

Abstract
Background
The pain experience for total shoulder arthroplasty (TSA) patients in the first 2 weeks after surgery has not been well described. Many approaches to pain management have been used, with none emerging as clearly superior; it is important that any approach minimizes postoperative opioid use.
Questions/purposes
(1) With a long-acting nerve block and comprehensive multimodal analgesia, what are the pain levels after TSA from day of surgery until postoperative day (POD) 14? (2) How many opioids do TSA patients take from the day of surgery until POD 14? (3) What are the PainOUT responses at POD 1 and POD 14, focusing on side effects from opioids usage?
Methods
From January 27, 2017 to December 6, 2017, 154 TSA patients were identified as potentially eligible for this prospective, institutional review board-approved observational study. Of those, 46 patients (30%) were excluded (either because they were deemed not appropriate for the study, research staff were not available, patients were not eligible, or they declined to participate), and another six (4%) had incomplete followup data and could not be studied, leaving 102 patients (66%) for analysis here. Median preoperative pain with movement was 7 (interquartile range [IQR], 5–9) and 13 of 102 patients used preoperative opioids. All patients received a single-injection bupivacaine interscalene block with adjuvant clonidine, dexamethasone, and buprenorphine. Multimodal analgesia included acetaminophen, NSAIDs, and opioids. The primary outcome was the Numerical Rating Scale (NRS) pain score with movement on POD 14. The NRS pain score ranges from 0 (no pain) to 10 (worst pain possible). Secondary outcomes included NRS pain scores at rest and with movement (day of surgery, and PODs 1, 3, 7 and 14), daily analgesic use from day of surgery to POD 14 (both oral and intravenous), Opioid-Related Symptom Distress Scale (which assesses 12 symptoms ranging from 0 to 4, with 4 being the most distressing; the composite score is the mean of the 12 symptom-specific scores) on POD 1, and the PainOut questionnaire on POD 1 and POD 14. The PainOut questionnaire includes questions rating nausea, drowsiness, itching from 0 (none) to 10 (severe), as well as rating difficulty staying asleep from 0 (does not interfere) to 10 (completely interferes).
Results
The median NRS pain scores with movement were 2 (IQR, 0–5) on POD 1, 5 (IQR, 3–6) on POD 3, and the pain score was 3 (IQR, 1–5) on POD 14. Median total opioid use (converted to oral morphine equivalents) was 16 mg (4–50 mg) for the first 24 hours, 30 mg (8–63 mg) for the third, and 0 mg (0–20 mg) by the eighth 24-hour period, while the most frequent number of activations of the intravenous patient-controlled analgesia device was 0. Median PainOut scores on POD 1 and POD 14 for sleep interference, nausea, drowsiness and itching were 0, and the median composite Opioid-Related Symptom Distress Scale score on day 1 was 0.3 (IQR, 0.1–0.5).
Conclusions
Clinicians using this protocol, which combines a long-acting, single-injection nerve block with multimodal analgesia, can inform TSA patients that their postoperative pain will likely be less than their preoperative pain, and that on average they will stop using opioids after 7 days. Future research could investigate what the individual components of this protocol contribute. Larger cohort studies or registries would document the incidence of rare complications. Randomized controlled trials could directly compare analgesic effectiveness and cost-benefits for this protocol versus alternative strategies, such as perineural catheters or liposomal bupivacaine. Perhaps most importantly, future studies could seek ways to further reduce peak pain and opioid usage on POD 2 and POD 3.
Level of Evidence
Level IV, therapeutic study.
Introduction
Total shoulder arthroplasty (TSA) patients often have severe postoperative pain, and the most effective analgesic therapy is unclear. Median pain scores on postoperative day (POD) 1 with conventional therapy can be as high as 6 at rest and 8.5 with movement when measured on a 0 to 10-point Numerical Rating Scale (NRS) [7]. There are a number of ways to use regional anesthetic techniques to address pain after TSA: long-acting nerve blockade, perineural catheters, and liposomal bupivacaine. Recently, the addition of multimodal oral analgesia to a single-injection nerve block was shown to provide good pain control after TSA, with median NRS pain scores on POD 1 of 2.3 at rest and 3.8 with movement [5]. Combining adjuvant analgesic compounds such as clonidine, dexamethasone, buprenorphine with local anesthetic for a single-injection interscalene block may prolong the duration of analgesia [25].
Many approaches to pain management after shoulder surgery have been used, with none emerging as clearly superior; it is important that any approach seek to minimize opioid use. Strategies that have been proposed to address pain after shoulder surgery include peripheral nerve blockade [6], peripheral nerve blockade with adjuvants [25], and multimodal analgesia with nerve blockade [11]. Liposomal bupivacaine infiltration may either improve [14] or worsen pain management after TSA [12]. Liposomal bupivacaine can be used as a component of the nerve blockade, but when comparing postoperative pain with baseline pain, patients receiving liposomal bupivacaine did not differ from patients receiving plain bupivacaine [18]. The current study uses a long-acting nerve blockade and multimodal analgesia, with a focus on subacute pain. Subacute pain can be defined as pain occurring after discharge from hospital until 3 months after surgery [19]. Subacute pain has been less well addressed than acute pain but is critically important to patients since they are largely managing their pain at home, which could make subacute pain potentially more complicated to handle [19]. This study chose subacute pain at the 14-day time point as a clinically relevant and psychologically important primary outcome [24]. POD 90 data is additionally presented because it corresponds to the end of the subacute phase of pain [19] and marks the onset of chronic pain [9]. It is helpful for physicians to have detailed information about postoperative pain, opioid use, and opioid side effects, so that they can appropriately advise their patients.
Therefore, we asked: (1) With a long-acting nerve block and comprehensive multimodal analgesia, what are the pain levels after TSA from the day of surgery to POD 14? (2) How many opioids do TSA patients take from the day of surgery to POD 14? (3) What are the PainOUT responses at POD 1 and POD 14, focusing on side effects from opioids usage?
Patients and Methods
After institutional review board approval (IRB#2017-0779), adult patients who were American Society of Anesthesiologists physical status 1, 2, or 3 were recruited from a single center into this prospective, observational cohort study. All patients provided written informed consent. Eligible patients were aged 18 to 80 years and were scheduled for an elective TSA or reverse TSA for degenerative conditions with participating surgeons and anesthesiologists. We identified 154 patients who were eligible for participation during a period from January 27, 2017 to December 6, 2017. We excluded 46 patients for the following reasons: revision procedures (n = 6), surgery for trauma or rheumatoid arthritis (n = 2), conversion to hemiarthroplasty (n = 3), declined to participate (n = 9), not deemed appropriate by a physician (n = 14) or research assistant not available (n = 12) (Fig. 1). Patients with preoperative opioid use or chronic pain diagnoses were included to improve generalizability. Patients receiving preoperative opioids for painful musculoskeletal conditions were not excluded. Four patients had a contraindication to NSAID use. They were included in the study but were not administered NSAIDs. This was designed as a prospective pragmatic trial [15], with the goal of describing pain, opioid use, and opioid side effects after using this protocol in a real-world context. For this reason, patient exclusions were limited, and the pain management protocol, although detailed, allowed changes to be made based on patient characteristics and preferences. This study design was selected to increase generalizability of the results. Patients were recruited for the study in the holding area on the day of surgery. If the anesthesiologist or the surgeon believed that the patient would be best served by a different protocol, or that the patient was apparently not psychologically able to tolerate a research informed consent discussion, then they were not approached and were characterized as “not deemed appropriate by a physician.” The surgeries were performed by two attending surgeons (DMD, LVG). There were five participating anesthesiologists; two completed fellowships in regional anesthesia (EAG, YL) and three have at least 20 years of experience in regional anesthesia (JTY, SSL, MAG). After enrolling 108 patients, six were lost to followup, allowing analysis of 102 patients. Patients with preoperative opioid use or chronic pain diagnoses were included to improve generalizability. Median preoperative pain with movement was 7 (IQR 5–9) and 13 of 102 patients used preoperative opioids (Table 1). The trial was registered on January 13, 2017, before enrollment of the first subject (clinical trials.gov, NCT 03021096).
Fig. 1.
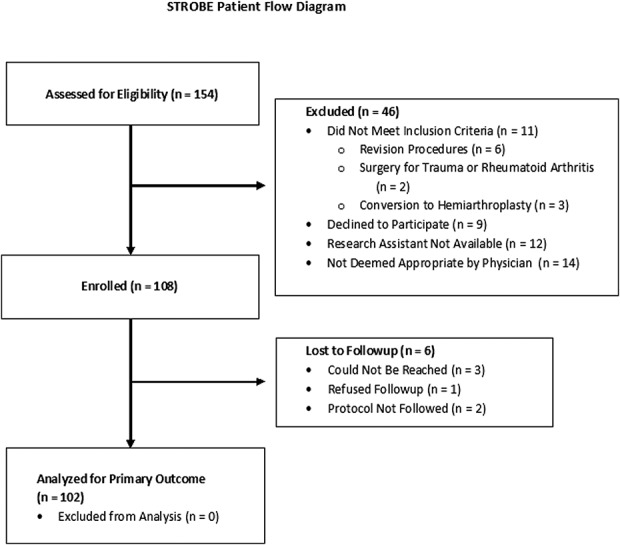
The patient flow diagram is reported according to the STROBE statement (Strengthening the Reporting of Observational Studies in Epidemiology).
Table 1.
Patient and surgery characteristics

Baseline Pain, Catastrophizing, and Anxiety Scores
On the day of surgery, we determined gender and past pain medication use (Table 1). The patients’ NRS pain scores were recorded at rest and with movement. NRS pain scores of 0 indicated no pain, 1 to 3 was mild pain, 4 to 6 was moderate pain, and 7 to 10 signaled severe pain [2].
Questionnaires also were administered for pain catastrophizing, anxiety/depression, and fibromyalgia trait. The Pain Catastrophizing Scale assesses how patients catastrophize their pain via rumination, magnification, and feelings of helplessness [16]. It ranges from 0 to 52, with high scores indicating more catastrophizing; a score of 30 or more represents a clinically relevant level of catastrophizing [16]. The Hospital Anxiety and Depression Scale has two subscales; each subscale ranges from 0 to 21, with higher scores indicating more anxiety or depression; a score of 0 to 7 in either subscale is normal [1]. We assessed the fibromyalgia trait using the Michigan Body Map, a schematic detailing the presence of pain in the body, combined with the Fibromyalgia Symptom Severity Index. This scale ranges from 0 to 31 with higher scores indicating greater likelihood of fibromyalgia. A diagnosis of fibromyalgia can be made with a score ≥ 13 [23]. Among patients undergoing lower extremity joint replacement, upper tertile scores of 9 to 31 were associated with a substantial increase in postoperative opioid use [3].
Description of Surgery
All operations were performed with the patient in the modified beach chair position (45-50o upright) and used a deltopectoral approach. All patients undergoing reverse TSA had a subscapularis peel, whereas patients undergoing anatomic TSA had either a tenotomy or lesser tuberosity osteotomy, depending on the surgeon’s preference. The humeral head was cut in 30° of retroversion in all patients, and the humeral canal was prepared by reaming and broaching. The long head of the biceps tendon was anchored to the surrounding soft tissue.
All patients undergoing anatomic TSA received a Comprehensive Total Shoulder Replacement (Biomet, Warsaw, IN, USA) with a hybrid glenoid component consisting of polyethylene pegs that were cemented into the glenoid vault, and a central porous ingrowth titanium post that was press fit into the vault. For patients under undergoing reverse TSA, a combination of the Comprehensive Reverse Shoulder Replacement system (Biomet, Warsaw, IN, USA) and the Surgical Reverse Shoulder Replacement system (DJO Global, Austin, TX, USA) were used. In both systems, a baseplate was affixed to the glenoid bone with a central compression screw and four peripheral locking screws. A glenosphere of appropriate size for the patient’s anatomy was then placed onto the baseplate.
The humeral component was pressfit in 30° of retroversion regardless of prosthesis type. Adequate soft tissue balance was assessed and achieved. The subscapularis was repaired in all patients undergoing anatomic TSA with sutures that were placed through drill holes in the humerus. For patients undergoing reverse TSA, the subscapularis was only repaired if a tension-free repair could be achieved with the shoulder in 15° of external rotation.
Patients were placed in a shoulder immobilizer for 4 weeks. Patients initiated pendulum exercises and distal range of motion (ROM; distal indicates elbow, forearm, wrist, and hand) on POD 1. Active ROM was allowed when the sling was discontinued at 4 weeks. Strengthening was started at 12 weeks with the goal of obtaining a full recovery by 6 months postoperatively.
Anesthesia and Pain Management Protocol
In the operating room, patients received intravenous sedation of up to 5 mg of midazolam, 10 to 20 mg of ketamine, and propofol as deemed appropriate. An ultrasound-guided interscalene peripheral nerve block was performed in the operating room, before surgery, using 25 mL bupivacaine, 0.5%, with added 100 µg clonidine, 2 mg preservative-free dexamethasone, and 150 µg buprenorphine (Table 2). During the procedure, patients received either intravenous sedation with a propofol infusion, or general anesthesia with propofol induction, either laryngeal mask airway or endotracheal tube insertion, and general anesthesia maintenance with titrated propofol and 1% sevoflurane. For the intravenous sedation and general anesthesia groups, patients received ketamine (total of 50 mg), ondansetron (4 mg), famotidine (20 mg), dexamethasone (4 mg) and ketorolac (15 mg) during surgery. For postoperative analgesia, patients received intravenous acetaminophen (1000 mg every 6 hours, four total doses) and intravenous ketorolac (15 mg every 8 hours, for three postoperative doses in addition to one dose in the operating room) followed by oral acetaminophen (650 mg every 6 hours for 3 days) and oral meloxicam (7.5–15 mg per day). Oral opioids were available on demand, based on patient description of pain to the nursing staff as mild, moderate, or severe: 50 mg tramadol for mild pain, 100 mg tramadol for moderate pain, or 5 mg oxycodone for severe pain, with escalation to more potent oral opioids if requested by the patient. Each patient also received intravenous patient-controlled analgesia of hydromorphone, but they were advised to use the intravenous patient-controlled analgesia as little as possible.
Table 2.
Multimodal analgesic strategy for total shoulder arthroplasty

Postoperative Data Collection
On POD 1, a research assistant not directly involved in patient care assessed patients while in the hospital. Data collected included NRS pain scores at rest and with movement if possible, opioid and nonopioid medication usage, administration of anticoagulants, Opioid-Related Symptoms Distress Scale, the Hospital Anxiety and Depression Scale, and the PainOUT questionnaire. The Opioid-Related Symptom Distress Scale assesses 12 symptoms ranging from 0 to 4, with 4 being the most distressing. If a symptom is present, it was evaluated for frequency, severity, and disruption level; the composite score was the mean of the 12 symptom-specific scores and ranges from 0 to 4. It has been validated for orthopaedic patients [26]. The PainOut questionnaire includes questions that rate nausea, drowsiness, itching from 0 (none) to 10 (severe), as well as rating difficulty staying asleep from 0 (does not interfere) to 10 (completely interferes) [13]. This study focused on pain, opioid use, and opioid-related complications. Bruising was also assessed on POD 14 and POD 90. We reviewed electronic medical records for unexpected events, but we did not conduct formal assessments of block-related nerve injuries. We recorded discharge time and the analgesics prescribed at discharge. On POD 3 and POD 7, patients were contacted by telephone to assess current NRS pain scores at rest and with movement as well as the pain medications and anticoagulants they had been taking since hospital discharge. On POD 14, a research assistant contacted the patient by telephone and collected NRS pain scores at rest and with movement (the primary outcome). Additionally, pain medication usage in the last week was noted and the PainOUT questionnaire was administered. On POD 90, patients were contacted to assess pain scores at rest and with movement and record whether they had taken opioid medications in the prior 24 hours.
Statistical Analysis and Sample Size
The primary outcome, pain intensity with movement on POD 14, is presented as a median with interquartile range (IQR) and a 95% confidence interval (CI) calculated using the percentile bootstrap method from 1000 resamples. Continuous and ordinal secondary outcomes, including pain intensity with movement (PODs 1, 3, 7, and 90), pain intensity at rest (PODs 1, 3, 7, 14, and 90), opioid consumption (PODs 0–14), number of activations of the intravenous patient-controlled analgesia (POD 0–hospital discharge), PainOut scores (PODs 1 and 14), and Opioid-Related Symptom Distress Scale composite score (POD 1) are presented as medians with IQRs. Binary secondary outcomes including NRS pain score with movement ≥ 4 on POD 14, ≥ five intravenous patient-controlled analgesia pushes during the first 24-hour period after surgery, and any opioid use on POD 90 are presented as frequencies with percentages. We used multivariable logistic regression to explore the potential associations of a subset of a priori selected baseline variables with (1) the odds of NRS pain score with movement ≥ 4 on POD 14 and (2) the odds of ≥ five intravenous patient-controlled analgesia pushes during the first 24-hour period after surgery. Models included the following baseline covariates: fibromyalgia trait score, Patient Catastrophizing Scale score, Hospital Anxiety and Depression Scale anxiety subscale score, depression subscale score, gender, preoperative opioid use (yes versus no), and NRS pain score with movement. There was no evidence of multicollinearity between the included covariates as evidenced by variance inflation factors < 2. We assessed logistic regression model discriminatory ability using the c-statistic. All statistical hypothesis tests were two-sided. Statistical analyses were performed with SAS Version 9.4 (SAS Institute Inc, Cary, NC, USA).
Assuming a SD in NRS pain score with movement on POD 14 of 2.3 points [24], we determined a priori that enrollment of 100 patients would provide acceptable precision, that is a 95% CI half-width of 0.5, for the mean NRS pain score estimate.
Results
Pain scores on POD 1 were lower than preoperative scores and peaked on POD 3 (Fig. 2). The median NRS pain scores with movement were 2 (IQR, 0–5) on POD 1, 5 (IQR, 3–6) on POD 3, and the pain score was 3 (IQR, 1–5) on POD 14, with a 95% CI, 2–3 (see Appendix, Supplemental Digital Content 1). The median (IQR) NRS pain score with movement on POD 14 (primary outcome) was 3 (IQR, 1–5) among reverse TSA patients and 3 (IQR, 1-4) for TSA patients (Wilcoxon rank-sum test; p = 0.138). In all, 40 of 102 patients (39%) reported an NRS pain score with movement ≥ 4 on POD 14. There were no associations between baseline measurements (fibromyalgia, catastrophizing, anxiety, depression, gender, preoperative opioid use, or pain scores) and the odds of reporting an NRS pain score with movement ≥ 4 on POD 14 (c-statistic = 0.662; Table 3). By POD 90, median pain scores were 0 (IQR, 0–0) at rest and 1 (IQR, 0–3) with movement (see Appendix, Supplemental Digital Content 1).
Fig. 2.

Pain scores over time are shown. The boxes consist of the first quartile, median, and third quartile. The whiskers extend to the most extreme observations within 1.5 times the interquartile range below and above the first and third quartiles, respectively. Diamonds represent mean values and circles represent outliers. POD 0 represents preoperative values; NRS = numerical rating scale.
Table 3.
Multivariable logistic regression model of NRS pain score with movement ≥ 4 on POD 14

Median opioid use peaked during the second 24-hour period after surgery, and the median opioid use declined to 0 by the eighth 24-hour period (Fig. 3). Median (IQR) total opioid use (converted to oral morphine equivalents) was 18 mg (IQR, 4–50) for the first 24 hours, 30 mg (IQR, 7–63) for the third, and 0 mg (IQR, 0–20) by the eight 24-hour period (see Appendix, Supplemental Digital Content 1). Opioid use at POD 90 was reported by seven of 83 patients (8%). The median number of activations of the intravenous patient-controlled analgesia over the entire hospital stay was 2 (IQR, 0–9; Fig. 4), while the most frequent number of activations was 0. Use of five or more patient-controlled analgesia activations during the first 24 hours postoperatively was noted in 24 of 101 patients (24%). There were no associations between baseline measurements and the odds of five or more patient-controlled analgesia activations during the first 24 hours postoperatively (c-statistic = 0.622; Table 4).
Fig. 3.
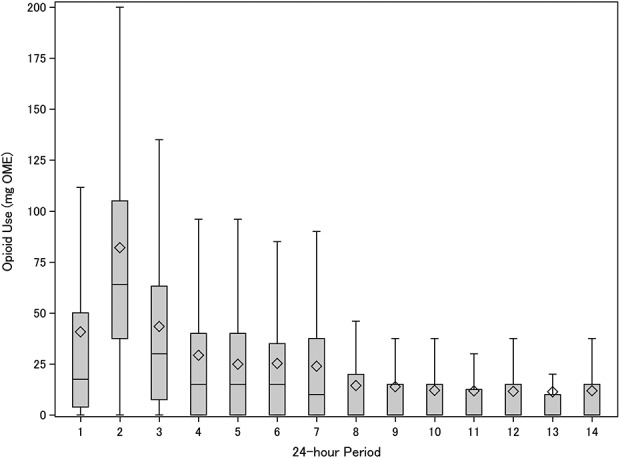
Opioid consumption over time is shown. Opioid use was converted to mg oral morphine equivalents (OME).
Fig. 4.

Cumulative number of activations of intravenous patient-controlled analgesia (IV PCA) over the hospital stay are depicted.
Table 4.
Multivariable logistic regression model of ≥ 5 IV patient-controlled analgesia pushes during the first 24-hour period after surgery

Median PainOut scores on POD 1 and POD 14 for sleep interference, nausea, drowsiness and itching were 0 (Table 5). Patients reported that they spent 0% (IQR, 0–0%) of their time on POD 1 in severe pain, with similar results POD 14; 0% (IQR, 0–10%). The median composite Opioid-Related Symptom Distress Scale score on POD 1 was 0.3 (IQR, 0.1–0.5).
Table 5.
Selected PainOUT questionnaire responses

Discussion
Reliance on opioids alone for pain management after TSA both gives poor quality analgesia and exposes patients to excessive amounts of opioids. Various methods have been proposed to manage pain, but none emerge as clearly superior; it is important that any approach minimizes postoperative opioid use. It is unclear with these protocols how much pain patients will experience, how many opioids will be used, and what opioid-related side effects they will experience. This study found that combining a long-acting single-injection nerve block with multimodal analgesia resulted in median NRS pain scores at movement that peaked on POD 3 at a score of 5, and were consistently lower than preoperative pain scores. Total opioid usage (oral and intravenous) peaked on POD 2, while the median number of activations of the intravenous patient-controlled analgesia was two. Opioid side-effects were not prominent; they were rated a median of 0 out of 10.
Weaknesses of the study include the absence of a comparator group. If the study had used the most extreme comparator group (no block, opioids only without multimodal adjuvants), it may have shown some distinct differences among groups, but the control group would have been outside of the standard of care for our institution and study designers would have lacked the equipoise necessary for efficient patient recruitment. The point of this study was to apply what we believed to be a “best of breed” protocol, and document the outcomes to serve as a benchmark. This a cohort study, so it was not blinded, and as such, there is the possibility of assessor bias. This limitation is inherent to the study design, but it is unclear that the research assistants would systematically introduce bias as they were not incentivized to achieve favorable outcomes. Patients may have taken opioids, including activation of the intravenous patient-controlled analgesia, without actual desire for pain relief, either as an experiment, as a sleep aid, or inadvertently. Given patient autonomy, there is no practical way to prevent such misuse, and this criticism applies to most studies that measure opioid use. Although no major adverse events were noted, a larger study would likely provide narrow confidence intervals for rates of rare or absent events. Because of the sample size and the low expected incidence, we did not directly question patients about block-related nerve injuries. A previous study at the authors’ institution rigorously assessed rates of complications after ultrasound-guided nerve blockade for shoulder surgery [10]. Among 1169 patients, no permanent nerve injuries occurred and temporary neurologic symptoms at 1 week were noted in 5 of 1169 patients (0.4%). Although this rate was for patients undergoing arthroscopic shoulder surgery, not TSA, there is no reason to think that block-related (as opposed to surgery-related) complications are more common for TSA. The study sample size was chosen to estimate an adequately precise estimate of the central tendency of NRS pain score with movement on POD 14. Therefore, this study was not specifically powered to detect associations between baseline variables and the odds of NRS pain score with movement ≥ 4 on POD 14 or ≥ five patient-controlled analgesia activations during the first 24 hours postoperatively, and thus may be prone to type II error. Further, whether associations (or lack thereof) between each covariate and outcome vary by gender (as determined by adequately-powered tests for interactions between gender and other covariates) will need to be explored in much larger samples. However, this study suggests that although gender and preexisting psychological conditions could affect the pain experiences of patients undergoing TSA, the effect size may not be large enough to make clinically useful predictions. Although patients were not excluded because of preexisting pain or psychiatric diagnoses, it is possible that a different cohort with a greater burden of either preoperative pain or psychological distress would have obtained different results. We believe that the data presented in this trial apply to our patient population. It would have been instructive to gather information about block duration, but we have previously published data about duration of interscalene nerve blockade using these adjuvant medications [25]. The previous randomized trial (investigating the same three additives combined with ropivacaine, a different long-acting local anesthetic) found that the blocks lasted 20 to 25 hours [25]. Due to the pragmatic trial design, the focus of the study was on the patient-oriented outcomes of pain, opioid use and opioid side-effects, not block duration per se.
The described protocol of a long-acting, single-shot block with multimodal analgesia was associated with median NRS pain with movement levels that peaked on POD 3 at 5, and subsided to 3 by POD 14. This information should be provided to patients so that they can have reasonable expectations about pain after TSA. In other studies, patients who did not receive complex pain management protocols reported peak pain levels as high as 8.5 on POD 1 [7]. Our pain results with a long-acting, single-shot block and multimodal analgesia are similar to pain results reported with use of perineural catheters. Median pain scores on POD 1 are reported to be 1.0 (IQR, 0.0–6.4) at rest and 2.0 (IQR, 0.0–8.7) with movement, in patients with effective catheters [7]. We noted virtually identical median (Q1, Q3) pain on POD 1 of 1 (IQR, 0–2) at rest and 2 (IQR, 0–5) with movement. However, catheters pose their own set of complications and problems. In the study referenced above, the investigators included only “accurately placed” catheters [7], implying there may be some technical variations that influence catheter effectiveness. In another cohort study, 6.8% of patients discharged with interscalene catheters needed interventions for problems such as catheter dislodgement, tip occlusion, and pump disconnection [17]. Therefore, our study shows that a single-shot block can provide similar pain relief as catheters, without the problems of inaccurate placement and various other catheter-specific complications. Combining adjuvant analgesic compounds (clonidine, dexamethasone, buprenorphine) with local anesthetic for single-injection interscalene blocks for TSA patients was previously shown to reduce NRS pain with movement at 24 hours from 4.9 +/- 2.5 (for control patients) to 3.4 +/- 1.8 (for patients receiving perineural adjuvant analgesics) [25]. The use of multiple perineural additives, while off-label, has been evaluated for stability and in vivo safety [21] and has been previously used for hip and knee arthroplasty and upper extremity procedures [22], TSA [25], and foot and ankle surgery [27]. Relatively little published information is available about pain scores on POD 14. In one study, mean pain scores for patients receiving perineural catheters were about 3.1 on POD 1 and about 3.7 on POD 14 compared with pain scores of about 3.5 on POD 1 and about 3.7 on POD 14 after liposomal bupivacaine injection [20]. In comparison, we reported a POD 14 pain score of 3. Given the additional cost of catheters and liposomal bupivacaine, it is hard to justify their use. However, further head-to-head studies are needed to definitively make such conclusions.
Median postoperative total opioid use (converted to oral morphine equivalents) was 16 mg for the first 24 hours, 30 mg for the third, and 0 mg by the eighth 24-hour period. Previously, a protocol that provided TSA patients with multimodal analgesia and a nerve block without adjuvants reported greater intake; 61.8 mg oral morphine equivalents (OMEs) in the first 24 hours, and 44.9 mg in the second 24-hour period [5]. A study that compared nerve block with nerve block plus multimodal analgesia showed that the use of multimodal analgesia reduced opioid consumption on POD 1 from approximately 110 mg OMEs to approximately 70 mg [11]. Patients undergoing TSA who had a liposomal bupivacaine injection used the equivalent of 130 mg OMEs in the first 24 hours, while use of perineural catheters was associated with 64 mg OMEs [20]. Thus, the current analgesic protocol was associated with fewer postoperative opioids than is reported with many other protocols. We found that many patients did not use intravenous patient-controlled analgesia, and the median number of doses was two, suggesting that these patients do not necessarily need to remain in the hospital for pain management and could potentially be discharged earlier. Future studies could investigate additional methods to further reduce opioid usage.
Median scores on POD 1 and POD 14 for sleep interference, nausea, drowsiness and itching were 0, while the median patient spent no time in severe pain on either POD 1 or POD 14. The median composite Opioid-Related Symptom Distress Scale score of 0.3 on POD 1 was less than the previously reported median POD 1 scores after either ACL reconstruction (0.52), knee arthroplasty (0.51), or posterior lumbar spine fusion (0.94) [26]. These results indicate that the opioid usage reported in this protocol is associated with a low risk of opioid-related side effects.
In conclusion, a long-acting, single-shot brachial plexus block coupled with multimodal analgesia can achieve low pain scores and allow rapid self-tapering of opioids in patients undergoing TSA. The pain scores seen in this study are consistent with those reported in other studies among patients receiving catheters and liposomal bupivacaine, but the current protocol was associated with less opioid usage. Patients with characteristics similar to those in this study who receive this multimodal analgesic protocol can be informed that, on average, their postoperative pain will likely be less than preoperative pain, that most of them will not use large amounts of intravenous opioids, that their use of opioids will likely peak on POD 2, and that they can expect to wean themselves off of opioids after about a week. Future research based on these results could investigate the precise contributions of each of the individual components of this protocol. Larger cohort studies or registries would document incidence of rare complications. Randomized controlled trials could directly compare analgesic effectiveness and cost-benefits for this protocol versus alternative strategies, such as perineural catheters or liposomal bupivacaine. Perhaps most importantly, future studies could seek ways to further reduce peak pain and opioid usage on POD 2 and POD 3.
Acknowledgments
We thank George Birch and Alexandra Sideris for assistance with the manuscript.
Footnotes
The work was supported by the Research and Education Fund of the Department of Anesthesiology, Critical Care & Pain Management at the Hospital for Special Surgery (JTY). REDCap use was supported by the National Center for Advancing Translational Science of the National Institute of Health (UL1TR000457).
One of the authors certifies that he (JTY) has received or may receive payments or benefits, during the study period, in an amount of USD 10,000 to USD 100,000 from Mallinckrodt (Hampton, NJ, USA). One of the authors certifies that he (DMD) has received or may receive payments or benefits, during the study period, in an amount of less than USD 10,000 from Thieme Inc (New York, NY, USA) and receives royalties in an amount of USD 100,001 to USD 1,000,000 from Zimmer Biomet Inc (Warsaw, IN, USA). One of the authors certifies that he (LVG) has received or may receive speaking and consultant fees, during the study period, in an amount of USD 10,000 to USD 100,000 from Zimmer Biomet Inc (Warsaw, IN, USA).
All ICMJE Conflict of Interest Forms for authors and Clinical Orthopaedics and Related Research® editors and board members are on file with the publication and can be viewed on request.
Clinical Orthopaedics and Related Research® neither advocates nor endorses the use of any treatment, drug, or device. Readers are encouraged to always seek additional information, including FDA approval status, of any drug or device before clinical use.
Each author certifies that his or her institution approved the human protocol for this investigation and that all investigations were conducted in conformity with ethical principles of research.
References
- 1.Bjelland I, Dahl AA, Haug TT, Neckelmann D. The validity of the Hospital Anxiety and Depression Scale. An updated literature review. J Psychosom Res. 2002;52:69-77. [DOI] [PubMed] [Google Scholar]
- 2.Breivik H, Borchgrevink PC, Allen SM, Rosseland LA, Romundstad L, Hals EK, Kvarstein G, Stubhaug A. Assessment of pain. Br J Anaesth. 2008;101:17-24. [DOI] [PubMed] [Google Scholar]
- 3.Brummett CM, Janda AM, Schueller CM, Tsodikov A, Morris M, Williams DA, Clauw DJ. Survey criteria for fibromyalgia independently predict increased postoperative opioid consumption after lower-extremity joint arthroplasty: a prospective, observational cohort study. Anesthesiology. 2013;119:1434-1443. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Bryan NA, Swenson JD, Greis PE, Burks RT. Indwelling interscalene catheter use in an outpatient setting for shoulder surgery: technique, efficacy, and complications. J Shoulder Elbow Surg. 2007;16:388-395. [DOI] [PubMed] [Google Scholar]
- 5.Goon AK, Dines DM, Craig EV, Gordon MA, Goytizolo EA, Lin Y, Lin E, YaDeau JT. A clinical pathway for total shoulder arthroplasty-a pilot study. HSS J. 2014;10:100-106. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Hadzic A, Williams BA, Karaca PE, Hobeika P, Unis G, Dermksian J, Yufa M, Thys DM, Santos AC. For outpatient rotator cuff surgery, nerve block anesthesia provides superior same-day recovery over general anesthesia. Anesthesiology. 2005;102:1001-1007. [DOI] [PubMed] [Google Scholar]
- 7.Ilfeld BM, Wright TW, Enneking FK, Morey TE. Joint range of motion after total shoulder arthroplasty with and without a continuous interscalene nerve block: a retrospective, case-control study. Reg Anesth Pain Med. 2005;30:429-433. [DOI] [PubMed] [Google Scholar]
- 8.Jeng CL, Torrillo TM, Rosenblatt MA. Complications of peripheral nerve blocks. Br J Anaesth. 2010;105:i97-i107. [DOI] [PubMed] [Google Scholar]
- 9.Kehlet H, Jensen TS, Woolf CJ. Persistent postsurgical pain: risk factors and prevention. Lancet. 2006; 367:1618-1625. [DOI] [PubMed] [Google Scholar]
- 10.Liu SS, Gordon MA, Shaw PM, Wilfred S, Shetty T, Yadeau JT. A prospective clinical registry of ultrasound-guided regional anesthesia for ambulatory shoulder surgery. Anesth Analg. 2010;111:617-623. [DOI] [PubMed] [Google Scholar]
- 11.McLaughlin DC, Cheah JW, Aleshi P, Zhang AL, Ma CB, Feeley BT. Multimodal analgesia decreases opioid consumption after shoulder arthroplasty: a prospective cohort study. J Shoulder Elbow Surg. 2018;27:686-691. [DOI] [PubMed] [Google Scholar]
- 12.Namdari S, Nicholson T, Abboud J, Lazarus M, Steinberg D, Williams G. Interscalene block with and without intraoperative local infiltration with liposomal bupivacaine in shoulder arthroplasty: a randomized controlled trial. J Bone Joint Surg Am. 2018;100:1373-1378. [DOI] [PubMed] [Google Scholar]
- 13.Rothaug J, Zaslansky R, Schwenkglenks M, Komann M, Allvin R, Backstrom R, Brill S, Buchholz I, Engel C, Fletcher D, Fodor L, Funk P, Gerbershagen HJ, Gordon DB, Konrad C, Kopf A, Leykin Y, Pogatzki-Zahn E, Puig M, Rawal N, Taylor RS, Ullrich K, Volk T, Yahiaoui-Doktor M, Meissner W. Patients' perception of postoperative pain management: validation of the International Pain Outcomes (IPO) questionnaire. J Pain. 2013;14:1361-1370. [DOI] [PubMed] [Google Scholar]
- 14.Sabesan VJ, Shahriar R, Petersen-Fitts GR, Whaley JD, Bou-Akl T, Sweet M, Milia M. A prospective randomized controlled trial to identify the optimal postoperative pain management in shoulder arthroplasty: liposomal bupivacaine versus continuous interscalene catheter. J Shoulder Elbow Surg. 2017;26:1810-1817. [DOI] [PubMed] [Google Scholar]
- 15.Sox HC, Lewis RJ. Pragmatic trials: practical answers to "real world" questions. JAMA. 2016;316:1205-1206. [DOI] [PubMed] [Google Scholar]
- 16.Sullivan MJ, Bishop SR, Pivik J. The pain catastrophizing scale: development and validation. Psychol Assess. 1995;7:524. [Google Scholar]
- 17.Swenson JD, Bay N, Loose E, Bankhead B, Davis J, Beals TC, Bryan NA, Burks RT, Greis PE. Outpatient management of continuous peripheral nerve catheters placed using ultrasound guidance: an experience in 620 patients. Anesth Analg. 2006;103:1436-1443. [DOI] [PubMed] [Google Scholar]
- 18.Vandepitte C, Kuroda M, Witvrouw R, Anne L, Bellemans J, Corten K, Vanelderen P, Mesotten D, Leunen I, Heylen M, Van Boxstael S, Golebiewski M, Van de Velde M, Knezevic NN, Hadzic A. Addition of liposome bupivacaine to bupivacaine HCl versus bupivacaine HCl alone for interscalene brachial plexus block in patients having major shoulder surgery. Reg Anesth Pain Med. 2017;42:334-341. [DOI] [PubMed] [Google Scholar]
- 19.Veal FC, Bereznicki LR, Thompson AJ, Peterson GM, Orlikowski C. Subacute pain as a predictor of long-term pain following orthopedic surgery: an Australian prospective 12 month observational cohort study. Medicine (Baltimore). 2015;94:e1498. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Weller WJ, Azzam MG, Smith RA, Azar FM, Throckmorton TW. Liposomal bupivacaine mixture has similar pain relief and significantly fewer complications at less cost compared to indwelling interscalene catheter in total shoulder arthroplasty. J Arthroplasty. 2017;32:3557-3562. [DOI] [PubMed] [Google Scholar]
- 21.Williams BA, Butt MT, Zeller JR, Coffee S, Pippi MA. Multimodal perineural analgesia with combined bupivacaine-clonidine-buprenorphine-dexamethasone: safe in vivo and chemically compatible in solution. Pain Med. 2015;16:186-198. [DOI] [PubMed] [Google Scholar]
- 22.Williams BA, Ibinson JW, Mangione MP, Modrak RT, Tonarelli EJ, Rakesh H, Kmatz AM, Cohen PZ. Research priorities regarding multimodal peripheral nerve blocks for postoperative analgesia and anesthesia based on hospital quality data extracted from over 1,300 cases (2011–2014). Pain Med. 2015;16:7-12. [DOI] [PubMed] [Google Scholar]
- 23.Wolfe F, Clauw DJ, Fitzcharles MA, Goldenberg DL, Hauser W, Katz RS, Mease P, Russell AS, Russell IJ, Winfield JB. Fibromyalgia criteria and severity scales for clinical and epidemiological studies: a modification of the ACR Preliminary Diagnostic Criteria for Fibromyalgia. J Rheumatol. 2011;38:1113-1122. [DOI] [PubMed] [Google Scholar]
- 24.YaDeau JT, Brummett CM, Mayman DJ, Lin Y, Goytizolo EA, Padgett DE, Alexiades MM, Kahn RL, Jules-Elysee KM, Fields KG, Goon AK, Gadulov Y, Westrich G. Duloxetine and subacute pain after knee arthroplasty when added to a multimodal analgesic regimen: a randomized, placebo-controlled, triple-blinded trial. Anesthesiology. 2016;125:561-572. [DOI] [PubMed] [Google Scholar]
- 25.YaDeau JT, Gordon MA, Goytizolo EA, Lin Y, Fields KG, Goon AK, Holck G, Miu TW, Gulotta LV, Dines DM, Craig EV. Buprenorphine, clonidine, dexamethasone, and ropivacaine for interscalene nerve blockade: aprospective, randomized, blinded, ropivacaine dose-response study. Pain Med. 2016;17:940-960. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.YaDeau JT, Liu SS, Rade MC, Marcello D, Liguori GA. Performance characteristics and validation of the Opioid-Related Symptom Distress Scale for evaluation of analgesic side effects after orthopedic surgery. Anesth Analg. 2011;113:369-377. [DOI] [PubMed] [Google Scholar]
- 27.YaDeau JT, Paroli L, Fields KG, Kahn RL, LaSala VR, Jules-Elysee KM, Kim DH, Haskins SC, Hedden J, Goon A. Addition of dexamethasone and buprenorphine to bupivacaine sciatic nerve block: a randomized, controlled trial. Reg Anesth Pain Med. 2015;40:321. [DOI] [PMC free article] [PubMed] [Google Scholar]