as transitory changes in several components of the organism, the dynamism of facial expressions plays a major role in emotion perception with a beneficial effect on FER accuracy.51 Moreover, neuroimaging studies have highlighted differential neural activity for static versus dynamic facial emotions, with higher activation in response to dynamic stimuli in regions processing socioemotional information, motion and faces and that belong to the mirror neuron system: superior temporal sulcus (STS), visual area, fusiform gyrus, inferior frontal gyrus, amygdala, and orbitofrontal cortex (OFC).52, 53, 54 However, only Kan et al48 investigated the effect of stimuli dynamism on FER in PD. They found that patients' performance clearly worsened when they had to recognize emotions from static rather than dynamic faces and concluded that this could artificially heighten the impact of PD on FER. In addition, the stimuli used in FER studies in PD generally depicted emotions at full‐blown intensity. As emotional intensity has been shown to have a beneficial effect on FER,24, 38, 45 it is important to take this factor into account, especially knowing that patients could lose this positive effect.32
Task Type and Difficulty
Task type variations across studies make consistent results less likely to emerge. In most cases, authors used identification tasks that require selecting the appropriate label for a given emotion. The remainder frequently chose discrimination/matching tasks that require judging whether or not 2 faces express the same emotion (Table 2). This may reflect different stages in the FER processs.55 Although both involve intact perceptual information processes occurring relatively early after stimulus onset, identification requires additional knowledge yielded by a categorization process. Thus, task type seems to determine task difficulty, and FER deficit in PD could be associated with a deficit in early perceptual and/or categorization processes. In the literature, identification tasks more frequently highlighted an FER deficit in PD (Table 2). However, Gray and Tickle‐Degnen12 showed a greater FER deficit during discrimination tasks. Furthermore, the level of difficulty can vary within the task. The forced‐choice procedure of Cohen et al19 only featured 2 emotional labels, even though participants were exposed to 5 facial emotions. This considerably increased the probability of giving a correct answer by chance and then could explain the absence of a significant difference between patients and HCs. Last, the above‐mentioned problem of using prototypical stimuli and the differing levels of difficulty across emotions could result in a ceiling effect, thus biasing results (see below).
Ceiling Effect and Task Sensitivity
A lack of task sensitivity may have meant that significant differences between patients and HCs went unnoticed. In some studies, scores were very close to maximum, which suggests a ceiling effect that would have concealed any deficit.20, 23, 31, 56, 57 This could also induce a bias in favour of an emotion‐specific deficit, especially when happiness recognition was compared with that of other emotions. Indeed, happy expressions are recognized more quickly and accurately than others. This could be related to its most distinctive configuration with a very salient feature, the smile, whereas other facial expressions show more overlapping, less distinctive features.58, 59, 60, 61, 62, 63 Thus, it is not suprising that a specific FER deficit for negative emotions emerges, whereas happiness recognition elicits higher accuracy scores.35, 47, 48, 64, 65, 66, 67, 68 One solution to avoid this biais would be to combine different task types within the same study15, 16, 17, 23, 24, 28, 36, 37, 56, 69 or use more refined assessment methods.22, 70 Alternatively, FER could be assessed in more detail using rating tasks in which participants assess emotions and quantify their intensity. More specifically, they rate a target expression on a set of emotional visual analog scales (VAS). Few studies used rating tasks,30, 32, 33, 56, 70, 71, 72 but all except one71 highlighted an FER deficit among patients. However, when intensity ratings were dichotomized as correct (when the scale corresponding to the target emotion had the highest intensity rating) versus incorrect, the deficit was not always reported.33, 72 Surprisingly, only Dujardin et al32 analyzed response patterns according to the intensity scores on each VAS. They showed that patients rated the target emotion lower than HCs did and systematically rated surprise higher, whatever the emotion displayed. Thus, using VAS allows for a deeper analysis. Although this methodology is still rare in studies investigating FER in PD, it has been successfully used to characterize emotional bias in schizophrenia and depression when no impairment emerged from categorical judgments based solely on response accuracy.73, 74
Clinical Factors
Patients' characteristics varied significantly across and within studies. Some enrolled patients who had recently been diagnosed and were not yet receiving medication, patients under dopamine replacement therapy (DRT) with a more severe disease including nonmotor symptoms, or patients who had temporarily interrupted their treatment. Thus, disease duration and severity, medication, cognitive/visuospatial impairments, and mood disorders are (quite interrelated) factors that could contribute to FER impairment in PD.
Disease Severity and Facial Hypomimia
Although an FER deficit has been highlighted in the early stages of the disease,21, 32, 66, 69, 70, 75 it was greater in the most severely affected patients.15, 28, 29, 36, 38, 68, 76 That said, when the link between deficit magnitude and disease severity was investigated with correlations, results differed. Based on these statistics, Gray and Tickle‐Degnen12 suggested that the level of FER deficit is unrelated to the level of motor disability reflected by Hoehn and Yahr staging.77 However, the average patients included in their meta‐analysis exhibited mild to moderate motor disability. Their conclusions would have been different in more severe cases. Even when disease severity was measured with the Unified Parkinson's Disease Rating Scale, regarded as more sensitive than Hoehn and Yahr staging,78, 79 results still diverged but seemed to be in favour of a positive correlation between disease severity and FER deficit.24, 64, 65, 67, 80, 81 PD progression is very heterogeneous and depends on several factors. Patients with the same disease duration/severity may have different patterns of neuronal loss in striatal, limbic, and cortical regions.82, 83 Thus, to examine the link between disease severity and FER deficit in PD, it might be useful to employ more sensitive markers (neuroimaging) of disease progression or subtype.84 Furthermore, FER deficit could also be linked to motor asymmetries in PD, but the question of whether patients with left‐dominant motor symptoms (LPD) showing relatively greater neural degeneration in the right hemisphere have a more severe deficit than patients with right‐dominant motor symptoms remains open. LPD patients could be more likely to show FER impairments considering the relatively greater role of the right hemisphere in FER (at least for anger, fear, and sadness) and the prominence of visuospatial deficits in LPD patients.85, 86 Last, since the earliest studies, emotional disorders in PD concern both expression and recognition, and some authors have even reported positive correlations between facial expression and FER impairment.17, 37, 87, 88, 89 These findings are in line with a peripheral component of the FER deficit arising from facial hypomimia in PD. This assumption is furhtuer developed in the Discussion section (see New Hypotheses Based on Embodied Simulation section).
Visuospatial Deficits and Other Cognitive Symptoms
From the earliest studies, authors controlled for visual functions with tasks such as the Benton Facial Recognition Test (BFRT).90 Some found FER impairment among patients with no deficit in neutral faces recognition,15, 16, 23, 29, 68, 69, 76, 91 whereas others showed that face‐processing impairment co‐occurs with the deficit.24, 46 Gray and Tickle‐Degnen12 did not report any significant differences in FER abilities between patients who performed normally on tests like BFRT and patients with abnormal performance. They concluded that FER deficit in PD exists beyond a general deficit in face processing. However, the BFRT may not be sensitive enough to highlight a deficit.38 Based on more accurate measurements of visuospatial abilities including low‐level visual functions (contrast sensitivity), some authors suggested that FER deficit could be related to visuospatial impairments in PD.28, 38, 47, 75, 92 For instance, showing that the ability to discriminate graded intensities of angry faces was positively correlated with the ability to discriminate unperfect/perfect circles (radial frequency patterns), Marneweck and Hammon indicated that impaired ability to perceive visual forms could contribute to FER deficit in PD.38 It is noteworthy that visual and emotional systems are extensively interconnected; for example, the amygdala is connected to the superior colliculus via the pulvinar, to the OFC, and the anterior cingulate cortex, as well as to cortical visual regions in the temporal cortex.41 Furthermore, the idea that FER deficit in PD could be secondary to executive dysfunction is an old one. Working memory impairment could influence FER as the ability to manage, maintain, and operate with present and stored information is affected (particularly true for sequentially presented stimuli29. Likewise, divided and selective attention is impaired in PD.93 Thus, FER deficit in PD could be linked to attentional difficulty to process different sources of information at the same time. As authors who assessed cognitive abilities used different tests measuring different aspects of executive function, no consistent conclusion could be drawn regarding the link between cognitive impairement and FER in PD.21, 32, 36, 45, 48, 56, 94 In recent studies,21, 22, 26, 29, 45, 95 however, an FER deficit was confirmed among patients after controlling for cognitive symptoms (including working memory and attention processes) but seemed to be influenced by their magnitude.
Mood Disorders
As emotional processes are disrupted in depression96, 97 and knowing the high incidence of depression in PD,7, 98 it has been suggested that FER deficit is not specific to PD but is linked to mood disorders. The studies we reviewed usually controlled for this aspect by selecting patients with normal depression scores and/or directly testing the effect of depression on performance. Here again, results were heterogeneous. When they compared the performance of relatively depressed patients with those with normal scores and assessed correlations between FER performance and depression score, Gray and Tickle‐Degnen12 concluded that FER deficit is not secondary to depression in PD. Since 2010, only Baggio et al64 and Linn et al76 have reported a link between depression and FER in PD. Concomitant with depression, apathy and anxiety are also frequent in PD.3, 99 However, these mood disorders have been taken into account less often, although some studies have highlighted their influence on FER (anxiety: Clark et al13 and Ille et al33; apathy: Robert et al100 and Martínez‐Coral et al25).
Dopamine Replacement Therapy
Some authors who assessed FER in patients who were not yet receiving medication or had temporarily withdrawn from DRT highlighted a deficit in the absence of treatment.32, 33, 34, 94 Others failed to find any difference between patients without DRT and HCs.18.,49 Only Sprengelmeyer et al68 directly compared medicated and unmedicated patients on FER. They reported a deficit in patients whatever the treatment condition, but found a greater one among unmedicated patients. This is consistent with the positive correlation between patients' performance and daily levodopa‐equivalent dose (LED) found by Assogna et al.45 However, no other authors who looked for such correlations found this result.19, 28, 38, 45, 64, 65, 67, 75 Otherwise, several studies have reported a beneficial effect of DRT on FER in PD. In Tessitore et al,101 both patients with and without DRT showed reduced amygdalar activation during angry and fearful faces processing. However, as evidenced by increased blood‐oxygen‐level dependent (BLOD) responses in the drug‐on relative to the drug‐off state, dopamine repletion partially restored the amygdala response. Similarly, Delaveau et al102 highlighted restoration of default mode network deactivation after levodopa administration in PD (posterior cingulate and lateral temporal cortices). In HCs, reduced activation of the mesocorticolimbic regions involved in emotional processing (with difficulties in recognizing anger103) followed the administration of a dopamine antagonist.103, 104 Conversely, Delaveau et al105, 106 reported reduced amygdala activity after levodopa administration in HCs and patients. These results might appear contradictory, with DRT having a beneficial effect on FER in some cases and a detrimental one in others, but it would depend on disease progression. In the early stages, mesocorticolimbic pathways would be relatively spared compared with the motor pathway.82, 107 Thus, the dose of levodopa needed to improve motor symptoms may simultaneously overdose mesolimbic projections to the amygdala. In more severe stages, DRT may have a beneficial effect, compensating for dopamine depletion, and blocking the responses of mesocorticolimbic structures in HCs by administering dopamine antagonists may mimic disease progression. The DRT overdose effect has already been highlighted in cognitive functions.108 Regarding emotion recognition, only 1 study specifically examined the impact of DRT in early PD109 and found more pronounced difficulty recognizing emotional prosody among early patients under DRT versus the drug‐off condition.
Discussion
A schematic diagram summarizing the review is shown in Figure 1.
Figure 1.
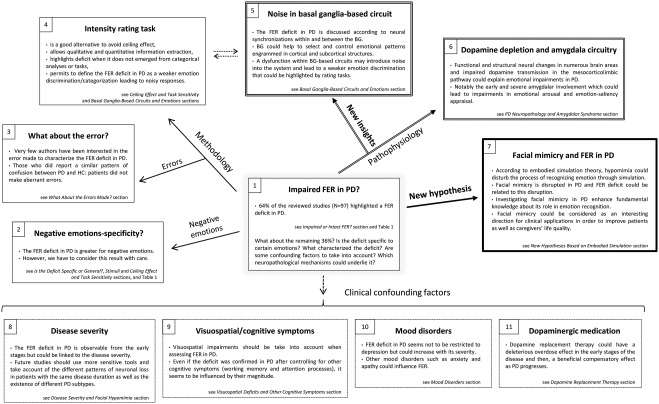
Facial emotion recognition in Parkinson's disease: review and discussion. (1) level of impairment, (2) emotions‐specificity, (3–4) methodology, (5‐6) underlying pathophysiological mechanisms with (5) recent considerations about basal ganglia‐based circuits in emotions, (7) new hypothesis related to hypomimia, (8–11) potential clinical confounding factors.
What Can We Learn From This Review?
Recognition of the 6 basic facial emotions is impaired in PD, but the deficit seems to be greater for negative emotions. Because of high variability in results, several potential confounding factors need to be considered. Although some of them were highlighted by Assogna et al11 and investigated by Gray and Tickle‐Degnen,12 no reliable conclusions could be drawn as to the effects of disease severity, depression, or cognitive/visuospatial symptoms or the impact of dopaminergic medication. Moreover, neither anxiety nor apathy was analyzed. Our review indicates that FER deficit in PD (1) depends on disease severity, while observable from disease onset; (2) is linked to visuospatial disturbances, notably low‐level visual dysfunction; (3) is more pronounced in patients with cognitive impairment; (4) is not restricted to depression but seems to increase with the magnitude of mood disorders including anxiety and apathy; and (5) fluctuates according to DRT, with an overdose effect in the early stages and a beneficial effect as PD progresses and treatment compensates for dopamine depletion.
One important aspect underlined is the potential lack of task sensitivity when assessing FER and other forms of processing. Some studies that failed to find behavioral differences nevertheless observed deficits at the cerebral level.57, 72, 81, 101 Wieser et al81 reported diminished early visual discrimination of facial emotions among patients at the electrocortical level, but no differences in affective ratings or recognition accuracy. Here, behavioral assessments were not sufficiently sensitive to detect subtle impairments already present at the neural level. Intensity rating tasks offer an alternative method for accurately studying FER in PD. Analyses of response patterns distinguishing between target and nontarget VAS allow both FER accuracy (qualitative information) and emotion discrimination (quantitative information) to be appraised. So far, however, only Dujardin et al32 have assessed FER among patients using intensity ratings per se. They reported a weaker level of emotion discrimination in PD, leading to noisy responses, with lower ratings on target scales and higher ratings on nontarget scales. In addition, such more refined methodologies should be used to avoid a potential ceiling effect. In the same vein, future studies should use dynamic stimuli portraying more subtle/complexe emotions such as tenderness, disappointment22, 34 (with more than one positive emotion) to investigated the deficit consequences in conditions closer to everyday reality.
Furthermore, this review encourages future studies to adopt a precautionary approach as far as possible avoiding the effects of clinical confounding factors and/or evaluating their impact on FER. Although it could increase study duration, patients should undergo an extensive neuropsychological/psychiatric interview investigating numerous aspects of cognitive functioning and mood‐related features. Thus, patients with mood and/or cognitive disorders could be excluded or test results could be correlated with FER outcomes. Likewise, knowing the clear influence of DRT on FER, future studies should take into account the LED calculated for each patient according to common guidelines110 or enrolled patients not receiving medication yet or assessed off medication. At last, as far as disease duration/severity is concerned, more sensitive markers should be privileged. Future studies will surely favour neuroimaging techniques rather than only clinical scales that despite scoring symptoms severity, do not convey much information about disease progression or subtype.
PD Neuropathology and Amygdalar Syndrome
Neural changes in numerous areas and impaired dopamine transmission in the mesocorticolimbic pathway are invoked to explain FER deficit in PD. Indeed, not only putaminal but also orbitofrontal and amygdalar presynaptic dopaminergic functions were altered in early PD.111 In addition, brain responses recordings during FER tasks have revealed decreases in striatal, amygdalar, and orbitofrontal activity and lower activation in analytic temporal facial recognition areas (STS and fusiform gyrus).57, 72, 101, 112 Lotze et al112 have shown that the less dopamine transporter availability (DAT) present in the putamen, the lower the ventrolateral prefrontal cortex activation in response to emotional gestures and highlighted a positive correlation between the putaminal DAT reduction and the number of errors in emotional gestures recognition. Similarly, morphometry analyses reported decreased gray‐matter volume in numerous limbic, paralimbic, and neocortical associative temporo‐occipital areas64, 66, 113, 114 and showed that the atrophy could be associated with the deficit, as gray‐matter volume in these regions correlated with patients' FER performance.64, 66 More specifically, impairment of the amygdala, observed since the early stages and worsening with disease progression,107, 115, 116 has often been invoked to explain emotional deficiencies in PD, as we know that the amygdala circuitry is involved in multiple behavioral functions including emotional arousal and emotion‐saliency appraisal.117, 118 In their recent review, Diederich et al119 clearly reported the behavioral consequences of amygdalar dysfunction in PD and depicted this amygdalar syndrome as both a “failing doorman” who struggles to identify emotional contents of sensory inputs and a “failing disk jockey” who cannot orchestrate emotional outputs adequately anymore. They also specified that dopamine could induce hyperactivity of the amygdala, a finding that fits with the hypothesis of an overdose effect on FER in early PD and that compensatory mechanisms could occur as well (see New Hypotheses Based on Embodied Simulation section).
Basal Ganglia‐Based Circuits and Emotions
FER deficit in PD could also be discussed in light of neural synchronizations within and between the basal ganglia (BG).120 The BG may be involved in emotion processing in the same way they are in motor and cognitive functions. Cortico‐BG‐thalamocortical loops may inhibit nonrelevant information (nontarget emotions/related facial features) and activate relevant ones (target emotions/related facial features) just as they select a specific movement by inhibiting competing programs and disinhibiting the selected one.121 Moreover, BG‐based circuits are involved in automated chunked representations of action/cognitive sequences and contribute to the suppression of goal‐directed behavioral control when it becomes habitual.122 The progressive loss of rapid habitual processing and the replacement of automatic control by effortful processing may make PD patients more vulnerable to interference and lead to difficulty in performing even well‐known procedures. The BG may perform similarly when it comes to processing emotional information efficiently. Regarding FER, the BG might help to select and control emotional patterns engrammed in cortical and subcortical structures (face fusiform area for face perception, amygdala for relevance detection, OFC for evaluation‐driven emotion processing) by inhibiting competing patterns and coordinating the whole process.120 Studies investigating subthalamic nucleus deep‐brain stimulation in PD suggest that the BG recruit and synchronize the activity of the face fusiform area, amygdala, and OFC.123, 124 Dysfunction within BG‐based circuits may therefore introduce noise into the system, disrupt the synchronization process, and lead to biased emotional judgments characterized by a weaker emotion discrimination (noisy responses) that could be highlighted by rating tasks.
New Hypotheses Based on Embodied Simulation
The link between facial expression and FER impairment highlighted since the earliest studies on FER in PD17, 37, 87 recall embodied simulation theory, suggesting that disturbed motor processing can lead to emotion recognition deficiency. According to this theory, emotion recognition is facilitated by internally generated somatosensory representations triggered by the simulation of a perceived facial expression that partially activates the corresponding emotional state in the observer.55, 125, 126, 127 This is subtended by somatosensory‐related cortices and could be linked to facial mimicry, the tendency to replicate others' facial expressions.128, 129 Hence, in HCs, facial electromyography (EMG) could highlight congruent facial muscle responses to facial expressions, which could foster emotion recognition.130, 131, 132 However, one of the most frequent and distinctive Parkinsonian motor symptoms is hypomimia.1 Thus, in addition to central disorders, emotional symptoms in PD may be induced by peripheral dysfunction associated with impaired facial mimicry. To our knowledge, only 2 studies tested this hypothesis.30, 133 By recording EMG responses during an FER task, authors showed that FER impairment was accompanied by disruption of facial mimicry in PD. During the experiment, facial expressions were mimicked as expected, but emotion‐specific EMG variations were disturbed among patients with weaker‐than‐normal corrugator and medial frontalis reactions in response to angry and sad faces respectively, and almost no reactions from the orbicularis and the zygomaticus in response to happy faces. These facial reactions could be linked to emotion‐decoding accuracy and response time: the weaker the responses, the lower the performance was. Neuroimaging and electrophysiological studies bring some very interesting elements here, suggesting a rearranging of the brain mechanisms underlying FER in PD.57, 72, 112, 134 Yoshimura et al57 have shown that event‐related potential recordings in response to fearful faces were generated within the parietal somatosensory cortex among patients instead of the amygdala and the visual temporal cortex as in HCs. Similarly, in accordance with Anders et al,134 who highlighted a ventrolateral premotor cortex compensatory activity during emotions processing in Parkin mutation carriers, Wabnegger et al72 showed a stronger activation in somatosensory regions among patients that was positively correlated with their recognition performance. The somatosensory recruitment could be considered a compensatory mechanism following dopamine depletion and/or pathological changes in the amygdala, which may overcome emotional deficits in PD. Finally, those results raise the question whether facial mimicry and its feedback to neural systems are a necessary part of the process of recognizing emotion through simulation. An alternative assumption stipulates that emotion recognition could only lie on sensorimotor simulation without measurable facial mimicry.127 In this view, FER impairment in PD could stem not from a disturbance of facial mimicry but from incongruent feedback that comes into conflict with the internal simulation of the observed facial expression. In any case, facial mimicry may not be mandatory but could constitute an interesting therapeutic lever to counteract FER deficit in PD when patients are asked to consciously imitate to accurately recognize.
Conclusion
Hypomimia has considerable repercussions on patients' (often perceived as bored, anxious or cranky135, 136, 137) and relatives' quality of life, damaging interpersonal relationships and gradually increasing social isolation.1, 138 Patients, caregivers, and clinicians can break this vicious cycle. It starts with awareness of the patients' difficulties in decoding, expressing, and mimicking emotions, along with their attendant social consequences. Research on these issues could also improve medical management, as therapeutic strategies can be adapted to patients' symptoms, especially knowing that there are several PD subtypes with 3 separate phenotypes: mainly motor/slow progression, intermediate, and diffuse/malignant.84 Patients with the latter are more likely to exhibit nonmotor symptoms, including cognitive and mood disorders, but patients with the main motor form may also develop emotional impairments as a consequence of impaired facial mimicry. Finally, these findings open up a new line of inquiry into patients' masked face and its impact on socioemotional communication among both patients and their caregivers.
Authors' roles
Supervision: Marc Vérin, Paul Sauleau, Didier Grandjean.
Design, execution and writing of the first draft: Soizic Argaud.
Review and critique: Marc Vérin, Didier Grandjean.
Acknowledgments
We warmly thank the National Center for Competence in Research (NCCR) in Affective Sciences at the University of Geneva for supporting Didier Grandjean, as well as Elizabeth Portier for revising the English style.
Relevant conflicts of interest/financial disclosures: The authors declare no competing financial interests.
Funding agencies: This work was supported by the Belgian pharmaceutical company UCB Pharma, the National Association of Patients with PD (France Parkinson), l'Association des Parkinsoniens d'Ille‐et‐Vilaine (APIV) and the National Center of Competence in Research Affective Sciences ‐ Emotions in Individual Behaviour and Social Processes (NCCR Affective Sciences; 51NF40‐104897 to D.G.). The funders had no role in study design, data collection and analysis, decision to publish, and preparation of the manuscript.
References
- 1. Bologna M, Fabbrini G, Marsili L, Defazio G, Thompson PD, Berardelli A. Facial bradykinesia. J Neurol Neurosurg Psychiatry 2013;84(6):681‐685. [DOI] [PubMed] [Google Scholar]
- 2. Defebvre L, Vérin M. La maladie de Parkinson. 3rd ed. Elsevier Masson; 2015. [Google Scholar]
- 3. Dissanayaka NNW, Sellbach A, Matheson S, et al. Anxiety disorders in Parkinson's disease: Prevalence and risk factors. Mov Disord. 2010;25(7):838‐45. [DOI] [PubMed] [Google Scholar]
- 4. García‐Ramos R, Villanueva C, Del Val J, Matías‐Guíu J. Apathy in Parkinson's disease. Neurol Engl Ed 2010;25(1):40‐50. [PubMed] [Google Scholar]
- 5. McKinlay A, Grace RC, Dalrymple‐Alford JC, Roger D. Cognitive characteristics associated with mild cognitive impairment in Parkinson's disease. Dement Geriatr Cogn Disord 2009;28(2):121‐129. [DOI] [PubMed] [Google Scholar]
- 6. Poewe W. Non‐motor symptoms in Parkinson's disease. Eur J Neurol 2008;15(s1):14‐20. [DOI] [PubMed] [Google Scholar]
- 7. Reijnders JSAM, Ehrt U, Weber WEJ, Aarsland D, Leentjens AFG. A systematic review of prevalence studies of depression in Parkinson's disease: The prevalence of depression in PD. Mov Disord. 2008;23(2):183‐189. [DOI] [PubMed] [Google Scholar]
- 8. Assogna F, Cravello L, Orfei MD, Cellupica N, Caltagirone C, Spalletta G. Alexithymia in Parkinson's disease: a systematic review of the literature. Parkinsonism Relat Disord 2016;28:1‐11. [DOI] [PubMed] [Google Scholar]
- 9. Péron J, Dondaine T, Le Jeune F, Grandjean D, Vérin M. Emotional processing in Parkinson's disease: a systematic review. Mov Disord 2011;27(2):186‐199. [DOI] [PubMed] [Google Scholar]
- 10. Schröder C, Nikolova Z, Dengler R. Changes of emotional prosody in Parkinson's disease. J Neurol Sci 2010;289(1):32‐35. [DOI] [PubMed] [Google Scholar]
- 11. Assogna F, Pontieri FE, Caltagirone C, Spalletta G. The recognition of facial emotion expressions in Parkinson's disease. Eur Neuropsychopharmacol 2008;18(11):835‐848. [DOI] [PubMed] [Google Scholar]
- 12. Gray HM, Tickle‐Degnen L. A meta‐analysis of performance on emotion recognition tasks in Parkinson's disease. Neuropsychology 2010;24(2):176‐91. [DOI] [PubMed] [Google Scholar]
- 13. Clark US, Neargarder S, Cronin‐Golomb A. Specific impairments in the recognition of emotional facial expressions in Parkinson's disease. Neuropsychologia 2008;46(9):2300‐2309. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14. Albuquerque L, Martins M, Coelho M, et al. Advanced Parkinson disease patients have impairment in prosody processing. J Clin Exp Neuropsychol. 2016;38(2):208‐216. [DOI] [PubMed] [Google Scholar]
- 15. Alonso‐Recio L, Martín P, Rubio S, Serrano JM. Discrimination and categorization of emotional facial expressions and faces in Parkinson's disease. J Neuropsychol 2013;8(2):269‐288. [DOI] [PubMed] [Google Scholar]
- 16. Ariatti A, Benuzzi F, Nichelli P. Recognition of emotions from visual and prosodic cues in Parkinson's disease. Neurol Sci 2008;29(4):219‐227. [DOI] [PubMed] [Google Scholar]
- 17. Borod JC, Welkowitz J, Alpert M, et al. Parameters of emotional processing in neuropsychiatric disorders: Conceptual issues and a battery of tests. J Commun Disord 1990;23(4):247‐271. [DOI] [PubMed] [Google Scholar]
- 18. Caekebeke JF, Jennekens‐Schinkel A, van der Linden ME, Buruma OJ, Roos RA. The interpretation of dysprosody in patients with Parkinson's disease. J Neurol Neurosurg Psychiatry 1991;54(2):145‐148. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19. Cohen H, Gagné M‐H, Hess U, Pourcher E. Emotion and object processing in Parkinson's disease. Brain Cogn 2010;72(3):457‐463. [DOI] [PubMed] [Google Scholar]
- 20. Haeske‐Dewick H. Are perception and memory for faces influenced by a specific age at onset factor in Parkinson's disease? Neuropsychologia 1996;34(4):315‐320. [DOI] [PubMed] [Google Scholar]
- 21. Herrera E, Cuetos F, Rodríguez‐Ferreiro J. Emotion recognition impairment in Parkinson's disease patients without dementia. J Neurol Sci 2011;310(1‐2):237‐240. [DOI] [PubMed] [Google Scholar]
- 22. Laskowska IP, Gawryś L, Łęski S, Koziorowski D. Emotional processing in Parkinson's disease and schizophrenia: evidence for response bias deficits in PD. Front Psychol 2015;6:1417. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23. Madeley P, Ellis AW, Mindham RH. Facial expressions and Parkinson's disease. Behav Neurol 1995;8(2):115‐119. [DOI] [PubMed] [Google Scholar]
- 24. Marneweck M, Palermo R, Hammond G. Discrimination and recognition of facial expressions of emotion and their links with voluntary control of facial musculature in Parkinson's disease. Neuropsychology 2014;28(6):917. [DOI] [PubMed] [Google Scholar]
- 25. Martínez‐Corral M, Pagonabarraga J, Llebaria G, et al. Facial emotion recognition impairment in patients with Parkinson's disease and isolated apathy. Park Dis 2010;2010:1‐5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26. Pietschnig J, Schröder L, Ratheiser I, et al. Facial emotion recognition and its relationship to cognition and depressive symptoms in patients with Parkinson's disease. Int Psychogeriatr 2016;28(07):1165‐1179. [DOI] [PubMed] [Google Scholar]
- 27. Ventura MI, Baynes K, Sigvardt KA, et al. Hemispheric asymmetries and prosodic emotion recognition deficits in Parkinson's disease. Neuropsychologia 2012;50(8):1936‐1945. [DOI] [PubMed] [Google Scholar]
- 28. Yip JTH, Lee TMC, Ho S‐L, Tsang K‐L, Li LSW. Emotion recognition in patients with idiopathic Parkinson's disease. Mov Disord 2003;18(10):1115‐1122. [DOI] [PubMed] [Google Scholar]
- 29. Alonso‐Recio L, Martín‐Plasencia P, Loeches‐Alonso Á, Serrano‐Rodríguez JM. Working memory and facial expression recognition in patients with Parkinson's disease. J Int Neuropsychol Soc 2014;20(05):496‐505. [DOI] [PubMed] [Google Scholar]
- 30. Argaud S, Delplanque S, Houvenaghel J‐F, et al. Does facial amimia impact the recognition of facial emotions? An EMG study in Parkinson's disease. PLoS One 2016;11(7):e0160329. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31. Dewick H, Hanley J, Davies A, Playfer J, Turnbull C. Perception and memory for faces in Parkinson's disease. Neuropsychologia 1991;29(8):785‐802. [DOI] [PubMed] [Google Scholar]
- 32. Dujardin K, Blairy S, Defebvre L, et al. Deficits in decoding emotional facial expressions in Parkinson's disease. Neuropsychologia 2004;42(2):239‐250. [DOI] [PubMed] [Google Scholar]
- 33. Ille R, Wabnegger A, Schwingenschuh P, et al. Intact emotion recognition and experience but dysfunctional emotion regulation in idiopathic Parkinson's disease. J Neurol Sci 2016;361:72‐78. [DOI] [PubMed] [Google Scholar]
- 34. Martins, Muresan A, Justo M, Simão C. Basic and social emotion recognition in patients with Parkinson disease. J Neurol Sci Turk. 2008;25(4). [Google Scholar]
- 35. Saenz A, Doé de Maindreville A, Henry A, de Labbey S, Bakchine S, Ehrlé N. Recognition of facial and musical emotions in Parkinson's disease. Eur J Neurol 2013;20(3):571‐577. [DOI] [PubMed] [Google Scholar]
- 36. Breitenstein C, Daum I, Ackermann H. Emotional processing following cortical and subcortical brain damage: contribution of the fronto‐striatal circuitry. Behav Neurol 1998;11(1):29‐42. [DOI] [PubMed] [Google Scholar]
- 37. Jacobs DH, Shuren J, Bowers D, Heilman KM. Emotional facial imagery, perception, and expression in Parkinson's disease. Neurology 1995;45(9):1696‐1702. [DOI] [PubMed] [Google Scholar]
- 38. Marneweck M, Hammond G. Discriminating facial expressions of emotion and its link with perceiving visual form in Parkinson's disease. J Neurol Sci 2014;346(1‐2):149‐155. [DOI] [PubMed] [Google Scholar]
- 39. Wagenbreth C, Wattenberg L, Heinze H‐J, Zaehle T. Implicit and explicit processing of emotional facial expressions in Parkinson's disease. Behav Brain Res 2016;303:182‐190. [DOI] [PubMed] [Google Scholar]
- 40. Liddell BJ, Brown KJ, Kemp AH, et al. A direct brainstem–amygdala–cortical “alarm” system for subliminal signals of fear. NeuroImage 2005;24(1):235‐243. [DOI] [PubMed] [Google Scholar]
- 41. Tamietto M, de Gelder B. Neural bases of the non‐conscious perception of emotional signals. Nat Rev Neurosci 2010;11(10):697‐709. [DOI] [PubMed] [Google Scholar]
- 42. Kawai N, Kubo K, Masataka N, Hayakawa S. Conserved evolutionary history for quick detection of threatening faces. Anim Cogn 2016;19(3):655‐660. [DOI] [PubMed] [Google Scholar]
- 43. LoBue V, Matthews K, Harvey T, Stark SL. What accounts for the rapid detection of threat? Evidence for an advantage in perceptual and behavioral responding from eye movements. Emotion 2014;14(4):816‐823. [DOI] [PubMed] [Google Scholar]
- 44. Quinlan PT. The visual detection of threat: a cautionary tale. Psychon Bull Rev 2013;20(6):1080‐1101. [DOI] [PubMed] [Google Scholar]
- 45. Assogna F, Pontieri FE, Cravello L, et al. Intensity‐dependent facial emotion recognition and cognitive functions in Parkinson's disease. J Int Neuropsychol Soc 2010;16(05):867‐876. [DOI] [PubMed] [Google Scholar]
- 46. Beatty WW, Goodkin DE, Weir WS, Staton RD, Monson N, Beatty PA. Affective judgments by patients with Parkinson's disease or chronic progressive multiple sclerosis. Bull Psychon Soc 1989;27(4):361‐364. [Google Scholar]
- 47. Narme P, Bonnet A‐M, Dubois B, Chaby L. Understanding facial emotion perception in Parkinson's disease: the role of configural processing. Neuropsychologia 2011;49(12):3295‐3302. [DOI] [PubMed] [Google Scholar]
- 48. Kan Y, Kawamura M, Hasegawa Y, Mochizuki S, Nakamura K. Recognition of emotion from facial, prosodic and written verbal stimuli in Parkinson's disease. Cortex J Devoted Study Nerv Syst Behav 2002;38(4):623‐630. [DOI] [PubMed] [Google Scholar]
- 49. McIntosh LG, Mannava S, Camalier CR, et al. Emotion recognition in early Parkinson's disease patients undergoing deep brain stimulation or dopaminergic therapy: a comparison to healthy participants. Front Aging Neurosci 2014;6:349. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 50. Paulmann S, Pell MD. Dynamic emotion processing in Parkinson's disease as a function of channel availability. J Clin Exp Neuropsychol 2010;32(8):822‐835. [DOI] [PubMed] [Google Scholar]
- 51. Krumhuber EG, Kappas A, Manstead AS. Effects of dynamic aspects of facial expressions: a review. Emot Rev 2013;5(1):41‐46. [Google Scholar]
- 52. Kessler H, Doyen‐Waldecker C, Hofer C, Hoffmann H, Traue HC, Abler B. Neural correlates of the perception of dynamic versus static facial expressions of emotion. GMS Pyscho‐Soc‐Med 2011;8:Doc03. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 53. Sato W, Kochiyama T, Yoshikawa S, Naito E, Matsumura M. Enhanced neural activity in response to dynamic facial expressions of emotion: an fMRI study. Cogn Brain Res 2004;20(1):81‐91. [DOI] [PubMed] [Google Scholar]
- 54. Trautmann SA, Fehr T, Herrmann M. Emotions in motion: Dynamic compared to static facial expressions of disgust and happiness reveal more widespread emotion‐specific activations. Brain Res 2009;1284:100‐115. [DOI] [PubMed] [Google Scholar]
- 55. Adolphs R. Recognizing emotion from facial expressions: psychological and neurological mechanisms. Behav Cogn Neurosci Rev 2002;1(1):21‐62. [DOI] [PubMed] [Google Scholar]
- 56. Pell MD, Leonard CL. Facial expression decoding in early Parkinson's disease. Brain Res Cogn Brain Res 2005;23(2‐3):327‐340. [DOI] [PubMed] [Google Scholar]
- 57. Yoshimura N, Kawamura M, Masaoka Y, Homma I. The amygdala of patients with Parkinson's disease is silent in response to fearful facial expressions. Neuroscience 2005;131(2):523‐534. [DOI] [PubMed] [Google Scholar]
- 58. Friesen WV, Ekman P. Pictures of Facial Affect. Consulting Psychologists Press; 1976. [Google Scholar]
- 59. Fevereisen P, Mallet C, Martin Y. Is the faster processing of expressions of happiness modality specific? In: Ellis HD, Jeeves MA, Newcombe F, Young A. Aspects of Face Processing. Boston: Nijhoff; 1986;349‐355. [Google Scholar]
- 60. Palermo R, Coltheart M. Photographs of facial expression: Accuracy, response times, and ratings of intensity. Behav Res Methods 2004;36(4):634‐638. [DOI] [PubMed] [Google Scholar]
- 61. Leppanen JM, Hietanen JK. Positive facial expressions are recognized faster than negative facial expressions, but why? Psychol Res Psychol Forsch 2004;69(1‐2):22‐29. [DOI] [PubMed] [Google Scholar]
- 62. Tottenham N, Tanaka JW, Leon AC, et al. The NimStim set of facial expressions: Judgments from untrained research participants. Psychiatry Res 2009;168(3):242‐249. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 63. Calvo MG, Beltrán D. Recognition advantage of happy faces: tracing the neurocognitive processes. Neuropsychologia 2013;51(11):2051‐2061. [DOI] [PubMed] [Google Scholar]
- 64. Baggio HC, Segura B, Ibarretxe‐Bilbao N, et al. Structural correlates of facial emotion recognition deficits in Parkinson's disease patients. Neuropsychologia 2012;50(8):2121‐2128. [DOI] [PubMed] [Google Scholar]
- 65. Enrici I, Adenzato M, Ardito RB, Mitkova A, Cavallo M, Zibetti M, et al. Emotion processing in Parkinson's disease: A three‐level study on recognition, representation and regulation. PLoS One. 2015;10(6):e0131470. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 66. Ibarretxe‐Bilbao N, Junque C, Tolosa E, et al. Neuroanatomical correlates of impaired decision‐making and facial emotion recognition in early Parkinson's disease. Eur J Neurosci 2009;30(6):1162‐1171. [DOI] [PubMed] [Google Scholar]
- 67. Narme P, Mouras H, Roussel M, Duru C, Krystkowiak P, Godefroy O. Emotional and cognitive social processes are impaired in Parkinson's disease and are related to behavioral disorders. Neuropsychology 2013;27(2):182‐192. [DOI] [PubMed] [Google Scholar]
- 68. Sprengelmeyer R, Young AW, Mahn K, et al. Facial expression recognition in people with medicated and unmedicated Parkinson's disease. Neuropsychologia 2003;41(8):1047‐1057. [DOI] [PubMed] [Google Scholar]
- 69. Blonder LX, Gur RE, Gur RC. The effects of right and left hemiparkinsonism on prosody. Brain Lang. 1989;36(2):193‐207. [DOI] [PubMed] [Google Scholar]
- 70. Suzuki A, Hoshino T, Shigemasu K, Kawamura M. Disgust‐specific impairment of facial expression recognition in Parkinson's disease. Brain 2006;129(3):707‐717. [DOI] [PubMed] [Google Scholar]
- 71. Adolphs R, Schul R, Tranel D. Intact recognition of facial emotion in Parkinson's disease. Neuropsychology 1998;12(2):253‐258. [DOI] [PubMed] [Google Scholar]
- 72. Wabnegger A, Ille R, Schwingenschuh P, et al. Facial emotion recognition in Parkinson's disease: An fMRI investigation. PLoS One 2015;10(8):e0136110. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 73. Dondaine T, Robert G, Péron J, et al. Biases in facial and vocal emotion recognition in chronic schizophrenia. Front Psychol 2014;5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 74. Péron J, El Tamer S, Grandjean D, et al. Major depressive disorder skews the recognition of emotional prosody. Prog Neuropsychopharmacol Biol Psychiatry 2011;35(4):987‐996. [DOI] [PubMed] [Google Scholar]
- 75. Hipp G, Diederich NJ, Pieria V, Vaillant M. Primary vision and facial emotion recognition in early Parkinson's disease. J Neurol Sci 2014;338(1‐2):178‐82. [DOI] [PubMed] [Google Scholar]
- 76. Lin CY, Tien YM, Huang JT, Tsai CH, Hsu LC. Degraded impairment of emotion recognition in Parkinson's disease extends from negative to positive emotions. Behav Neurol 2016;2016:1‐8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 77. Hoehn MM, Yahr MD. Parkinsonism: onset, progression, and mortality. Neurology 1967;57(10 Suppl 3):S11‐S26. [PubMed] [Google Scholar]
- 78. Fahn S, Elton R, Committee UD, others. Unified Parkinson's Disease Rating Scale Fahn S, Marsden CD, Goldstein M, et al, eds. Recent Developments in Parkinson's Disease II. New York: Macmillan; 1987:153‐163. [Google Scholar]
- 79. Goetz CG, Poewe W, Rascol O, et al. Movement Disorder Society Task Force report on the Hoehn and Yahr staging scale: status and recommendations. Mov Disord 2004;19(9):1020‐1028. [DOI] [PubMed] [Google Scholar]
- 80. Buxton SL, MacDonald L, Tippett LJ. Impaired recognition of prosody and subtle emotional facial expressions in Parkinson's disease. Behav Neurosci 2013;127(2):193‐203. [DOI] [PubMed] [Google Scholar]
- 81. Wieser MJ, Klupp E, Weyers P, et al. Reduced early visual emotion discrimination as an index of diminished emotion processing in Parkinson's disease? – Evidence from event‐related brain potentials. Cortex 2012;48(9):1207‐1217. [DOI] [PubMed] [Google Scholar]
- 82. Halliday G, Hely M, Reid W, Morris J. The progression of pathology in longitudinally followed patients with Parkinson's disease. Acta Neuropathol (Berl) 2008;115(4):409‐415. [DOI] [PubMed] [Google Scholar]
- 83. Pagano G, Ferrara N, Brooks DJ, Pavese N. Age at onset and Parkinson disease phenotype. Neurology 2016;86(15):1400‐407. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 84. Fereshtehnejad S‐M, Romenets SR, Anang JBM, Latreille V, Gagnon J‐F, Postuma RB. New clinical subtypes of Parkinson's disease and their longitudinal progression: A prospective cohort comparison with other phenotypes. JAMA Neurol 2015;72(8):863. [DOI] [PubMed] [Google Scholar]
- 85. Najt P, Bayer U, Hausmann M. Models of hemispheric specialization in facial emotion perception—a reevaluation. Emotion 2013;13(1):159‐167. [DOI] [PubMed] [Google Scholar]
- 86. Verreyt N, Nys GMS, Santens P, Vingerhoets G. Cognitive differences between patients with left‐sided and right‐sided Parkinson's disease. A review. Neuropsychol Rev 2011;21(4):405‐424. [DOI] [PubMed] [Google Scholar]
- 87. Ricciardi L, Bologna M, Morgante F, et al. Reduced facial expressiveness in Parkinson's disease: A pure motor disorder? J Neurol Sci 2015;358(1‐2):125‐30. [DOI] [PubMed] [Google Scholar]
- 88. Wu P, Gonzalez I, Patsis G, et al. Objectifying Facial expressivity assessment of Parkinson's patients: preliminary study. Comput Math Methods Med 2014;2014:1‐12. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 89. Bandini A, Orlandi S, Escalante HJ, et al. Analysis of facial expressions in parkinson's disease through video‐based automatic methods. J Neurosci Methods 2017;281:7‐20. [DOI] [PubMed] [Google Scholar]
- 90. Benton AL, Hamsher K de S, Varney NR, Spreen O. Contributions to neuropsychological assessment. New York: Oxford University Press; 1983. [Google Scholar]
- 91. Lachenal‐Chevallet K, Bediou B, Bouvard M, et al. Troubles de la reconnaissance des expressions faciales émotionnelles dans la maladie de Parkinson. Psychol Neuropsychiatr Vieil 2006;4(1):61‐67. [PubMed] [Google Scholar]
- 92. Clark US, Neargarder S, Cronin‐Golomb A. Visual exploration of emotional facial expressions in Parkinson's disease. Neuropsychologia 2010;48(7):1901‐1913. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 93. Dujardin K, Tard C, Duhamel A, et al. The pattern of attentional deficits in Parkinson's disease. Parkinsonism Relat Disord 2013;19(3):300‐305. [DOI] [PubMed] [Google Scholar]
- 94. Lawrence AD, Goerendt IK, Brooks DJ. Impaired recognition of facial expressions of anger in Parkinson's disease patients acutely withdrawn from dopamine replacement therapy. Neuropsychologia 2007;45(1):65‐74. [DOI] [PubMed] [Google Scholar]
- 95. Alonso‐Recio L, Serrano JM, Martin P. Selective Attention and facial Expression recognition in patients with Parkinson's disease. Arch Clin Neuropsychol 2014;29(4):374‐384. [DOI] [PubMed] [Google Scholar]
- 96. Bourke C, Douglas K, Porter R. Processing of facial emotion expression in major depression: a review. Aust N Z J Psychiatry 2010;44(8):681‐696. [DOI] [PubMed] [Google Scholar]
- 97. Delle‐Vigne D, Wang W, Kornreich C, Verbanck P, Campanella S. Emotional facial expression processing in depression: data from behavioral and event‐related potential studies. Neurophysiol Clin Neurophysiol 2014;44(2):169‐187. [DOI] [PubMed] [Google Scholar]
- 98. Remy P, Doder M, Lees A, Turjanski N, Brooks D. Depression in Parkinson's disease: loss of dopamine and noradrenaline innervation in the limbic system. Brain 2005;128(6):1314‐1322. [DOI] [PubMed] [Google Scholar]
- 99. Starkstein SE, Brockman S. Apathy and Parkinson's disease. Curr Treat Options Neurol 2011;13(3):267‐273. [DOI] [PubMed] [Google Scholar]
- 100. Robert G, Le Jeune F, Dondaine T, et al. Apathy and impaired emotional facial recognition networks overlap in Parkinson's disease: a PET study with conjunction analyses. J Neurol Neurosurg Psychiatry 2014;85(10):1153‐1158. [DOI] [PubMed] [Google Scholar]
- 101. Tessitore A, Hariri AR, Fera F, et al. Dopamine modulates the response of the human amygdala: a study in Parkinson's disease. J Neurosci 2002;22(20):9099‐9103. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 102. Delaveau P, Salgado‐Pineda P, Fossati P, Witjas T, Azulay J‐P, Blin O. Dopaminergic modulation of the default mode network in Parkinson's disease. Eur Neuropsychopharmacol 2010;20(11):784‐792. [DOI] [PubMed] [Google Scholar]
- 103. Lawrence AD, Calder AJ, McGowan SW, Grasby PM. Selective disruption of the recognition of facial expressions of anger. Neuroreport 2002;13(6):881‐884. [DOI] [PubMed] [Google Scholar]
- 104. Takahashi H, Yahata N, Koeda M, et al. Effects of dopaminergic and serotonergic manipulation on emotional processing: A pharmacological fMRI study. Neuroimage 2005;27(4):991‐1001. [DOI] [PubMed] [Google Scholar]
- 105. Delaveau P, Salgado‐Pineda P, Micallef‐Roll J, Blin O. Amygdala activation modulated by levodopa during emotional recognition processing in healthy volunteers: A double‐blind, placebo‐controlled study. J Clin Psychopharmacol 2007;27(6):692‐697. [DOI] [PubMed] [Google Scholar]
- 106. Delaveau P, Salgado‐Pineda P, Witjas T, et al. Dopaminergic modulation of amygdala activity during emotion recognition in patients with Parkinson disease. J Clin Psychopharmacol 2009;29(6):548‐554. [DOI] [PubMed] [Google Scholar]
- 107. Braak H, Ghebremedhin E, Rüb U, Bratzke H, Del Tredici K. Stages in the development of Parkinson's disease‐related pathology. Cell Tissue Res 2004;318(1):121‐134. [DOI] [PubMed] [Google Scholar]
- 108. MacDonald AA, Monchi O, Seergobin KN, Ganjavi H, Tamjeedi R, MacDonald PA. Parkinson's disease duration determines effect of dopaminergic therapy on ventral striatum function: Testing the dopamine overdose hypothesis. Mov Disord 2013;28(2):153‐160. [DOI] [PubMed] [Google Scholar]
- 109. Péron J, Grandjean D, Drapier S, Vérin M. Effect of dopamine therapy on nonverbal affect burst recognition in Parkinson's disease. Fleming S, editor. PLoS One 2014;9(3):e90092. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 110. Tomlinson CL, Stowe R, Patel S, Rick C, Gray R, Clarke CE. Systematic review of levodopa dose equivalency reporting in Parkinson's disease. Mov Disord 2010;25(15):2649‐2653. [DOI] [PubMed] [Google Scholar]
- 111. Ouchi Y, Yoshikawa E, Okada H, et al. Alterations in binding site density of dopamine transporter in the striatum, orbitofrontal cortex, and amygdala in early Parkinson's disease: Compartment analysis for β‐CFT binding with positron emission tomography. Ann Neurol 1999;45(5):601‐610. [PubMed] [Google Scholar]
- 112. Lotze M, Reimold M, Heymans U, Laihinen A, Patt M, Halsband U. Reduced ventrolateral fMRI response during observation of emotional gestures related to the degree of dopaminergic impairment in Parkinson's disease. J Cogn Neurosci 2009;21(7):1321‐1331. [DOI] [PubMed] [Google Scholar]
- 113. Junqué C, Ramírez‐Ruiz B, Tolosa E, et al. Amygdalar and hippocampal MRI volumetric reductions in Parkinson's disease with dementia. Mov Disord 2005;20(5):540‐544. [DOI] [PubMed] [Google Scholar]
- 114. Ramírez–Ruiz B, Martí MJ, Tolosa E, et al. Longitudinal evaluation of cerebral morphological changes in Parkinson's disease with and without dementia. J Neurol 2005;252(11):1345‐1352. [DOI] [PubMed] [Google Scholar]
- 115. Braak H, Bohl JR, Müller CM, Rüb U, de Vos RAI, Del Tredici K. Stanley Fahn Lecture 2005: The staging procedure for the inclusion body pathology associated with sporadic Parkinson's disease reconsidered. Mov Disord 2006;21(12):2042‐2051. [DOI] [PubMed] [Google Scholar]
- 116. Hawkes CH, Del Tredici K, Braak H. A timeline for Parkinson's disease. Parkinsonism Relat Disord 2010;16(2):79‐84. [DOI] [PubMed] [Google Scholar]
- 117. Armony JL. Current emotion research in behavioral neuroscience: the role (s) of the amygdala. Emot Rev 2013;5(1):104‐115. [Google Scholar]
- 118. Murray RJ, Brosch T, Sander D. The functional profile of the human amygdala in affective processing: Insights from intracranial recordings. Cortex 2014;60:10‐33. [DOI] [PubMed] [Google Scholar]
- 119. Diederich NJ, Goldman JG, Stebbins GT, Goetz CG. Failing as doorman and disc jockey at the same time: Amygdalar dysfunction in Parkinson's disease: Amygdala in PD. Mov Disord 2016;31(1):11‐22. [DOI] [PubMed] [Google Scholar]
- 120. Péron J, Frühholz S, Vérin M, Grandjean D. Subthalamic nucleus: A key structure for emotional component synchronization in humans. Neurosci Biobehav Rev 2013;37(3):358‐373. [DOI] [PubMed] [Google Scholar]
- 121. Nambu A, Tokuno H, Takada M. Functional significance of the cortico–subthalamo–pallidal “hyperdirect” pathway. Neurosci Res 2002;43(2):111‐117. [DOI] [PubMed] [Google Scholar]
- 122. Graybiel AM. Habits, rituals, and the evaluative brain. Annu Rev Neurosci 2008;31:359‐387. [DOI] [PubMed] [Google Scholar]
- 123. Le Jeune F, Péron J, Biseul I, et al. Subthalamic nucleus stimulation affects orbitofrontal cortex in facial emotion recognition: a pet study. Brain 2008;131(6):1599‐608. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 124. Geday J, Ostergaard K, Gjedde A. Stimulation of subthalamic nucleus inhibits emotional activation of fusiform gyrus. Neuroimage 2006;33(2):706‐714. [DOI] [PubMed] [Google Scholar]
- 125. Goldman A, Sripada CS. Simulationist models of face‐based emotion recognition. Cognition 2005;94(3):193‐213. [DOI] [PubMed] [Google Scholar]
- 126. Gallese V. Embodied simulation: from neurons to phenomenal experience. Phenomenol Cogn Sci 2005;4(1):23‐48. [Google Scholar]
- 127. Wood A, Lupyan G, Sherrin S, Niedenthal P. Altering sensorimotor feedback disrupts visual discrimination of facial expressions. Psychon Bull Rev 2016;23(4):1150‐1156. [DOI] [PubMed] [Google Scholar]
- 128. Niedenthal PM, Barsalou LW, Winkielman P, Krauth‐Gruber S, Ric F. Embodiment in attitudes, social perception, and emotion. Personal Soc Psychol Rev 2005;9(3):184‐211. [DOI] [PubMed] [Google Scholar]
- 129. Hess U, Fischer A. Emotional mimicry: why and when we mimic emotions? Soc Personal Psychol Compass 2014;8(2):45‐57. [Google Scholar]
- 130. Korb S, With S, Niedenthal P, Kaiser S, Grandjean D. The perception and mimicry of facial movements predict judgments of smile authenticity. PLoS One 2014;9(6):e99194. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 131. Kunecke J, Hildebrandt A, Recio G, Sommer W, Wilhelm O. Facial EMG responses to emotional expressions are related to emotion perception ability. PLoS One. 2014;9(1):e84053. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 132. Sato W, Fujimura T, Kochiyama T, Suzuki N. Relationships among facial mimicry, emotional experience, and emotion recognition. PLoS One 2013;8(3):e57889. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 133. Livingstone SR, Vezer E, McGarry LM, Lang AE, Russo FA. Deficits in the mimicry of facial expressions in Parkinson's disease. Front Psychol 2016;7:780. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 134. Anders S, Sack B, Pohl A, et al. Compensatory premotor activity during affective face processing in subclinical carriers of a single mutant Parkin allele. Brain J Neurol 2012;135(Pt 4):1128‐1140. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 135. Hemmesch AR, Tickle‐Degnen L, Zebrowitz LA. The influence of facial masking and sex on older adults' impressions of individuals with Parkinson's disease. Psychol Aging 2009;24(3):542‐549. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 136. Pentland B, Gray JM, Riddle WJ, Pitcairn TK. The effects of reduced non‐verbal communication in Parkinson's disease. Br J Disord Commun 1988;23(1):31‐34. [DOI] [PubMed] [Google Scholar]
- 137. Tickle‐Degnen L, Lyons KD. Practitioners' impressions of patients with Parkinson's disease: the social ecology of the expressive mask. Soc Sci Med 2004;58(3):603‐614. [DOI] [PubMed] [Google Scholar]
- 138. Jankovic J. Parkinson's disease: clinical features and diagnosis. J Neurol Neurosurg Psychiatry 2008;79(4):368‐376. [DOI] [PubMed] [Google Scholar]