

Abstract
Meningiomas are the most common primary intracranial tumor. Important advances are occurring in meningioma research. These are expected to accelerate, potentially leading to impactful changes on the management of meningiomas in the near and medium term. This review will cover the histo- and molecular pathology of meningiomas, including recent 2016 updates to the WHO classification of CNS tumors. We will discuss clinical and radiographic presentation and therapeutic management. Surgery and radiotherapy, the two longstanding primary therapeutic modalities, will be discussed at length. In addition, data from prior and ongoing investigations of other treatment modalities, including systemic and targeted therapies, will be covered. This review will quickly update the reader on the contemporary management and future directions in meningiomas.
Keywords: : chemotherapy, imaging, meningioma, molecular pathology, mutations, radiotherapy, stereotactic radiosurgery, surgery, targeted therapy, tumor treating fields
Meningiomas are the most common primary tumor of the CNS and were well described in the centuries before Harvey Cushing coined the term in 1922 [1]. These dural-based tumors are routinely encountered not only by neurologists and neurosurgeons, but also by general clinicians. Despite a reputation as a purely benign disease, meningiomas are frequently associated with morbidity such as focal neurological deficits, seizures and decreased quality of life. In this review, we will discuss the clinical and molecular features of meningioma, the present standard of care treatment and key clinical trials that inform current decision-making, as well as ongoing trials for molecularly defined meningioma subtypes.
Epidemiology
Meningiomas comprise 36.6% of all primary CNS tumors, as reported by histology, and 53.2% of nonmalignant primary CNS tumors in the USA [2]. Meningioma has an overall incidence of 8.3 per 100,000 persons during the period 2010–2014, which has increased over the past decade from a rate of 4.52 during the period 1998–2002 [2,3]. Meningioma incidence is quite age dependent, increasing from 0.14 per 100,000 in children 0–19 years to 37.75 per 100,000 in the 75–84 year age group [2]. It remains unclear if the increased overall incidence of these tumors is true or due to more frequent incidental detection of these tumors by neuro-imaging or improved accuracy of disease reporting. Data also reveal an increasing incidence with age and increased prevalence in African–Americans compared with Caucasians and 2.27:1 female predominance [2]. It is thought that this female predilection correlates, at least in part, with endogenous sex hormone levels and is even higher (∼3:1) during child-bearing years [4]. Of those meningiomas with documented WHO grade, 81.1% are grade I (typical), 16.9% are grade II (atypical) and 1.7% are grade III (anaplastic) [2].
Ionizing radiation to the skull is considered a risk factor for the development of meningioma, with from a six to tenfold relative risk following a variable latency period, and without a clear dose–response relationship [5]. Furthermore, epidemiological associations, such as a history of head trauma, cigarette smoking and cellular phone use, have not been consistently shown as associated with significantly increased risk of meningioma, although such studies are often confounded by recall biases and frequently lack pathologic confirmation.
There are several familial syndromes that predispose meningioma development, with the most common hereditary cause being neurofibromatosis type 2 (NF2), an autosomal dominant condition. In the general population, phenotypic NF2 is rare and seen in <1% of meningioma cases [6]. Other notable meningioma-associated syndromes include Li-Fraumeni, Gorlin, von Hippel-Lindau, Cowden disease and multiple endocrine neoplasia (MEN) type 1 [1].
Clinical presentation
The presentation of meningiomas, like other CNS tumors, depends upon their location. Meningiomas can be found arising from any intracranial or spinal dural surface. Rarely, intraventricular meningiomas are identified. Meningiomas are typically not fast growing or infiltrative lesions, and they have an insidious symptom onset. Many are discovered incidentally on brain imaging. While there is no pathognomonic presentation of meningioma, clinical symptoms of headache due to increased intracranial pressure, focal neurological (including cranial nerve) deficits or generalized and partial seizures caused by focal mass effect, are typical. Personality changes, confusion and altered level of consciousness can be seen, especially in anterior (frontal) or parasagittal meningiomas, and they may be initially misdiagnosed as dementia or depression. The differential diagnosis of a patient presenting with such symptoms is quite broad and should include other intracranial lesions (such a glioma or metastatic tumors).
Natural history & prognosis
An important concern for patients and clinicians is the natural course of tumors, especially when incidentally detected. While biopsy or resection is the only method to definitively confirm diagnosis, through histopathologic analysis, a typical radiologic appearance is often sufficient and remains the most common technique for diagnosing meningioma (see the section ‘Radiological diagnosis & imaging characteristics of meningioma & the role of advanced imaging’). Several observational studies have shown a linear growth rate of 2–4 mm/year for asymptomatic meningioma [1]. Some tumors, however, display nonlinear, exponential growth patterns or no growth at all, underscoring the importance of surveillance imaging in untreated patients [7]. Moreover, it is thought that larger, symptomatic meningiomas have a different natural history and more aggressive growth pattern, but since these tumors are rarely left untreated, their true natural history is not well understood [6].
Estimated 10-year overall survival for meningioma is 57.1 and 77.7% for patients at a younger age at diagnosis (20–44 years) [2]. The natural history of grade II and grade III tumors is much more aggressive, with rates of recurrence at 5 years approximating 50% for grade II tumors and 90% for grade III tumors. These recurrences translate into meningioma-specific mortality in these patients, with 10-year overall survival rates of 53% for grade II patients and 0% for grade III patients, despite aggressive therapeutic efforts.
The definition of tumor recurrence or progression is complicated for meningioma. The term progression when discussing meningiomas is utilized to describe the growth of residual tumor. It can also be used to describe transformation from a lower to a higher grade tumor (e.g., from grade I to WHO grade II). Although there is often stability (lack of growth) following nonsurgical treatment with radiation therapy, meningiomas rarely demonstrate decrease in size (radiographic response). There has not been a consensus definition of treatment response or progression for meningioma, but a response assessment in neuro-oncology (RANO) working group currently seeks to establish one for clinician and clinical trial use [6]. Various strategies to assess tumor growth have been evaluated, such as linear 2D versus volumetric 3D growth versus growth rate, but none is a standard [7–9]. Precedent for both types of approaches exists in neuro-oncology. The use of change in cross-sectional area is routinely utilized in high-grade gliomas [10] and volumetric reduction has been successfully utilized in trials of systemic therapies for subependymal giant cell astrocytomas [11]. Moreover, as most published studies of meningioma treatment have applied imaging-based end points (response rate, progression-free survival, time to tumor recurrence) as the primary outcome measures, potential impact on survival is difficult to discern because meningiomas often remain radiographically stable in response to nonsurgical treatments.
Radiological diagnosis & imaging characteristics of meningioma & the role of advanced imaging
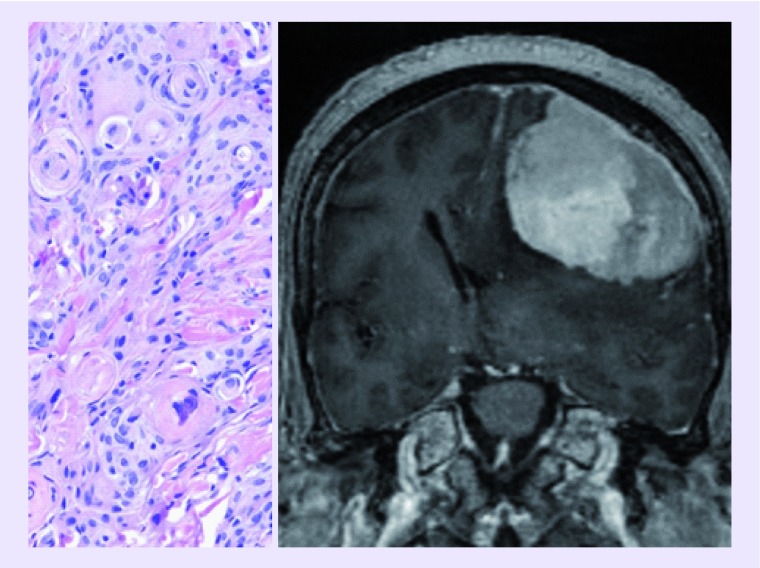
Magnetic resonance imaging (MRI) is the standard modality for the radiologic diagnosis and surveillance of meningioma (Figure 1). In patients who cannot undergo MRI, contrast-enhanced computed tomography (CT) may be used. MR typically reveals a dural-based, homogeneously enhancing and well-circumscribed lesion. Benign meningioma will characteristically have a thickened, contrast-enhancing dural tail and tumors are isointense to gray matter on noncontrast sequences. Meningiomas are extra-axial lesions, and the presence of a CSF cleft adjacent to the tumor can sometimes be seen. On CT, intralesional calcification is common, and bony changes, such as hyperostosis and a ‘beaten brass’ appearance of the remodeled skull, can also be seen in tumors located along the convexity. While patients generally present with a solitary tumor, multiple meningiomas may be seen (‘meningiomatosis’), particularly in syndromic patients (e.g., NF-2), but the finding of multiple extra-axial lesions should raise suspicion for metastases. Of note, the dural tail is not pathognomonic for meningioma and may also be seen in metastases or hemangiopericytomas, but is frequently useful in distinguishing meningioma from other lesions (such as schwannoma) where it is absent [12]. Although less common, peritumoral edema on T2 and T2-FLAIR imaging may also be seen, particularly in secretory meningioma subtype and in more aggressive meningiomas that invade the brain. Central necrosis (hypointense T1, nonenhancing) is not specific for malignant (higher grade) meningiomas as this finding also is seen in benign tumors. Calcification, while better resolved on CT, can be seen on susceptibility weighted MRI sequences. Involvement of cerebral vessels is a common feature, particularly for skull base meningiomas, which may abut or encase the carotid and basilar arteries, or their branches. Cystic features are rarely seen [12]. Vascular imaging, such as an MR venogram may be useful for parafalcine tumors that can involve the superior sagittal sinus either by direct tumor invasion or secondarily result in sinus compression or thrombosis.
Figure 1. . MRI of convexity meningioma.

Coronal T1 postcontrast MRI images demonstrating a large convexity meningioma compressing underlying brain. The tumor arises from the dura is homogenously enhancing and distinct from the underlying brain. (A) Postcontrast images demonstrating subsequent resection of the tumor and (B) the postcontrast enhancement of the dura most likely represents postoperative changes, however, residual tumor cannot be ruled out.
Although these characteristics of meningioma are reliable aides in diagnosis, conventional MR cannot predictably determine pathological grade for meningioma or its growth potential. There is an inverse relationship between decreased apparent diffusion coefficient and higher grade for some tumors, but this is not well validated. Furthermore, conventional MR can be unreliable for discerning early recurrence versus treatment-related radiographic changes such as mild dural thickening. Thus, there is a growing need for applying advanced MR imaging techniques and nuclear medicine studies in meningioma surveillance.
Although not yet standard clinical practice, positron emission tomography (PET) using, for example, a 68-Gallium-labeled somatostatin-receptor analogue (68-Ga-DOTATE) can have a role in monitoring for recurrence in previously irradiated meningioma as well as in aiding diagnosis when surgical biopsy is not feasible [13,14]. Similarly, use of 18-Fluoro-ethyl-tyrosine (18-FET) PET may aid in the visualization of skull base meningioma compared with MRI [15]. The utilization of tryptophan metabolism via α-[(11)C]-methyl-L-tryptophan PET (AMT-PET) may provide insight into tumor grade among meningiomas [16].
Similarly, MR spectroscopy (MRS) studies of meningioma reveal features of increased choline and alanine peaks combined with decreased N-acetyl aspartate and creatinine peaks in comparison with normal brain [17]. Application of MRS to tumor grade is not well established, but an elevated lactate peak characteristic of necrotic tumor tissue can be seen in atypical meningioma [18]. This is also, however, nonspecific in distinguishing meningioma from other necrotic lesions such as bacterial abscesses. Lipid peak elevation on MRS is a marker of micronecrosis seen in atypical and malignant tumors, but is also seen in low-grade microcystic variant tumors [12].
Histopathology
The pathognomonic histologic feature of a meningioma is spherical formations of meningothelial cells, called whorls, which eventually mineralize into psammoma bodies (Figure 2). Central chromatin clearing is also common in tumor nuclei, as are cytoplasmic invaginations into the nuclei, known as intranuclear cytoplasmic pseudoinclusions. However, these features are often inconspicuous or absent in many meningiomas. A range of histologic patterns and findings can be seen that often mimic other soft tissue tumors, as indicated by the numerous variants just among benign grade I tumors: meningothelial, fibrous, transitional, psammomatous, angiomatous, microcystic, secretorym, lymphoplasmacyte-rich and metaplastic. The most widely used immunohistochemical marker to identify a meningioma is epithelial membrane antigen, although more recent studies have clearly shown that somatostatin receptor 2A (SST2A) is a superior immunostain target [19]. Approximately 70–80% of meningiomas are positive for progesterone receptor and, to a much lesser degree, estrogen receptor [20,21], consistent with the epidemiologic preponderance of meningiomas in females, and strongly suggesting a hormonal component to tumor growth.
Figure 2. . Histologic features of WHO grade I–III meningiomas.

(A) Grade I tumors typically contain numerous whorls of meningothelial cells (black arrow), with varying stages of maturation into mineralized psammoma bodies (white arrow). (B) Nuclear clearing (black arrows) and intranuclear cytoplasmic pseudoinclusions (white arrow) are common in grade I tumors, but mitoses and large nucleoli are not. (C) Invasion into the underlying brain (black arrow) is a feature of many grade II meningiomas. (D) Four to 19 mitoses per ten high-power fields (black arrow) and prominent nucleoli (white arrow) are also seen in grade II tumors. (E) Grade III meningiomas usually show increased cellularity and micronecrotic foci (black arrows) and (F) such tumors have 20 or more mitoses per ten high-power fields (black arrows). Scale bar in F = 120 μm in (A) and (C), 300 μm in (E) and 30 μm in (B), (D) and (F).
Since the publication of revised WHO 2016 guidelines (Table 1), meningiomas are classified as grade II ‘atypical’ tumors if they have either 4+ mitoses per ten consecutive high-power fields (using a 40× objective) or brain invasion, defined as meningioma pushing into the underlying cortex without an intervening layer of connective tissue [22]. In other words, a meningioma that is adherent to underlying brain is not necessarily grade II, as there must be unequivocal invasion of the tumor into the gray matter. If neither feature is present, at least three of the following five histologic criteria must be evident to arrive at a grade II diagnosis: intratumoral micronecrosis not caused by presurgical thrombosis therapy; patternless sheets of tumor cells; prominent nucleoli (i.e., readily visible with a 10× objective); high cellularity; and tumor cells with scant cytoplasm relative to nuclear size (small cell changes) [22]. Brain invasion, which has been shown to be an independent adverse marker of tumor recurrence, is now used as a standalone criterion for a grade II diagnosis [22]. A Ki67 proliferation index over 4% has also been correlated with increased recurrence risk [23], but is most commonly used as an adjunct to standard WHO grading, rather than as an independent indicator of grade.
Table 1. . Meningioma grading criteria and frequency.
| WHO grade | Description | Frequency |
|---|---|---|
| Grade I | Low mitotic rate, <4 per 10 HPFs Absence of brain invasion 9 histologic subtypes |
80–85% |
| Grade II atypical | Mitotic rate 4–19 per 10 HPF OR Brain invasion OR ≥3 or 5 specific histologies: • Spontaneous or geographic necrosis, • Patternless sheet-like growth • Prominent nucleoli • High cellularity • Small cells with high n:c ratio |
15–20% |
| Grade III anaplastic (malignant) | Mitotic rate >20 per 10 HPF OR Specific histologies: papillary or rhabdoid |
1–2% |
HPF: High-power field.
Although elevated mitoses and invasion are each regarded as sufficient for a grade II classification, multiple grade II features usually occur within the same atypical tumor, for example, invasion plus increased mitoses, sheet-like growth pattern and areas of high cellularity with small cell changes. Likewise, the other two subtypes of grade II meningiomas, clear cell and chordoid, almost always show additional findings like elevated mitotic activity, micronecrosis and invasion. In fact, the most efficient microscopic evaluation of a meningioma, which usually involves multiple blocks of large tissue fragments, is to scan all the slides at lower power (2× or 4× objective) while looking for foci with micronecrosis, patternless sheets of cells and high cellularity, as those areas are more likely to show elevated mitotic activity. Brain invasion is also most readily identified at lower power by scanning the periphery of the tumor; in cases with equivocal brain tissue involvement, an immunostain for glial fibrillary acidic protein will usually highlight reactive astrocytosis if the tumor is invading the brain.
Grade III anaplastic meningiomas often resemble high-grade sarcomas and will show most or all of the features of grade II atypical tumors, but the only required finding is 20+ mitoses per ten consecutive high-power fields. This means that meningiomas with 4–19 mitoses, a very broad range, all still fall within the grade II spectrum. Rhabdoid and papillary morphologic variants are automatically grade III. Whereas adjuvant radiotherapy is generally withheld in grade I tumors and nearly always given in grade III tumors, a grade II designation offers the clinician much less guidance in the decision to administer or refrain from radiation – a continuing source of controversy, and frustration, among clinicians (discussed below).
Molecular biology
The first genetic alteration observed in meningiomas was deletion of chromosome 22q; subsequent studies discovered that the key gene involved, NF2, is on 22q12, encoding the tumor suppressor merlin [24,25]. But while some sort of merlin inactivation occurs in approximately half of all meningiomas [26,27], its prognostic value is rather weak. Indeed, for many years no molecular markers had been consistently shown to predict recurrence, much less improve upon traditional WHO grading and very little was known about molecular drivers besides NF2. More recent whole genomic analyses have greatly extended our understanding of meningioma biology, suggesting that non-NF2 meningiomas are driven by four mutually exclusive pathways: increased hedgehog signaling (through SMO, SUFU or PRKAR1A mutations); TRAF7 (with either KLF4 mutation or PI3K pathway activation); POLR2A mutations; and other rarer mutations [28,29]. Nearly 10% of non-NF2 meningiomas have mutations in KDM5C, KDM6A or SMARCB1, all of which encode epigenetic modifiers [26]. SMO and AKT1-MTOR mutations are relatively common in non-NF2, genomically stable meningiomas arising in the skull base [26]. In contrast, meningiomas with NF2 inactivation tend to be genomically unstable and localized to the hemispheres [30]. Some of the mutations are more likely to be associated with specific histopathologic variants of meningioma, such as NF2 in fibroblastic/transitional meningiomas [26,31] KLF4 and TRAF7 in secretory meningiomas [32], and AKT1 mutations in grade I meningothelial meningiomas of the skull base and spine [26,34].
Despite these impressive studies, advanced molecular diagnostics have not yet revolutionized the workup and classification of meningiomas, as has been the case for gliomas. With the possible exceptions of TERT promoter mutations and overall copy number instability, which appear to confer a risk of much earlier recurrence [34–36], most correlations are not sufficiently robust for identifying patients that need postsurgical radiation and closer follow-up. It is important to emphasize that none of these molecular markers can replace traditional WHO grading.
Interestingly, and in contrast, methylation profiling of meningiomas has consistently shown a great deal of promise for identifying patients whose tumors are at the greatest risk of recurrence and progression. In discovery and validation cohorts totaling 637 cases, Sahm and colleagues showed that meningiomas can be sorted into two distinct CpG methylation superclusters and further divided into six subclasses [37]. While each WHO grade showed nonrandom subclass associations, histologic grade and methylation class did not always correspond with each other. In such cases, outcome data unequivocally showed that methylation class was a superior predictor of eventual recurrence than histological grade and in particular was able to more accurately assign recurrence risk among grade II meningiomas. Some grade I tumors had a methylation pattern associated with higher grade meningioma and these grade I tumors had higher rates of recurrence than grade I tumors lacking this methylation pattern. Similarly, Olar and colleagues developed a set of 64 CpG loci whose methylation status could predict tumor recurrence, independent of WHO grade [38]. Furthermore, CpG methylation accurately discriminated meningiomas from other radiologic and histologic mimickers like solitary fibrous tumors, sarcomas and Schwannomas. Together, these seminal studies suggest that epigenomic profiling may eventually supplant traditional light microscopy-based diagnosis and grading of dural-based tumors like meningioma. The identification of specific genes that are most differentially methylated and differentially expressed among the meningioma superclusters and subclasses will likely reveal key drivers of aggressive tumor behavior and potentially indicate innovative therapeutic targets.
Surgical treatment
For many patients who present with meningioma, in particular asymptomatic tumors, observation with routine surveillance imaging alone is an acceptable strategy. For tumors that are growing or causing symptomatology, maximal safe surgical resection remains the standard of care for therapeutic management of meningioma. However, the ability to achieve complete resection may be limited by a number of factors, including tumor location; involvement of nearby dural venous sinuses, arteries, cranial nerves, and brain invasion into eloquent tissue; and other patient factors affecting safety of surgery and anesthesia in general. All of these ultimately influence the decision as to whether to offer surgery, as well as the surgical approach and extent of resection planned.
Neuroanatomic location dictates the surgical approach to meningiomas. Convexity meningiomas are relatively simple to approach and resect, but these account for only about one sixth of meningiomas. Parasagittal tumors, while still superficial, are more complex to resect because they often involve or invade the sagittal sinus. Often, in instances where the tumor invades but does not completely occlude the sinus, the portion of the tumor within the sinus is not resected due to high risk of air embolism, high-volume blood loss or acute postoperative sinus thrombosis. Tumors at the base of skull (sphenoid wing, olfactory groove, tuberculum sella, cerebellopontine angle or petroclival region) require more advanced surgical techniques and approaches to safely access the tumor without extensive brain retraction and injury. Recently, with advances in endoscopic technology and techniques, a number of midline anterior skull base tumors are being resected through an endoscopic endonasal approach [39]. Alternatively, radiotherapy should be considered as an upfront treatment approach if subtotal resection or operative morbidity is likely outcomes.
Several principles of surgery on meningiomas are universally applicable. First, if possible, the blood supply to the tumor is addressed by coagulation, as meningiomas can otherwise have relatively high vascularity. Next, firm and often calcified tumors are debulked centrally in order to allow the tumor to be more safely and easily manipulated at its peripheral interface with the brain. Tumor capsules are carefully dissected from the overlying brain, cranial nerve(s) and neurovasculature. Most often an arachnoid plane can be identified over the tumor surface, which may be dissected off the tumor to protect the pia and neurovasculature from injury. Unlike dural venous sinuses, the cranial nerves and arteries may often be enveloped or even encased by a meningioma, but they are rarely invaded by tumor, and identification of the arachnoid plane can allow for safe dissection of tumor from normal structures. The process of debulking centrally and dissecting peripherally is repeated until the full resection is achieved. After reconstruction of the dura with a dural patch substitute, any grossly involved bone is removed when possible, as recurrences may arise from invasion into the bone.
Numerous factors, including venous sinus involvement, arterial or cranial nerve envelopment and extensive involvement of the base of the skull, can preclude gross total resection. This accounts for, at least in part, the improved survival of patients with convexity meningiomas over those with parasagittal and skull base meningiomas [40].
Rates of recurrence for surgically treated meningiomas are impacted heavily by the extent of resection. The traditional measurement of the extent of resection has been the Simpson grade (Table 2), defined both by postoperative imaging and the neurosurgeon's assessment [41]. Simpson grade 5 is biopsy, grade 4 is subtotal resection, grade 3 is macroscopic resection without dural excision or coagulation, grade 2 is gross total resection with dural coagulation, whereas grade 1 is complete resection including dural and adjacent bone resection [41]. While recurrence rates after gross total resection in grade I meningiomas are quite low, they rise substantially with an increase in pathologic grade. Five-year recurrence rates after gross total resection in grade I meningiomas are reported as 7–23%, in grade II they are 50–55% and in grade III 72–78% [2,6]. With subtotal resection, the likelihood of progressive disease substantially increases [6,42]. Specifically, there is increased recurrence-free survival at 5 years in grade I tumors following Simpson grade 4 resection compared with Simpson grade 1–3 resection [43]. The benefit of gross total resection (Simpson grade 1–3) was more pronounced for tumors of the convexity than for parasaggital, parafalcine or skull base tumors and more clear for those tumor with high levels of proliferation (MIB-1 labeling index >3%) [43]. Thus, for completely resected WHO grade I meningiomas, it is reasonable to follow with routine surveillance imaging. For WHO grade I tumors that are incompletely resected (Simpson grade 4 or 5), and for tumors of higher pathological grade (grade II or III), adjuvant treatment is necessary to avert, or at least delay, recurrence.
Table 2. . Extent of resection.
| Simpson resection | Description |
|---|---|
| Grade 1 | Gross total resection of tumor, dural attachment and involved bone (extradural extension) |
| Grade 2 | Gross total resection of tumor, coagulation of dural attachment |
| Grade 3 | Gross total resection of tumor without resection of coagulation of dural and extradural components |
| Grade 4 | Partial (subtotal) resection of tumor |
| Grade 5 | Biopsy only |
Radiation therapy
For decades, radiation therapy (RT) has been the primary treatment for nonsurgically resectable growing tumors. It is also used as an adjuvant therapy (postresection) and in the setting of recurrence for previously resected meningiomas. Both fractionated external beam RT (EBRT) and single-fraction stereotactic radiation (SRS) are employed. Unfortunately, there is a scarcity of strong data from randomized controlled clinical trials for radiotherapy of meningiomas, although several trials are currently ongoing. Much of the data for the role of both RT and surgical resection stems from retrospective or single-institution series. It is also important to emphasize that few high quality studies have not directly compared surgery with RT for resectable tumors, nor have studies directly compared different radiotherapy delivery techniques or doses with each other. Proton therapy in particular has not been extensively studied for meningioma and its role is uncertain. Finally, evaluating treatment modalities based on solely recurrence rates, may miss the complex nature of tumor- and treatment-related disability, symptoms and toxicity.
Generally, WHO grade I tumors are irradiated to a dose of approximately 50 Gy, while WHO grade II–III tumors are treated to approximately 60 Gy with daily fractions over 5–6 weeks using EBRT. While these doses are those employed by most clinical trials of RT in meningioma, optimum dosing, especially for grade II tumors have not been rigorously established. Single-fraction SRS is typically limited to tumors <30 mm diameter and for tumors not directly adjacent to (or compressing) radiation-sensitive structures such as the optic chiasm. Multifraction SRS can be utilized for larger sized tumors. Brachytherapy using radioactive 125-Iodine seeds had been used infrequently for meningioma [44].
The principal acute toxicities of EBRT are location dependent but commonly include focal alopecia and fatigue (CTC AE grade 1–2). SRS has infrequent acute toxicities, although transiently increased focal edema and increased steroid requirements have been noted [45–47], often for parasagittal, parafalcine or posterior fossa tumors. Long-term toxicities of cranial radiotherapy are likewise dependent on the field size and location and may include endocrinopathies, cognitive effects, increased cerebrovascular events and/or secondary malignancy risks. While absolute rates of any of these events in meningioma patients are low, they warrant consideration and discussion at consultation given the normal life expectancy for patients with benign disease.
When considering RT as the primary treatment modality, it must be noted that RT is not as successful as surgery at relief of tumor-related neurological symptoms. However, for patients who are poor surgical candidates, including those whose tumors are surgically inaccessible, RT is often successfully employed for the control of local tumor growth. It is important to note that many meningiomas treated as such with RT do not undergo biopsy, which prevents histological confirmation of grade or molecular features. Thus, extrapolation about outcomes based on this limited information creates bias in favor or surgical outcomes of pathologic WHO grade I meningiomas as compared with outcomes for ‘radiographic’ presumed WHO grade I meningiomas, which likely include some higher-grade lesions.
These factors notwithstanding, outcomes for presumed WHO grade I tumors treated with RT alone exhibit high rates of local control. A recent RANO working group systematic literature review reports overall control rates at the 5- or 10-year interval of 68–100%. For EBRT, meningiomas when treated to 50–54 Gy in 27–30 fractions, and as based on location, control rates of 87–100% have been reported for SRS, when treated to 12–16 Gy, WHO grade I meningiomas had 10-year control rates greater than 90%, but somewhat lower (69–90%) in studies of parasellar and skull base tumors [6]. In one single-institution retrospective observational study comparing SRS (mean dose: 17.7 Gy) with surgical resection for tumors <35 mm diameter, progression-free survival was better with RT compared with Simpson grade 2–5 resection, although not for Simpson grade 1 [48]. All tumors were WHO grade I or presumed to be without histological confirmation. The results of this study also revealed a lower complication rate with SRS (10 vs 22%), although the result was of marginal statistical significance.
Larger tumor size and volume were also associated with decreased local control when treated with single fraction SRS. Radiation-related complication rates from radiation increase from 5 to 23% as treatment volume size increases for SRS of higher grade meningiomas [49]. Generally, patients treated with EBRT have fewer edema-related complications in the short-term, but more potential for longer-term neurocognitive and white matter toxicities. Of course, for brain-invasive or more aggressively behaving tumors, the larger RT field margins around the tumor can be an effective strategy to avert local recurrence. Recently, multiple fraction SRS techniques using up to five fractions (often referred to as hypofractionated SRS) have demonstrated decreased complication rates (particularly from edema and radiation necrosis) in the treatment of larger volume tumors, typically for those tumors >10 mm3 [6]. Moreover, there is sound radiobiological rationale for hypofractionation of SRS, to allow for repair of normal tissues between treatments and thus, mitigate the development of toxicity [50]. In one retrospective single-institution study of hypofractionated SRS for mostly grade I and II meningioma, local control at 1 year was reportedly 95 and 71%, respectively, with no acute toxicities [51]. Another retrospective single-institution study found that 100% progression-free survival and local control for tumors smaller than 9.1 mm3 volume [52]. It remains to be proved whether hypofractionated SRS has a more than niche role in treatment of meningioma or how it compares with traditional EBRT techniques for lesions of similar size and pathological grade.
For adjuvant RT, the goal of treatment is preventing progression to higher-grade malignancy and decreasing recurrence rate. In cases of grade II (atypical) and grade III (anaplastic/malignant) meningiomas, there is a substantially greater risk of recurrence and a clearer role for adjuvant RT even following a gross total resection. For example, even for grade II meningiomas with Simpson grade 1 or grade 1–2 surgical resections, recurrence rates at 5 years have been found to be 50 and 71% respectively [53,54]. Progression-free survival at 5 years for patients with grade III tumors who do not receive RT is worse: 28% following gross total resection and 0% for subtotal resection [55]. In observational series, results from the addition of RT is promising: compared with surgery alone, EBRT (to 59.4 Gy) demonstrated only 20% recurrence rate at 6 years versus 65% without RT [54], but there are conflicting findings from other teams [6]. Importantly, there is no consensus on the dose and timing of adjuvant RT for these more aggressive meningiomas.
The use of adjuvant EBRT has recently been assessed prospectively, in a nonrandomized fashion, in the cooperative group trial NRG/RTOG 0539 (NCT00895622). The trial design divided patients into three risk categories based on tumor grade and resection status. Low-risk patients were defined as having newly diagnosed grade I tumors following either gross total (Simpson grade 1–3) resection or subtotal (Simpson grade 4–5) resection. After surgery, these low-risk patients were followed with observation alone; preliminary data reported a recurrence-free survival of 86% in the low risk group. Recurrence was higher (40%) for subtotal (Simpson 4 or 5) resections compared with gross total resections (Simpson grade 1–3) tumors, whereas the 5-year recurrence rate was only 8.6% [56]. These outcomes would support withholding adjuvant radiation for gross totally resected grade I tumors.
Intermediate risk patients for NRG/RTOG 0539 were defined as any recurrent grade I tumor, or any patient with newly diagnosed gross totally resected grade II tumor. These patients were treated with salvage (for recurrent grade I) or adjuvant (resected grade II) EBRT to a uniform dose of 54 Gy. Of the 52 patients reported, 36 (69%) were grade II, while 16 (31%) were recurrent grade I patients. The 3-year actuarial rate of local failure was 4.1%, with no grade 3 toxicities reported [57]. These results support the use of EBRT for recurrent grade I tumors. For gross totally resected tumors, the adjuvant use of 54 Gy is now being prospectively tested in a randomized fashion (vs observation after gross total resection) for newly diagnosed grade II meningiomas in NRG BN003 (NCT03180268). A similar prospective randomized trial (ROAM/EORTC-1308; ISRCTN71502099) is also underway to directly compare RT with observation in postresection WHO grade II meningiomas [58]. Another prospective trial EORTC 22042-26042 (NCT00626730) comparing 60 Gy in standard fractions EBRT following GTR with 60 Gy + 10 Gy boost to resection cavity has closed, but no results have been reported to date.
High-risk meningioma was defined (per NRG/RTOG 0539) as any recurrent grade II tumor, subtotally resected grade II tumor or any grade III tumor. These patients were treated either with salvage (for recurrent grade II tumors) or adjuvant (for subtotally resected grade II or gross totally resected grade III tumors) with EBRT to a uniform dose of 60 Gy in 30 fractions. Outcomes were recently reported, with 3-year progression-free survival of 59.2%, 3-year local control of 68.9% and 3-year overall survival of 78.6% [59]. This treatment stratum was also designed to evaluate the proton RT (also to a dose of 60 CGE over 30 fractions) for patient in the high-risk group; however no data has been reported. Previous studies examining EBRT in grade III tumors have suggested benefit (progression-free) for patients treated with EBRT at 5 years were only demonstrated in the adjuvant setting (15–80%) but not when RT was used at recurrence [55]. Dose ranges of 50–60 Gy have shown improved outcomes compared with less than 50 Gy in several studies [6]. Nonetheless, these results suggest that further investigations are needed to optimize control of high-risk meningioma.
Progression and recurrence-free survival rates of 58–83% at 5 years have been shown for SRS used either in the recurrent or adjuvant settings for grade II meningioma, with earlier treatment, higher doses and larger treatment volume associated with improved outcomes [6]. For grade III tumors, SRS to 14 Gy (median dose) resulted in a 57% 5-year progression-free survival in a combined adjuvant and recurrent malignant meningioma cohort [60]. However, head-to-head comparisons of SRS and EBRT for atypical and anaplastic meningioma are lacking and the role of SRS in this high-risk group is less clear [44]. There is some concern in particular for inherently brain invasive tumors that the tightly conformal treatment plans used in SRS may decrease tumor control compared with EBRT techniques, resulting in undue recurrence, although for skull base meningiomas the radiation-related toxicity to normal structures may favor SRS. This implication is yet to be proven in a prospectively designed fashion and practice patterns differ.
Current National Comprehensive Cancer Network (NCCN) guidelines for CNS tumors [61] recommend RT in several scenarios of meningioma care with Level 2A evidence. RT should be considered for small (<30 mm) asymptomatic meningioma at presentation, if grade II and subtotally resected or grade III regardless of resection volume, and in grade I tumors when sub-totally resected if there is a ‘potential’ symptom; pursue RT for large (>30 mm) asymptomatic tumors if grade III; and consider RT if WHO grade II or incompletely resected grade I. For all asymptomatic meningiomas, it should be noted that observation alone (with serial imaging) is also recommended. For symptomatic meningiomas at initial presentation, RT is recommended following surgery for any grade III and should be considered for any grade II tumors or large (>30 mm) incompletely resected grade I tumors. For surgically inaccessible tumors or surgically contraindicated patients, RT alone is also recommended. Upon recurrence, surgery (if accessible) followed by RT or re-RT, or RT alone (if inaccessible) is recommended. Of note, NCCN guidelines do not take into consideration patient age, tumor location or any molecular pathologic markers. No recommendation is made for EBRT versus SRS or proton versus photon sources. Recently published European guidelines (from EANO, the European Association of Neuro-Oncology [62]) also recommend RT for subtotally resected grade I tumors, either EBRT or SRS. For subtotally resected grade II meningiomas, EBRT is recommended with level C evidence, and either EBRT or observation in the setting of a gross total resection. Grade III anaplastic meningiomas are recommended to have EBRT regardless of the extent of resection with level B evidence. As with the National Cancer Institute (NCI)-sponsored guidelines, tumor location and molecular markers do not affect the recommended treatment strategy.
It is also important to consider both study outcomes and consensus guidelines published prior to the revised 2016 WHO classification for meningioma in context, as new criteria may result in more tumors being designated grade II that would have been deemed grade I under the older criteria.
Figure 3 of EANO [62] flowchart for treatment guidelines.
Figure 3. . European association of neuro-oncology guidelines for evaluation and treatment of meningioma.

Systemic treatments
Effective medical treatments for meningiomas are lacking. Presently, there is not an established role for chemotherapeutics or other systemic therapies following resection or biopsy for newly diagnosed meningioma. Current NCCN guidelines for meningioma recommend chemotherapy only in the setting of recurrent (progressive) disease when RT or further surgical resection is not feasible [61]. Given the established efficacy and safety of EBRT even in eloquent and radio-sensitive areas of the brain (such as near the optic structures), this determination should be made in consultation with a radiation oncologist, with systemic therapy largely reserved for postradiotherapy progression.
As with clinical studies involving radiation therapy for meningioma, these are a substantial paucity of large, high-quality studies for medical systemic treatments. Generally, they have been observational or retrospective rather than prospective in design and often small, single-institution cohorts. Nonetheless, despite investigations of a wide variety of chemotherapeutics over several decades, the only three classes of medical therapy recommended for meningioma by the NCCN are α-IFN, somatostatin receptor agonists and vascular endothelial growth factor (VEGF) inhibitors [63]. By contrast, EANO guidelines consider systemic pharmacotherapy to be experimental, with level C evidence for grade III or progressive grade II meningioma and do not recommend specific agents or classes of therapeutics [62].
A recent meta-analysis highlights the limitations of these prior medical trials in meningioma, including small study sizes, lack of randomization and heterogeneous inclusion criteria [64]. Many studies are further encumbered by the use of radiographic diagnosis only and a lack of histopathological concordance of WHO grade. Nevertheless, authors have been able to extrapolate 6-month progression-free survival (PFS-6) across the studies of various agents for recurrent grade I and recurrent grade II/III combined meningioma. Kaley and colleagues found a PFS-6 of 29% (95% CI: 20.3–37.7%) for all prospective studies of refractory WHO grade I meningioma treated with either temozolomide, irinotecan, interferon-α, somatostatin analogues pasireotide or sandostatin, and RTK inhibitors imatinib, erlotinib or gefitinib [64]. Data for PFS-6 of higher grade (grade II/III) meningioma patients in the recurrent setting (having failed prior RT and surgery) have demonstrated minimal benefit, at best a PFS-6 of 26% depending on the stringency of inclusion criteria employed [64]. However, even the use of PFS-6 as a response outcome requires consensus on how clinical or radiographic progression or response are defined. As discussed above, disability- or symptom-free survival may also become useful as a patient-centered clinical outcome metric.
Cytotoxic chemotherapeutic agents investigated have had limited efficacy and are not recommended by consensus guidelines. Hydroxyurea, although well tolerated, did not demonstrate durable responses in progressive grade I [65] or grade II/III meningioma [66], with PFS-6 of 10 and 3% respectively in two retrospective series. The alkylating agent temozolomide showed little activity in recurrent grade I meningioma with a PFS-6 of 0% in a small series of 16 patients, with an adverse event profile that include CTC grade III myelosuppression in the 18–38% range [67]. Similar findings were seen with a 16-patient series of recurrent grade I meningiomas using irinotecan, with a PFS-6 of 6% and with myelosuppressive side effects in the 10–20% range [68].
Early studies determined that interferon-α inhibits the growth of meningioma cells in vitro [69], and IFN-α has shown some activity in patients with recurrent grade I [70] and higher grade [71] meningioma, by demonstrating PFS-6 of 54 and 17% in small studies. More promising results have been seen with antiangiogenic agents targeting VEGF. Meningiomas are highly vascular tumors and upregulate expression of VEGF [72]. Sunitinib, a small molecule inhibitor of VEGF signaling (and multiple other pathways), was shown to have an impressive PFS-6 of 42% in a Phase II trial of 36 patients with grade II/III refractory meningioma, although toxicity of the drug was common (60% with severe adverse events) [73]. Tumoral expression of VEGF receptor 2 was predictive of response to sunitinib in this trial. Treatment with another small molecular inhibitor of VEGF signaling, valatinib, resulted in a PFS-6 of 37.5% in a phase study of 22 patients with recurrent high-grade meningioma [74]. The anti-VEGF monoclonal antibody bevacizumab has shown efficacy against recurrent meningioma in a Phase II clinical trial with PFS-6 of 87, 77 and 46% in grade I, II and III tumors, respectively [75]. There is also a role for bevacizumab for control of peritumoral edema or for decreasing the need for corticosteroids in meningiomas in a recent retrospective series [76]. A Phase II prospective trial of bevacizumab is ongoing (NCT01125046).
Other classes of small molecule inhibitors for the receptor tyrosine kinase receptors epidermal growth factor receptor (EGFR) and platelet-derived growth factor receptor (PDGFR), both of which are expressed on meningioma, have been studied. Single-arm Phase II trials of the EGFR inhibitor, erlotinib and gefitinib, demonstrated PFS-6 of 25% for recurrent grade I and 29% for recurrent grade II/III tumors [77]. A Phase II trial of the PDGFR inhibitor imatinib revealed a PFS-6 of 45% for recurrent grade I meningioma, but 0% for higher grade tumors [78].
Hormone receptors have been identified as being broadly expressed on meningiomas, including the receptors for somatostatin (in particular, the SST2A subtype [19]), growth hormone and sex hormones: estrogen, progesterone and androgen [72]. Investigations of inhibitors and analogs for hormone receptors used with therapeutic intent have failed to demonstrate clinical activity in meningioma. In the largest trial involving this class of therapeutic, a Phase III prospective randomized trial of mifepristone (SWOG-S9005) in either primary or recurrent meningioma deemed to be unresectable, there was no difference in failure-free survival or overall survival [79]. A Phase II trial of the somatostatin receptor pasireotide long-acting release (LAR) in recurrent meningioma that failed prior surgical or RT revealed a PFS-6 of 17% in the high grade (grade II/III) cohort and 50% in the low grade, grade I cohort and was well tolerated [80]. There were no radiographic responses; however, in another small Phase II study of nine patients clinical with recurrent high-grade meningioma (WHO grade II/III, intramuscular octreotide failed to demonstrate clinical response or durable stability, but a PFS-6 of 44% was reported [81]. A similar result of PFS-6 of 44% was shown in a pilot study of a long-acting octreotide LAR formulation in recurrent meningioma using SSTR expression as an inclusion criterion and in which radiographic responses were seen [82]. Last, two radioactive isotope-linked analogs of the somatostatin receptor, 90-Y- and 177-Lu-DOTATOC, have been explored in progressive meningioma in a single Phase II trial with several cases of long-term stability reported, but also with multiple adverse events [83].
There are numerous ongoing clinical trials seeking improved medical therapies for meningioma. A recent US FDA approved antineoplastic agent, trabectedin (ET-743), which inhibits transcription and cell cycle progression, was recently investigated in recurrent higher grade (II/III) meningiomas, with no published results to date (EORTC-1320, NCT02234050). The novel therapeutic class of histone deacetylase inhibitors is also being assessed for response in meningioma with clinical trials of panobinostat (in combination with RT, NCT01324635) and AR-42 (NCT02282917).
A series of other trials are investigating immunotherapy agents in meningioma such as the checkpoint inhibitors nivolumab (NCT02648997 and NCT033950), pembrolizumab (NCT03279692 and NCT03016091) or avelumab (in combination with proton radiotherapy, NCT03267836). No results are yet available for these studies. Application of agents targeting the mTOR-pathway, which has been successful in human meningioma cell lines in vitro [84,85], is currently being examined in trials with everolimus (NCT01880749 and NCT01419639) and vistusertib (AZD2014, NCT03071874 and NCT02831257). Everolimus is also being studied in combination with the somatostatin receptor analog octreotide (CAVOREM, NCT02333565) in recurrent meningioma.
Work on the molecular characterization of meningioma (discussed elsewhere in this article) has also resulted in the identification of specific mutations that are potential therapeutic targets or help to stratify patients’ risk of meningioma recurrence. There is also an ongoing clinical trial for meningiomas harboring mutations in the SMO (smoothened) gene and the NF2 gene using the targeted agents vismodegib and GSK2256098, an inhibitor of FAK, respectively (NCT02523014). Similar pathway-directed therapy is being applied to the many NF2-associated tumors (including meningioma) with trials investigating inhibition of the MEK pathway with selumetinib (SEL-TH-1601, NCT03095248) or the CDK-p16-Rb pathway with ribociclib (LEE-011, NCT02933736).
Nonchemotherapeutic modalities for meningioma treatment are also under investigation. For example, a pilot study using NovoTTF-100A (electromagnetic tumor treatment fields, currently FDA-approved for treatment of newly diagnosed and recurrent glioblastoma) in recurrent atypical and anaplastic meningioma reported stable disease in four of six patients without any reported severe adverse events [86]. A clinical trial using the tumor treating fields device for progressive WHO grade II and III meningioma is active, although this device is limited to supratentorial tumors (NCT02847559).
Conclusion & future perspective
These studies for medical treatment of meningioma aim to expand the few available treatments for recurrent or nonsurgical cases of meningioma. Overall, the approach for newer studies is to be prospective in design, to use clearly defined inclusion criteria, selecting patients with histological confirmation or molecularly defined tumors, and to apply validated outcome measurements (such as PFS-6) and comparable response assessment metrics, such as the RANO meningioma guidelines currently being created [87]. In addition, the use to patient-centered outcomes for treatments and clinical trials may be applicable to meningioma both for more aggressive, higher grade tumors and for benign tumors for which symptomatic relief and quality of life rather than growth (or shrinkage) over a 6-month timeframe is valuable. Furthermore, the application of new classes of chemotherapeutics as well as pathway- and molecularly targeted drugs as well as nonstandard approaches such as tumor-treatment fields for meningioma signifies an invigorated interest in these common brain tumors that are often refractory to current treatments.
Recent advances in the mutations and methylation profiles associated with meningiomas may prove to influence our management of these tumors in the next number of years. It is possible that a subset of patients may respond to targeted therapies. It is likely that a substantial shift in the standard of care to incorporate systemic therapies would be feasible in the 5–10 year time frame. This type of change could be quite impactful for both the patient and the clinician as meningiomas comprise the largest percentage of primary intracranial tumors. As the population in many countries ages, the incidence of these tumors will presumably increase, making well-tolerated efficacious therapies of even greater importance.
Executive summary.
Epidemiology
Meningiomas comprise over one-third of primary CNS tumors.
Incidence of meningiomas increases with age.
Clinical presentation
Meningiomas may be diagnosed incidentally.
When symptomatic, symptom presentation is often chronic or subacute.
Natural history & prognosis
Meningiomas will often grow slowly over time.
There is increased risk of disease-specific mortality with increasing grade.
Imaging
MRI often demonstrates a homogenously enhancing extra-axial lesion.
Histology
A recent update to the WHO classification system notes brain invasion qualifies the meningioma as at least a grade II.
Molecular pathology
Specific mutations have been found to have specific neuroanatomic correlation.
Epigenomic profiling via methylation profiles reveals patterns which correlate with the risk of recurrence.
Surgery
Extent of resection influences the risk of recurrence.
Radiation therapy
The role of radiotherapy in intermediate risk meningiomas is actively being studied.
Systemic therapies
Numerous systemic therapies for meningiomas have been investigated with none demonstrating definitive benefit.
Systemic therapies addressing specific molecular targets are undergoing investigation within clinical trials.
Acknowledgements
The authors acknowledge I Gardner of UCSF for copyright assistance.
Footnotes
Financial & competing interests disclosure
This work is supported by P50CA221747 SPORE for Translational Approaches to Brain Cancer (CM Horbinski, CD James, RV Lukas). The authors have no other relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript apart from those disclosed.
No writing assistance was utilized in the production of this manuscript.
References
Papers of special note have been highlighted as: • of interest; •• of considerable interest
- 1.Chamberlain MC. Meningiomas. In: Norden AD, Reardon DA, Wen PCY, editors. Primary Central Nervous System Tumors: Pathogenesis and Therapy. Humana Press; NJ, USA: 2011. pp. 355–375. [Google Scholar]
- 2.Ostrom QT, Gittleman H, Xu J, et al. CBTRUS statistical report: primary brain and other central nervous system tumors diagnosed in the United States in 2009–2013. Neuro-oncology. 2016;18(Suppl. 5):v1–v75. doi: 10.1093/neuonc/now207. [DOI] [PMC free article] [PubMed] [Google Scholar]; •• Epidemiology of primary CNS tumors including meningiomas.
- 3.Central Brain Tumor Registry of the United States (CBTRUS) Primary brain tumors in the United States statistical report 1998–2002. 2005 www.cbtrus.org/reports/2005-2006/2006report.pdf [Google Scholar]
- 4.Hatch EE, Linet MS, Zhang J, et al. Reproductive and hormonal factors and risk of brain tumors in adult females. Int. J. Cancer. 2005;114(5):797–805. doi: 10.1002/ijc.20776. [DOI] [PubMed] [Google Scholar]
- 5.Wiemels J, Wrensch M, Claus EB. Epidemiology and etiology of meningioma. J. Neurooncol. 2010;99(3):307–314. doi: 10.1007/s11060-010-0386-3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Rogers L, Barani I, Chamberlain MC, et al. Meningiomas: knowledge base, treatment outcomes, and uncertainties. a RANO review. J. Neurosurg. 2015;122(1):4–23. doi: 10.3171/2014.7.JNS131644. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Hashiba T, Hashimoto N, Izumoto S, et al. Serial volumetric assessment of the natural history and growth pattern of incidentally discovered meningiomas. J. Neurosurg. 2009;110(4):675–684. doi: 10.3171/2008.8.JNS08481. [DOI] [PubMed] [Google Scholar]
- 8.Soon WC, Fountain DM, Koczyk K, et al. Correlation of volumetric growth and histological grade in 50 meningiomas. Acta Neurochir. 2017;159(11):2169–2177. doi: 10.1007/s00701-017-3277-y. [DOI] [PubMed] [Google Scholar]
- 9.Fountain DM, Soon WC, Matys T, Guilfoyle MR, Kirollos R, Santarius T. Volumetric growth rates of meningioma and its correlation with histological diagnosis and clinical outcome: a systematic review. Acta Neurochir. 2017;159(3):435–445. doi: 10.1007/s00701-016-3071-2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Wen PY, MacDonal DR, Reardon DA, et al. Updated response assessment criteria for high-grade gliomas: response assessment in neuro-oncology working group. J. Clin. Oncol. 2010;28(11):1963–1972. doi: 10.1200/JCO.2009.26.3541. [DOI] [PubMed] [Google Scholar]
- 11.Franz DN, Belousova E, Sparagana S, et al. Everolimus for subependymal giant cell astrocytoma in patients with tuberous sclerosis complex: 2-year open label extension of the randomised EXIST-1 study. Lancet Oncol. 2014;15(13):1513–1520. doi: 10.1016/S1470-2045(14)70489-9. [DOI] [PubMed] [Google Scholar]
- 12.Watts J, Box G, Galvin A, Brotchie P, Trost N, Sutherland T. Magnetic resonance imaging of meningiomas: a pictorial review. Insights Imaging. 2014;5(1):113–122. doi: 10.1007/s13244-013-0302-4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Rachinger W, Stoecklein VM, Terpolilli NA, et al. Increased 68Ga-DOTATATE uptake in PET imaging discriminates meningioma and tumor-free tissue. J. Nuc. Med. 2015;56(3):347–353. doi: 10.2967/jnumed.114.149120. [DOI] [PubMed] [Google Scholar]
- 14.Afshar-Oromieh A, Wolf MB, Kratochwil C, et al. Comparison of 68Ga-DOTATOC-PET/CT and PET/MRI hybrid systems in patients with cranial meningioma: initial results. Neuro-oncology. 2015;17(2):312–319. doi: 10.1093/neuonc/nou131. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Rutten I, Cabay J-E, Withofs N, et al. PET/CT of skull base meningiomas using 2-18F-fluoro-L-tyrosine: initial report. J. Nucl. Med. 2007;48(5):720–725. doi: 10.2967/jnumed.106.038216. [DOI] [PubMed] [Google Scholar]
- 16.Bosnyak E, Kamson DO, Guastella AR, et al. Molecular imaging correlates of tryptophan metabolism via the kynurenine pathway in human meningiomas. Neuro-oncology. 2015;17(9):1284–1292. doi: 10.1093/neuonc/nov098. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Harting I, Hartmann M, Bonsanto MM, Sommer C, Sartor K. Characterization of necrotic meningioma using diffusion MRI, perfusion MRI, and MR spectroscopy: case report and review of the literature. Neuroradiology. 2004;46(3):189–193. doi: 10.1007/s00234-003-1144-4. [DOI] [PubMed] [Google Scholar]
- 18.Buhl R, Nabavi A, Wolff S, et al. MR spectroscopy in patients with intracranial meningiomas. Neurol. Res. 2007;29(1):43–46. doi: 10.1179/174313206X153824. [DOI] [PubMed] [Google Scholar]
- 19.Menke JR, Raleigh DR, Gown AM, Thomas S, Perry A, Tihan T. Somatostatin receptor 2a is a more sensitive diagnostic marker of meningioma than epithelial membrane antigen. Acta Neuropathologica. 2015;130(3):441–443. doi: 10.1007/s00401-015-1459-3. [DOI] [PubMed] [Google Scholar]
- 20.Hsu DW, Efird JT, Hedley-Whyte ET. Progesterone and estrogen receptors in meningiomas: prognostic considerations. J. Neurosurg. 1997;86(1):113–120. doi: 10.3171/jns.1997.86.1.0113. [DOI] [PubMed] [Google Scholar]
- 21.Pravdenkova S, Al-Mefty O, Sawyer J, Husain M. Progesterone and estrogen receptors: opposing prognostic indicators in meningiomas. J. Neurosurg. 2006;105(2):163–173. doi: 10.3171/jns.2006.105.2.163. [DOI] [PubMed] [Google Scholar]
- 22.Louis DN, Perry A, Reifenberger G, et al. The 2016 World Health Organization classification of tumors of the central nervous system: a summary. Acta Neuropathologica. 2016;131(6):803–820. doi: 10.1007/s00401-016-1545-1. [DOI] [PubMed] [Google Scholar]; •• Definitive summary of the WHO 2016 CNS tumor classification system.
- 23.Vranic A, Popovic M, Cör A, Prestor B, Pizem J. Mitotic count, brain invasion, and location are independent predictors of recurrence-free survival in primary atypical and malignant meningiomas: a study of 86 patients. Neurosurgery. 2010;67(4):1124–1132. doi: 10.1227/NEU.0b013e3181eb95b7. [DOI] [PubMed] [Google Scholar]
- 24.Rouleau GA, Merel P, Lutchman M, et al. Alteration in a new gene encoding a putative membrane-organizing protein causes neuro-fibromatosis type 2. Nature. 1993;363(6429):515–521. doi: 10.1038/363515a0. [DOI] [PubMed] [Google Scholar]
- 25.Trofatter JA, MacCollin MM, Rutter JL, et al. A novel moesin-, ezrin-, radixin-like gene is a candidate for the neurofibromatosis 2 tumor suppressor. Cell. 1993;72(5):791–800. doi: 10.1016/0092-8674(93)90406-g. [DOI] [PubMed] [Google Scholar]
- 26.Brastianos PK, Horowitz PM, Santagata S, et al. Genomic sequencing of meningiomas identifies oncogenic SMO and AKT1 mutations. Nat. Genet. 2013;45(3):285–289. doi: 10.1038/ng.2526. [DOI] [PMC free article] [PubMed] [Google Scholar]; •• A key study describing potentially actionable mutations within subsets of meningiomas.
- 27.Choy W, Kim W, Nagasawa D, et al. The molecular genetics and tumor pathogenesis of meningiomas and the future directions of meningioma treatments. Neurosurg. Focus. 2011;30(5):E6. doi: 10.3171/2011.2.FOCUS1116. [DOI] [PubMed] [Google Scholar]
- 28.Abedalthagafi M, Bi WL, Aizer AA, et al. Oncogenic PI3K mutations are as common as AKT1 and SMO mutations in meningioma. Neuro-oncology. 2016;18(5):649–655. doi: 10.1093/neuonc/nov316. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Clark VE, Harmancı AS, Bai H, et al. Recurrent somatic mutations in POLR2A define a distinct subset of meningiomas. Nat. Genet. 2016;48(10):1253–1259. doi: 10.1038/ng.3651. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Clark VE, Erson-Omay EZ, Serin A, et al. Genomic analysis of non-NF2 meningiomas reveals mutations in TRAF7, KLF4, AKT1, and SMO. Science. 2013;339(6123):1077–1080. doi: 10.1126/science.1233009. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Wellenreuther R, Kraus JA, Lenartz D, et al. Analysis of the neurofibromatosis 2 gene reveals molecular variants of meningioma. Am. J. Pathol. 1995;146(4):827–832. [PMC free article] [PubMed] [Google Scholar]
- 32.Reuss DE, Piro RM, Jones DTW, et al. Secretory meningiomas are defined by combined KLF4 K409Q and TRAF7 mutations. Acta Neuropathol. 2013;125(3):351–358. doi: 10.1007/s00401-013-1093-x. [DOI] [PubMed] [Google Scholar]
- 33.Sahm F, Bissel J, Koelsche C, et al. AKT1E17K mutations cluster with meningothelial and transitional meningiomas and can be detected by SFRP1 immunohistochemistry. Acta Neuropathol. 2013;126(5):757–762. doi: 10.1007/s00401-013-1187-5. [DOI] [PubMed] [Google Scholar]
- 34.Aizer AA, Abedalthagafi M, Bi WL, et al. A prognostic cytogenetic scoring system to guide the adjuvant management of patients with atypical meningioma. Neuro-oncology. 2016;18(2):269–274. doi: 10.1093/neuonc/nov177. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.Goutagny S, Nault JC, Mallet M, Henin D, Rossi JZ, Kalamarides M. High incidence of activating TERT promoter mutations in meningiomas undergoing malignant progression. Brain Pathol. 2014;24(2):184–189. doi: 10.1111/bpa.12110. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36.Sahm F, Schrimpf D, Olar A, et al. TERT promoter mutations and risk of recurrence in meningioma. J. Natl Cancer Inst. 2016;108(5):djv377. doi: 10.1093/jnci/djv377. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37.Sahm F, Schrimpf D, Stichel D, et al. DNA methylation-based classification and grading system for meningioma: a multicentre, retrospective analysis. Lancet Oncol. 2017;18(5):682–694. doi: 10.1016/S1470-2045(17)30155-9. [DOI] [PubMed] [Google Scholar]; • A study utilizing methylation status to classify meningiomas.
- 38.Olar A, Wani KM, Wilson CD, et al. Global epigenetic profiling identifies methylation subgroups associated with recurrence-free survival in meningioma. Acta Neuropathol. 2017;133(3):431–444. doi: 10.1007/s00401-017-1678-x. [DOI] [PMC free article] [PubMed] [Google Scholar]; • Another key study using methylation status to define subtypes of meningiomas and their associated natural history.
- 39.Zada G, Başkaya MK, Shah MV. Introduction: surgical management of skull base meningiomas. Neurosurg. Focus. 2017;43(Video Suppl. 2) doi: 10.3171/2017.10.FocusVid.Intro. Intro. [DOI] [PubMed] [Google Scholar]
- 40.Mirimanoff RO, Dosoretz DE, Linggood RM, Ojemann RG, Martuza RL. Meningioma: analysis of recurrence and progression following neurosurgical resection. J. Neurosurg. 1985;62(1):18–24. doi: 10.3171/jns.1985.62.1.0018. [DOI] [PubMed] [Google Scholar]
- 41.Simpson D. The recurrence of intracranial meningiomas after surgical treatment. J. Neurol. Neurosurg. Psych. 1957;20(1):22–39. doi: 10.1136/jnnp.20.1.22. [DOI] [PMC free article] [PubMed] [Google Scholar]; • Classic manuscript defining the extent of resection in meningiomas.
- 42.Sun SQ, Hawasli AH, Huang J, Chicoine MR, Kim AH. An evidence-based treatment algorithm for the management of WHO grade II and III meningiomas. Neurosurg. Focus. 2015;38(3):E3. doi: 10.3171/2015.1.FOCUS14757. [DOI] [PubMed] [Google Scholar]
- 43.Oya S, Kawai K, Nakatomi H, Saito N. Significance of Simpson grading system in modern meningioma surgery: integration of the grade with MIB-1 labeling index as a key to predict the recurrence of WHO grade I meningiomas. J. Neurosurg. 2012;117(1):121–128. doi: 10.3171/2012.3.JNS111945. [DOI] [PubMed] [Google Scholar]
- 44.Walcott BP, Nahed BV, Brastianos PK, Loeffler JS. Radiation treatment for WHO grade II and III meningiomas. Front. Oncol. 2013;3:227. doi: 10.3389/fonc.2013.00227. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 45.Nicolato A, Foroni R, Pellegrino M, et al. Gamma knife radiosurgery in meningiomas of the posterior fossa. Experience with 62 treated lesions. Minim. Invasive Neurosurg. 2001;44(4):211–217. doi: 10.1055/s-2001-19934. [DOI] [PubMed] [Google Scholar]
- 46.Sheehan JP, Cohen-Inbar O, Ruangkanchanasetr R, et al. Post-radiosurgical edema associated with parasagittal and parafalcine meningiomas: a multicenter study. J. Neurooncol. 2015;125(2):317–324. doi: 10.1007/s11060-015-1911-1. [DOI] [PubMed] [Google Scholar]
- 47.Sheehan JP, Starke RM, Kano H, et al. Gamma Knife radiosurgery for posterior fossa meningiomas: a multicenter study. J. Neurosurg. 2015;122(6):1479–1489. doi: 10.3171/2014.10.JNS14139. [DOI] [PubMed] [Google Scholar]
- 48.Pollock BE, Stafford SL, Utter A, Giannini C, Schreiner SA. Stereotactic radiosurgery provides equivalent tumor control to Simpson grade 1 resection for patients with small- to medium-size meningiomas. Int. J. Radiat. Oncol. Biol. Phys. 2003;55(4):1000–1005. doi: 10.1016/s0360-3016(02)04356-0. [DOI] [PubMed] [Google Scholar]
- 49.Pollock BE, Stafford SL, Link MJ, Garces YI, Foote RL. Stereotactic radiosurgery of World Health Organization grade II and III intracranial meningiomas: treatment results on the basis of a 22-year experience. Cancer. 2012;118(4):1048–1054. doi: 10.1002/cncr.26362. [DOI] [PubMed] [Google Scholar]
- 50.Kirkpatrick JP, Soltys SG, Lo SS, Beal K, Shrieve DC, Brown PD. The radiosurgery fractionation quandary: single fraction or hypofractionation? Neuro-oncology. 2017;19(Suppl. 2):ii38–ii49. doi: 10.1093/neuonc/now301. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 51.Bria C, Wegner RE, Clump DA, et al. Fractionated stereotactic radiosurgery for the treatment of meningiomas. J. Cancer Res. Ther. 2011;7(1):52–57. doi: 10.4103/0973-1482.80462. [DOI] [PubMed] [Google Scholar]
- 52.Onodera S, Aoyama H, Katoh N, et al. Long-term outcomes of fractionated stereotactic radiotherapy for intracranial skull base benign meningiomas in single institution. Jpn J. Clin. Oncol. 2011;41(4):462–468. doi: 10.1093/jjco/hyq231. [DOI] [PubMed] [Google Scholar]
- 53.Aghi MK, Carter BS, Cosgrove GR, et al. Long-term recurrence rates of atypical meningiomas after gross total resection with or without postoperative adjuvant radiation. Neurosurgery. 2009;64(1):56–60. doi: 10.1227/01.NEU.0000330399.55586.63. [DOI] [PubMed] [Google Scholar]
- 54.Komotar RJ, Iorgulescu JB, Raper DMS, et al. The role of radiotherapy following gross-total resection of atypical meningiomas. J. Neurosurg. 2012;117(4):679–686. doi: 10.3171/2012.7.JNS112113. [DOI] [PubMed] [Google Scholar]
- 55.Dziuk TW, Woo S, Butler EB, et al. Malignant meningioma: an indication for initial aggressive surgery and adjuvant radiotherapy. J. Neurooncol. 1998;37(2):177–188. doi: 10.1023/a:1005853720926. [DOI] [PubMed] [Google Scholar]
- 56.Rogers L, Zhang P, Vogelbaum MA, et al. Low-risk meningioma: initial outcomes from NRG oncology/RTOG 0539. Int. J. Radiat. Oncol. Biol. Phys. 2016;96(5):939–440. [Google Scholar]
- 57.Rogers L, Zhang P, Vogelbaum MA, et al. Intermediate-risk meningioma: initial outcomes from NRG Oncology RTOG 0539. J. Neurosurg. 2017;5:1–13. doi: 10.3171/2016.11.JNS161170. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 58.Jenkinson MD, Weber DC, Haylock BJ, Mallucci CL, Zakaria R, Javadpour M. Radiotherapy versus observation following surgical resection of atypical meningioma (the ROAM trial) Neuro-oncology. 2014;16(11):1560–1561. doi: 10.1093/neuonc/nou149. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 59.Rogers L, Zhang P, Vogelbaum M, et al. MNGI-08. High-risk meningioma: initial outcomes from NRG ONCOLOGY/RTOG-0539. Neuro-oncology. 2017;19(Suppl. 6):vi133. doi: 10.3171/2018.8.JNS161170a. [DOI] [PubMed] [Google Scholar]
- 60.El-Khatib M, Majdoub El F, Hoevels M, et al. Stereotactic LINAC radiosurgery for incompletely resected or recurrent atypical and anaplastic meningiomas. Acta Neurochirurgica. 2011;153(9):1761–1767. doi: 10.1007/s00701-011-1073-7. [DOI] [PubMed] [Google Scholar]
- 61.NCCN Guidelines: central nervous system cancers. http://nccn.org/
- 62.Goldbrunner R, Minniti G, Preusser M, et al. EANO guidelines for the diagnosis and treatment of meningiomas. Lancet Oncol. 2016;17(9):e383–e391. doi: 10.1016/S1470-2045(16)30321-7. [DOI] [PubMed] [Google Scholar]; •• Contemporary guidelines for the clinical management of meningiomas.
- 63.Karsy M, Guan J, Cohen A, Colman H, Jensen RL. Medical management of meningiomas: current status, failed treatments, and promising horizons. Neurosurg. Clin. N. Am. 2016;27(2):249–260. doi: 10.1016/j.nec.2015.11.002. [DOI] [PubMed] [Google Scholar]
- 64.Kaley T, Barani I, Chamberlain MC, et al. Historical benchmarks for medical therapy trials in surgery- and radiation-refractory meningioma: a RANO review. Neuro-oncology. 2014;16(6):829–840. doi: 10.1093/neuonc/not330. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 65.Chamberlain MC, Johnston SK. Hydroxyurea for recurrent surgery and radiation refractory meningioma: a retrospective case series. J. Neurooncol. 2011;104(3):765–771. doi: 10.1007/s11060-011-0541-5. [DOI] [PubMed] [Google Scholar]
- 66.Chamberlain MC. Hydroxyurea for recurrent surgery and radiation refractory high-grade meningioma. J. Neurooncol. 2012;107(2):315–321. doi: 10.1007/s11060-011-0741-z. [DOI] [PubMed] [Google Scholar]
- 67.Chamberlain MC, Tsao-Wei DD, Groshen S. Temozolomide for treatment-resistant recurrent meningioma. Neurology. 2004;62(7):1210–1212. doi: 10.1212/01.wnl.0000118300.82017.f4. [DOI] [PubMed] [Google Scholar]
- 68.Chamberlain MC, Tsao-Wei DD, Groshen S. Salvage chemotherapy with CPT-11 for recurrent meningioma. J. Neurooncol. 2006;78(3):271–276. doi: 10.1007/s11060-005-9093-x. [DOI] [PubMed] [Google Scholar]
- 69.Koper JW, Zwarthoff EC, Hagemeijer A, et al. Inhibition of the growth of cultured human meningioma cells by recombinant interferon-alpha. Eur. J. Cancer. 1991;27(4):416–419. doi: 10.1016/0277-5379(91)90375-n. [DOI] [PubMed] [Google Scholar]
- 70.Chamberlain MC, Glantz MJ. Interferon-alpha for recurrent World Health Organization grade 1 intracranial meningiomas. Cancer. 2008;113(8):2146–2151. doi: 10.1002/cncr.23803. [DOI] [PubMed] [Google Scholar]
- 71.Chamberlain MC. IFN-α for recurrent surgery- and radiation-refractory high-grade meningioma: a retrospective case series. CNS Oncol. 2013;2(3):227–235. doi: 10.2217/cns.13.17. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 72.Le Rhun E, Taillibert S, Chamberlain MC. Systemic therapy for recurrent meningioma. Expert Rev. Neurotherapeutics. 2016;16(8):889–901. doi: 10.1080/14737175.2016.1184087. [DOI] [PubMed] [Google Scholar]
- 73.Kaley TJ, Wen P, Schiff D, et al. Phase II trial of sunitinib for recurrent and progressive atypical and anaplastic meningioma. Neuro-oncology. 2015;17(1):116–121. doi: 10.1093/neuonc/nou148. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 74.Raizer JJ, Grimm SA, Rademaker A, et al. A Phase II trial of PTK787/ZK 222584 in recurrent or progressive radiation and surgery refractory meningiomas. J. Neurooncol. 2014;117(1):93–101. doi: 10.1007/s11060-014-1358-9. [DOI] [PubMed] [Google Scholar]
- 75.Grimm S, Kumthekar P, Chamberlain MC, et al. MNGO-04 Phase II trial of bevacizumab in patients with surgery and radiation refractory progressive meningioma. Neuro-oncology. 2015;17(Suppl. 5):v130. [Google Scholar]
- 76.Furtner J, Schöpf V, Seystahl K, et al. Kinetics of tumor size and peritumoral brain edema before, during, and after systemic therapy in recurrent WHO grade II or III meningioma. Neuro-oncology. 2016;18(3):401–407. doi: 10.1093/neuonc/nov183. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 77.Norden AD, Raizer JJ, Abrey LE, et al. Phase II trials of erlotinib or gefitinib in patients with recurrent meningioma. J. Neurooncol. 2009;96(2):211–217. doi: 10.1007/s11060-009-9948-7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 78.Wen PY, Yung WKA, Lamborn KR, et al. Phase II study of imatinib mesylate for recurrent meningiomas (North American Brain Tumor Consortium study 01-08) Neuro-oncology. 2009;11(6):853–860. doi: 10.1215/15228517-2009-010. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 79.Ji Y, Rankin C, Grunberg S, et al. Double-blind Phase III randomized trial of the antiprogestin agent mifepristone in the treatment of unresectable meningioma: SWOG S9005. J. Clin. Oncol. 2015;33(34):4093–4098. doi: 10.1200/JCO.2015.61.6490. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 80.Norden AD, Ligon KL, Hammond SN, et al. Phase II study of monthly pasireotide LAR (SOM230C) for recurrent or progressive meningioma. Neurology. 2015;84(3):280–286. doi: 10.1212/WNL.0000000000001153. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 81.Simó M, Argyriou AA, Macià M, et al. Recurrent high-grade meningioma: a Phase II trial with somatostatin analogue therapy. Cancer Chemother. Pharmacol. 2014;73(5):919–923. doi: 10.1007/s00280-014-2422-z. [DOI] [PubMed] [Google Scholar]
- 82.Chamberlain MC, Glantz MJ, Fadul CE. Recurrent meningioma: salvage therapy with long-acting somatostatin analogue. Neurology. 2007;69(10):969–973. doi: 10.1212/01.wnl.0000271382.62776.b7. [DOI] [PubMed] [Google Scholar]
- 83.Marincek N, Radojewski P, Dumont RA, et al. Somatostatin receptor-targeted radiopeptide therapy with 90Y-DOTATOC and 177Lu-DOTATOC in progressive meningioma: long-term results of a Phase II clinical trial. J. Nuc. Med. 2015;56(2):171–176. doi: 10.2967/jnumed.114.147256. [DOI] [PubMed] [Google Scholar]
- 84.Graillon T, Romano D, Defilles C, et al. Pasireotide is more effective than octreotide, alone or combined with everolimus on human meningioma in vitro . Oncotarget. 2017;8(33):55361–55373. doi: 10.18632/oncotarget.19517. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 85.Graillon T, Defilles C, Mohamed A, et al. Combined treatment by octreotide and everolimus: octreotide enhances inhibitory effect of everolimus in aggressive meningiomas. J. Neurooncol. 2015;124(1):33–43. doi: 10.1007/s11060-015-1812-3. [DOI] [PubMed] [Google Scholar]
- 86.Wu S, Gavrilovec I, La Fuente De MI, Kreisl T, Kaley T. ACTR-43. Pilot study of optune (NOVOTTF-100A) for recurrent atypical and anaplastic meningioma. Neuro-oncology. 2016;18(Suppl. 6):vi11–vi11. [Google Scholar]
- 87.Eisele SC, Wen PY, Lee EQ. Assessment of brain tumor response: RANO and its offspring. Curr. Treat. Options Oncol. 2016;17(7):35. doi: 10.1007/s11864-016-0413-5. [DOI] [PubMed] [Google Scholar]; • An overview of radiographic assessment of brain tumors including meningiomas.