

Dear editor,
Inguinal hernias affect 5% of children and are usually defined as a protrusion of intestine or omentum through abdominal wall or inguinal canal defects.[1] Inguinal hernias may contain structures other than bowel and unique cases have been documented since the early 1900’s.[2–10] Ultrasound has been demonstrated to differentiate superficial swellings and has been used by radiologists to evaluate inguinal masses for decades.[1–5,11–13] Although the use of radiology-performed ultrasound for the diagnosis of congenital inguinal hernias containing ovaries, uterus, and fallopian tubes has been documented; the use of point-of-care ultrasound for the evaluation of the acute inguinal mass prior to reduction has not been demonstrated. Accurate identification by the emergency physician of the herniated structures may lead to earlier diagnosis, faster consultation, improve patient management, and superior patient outcomes.
CASE
An 11-year-old girl presented to an emergency department (ED) with the complaint of sudden onset bulging mass in the left groin. The patient stated that she had a sudden onset of pain after wrestling with her brother and subsequently noticed the mass in her left groin. Due to the patient’s persistent pain and nausea, she was brought in to be evaluated. Upon presentation, the patient was noted to be well appearing and in noticeable pain. On exam, the patient had a palpable inguinal mass. The mass was firm, and there was no discoloration of the skin. The physician immediately attempted to reduce the mass but was unsuccessful. Prior to the second failed attempt at reduction, the patient was placed in Trendelenburg position, an ice pack was applied to the affected groin, and intravenous pain medications were administered. Due to the possibility for incarceration and the need for surgical evaluation, the patient was transferred to a tertiary care hospital for surgical evaluation. No further manipulations, imaging, or lab studies were performed in order to facilitate rapid transfer.
Upon arrival to the tertiary care ED, the patient was pain free, did not have systemic symptoms, but continued to have a firm mass in her left groin. The emergency physician immediately performed a point-of-care ultrasound of the inguinal region and the findings were consistent with a herniated ovary (Figures 1–4). The pediatric surgeon was consulted and arrived promptly. Ultrasound images and findings were reviewed and discussed with the pediatric surgeon. As a result of the ultrasound imaging, the decision was made to take the patient directly to the operating room (OR). As the patient and OR were prepared, a radiology-performed ultrasound was obtained per the consultant’s request. The additional study did not alter patient management but confirmed the point-of-care ultrasound findings and diagnosis of herniated ovary. Surgical exploration revealed a well-perfused herniated ovary and fallopian tube through the inguinal canal. The patient’s ovary and fallopian tube were salvaged, and the patient was discharged without additional complications. Although the patient has not had subsequent genetic testing, the patient received a comprehensive pelvic ultrasound 2 years after the event that demonstrated normal appearing bilateral ovaries, an anteverted uterus with normal echotexture, and a uniform and homogenous endometrial stripe measuring 5 mm.
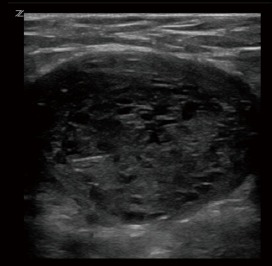
Figure 1.

Left inguinal region superior to herniated ovary.
Figure 2.

Left inguinal region in sagittal plane, demonstrating the left adnexa ventral to the left superior pubic ramus.
Figure 3.
Left inguinal region with herniated left ovary.
Figure 4.

Doppler ultrasound demonstrating normal appearing arterial flow to the left ovary.
DISCUSSION
Patients who present to the ED with complaints of an inguinal mass often have a primary attempt at manual reduction of the hernia by the emergency physician. This patient population is at risk for incarceration and subsequent ischemia, therefore current recommendations are to attempt gentle reduction with or without the use of sedation prior to emergent surgery.[14–16] When reduction is not successful, urgent consultation with the appropriate surgical specialty is obtained for repeat attempt at reduction or definitive operative repair. Although, the diagnosis of an inguinal hernia is generally made clinically by examining the inguinal canal and external genitalia, inadequate identification of the contents of inguinal hernias may lead to injury or complications. Point-of-care ultrasound can help the clinician evaluate the herniated anatomy and thereby consult the correct surgical specialists. In this case, reducing an ovarian hernia that has threatened blood supply can lead to torsion, necrosis and organ loss.
Traditionally, sonographic evaluation has been performed when attempts at manual reduction are unsuccessful. Ultrasound has been considered a valuable tool in the diagnosis of inguinal contents for many years. In fact, in 1984, Dr. Goske published a case series demonstrating the utility of using real-time ultrasound in the diagnosis of inguinal hernias with correct identification of the contents of the hernia sac.[15,16] With high-frequency transducers, ultrasound has become very reliable in determining the hernia sac and assessing its content. In addition, evaluating the inguinal mass for vascularity or vascular compromise can be assessed by a simultaneous Doppler examination. Although Doppler can provide very useful information, clinicians should be aware that incomplete or intermittent ovarian torsion can demonstrate normal or increased arterial and venous flow. Additionally, the presence of flow does not necessarily rule out torsion because of dual blood supply to the ovary.[7,8] In our case, point-of-care ultrasound of the inguinal hernia prevented further attempts at manual reduction and facilitated rapid transfer to the operating room. A proposed algorithm for the management of incarcerated inguinal hernias is presented in Figure 5.
Figure 5.

Therapeutic algorithm for incarcerated inguinal hernias.
By applying basic ultrasound skills in unusual presentations, emergency providers can decrease delays to definitive diagnosis and treatment. If the initial treating physicians in our case had performed the point-of-care ultrasound and found the herniated ovary, they likely would not have conducted numerous attempts at reduction. In addition, this patient could have potentially suffered ovarian torsion or necrosis had the consultant performed further reduction attempts.
CONCLUSIONS
Point-of-care ultrasound can prevent the misdiagnosis of complicated inguinal hernias, expedite consultation, and accelerate the appropriate management plan.
Footnotes
Funding: None.
Ethical approval: Not needed.
Conflicts of interest: The authors declare there is no competing interest related to the study, authors, other individuals or organizations.
Contributors: RA proposed the study and wrote the first draft. All authors read and approved the final version of the paper.
References
- 1.Bronsther B, Abrams MW, Elboim C. Inguinal hernias in children--a study of 1,000 cases and a review of the literature. J Am Med Womens Assoc. 1972;27(10):522–5. passim. [PubMed] [Google Scholar]
- 2.Değirmenci NA, Ozkan IR, Ilhan H. Case report:Ovarian torsion in inguinal canal. Tani Girisim Radyol. 2003;9(3):388–90. [PubMed] [Google Scholar]
- 3.Kaya O, Esen K, Gulek B, Yilmaz C, Soker G, Onem O. The inguinal herniation of the ovary in the newborn:ultrasound and color Doppler ultrasound findings. Case Rep Radiol. 2014;2014:281280. doi: 10.1155/2014/281280. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Ming YC, Luo CC, Chao HC, Chu SM. Inguinal hernia containing uterus and uterine adnexa in female infants:report of two cases. Pediatr Neonatol. 2011;52(2):103–5. doi: 10.1016/j.pedneo.2011.02.006. [DOI] [PubMed] [Google Scholar]
- 5.Yang DM, Kim HC, Kim SW, Lim SJ, Park SJ, Lim JW. Ultrasonographic diagnosis of ovary-containing hernias of the canal of Nuck. Ultrasonography. 2014;33(3):178–83. doi: 10.14366/usg.14010. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Artas H, Gurbuzer N. Inguinal hernia containing both ovaries and the uterus in an infant. J Ultrasound Med. 2012;31(7):1138–9. doi: 10.7863/jum.2012.31.7.1138. [DOI] [PubMed] [Google Scholar]
- 7.Jedrzejewski G, Stankiewicz A, Wieczorek AP. Uterus and ovary hernia of the canal of Nuck. Pediatr Radiol. 2008;38(11):1257–8. doi: 10.1007/s00247-008-0959-x. [DOI] [PubMed] [Google Scholar]
- 8.Laing FC, Townsend BA, Rodriguez JR. Ovary-containing hernia in a premature infant:sonographic diagnosis. J Ultrasound Med. 2007;26(7):985–7. doi: 10.7863/jum.2007.26.7.985. [DOI] [PubMed] [Google Scholar]
- 9.Okada T, Sasaki S, Honda S, Miyagi H, Minato M, Todo S. Irreducible indirect inguinal hernia containing uterus, ovaries, and Fallopian tubes. Hernia. 2012;16(4):471–3. doi: 10.1007/s10029-010-0764-y. [DOI] [PubMed] [Google Scholar]
- 10.Yao L, Mou Y, Wang HX. Sonographic diagnosis of an ovary-containing inguinal hernia with the formation of a corpus luteum in an adult female. Ultrasound Obstet Gynecol. 2009;34(3):359–60. doi: 10.1002/uog.7331. [DOI] [PubMed] [Google Scholar]
- 11.Lau ST, Lee YH, Caty MG. Current management of hernias and hydroceles. Semin Pediatr Surg. 2007;16(1):50–7. doi: 10.1053/j.sempedsurg.2006.10.007. [DOI] [PubMed] [Google Scholar]
- 12.Patel B, Zivin S, Panchal N, Wilbur A, Bresler M. Sonography of female genital hernias presenting as labia majora masses. J Ultrasound Med. 2014;33(1):155–9. doi: 10.7863/ultra.33.1.155. [DOI] [PubMed] [Google Scholar]
- 13.Aydin R, Polat AV, Ozaydin I, Aydin G. Gray-scale and color Doppler ultrasound imaging findings of an ovarian inguinal hernia and torsion of the herniated ovary:a case report. Pediatr Emerg Care. 2013;29(3):364–5. doi: 10.1097/PEC.0b013e318285465c. [DOI] [PubMed] [Google Scholar]
- 14.Grosfeld JL. Current concepts in inguinal hernia in infants and children. World J Surg. 1989;13(5):506–15. doi: 10.1007/BF01658863. [DOI] [PubMed] [Google Scholar]
- 15.Goske MJ, Emmens RW, Rabinowitz R. Inguinal ovaries in children demonstrated by high resolution real-time ultrasound. Radiology. 1984;151(3):635–6. doi: 10.1148/radiology.151.3.6718721. [DOI] [PubMed] [Google Scholar]
- 16.Goldstein IR, Potts WJ. Inguinal hernia in female infants and children. Ann Surg. 1958;148(5):819–22. doi: 10.1097/00000658-195811000-00013. [DOI] [PMC free article] [PubMed] [Google Scholar]