

Abstract
Background:
Sleep health can be characterized using multiple dimensions, including regularity, satisfaction, alertness, timing, efficiency, and duration. This study provides a preliminary derivation of a Sleep Health Composite score in adolescents with eveningness chronotype and examined its associations with mental and physical health outcomes.
Methods:
Participants were 176 adolescents (mean age 14.77 years, 58% female) who participated in an RCT examining the Transdiagnostic Sleep and Circadian Intervention. At study entry, the sample was characterized by evening circadian preference, later bedtime, and increased risk in one of five health domains (emotional, cognitive, behavioral, social, and physical). The Sleep Health Composite was derived using 7-days sleep diary and self-report rating scales. Each dimension was categorized as “good” or “poor” using cut-offs informed by prior studies and expert consensus. Mental and physical health outcomes were assessed using self-report rating scales, semi-structured clinical interviews, parent report, or biometric measurement.
Results:
Sleep duration and satisfaction dimensions were most commonly rated as poor. Greater sleep health, as indexed by greater Sleep Health Composite score, was concurrently associated with lower risk in emotional, cognitive, and social domains, fewer physical symptoms, and reduced odds for obesity and current mood or anxiety disorders.
Conclusions:
Sleep health is an important correlate of mental and physical health outcomes in adolescents. The Sleep Health Composite has potential application as an outcome measure in treatment studies of sleep and circadian problems.
Keywords: sleep health, adolescents, evening circadian preference, depression, anxiety, obesity
Sleep and circadian disturbances are prominent across a wide range of mental and medical disorders. These disturbances may include insomnia, hypersomnia, reduced sleep need, delayed and advanced sleep phase, each of which may co-occur with the others, and be present at syndromal or sub-syndromal levels.1–3 Our goal was to provide a “proof-of-concept” example of a composite measurement that includes multiple sleep dimensions. In so doing, we build on prior work designed to unify methodological practices for single disorders, such as the standard research assessment for insomnia.4
The sleep health framework is the theoretical basis for this study.5 Sleep health is defined as ‘a multidimensional pattern of sleep-wakefulness, adapted to individual, social, and environmental demands, that promotes physical and mental well-being.’ This definition emphasizes that sleep health is a broader construct than specific sleep disorders, and that it plays a positive role in the overall health and functioning of an individual or population.5 This approach encourages us to view sleep health as a multidimensional construct comprising six dimensions of sleep and circadian functioning: satisfaction, alertness, timing, efficiency, duration and regularity. These six dimensions were proposed based on theoretical plausibility and empirical evidence linking each dimension with physical and mental health outcomes.5 A recent investigation found that an aggregate measure based on five of the dimensions proposed in the sleep health framework was associated with prevalent and incident depression symptoms.6 Another recent study found multidimensional sleep variables were associated with mortality in older men.7 The present study sought to extend this approach by testing the utility of a Sleep Health Composite score derived from self-reported sleep measure.
Composite measures of sleep health can also inform treatment. The transdiagnostic sleep and circadian (TranS-C) intervention is under empirical examination in youth and adult populations.8 TranS-C is designed to address a variety of sleep problems across psychiatric disorders, including insomnia, delayed and advanced sleep phase, difficulty waking up or getting out of bed in the morning, too much time in bed, daytime sleepiness, inadequate opportunity to sleep, irregular sleep-wake schedules, and worry/rumination. During the development and testing of TranS-C, it became apparent that the use of single disorder-focused measures for a transdiagnostic treatment is problematic. For example, decreased time in bed is often indicated in the treatment of insomnia, but increased time in bed is indicated in the case of insufficient sleep. Also, an earlier bedtime indicates a positive change in the case of delayed sleep phase, but a later bedtime is a positive change in the case of advanced sleep phase. Therefore, simple computations of time in bed and sleep timing cannot be used as outcome measures for TranS-C. The Sleep Health Composite is intended to capture the variety and complexity of the sleep problems experienced by people with a wide range of mental and medical disorders and accommodates differences in treatment goals that may vary depending on the presenting sleep-circadian problem.
The current study provides a proof-of-concept example of the utility of measuring multidimensional sleep health in adolescents. This is a particularly important and interesting group developmentally, as it poses challenges to several of the proposed sleep health dimensions, especially timing, duration, and regularity. Social changes (e.g., less parental control), increased academic demands (e.g., early wake-up times for school), and a biological shift towards a delayed phase sleep triggered by puberty onset often interact to result in short duration, late timing, and reduced regularity of sleep. The current study used baseline data from a randomized controlled trial testing TranS-C in adolescents who exhibited these sleep problems.The current study had three specific aims: 1) to describe the preliminary development of a Sleep Health Composite derived from self-reported sleep measures and report its descriptive statistics; 2) to investigate whether the Sleep Health Composite was concurrently associated with the primary outcomes related to the five health domains of the TranS-C RCT at pre-treatment; 3) to investigate whether the Sleep Health Composite was concurrently associated with additional psychiatric and physical conditions, as well as past year medical history at pre-treatment. We examined outcomes such as obesity 9 and major depressive disorders 6 that have been associated with sleep disturbances, and/or evening circadian chronotype in the extant literature.
Methods
Participants and Procedures
Participants were 176 adolescents recruited through clinician referrals and advertisements from January 2013 to February 2016. Table 1 shows the demographic information for the participants. A detailed description of the study procedure can be found elsewhere.10 Briefly, participants and parents/guardians were first screened for eligibility via a telephone interview, and potentially eligible individuals participated in an in-person assessment session to determine eligibility. Eligible participants were randomized to receive either TranS-C or psychoeducation for 6 weekly sessions. All participants’ parents or guardians provided informed consent and participants provided informed assent. The current study used only pre-treatment data for the whole sample.
Table 1.
Demographic Characteristics of the Sample (N=176).
| Characteristic | N (%) or M (SD) |
|---|---|
| Female | 102 (58) |
| Hispanic/Latino | 27(15) |
| Race | |
| Caucasian | 114 (65) |
| African American/Black | 12 (7) |
| American Indian or Alaska Native | 0 (0) |
| Asian | 18 (10) |
| Native Hawaiian/Other Pacific Islander | 2 (1) |
| Mixed Race | 30 (17) |
| Family annual income | |
| ≤ 20,000 | 6 (3) |
| 20,001 – 50,000 | 21 (12) |
| 50,001 – 100,000 | 42 (24) |
| 100,000+ | 102 (58) |
| Refused to answer/missing | 5 (3) |
| Current grade | 9.39 |
| Any current K-SADS Dx (teen report) | 63/171 (37) |
| Any past K-SADS Dx (teen report) | 77/171 (45) |
| Any current K-SADS Dx (parent report) | 49/168 (29) |
| Any past K-SADS Dx (parent report) | 55/168 (33) |
| Age | 14.77 (1.84) |
Note. M = Mean. SD = Standard Deviation. K-SADS = Kiddie Schedule for Affective Disorders and Schizophrenia.
Inclusion criteria were: 1) 10 to 18 years old, living with a parent or guardian, and attending a class/job by 9AM at least 3 days per week; 2) fluent in English; 3) able and willing to give informed assent; 4) self-reported eveningness as demonstrated by scoring within the lowest quartile of the Children’s Morningness-Eveningness Preferences Scale (CMEP; 27 or lower 11) and sleep onset time of 10:40 PM or later for 10–13 year olds, 11:00 PM or later for 14–16 year olds, and 11:20 PM or later for 17–18 year olds at least 3 nights per week for the last 3 months with a 7-day sleep diary; 12,13 5) scoring ‘at risk’ on at least one of the five health domains (for specific criteria see Appendix).
Exclusion criteria included an active, progressive physical illness or neurological degenerative disease directly related to the sleep disturbance, evidence of obstructive sleep apnea, restless legs syndrome, or periodic limb movement disorder (per self-report or Duke structured interview for sleep disorders), pervasive developmental disorder, bipolar, schizophrenia, taking medications that directly affect sleep (e.g., hypnotics) within 4 weeks of the assessment (2 weeks for melatonin), substance dependence in the past six months, and current suicide risk sufficient to preclude treatment on an outpatient basis.
Measures
Sleep Diary.14
Sleep diary was collected by trained research assistants via phone calls in the morning to adolescent participants during a one week (7-day) period at pre-treatment. Sleep duration (total sleep time), timing (midpoint sleep), regularity (SD of midpoint sleep), and sleep efficiency (total sleep time/total time in bed) dimensions of the Sleep Health Composite were derived using sleep diary indices. Total sleep time was calculated as follows: total sleep time = time in bed – sleep onset latency - wake after sleep onset - terminal wakefulness. Descriptive statistics of all sleep diary indices are reported in supplemental Table S1.
Pittsburgh Sleep Quality Index (PSQI).15
PSQI was administered at pre-treatment assessment. The satisfaction dimension of the Sleep Health Composite was derived using question 6 from the PSQI: “During the past month, how would you rate your sleep quality overall?” Participants were asked to rate on a 4-point scale (0 = Very Good, 1 = Fairly Good, 2 = Fairly Bad, and 3 = Very Bad).
Sleepiness Scale.
The 10-item Sleepiness Scale 16 was administered at pre-treatment assessment. Each item was rated on a 4-point scale (0 = No, 1 = Struggled to stay awake, 2 = Fallen asleep, 3 = Both struggled to stay awake and fall asleep). The alertness dimension of the Sleep Health Composite was derived using the Sleepiness Scale (reverse coded).
Children’s Morningness-Eveningness Preferences Scale (CMEP).17
CMEP was used to assess the adolescents’ chronotype. Scores range from 10 (Extreme evening preference) to 43 (Extreme morning preference).
Functioning in five health domains.
Five youth self-report composite risk scores, each composed of measures in emotional, cognitive, behavioral, social, or physical health, were used to indicate functioning in five health domains. Specific measures for each domain are detailed in the supplement. The composite scores were calculated for each of the five health domains by taking the mean of standardized summary scores for specific measures within that domain. Composite scores were created because individual measures within each domain used different scales. Due to the large number of measures in this study, creating a composite score was also a method to control for the multiplicity problem and increase statistical power.18 As shown in Table 3, composite scores have means close to 0 and standard deviations slightly less than 1. The interpretation of the composite scores is similar to standardized scores: a positive/larger composite score indicates greater risk in that domain, whereas a negative/smaller composite score indicates lower risk. Summary scores for specific measures were reverse coded when necessary so that all scores of specific measures within a domain would have the same direction.
Table 3.
Descriptive Statistics of the Sleep Health Composite and Other Study Variables.
| Variables | M (SD) or N (%) |
|---|---|
| Sleep Health Composite | |
| Total score (continuous) | 3.66 (1.36) |
| Total count | 175** (100.00) |
| 0 | 3 (1.71) |
| 1 | 10 (5.71) |
| 2 | 19 (10.86) |
| 3 | 42 (24.00) |
| 4 | 49 (28.00) |
| 5 | 41 (23.43) |
| 6 | 11 (6.29) |
| Dimensions (% poor) | |
| Regularity | 52 (31.52) |
| Satisfaction | 78 (46.71) |
| Alertness | 63 (36.63) |
| Timing | 30 (18.07) |
| Efficiency | 25 (15.06) |
| Duration | 113 (68.07) |
| Sleep and Circadian Outcomes | |
| Total sleep time weeknights | 456.48 min (63.18 min) |
| Bedtime weeknights | 22 hr 56 min (1 hr 04 min) |
| Children’s Morningness-Eveningness Preferences (CMEP) | 21.35 (3.81) |
| Youth Self-Report Composite Risk Score | |
| Emotional domain* | 0.02 (0.86) |
| Children’s Depression Rating Scale | 33.52 (9.55) |
| Multidimensional Anxiety Scale for Children | 46.07 (16.82) |
| Cognitive domain* | 0.004 (0.80) |
| Attention Control Scale | 50.94 (7.73) |
| Youth Social Adjustment Scale: school/cognitive | 11.78 (2.89) |
| Behavioral domain* | −0.003 (0.83) |
| Sensation Seeking Scale | 26.86 (6.07) |
| Alcohol and Substance Use | 5.73 (7.42) |
| Social domain* | −0.005 (0.66) |
| Youth Social Adjustment Scale: friends | 18.66 (4.79) |
| Youth Social Adjustment Scale: family | 12.14 (3.57) |
| Youth Social Adjustment Scale: romantic | 7.45 (1.86) |
| Physical domain* | 0.01 (0.71) |
| Modifiable Activity Questionnaire | 3.10 (4.85) |
| Physical Health Questionnaire | 8.92 (4.89) |
| Body Mass Index (BMI) | |
| BMI (continuous) | 22.28 (4.68) |
| Obese (BMI ≥30) | 9 (5.20) |
| Overweight & Obese (BMI ≥ 25) | 32 (25.00) |
| Underweight (BMI < 18.5) | 36 (27.27) |
| Normal weight (BMI 18.5–24.99) | 96 (55.49) |
| Medical problem (past year) | 31 (17.03) |
| K-SADS diagnostic classes | |
| Any current mood disorder (T) | 16 (9.09) |
| Any current mood disorder (P) | 15 (8.57) |
| Any current anxiety disorder (T) | 49 (27.84) |
| Any current anxiety disorder (P) | 29 (16.57) |
| Any current behavior disorder (T) | 23 (13.37) |
| Any current behavior disorder (P) | 20 (11.43) |
Note. All models controlled for age and sex. Higher Sleep Health Composite indicates better sleep health.
indicates composite scores derived by obtaining the mean of the standardized scores of all measures within each domain. Higher composite risk scores indicate greater risk in that health domain.
One participant had an incomplete sleep diary at pre-treatment and thus had a missing value on the Sleep Health Composite. For variables under “Youth Self-Report Composite Risk Score,” all variables, except for Attention Control Scale and Modifiable Activity Questionnaire, were coded such that higher score indicates greater risk/worse outcome. K-SADS = Kiddie Schedule for Affective Disorders and Schizophrenia. Medical problem (past year) include diabetes, infections, hypertension, high cholesterol, and injury/accidents. Any current mood disorder includes major depressive disorder, dysthymia, bipolar I, bipolar II, bipolar not otherwise specified. Any current anxiety disorder includes agoraphobia, generalized anxiety disorder, social phobia, specific phobia, panic disorder, post-traumatic stress disorder, and acute stress disorder. Any current behavior disorder includes attention deficit hyperactivity disorder, oppositional defiant disorder, conduct disorder, and substance use disorders (alcohol abuse/dependence and drug abuse dependence.
Kiddie Schedule for Affective Disorders and Schizophrenia-Present and Lifetime Version (K-SAD-PL).19
K-SADS-PL was administered to adolescent and one parent to determine current and lifetime DSM-IV Axis I disorder at the pre-treatment assessment by trained graduate-level clinicians and trained project coordinators under the supervision of licensed clinical psychologists. We focused on current DSM-IV Axis I disorders in the current study. The inter-rater reliability in the current study for the K-SADS diagnosis was kappa = 0.78.
To simplify K-SADS variables for the current analysis, we categorized DSM-IV diagnoses into three main classes following Merikangas et al. 20: 1) any current mood disorder, including major depressive disorder, dysthymia, bipolar I, bipolar II, bipolar not otherwise specified; 2) any current anxiety disorder, including agoraphobia, generalized anxiety disorder, social phobia, specific phobia, panic disorder, post-traumatic stress disorder, and acute stress disorder; and 3) any current behavioral disorder, including attention deficit hyperactivity disorder, oppositional defiant disorder, conduct disorder, and substance use disorders (alcohol abuse/dependence and drug abuse dependence. Note that substance use disorders were grouped into the behavioral disorder class due to very low occurrence (2 cases based on adolescent interview and 1 based on parent interview). There was no case for eating disorder in this sample.
Medical History.
At pre-treatment assessment, parents provided a past year medical history of the adolescents via questionnaire. For the purpose of this study, to construct the past year medical problem variable, we selected five medical conditions (diabetes, infections, hypertension, high cholesterol, and injury/accidents) most relevant to sleep health based on evidence reviewed in Buysse (2014).5
Body Mass Index (BMI).
Adolescents’ weight and height were measured twice at pre-assessment, and the average of the two measurements was used to derive the age- and sex-adjusted BMI using the BMI calculator for teens made available by the Centers for Disease Control and Prevention.21
Derivation of the Sleep Health Composite
Derivation of the Sleep Health Composite (see Table 2 for summary) was based on several considerations. First, we made a priori decision to dichotomize each dimension as “good” or “poor,” because this approach is deemed more feasible and deployable in clinical practice as opposed to keeping each individual dimension as a continuous scale. For each dimension, “good” is coded as 1 and “poor” is coded as 0. The Sleep Health Composite was constructed such that higher score indicates better sleep health. The reverse of the Sleep Health Composite represents the number of “poor” or risk dimensions a participant met, similar to a cumulative risk score. e.g., 22 Second, to choose the most appropriate cutoff point for each dimension, we combined three approaches: 1) wherever available, the cutoff point was primarily guided by recommendations from the extant literature; 2) when recommendations were not available, the cutoff point was informed by data from previously published studies in normative samples (i.e., healthy, community adolescents); 3) if none of the aforementioned were available, in addition to 2), we also considered the observed distribution in the current sample, keeping in mind that it is a unique, non-representative sample of community adolescents with eveningness chronotype and who exhibit increased risk in one of the health domains.
Table 2.
Operational Definition of Six Sleep Health Dimensions and Tabulation of Each Dimension in the Current Sample.
| Dimension | Definition |
|---|---|
| Regularity | Midpoint sleep fluctuation across a 7-day sleep diary ≤ 1 hour |
| Satisfaction | Question 6 of the PSQI rated “very good” or “fairly good” |
| Alertness | Sleepiness Scale score ≤ 7.5 |
| Timing | Average midpoint sleep across 7-day sleep diary between 2 and 4 AM |
| Efficiency | Average sleep efficiency of the 7-day sleep diary ≥ 85% |
| Duration | Total sleep time (TST) average across 7-day sleep diary between 9–11 hours for 10–13 years and 8–10 hours for 14–18 years |
Regularity.
Regularity is operationalized as midpoint sleep fluctuation (i.e., SD for midpoint across 7-day sleep diary) ≤ 1 hour. Midpoint sleep is preferred over bedtime or risetime because it incorporates both bedtime and risetime. To the best of our knowledge, no prior literature offers an exact recommendation or cut-off point for what constitutes good regularity. The one-hour cut-off was selected based on both prior literature and the sample distribution in the current study as follows. First, a main source of the intraindividual variability for adolescents comes from the weekday-weekend discrepancy in sleep patterns. Sleep midpoint values reported in Crowley et al. 23 were 2 AM for weekdays and 4 AM for weekends in middle schoolers and 3AM for weekdays and 5 AM for weekends in high schoolers. Therefore, roughly 1-hour weekday-weekend discrepancy on midpoint was observed for both younger and older adolescents in normative samples. Second, in a sample of community-dwelling adolescents with naturalistically unconstrained sleep, low intraindividual variability (IIV; defined as the lower 20% of the sample) was about 0.8 hour for bedtime, about 0.9 hour for rise time, and about 1 hour for time in bed.24 Third, in the current sample, the mean SD for midpoint sleep is 0.9 hours and the majority (75%) of the sample had ≤ 1 hour of sleep fluctuation over a week.
Satisfaction.
Satisfaction is operationalized as the rating for question 6 on the Pittsburgh Sleep Quality Index (PSQI). This question asks “how would you rate your sleep quality.” For the Sleep Health Composite, responses of “Very good and fairly good” were combined to create the category of good satisfaction and “fairly bad and very bad” were combined to create the category of poor satisfaction.
Alertness.
Alertness is operationalized as the total score on the 10-item Sleepiness Scale ≤ 7.5. This cut off was selected because 7.5 equals the mean plus 1 SD reported in healthy adolescents with adequate sleep.16
Timing.
Good sleep timing is operationalized as having an average midpoint sleep across the 7-day sleep diary between 2 and 4 AM. The cut off range was selected because 2–4 AM was derived from normative samples as follows. First, midpoint was 2:42 AM for weekdays and 3:47 AM for weekends in adolescents from National Sleep Foundation 2011 Poll.25 Second, midpoint values calculated using average bedtime and rise time reported in the Crowley et al. 23 review were 2 AM for weekdays and 4 AM for weekends in middle schoolers and 3 AM for weekdays and 5 AM for weekends in high schoolers. Third, the observed midpoint averaged across 7-day sleep diary (Mean +/− 1SD) in our sample of adolescents with evening circadian preference at pre-treatment is between 2:16 AM and 4:36 AM.
Efficiency.
Good sleep efficiency, derived from recommendations in the adolescent sleep literature, e.g., 26,27 is operationalized as ≥ 85% average sleep efficiency in the 7-day sleep diary.
Duration.
Good sleep duration is operationalized as total sleep time (TST), averaged across the 7-day sleep diary, as 9–11 hours for 10–13 year-olds and 8–10 hours for 14–18 year-olds. These cutoffs are derived from recommendations in the literature 28,29 and values used in prior research 13.
Data Analysis
All analyses were completed in Stata 15. The Sleep Health Composite score was modeled as a continuous variable. Multiple regression analysis was used for Aims 2 and 3 for continuous outcomes (e.g., composite risk scores), logistic regression was used for binary outcomes (e.g., K-SADS variables, BMI categories), and negative binomial regression was used for count data (alcohol and substance use, modifiable activity questionnaire). Due to the significant developmental changes as well as documented sex differences during adolescents in terms of sleep, chronotype, and health, we adjusted for sex and age in all models. A significance level of 0.05 was used throughout.
Results
Aim 1.
Table 3 shows the descriptive statistics of the Sleep Health Composite in the current sample; higher scores indicate better sleep health. The average Sleep Health Composite was 3.66 at pre-treatment, suggesting that adolescents had good sleep health in fewer than 4 of the 6 dimensions. Duration and satisfaction were the dimensions most commonly rated as poor in this sample. Table 4 shows the most common poor sleep profiles in the current sample. Poor duration (while being good on other sleep health dimensions) was the most common poor sleep profile (15.4%).
Table 4.
Most Common Poor Sleep Health Profiles for One, Two, and Three “Poor” Sleep Dimensions.
| Most Common Poor Sleep Health Profiles | N | % |
|---|---|---|
| One “poor” sleep dimension | ||
| Duration | 27 | 15.40 |
| Satisfaction | 10 | 5.70 |
| Two “poor” sleep dimensions | ||
| Alertness + Duration | 8 | 4.60 |
| Satisfaction + Duration | 7 | 4.00 |
| Three “poor” sleep dimensions | ||
| Satisfaction + Alertness + Duration | 13 | 7.40 |
| Regularity + Satisfaction + Duration | 4 | 4.49 |
Aim 2.
Better sleep health, as indexed by a higher Sleep Health Composite, was associated with reduced risk in the emotional (b = −0.19, p < 0.001), cognitive (b = −0.13, p = 0.01), and social domains (b = −0.09, p = 0.04) (Table 5). The regression coefficients for behavioral (b = −0.07, p = 0.20) and physical domains (b = −0.08, p = 0.11) were in the expected direction, though not statistically significant. For specific measures under the five health domains, better sleep health was associated with lower depressive (b = −1.44, p = 0.01) and anxiety (b = −3.04, p = 0.003) symptoms, lower cognitive problems (b = −0.49, p = 0.003), fewer social problems related to friends (b = −0.62, p = 0.02) and family (b = −0.67, p = 0.001), and fewer physical symptoms (b = −0.76, p = 0.01). Better sleep health was associated with more social problems related to romantic relationship (b = 0.22, p = 0.04). Regression coefficients for the covariates (age and sex) in these models are reported in Supplemental Table S2.
Table 5.
Association between Sleep Health Composite and Primary Outcomes of the RCT Measured at Pre-treatment Baseline
| Sleep Health Composite (predictor) | b | SE | p | 95% CI |
|---|---|---|---|---|
| Youth Self-Report Composite Risk Score (outcome) | ||||
| Emotional domain* | −0.19 | 0.05 | <0.001 | −0.30, −0.09 |
| Children’s Depression Rating Scale | −1.44 | 0.55 | 0.01 | −2.52, −0.36 |
| Multidimensional Anxiety Scale for Children | −3.04 | 0.99 | 0.003 | −5.01, −1.08 |
| Cognitive domain* | −0.13 | 0.05 | 0.01 | −0.24, −0.03 |
| Attention Control Scale | 0.39 | 0.45 | 0.39 | −0.50, 1.29 |
| YSAS: school/cognitive | −0.49 | 0.16 | 0.003 | −0.81, −0.16 |
| Behavioral domain* | −0.07 | 0.05 | 0.20 | −0.17, 0.03 |
| Sensation Seeking Scale | −0.43 | 0.35 | 0.22 | −1.12, 0.26 |
| Alcohol and Substance Use | −0.12 | 0.07 | 0.08 | −0.25, 0.17 |
| Social domain* | −0.09 | 0.04 | 0.04 | −0.18, −0.01 |
| YSAS: friends | −0.62 | 0.27 | 0.02 | −1.17, −0.08 |
| YSAS: family | −0.67 | 0.20 | 0.001 | −1.07, −0.27 |
| YSAS: romantic | 0.22 | 0.10 | 0.04 | 0.01, 0.43 |
| Physical domain* | −0.08 | 0.05 | 0.11 | −0.17, 0.02 |
| Modifiable Activity Questionnaire | −0.04 | 0.09 | 0.63 | −0.21, 0.13 |
| Physical Health Questionnaire | −0.76 | 0.29 | 0.01 | −1.34, −0.19 |
Note. YSAS = Youth Social Adjustment Scale.
indicates composite scores derived by obtaining the mean of the standardized scores of all measures within each domain. Higher composite risk scores indicate greater risk in that health domain. All models controlled for age and sex. All variables, except for Attention Control Scale and Modifiable Activity Questionnaire, were coded such that higher score indicates greater risk/worse outcome. A value of 0 in the risk composite score indicates the average level of “risk” in that health domain in this sample.
Figure 1 presents the means of the five health composite risk scores in relation to Sleep Health Composite scores; participants with higher Sleep Health Composite score had lower health composite risk scores. Figure 2 illustrates the associations between sleep health and risk in the five health domains.
Fig. 1.
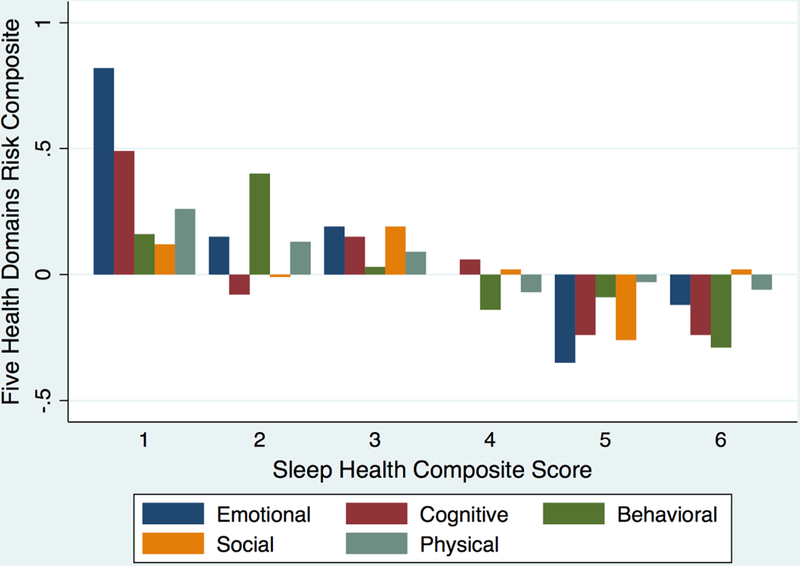
Means of the five health risk domains over the Sleep Health Composite Score. Positive and larger values for the 5 health risk domains composite scores indicate greater risk; negative and smaller values indicate lower risk. Sleep Health Composite Score = 0 was not plotted because there were only 3 observations.
Fig. 2.
Negative associations between Sleep Health Composite and 5 health risk domains. Graphs show fitted regression lines with 95% confidence intervals. Higher Sleep Health Composite Score indicates better sleep health. Positive and larger health risk composite score indicates greater risk in that domain; negative and smaller health risk composite score indicates lower risk in that domain.
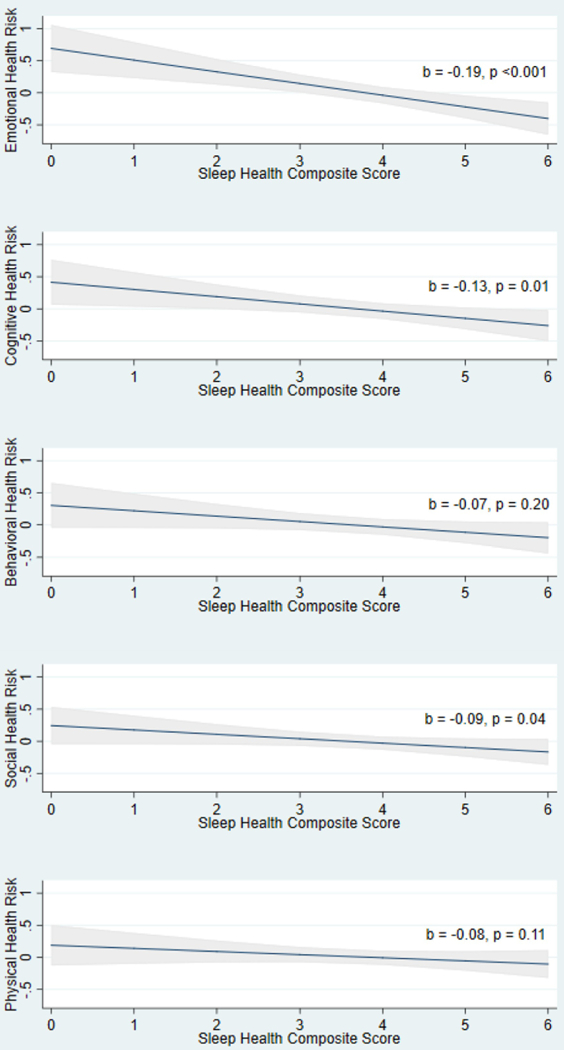
Note. Graphs showing fitted regression lines with 95% CIs. Higher Sleep Health Composite Score indicates better sleep health. Positive and larger health risk composite score indicates greater risk in that domain; nagative and smaller health risk composite score indicates lower risk in that domain
Aim 3.
Table 3 presents the descriptive statistics for BMI, past year medical problems, and K-SADS psychiatric disorder diagnostic categories (mood, anxiety, and behavior disorders). As presented in Table 6, better sleep health, as indexed by a higher Sleep Health Composite score, was significantly associated with decreased odds for obesity (OR = 0.60, p = 0.03), but was not associated with overweight, underweight, normal weight, or continuous BMI. Sleep health was not associated with any past year medical problem (diabetes, infections, hypertension, high cholesterol, and injury/accidents) per parent-report.
Table 6.
Association between Sleep Health Composite and Psychiatric and Medical Conditions
| Sleep Health Composite | b | SE | p | 95% CI |
|---|---|---|---|---|
| BMI (continuous) | −0.51 | 0.26 | 0.05 | −1.03, 0.01 |
| OR | SE | p | 95% CI | |
| Obese (BMI ≥30) | 0.60 | 0.14 | 0.03 | 0.37, 0.96 |
| Overweight (BMI ≥25) | 0.97 | 0.15 | 0.87 | 0.72, 1.32 |
| Underweight (BMI < 18.5) | 1.15 | 0.18 | 0.37 | 0.85, 1.55 |
| Normal weight (BMI 18.5–24.99) | 1.02 | 0.12 | 0.89 | 0.81, 1.27 |
| Medical problem (past year) | 1.15 | 0.16 | 0.33 | 0.87, 1.51 |
| K-SADS diagnostic classes | ||||
| Any current mood disorder (T) | 0.65 | 0.14 | 0.04 | 0.43, 0.98 |
| Any current mood disorder (P) | 0.93 | 0.19 | 0.71 | 0.62, 1.38 |
| Any current anxiety disorder (T) | 0.63 | 0.09 | 0.002 | 0.47, 0.84 |
| Any current anxiety disorder (P) | 0.98 | 0.17 | 0.89 | 0.69, 1.38 |
| Any current behavior disorder (T) | 0.76 | 0.14 | 0.14 | 0.61, 1.30 |
| Any current behavior disorder (P) | 1.07 | 0.22 | 0.74 | 0.65, 1.47 |
Note. All models controlled for sex and age. BMI was adjusted for age and sex. Medical problem = presence of any following medical conditions in the past year per parent-report: diabetes, infections, hypertension, high cholesterol, and injury/accidents. T = teenager interview. P = parent interview. Current episode includes those that were probable, in partial remission, and definite. Any current mood disorder includes major depressive disorder, dysthymia, bipolar I, bipolar II, bipolar not otherwise specified. Any current anxiety disorder includes agoraphobia, generalized anxiety disorder, social phobia, specific phobia, panic disorder, post-traumatic stress disorder, and acute stress disorder. Any current behavior disorder includes attention deficit hyperactivity disorder, oppositional defiant disorder, conduct disorder, and substance use disorders (alcohol abuse/dependence and drug abuse dependence).
Better sleep health was significantly associated with reduced odds of having any current mood disorder (OR = 0.65, p = 0.04) and any current anxiety disorders (OR = 0.63, p = 0.002) per teenager interview. Better sleep health was not associated with any current behavior disorder per teenager interview or any K-SADS diagnostic classes per parent interview. Regression coefficients for the covariates (age and sex) in these models are reported in Supplemental Table S2.
Additional Analyses.
We conducted sensitivity analyses to examine whether applying different cut-offs for the Sleep Health Composite would change the results. Supplemental Tables S3 and S4 present these cut-offs and the distributions of resulting Sleep Health Composite scores. We repeated the analyses conducted for Aims 2 and 3 using the alternative Sleep Health Composite, and found similar results (Supplemental Table S5), supporting the conclusion that the Sleep Health Composite is associated with mental and physical outcomes.
We also conducted additional analyses examining the associations between single dimensions of sleep health and mental/physical outcomes. Due to the relatively large number of sleep health dimensions and outcomes, we examined only composite risk scores in the five health domains that were significantly related to the Sleep Health Composite (i.e., K-SADS diagnostic categories and obesity). Supplemental Table S6 suggests that the Sleep Health Composite was more consistently associated with outcomes of interest than single dimensions.
Discussion
The current study presents the preliminary derivation of a Sleep Health Composite based on the sleep health framework 5 and examined whether the Sleep Health Composite was concurrently associated with functioning in sleep, circadian, physical and mental health domains in a sample of adolescents who exhibited late bedtime, evening circadian chronotype, and were at risk in at least one of five health domains. This Sleep Health Composite was associated with elevated risk in multiple health domains in adolescents with eveningness chronotype.
Most participants scored “good” on only 3 or 4 sleep health dimensions. Sleep duration and sleep satisfaction were most frequently rated as “poor,” but no single problem, or combination of problems, accounted for large percentages of the poor sleep health profiles. This heterogeneity suggests a strength of the multidimensional Sleep Health Composite approach. We found a paucity of literature on what constitutes “good” sleep health for adolescents, particularly for the regularity and timing dimensions. We consulted the distributions of these dimensions in normative adolescent samples, but such samples are unlikely to constitute an ideal index of optimal adolescent health. Given the prevalence of eveningness in adolescents, future research should examine specific parameters that define good sleep health in this population.
As predicted, better Sleep Health Composite scores were associated with less risk in the emotional, cognitive, and social health domains. Similar, but statistically nonsignificant, trends were observed in behavioral and physical health domains. Additionally, better sleep health was associated with reduced odds of obesity and having any current mood or anxiety disorder per clinical interview with the adolescent These results are consistent with prior research suggesting associations between individual sleep health dimensions and health domains, including physical health such as obesity 9 and general health, 30,31 as well as mental health such as depression and anxiety.32,33 Two other recent studies have examined the association between multivariate measures of sleep based on the sleep health framework in the context of depression 6 and mortality 7 among large, older adult populations. Together, these results provide additional evidence for the sleep health framework.
Some of the observed relationships have uncertain significance. For instance, better sleep health was associated with more problems in romantic relationships. In addition, although we found that higher Sleep Health Composite was associated with fewer self-reported physical symptoms, we did not find a relationship between the Sleep Health Composite and relevant past year medical problems. This lack of association could be attributed to measurement problems such as low base rates of these disorders, or to the use of retrospective parent reports.
The current analyses have several limitations. First, the sample was not a representative sample of community-dwelling, healthy adolescents. As such, results cannot be generalized to healthy adolescents, other age groups (e.g., adults), or to clinical populations such as those with other sleep disorders (e.g., obstructive sleep apnea). However, the unique features of the current sample may serve as a first step to gauge the potential utility of the Sleep Health Composite. A more thorough psychometric study should evaluate the reliability and validity indices of the Sleep Health Composite score using large representative samples of healthy adolescents as well as other clinical and non-clinical samples. Second, the sleep health framework was not proposed specifically for adolescents. It is possible that the dimensions most important for sleep health in adolescents may be different from adults. A related limitation is that in the current study each dimension was given equal weight in the construction of the Sleep Health Composite score. Different dimensions may warrant different weights in adolescent or adult samples, or other specific populations. Third, the construction of the six sleep health dimensions relied on sleep diary and self-report rating scales. Future studies should employ objective measures of sleep such as actigraphy, as was done in Wallace et al. (2017). Nevertheless, sleep diary is considered the gold standard for measuring subjective sleep and is widely used in clinical practice, 4,14 presumably making the derivation of Sleep Health Composite more deployable in clinical settings.
The current study only provides a proof-of-concept example of the utility of a Sleep Health Composite using the baseline data of an intervention study. Future research may consider using a similar approach as offered here to derive a Sleep Health Composite in other populations and contexts. Additional methods include using the simple self-report scale “RU SATED,” which is designed to assess the construct of sleep health.5 The current study focused on the linear relationship between the Sleep Health Composite score and health outcomes. Future research should examine the contribution of each sleep health dimension on health outcomes and test for both linear and non-linear effects between specific dimensions of sleep health and health outcomes. Future research should also examine potential age effects on the multidimensional construct of sleep health, both within adolescence and across even broader age ranges. Finally, we tested cut-offs values for each sleep health dimension that were based on values and recommendations from previously-published literature. However, other strategies, such as receiver operating characteristic analyses, could be used to empirically define these cut-points in subsequent, larger studies.
To summarize, the current study documents a process for constructing a Sleep Health Composite in a sample of community-residing adolescents with evening circadian chronotype and at risk in one of the five health domains. The derivation of a multidimensional Sleep Health Composite has potential research and clinical application as an outcome measure in treatment studies of sleep and circadian problems. Finally, these results support sleep health as an important correlate of physical and mental health in adolescents.
Supplementary Material
Acknowledgment
We are grateful to National Institute of Child Health and Human Development (R01HD071065) for funding this research, the families who participated in this study, and to the team for their assistance with project set-up, project coordination, conducting assessments and providing treatment. We also thank Michael Dolsen, Nicole B. Gumport, Caitlin E. Gasperetti, Courtney C. Armstrong, and Garret Z. Zieve for helpful discussion on this paper.
This research was supported by National Institute of Child Health and Human Development R01HD071065.
Appendix
Inclusion criteria operationalizing ‘at risk’ for the five health domains from 10
| Risk Domain | Criteria for Inclusion |
|---|---|
| Emotional | ≥ 4 on any of the following items on the CDRS: Difficulty Having Fun, Social Withdrawal, Irritability, Depressed Feelings, Excessive Weeping, or a T-score of 61 or above on the MASC-10, based on age group (10–11 years, 12–15 year, 16–19 years) using the MASC-10 Profile. |
| Behavioral | An SSS score greater than 3.93 for males aged 10–13, greater than 3.19 for females aged 10–13, greater than 4.07 for males aged 14–18, or greater than 3.19 for females aged 14–18 or taking ADHD medication or the K-SADS indicating a diagnosis of ADHD or current alcohol or substance abuse assessed with the K-SADS. |
| Social | A parent rating their child as “worse” than others the participants age on one or more of the social behavior items (Section VI) from the CBCL. |
| Cognitive | A parent rating their child as “failing” in one or more academic class from CBCL Section VII. |
| Physical | A score of 4 or above on the PHQ-15, six or more days of school absences, or a BMI above the 85th percentile for the participant’s sex and age. |
Note. CDRS = Child Depression Rating Scale 34, the cutoff is commensurate with “clinical symptoms.” MASC-10 = Multidimensional Anxiety Scale for Children, the cutoff T-score was selected to capture the ‘slightly elevated’ through to the ‘very elevated’ range 35. SSS = Sensation Seeking Scale 36, the cutoff corresponds to at or above one standard deviation over the normative average 37. K-SADS = Schedule for Affective Disorders and Schizophrenia for School-Age Children 19. CBCL = Child Behavior Checklist 38, which asks the parent if their child does “worse”, “average”, or “better” than other teens their age or if the teen is “failing”, “below average”, “ average” or “above average.” PHQ-15 = Physical Health Questionnaire-15, the cutoff corresponds to ‘minimal somatic symptom severity’ through to the ‘high somatic symptom severity’ range 39. BMI = Body Mass Index, the cutoff corresponds to 1 standard deviation above the mean.
Footnotes
Publisher's Disclaimer: This is a PDF file of an unedited manuscript that has been accepted for publication. As a service to our customers we are providing this early version of the manuscript. The manuscript will undergo copyediting, typesetting, and review of the resulting proof before it is published in its final citable form. Please note that during the production process errors may be discovered which could affect the content, and all legal disclaimers that apply to the journal pertain.
Disclosure Statement
Dr. Buysse has served as a paid consultant to BeHealth Solutions and Emmi Solutions, and participated in a CME program sponsored by CME Institute. The other authors declared no conflicts of interest.
References
- 1.Kamath J, Virdi S, Winokur A. Sleep Disturbances in Schizophrenia. Psychiatr Clin North Am 2015;38(4):777–792. doi: 10.1016/j.psc.2015.07.007. [DOI] [PubMed] [Google Scholar]
- 2.Harvey AG. Sleep and circadian functioning: Critical mechanisms in the mood disorders? Annu Rev Clin Psychol 2011;7:297–319. doi: 10.1146/annurev-clinpsy-032210-104550. [DOI] [PubMed] [Google Scholar]
- 3.Gillette MU. Progress in Molecular Biology and Translational Science. Volume One Hundred and Nineteen, Chronobiology: Biological Timing in Health and Disease Elsevier Inc.; 2013. [DOI] [PubMed] [Google Scholar]
- 4.Buysse DJ, Ancoli-Israel S, Edinger JD, Lichstein KL, Morin CM. Recommendations for a standard research assessment of insomnia. Sleep 2006;29(9):1155–1173. [DOI] [PubMed] [Google Scholar]
- 5.Buysse DJ. Sleep Health: Can We Define It? Does It Matter? Sleep 2014;37(1):9–17. doi: 10.5665/sleep.3298. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Furihata R, Hall MH, Stone KL, et al. An Aggregate Measure of Sleep Health Is Associated With Prevalent and Incident Clinically Significant Depression Symptoms Among Community-Dwelling Older Women. Sleep 2017;40(3). doi: 10.1093/sleep/zsw075. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Wallace ML, Stone K, Smagula SF, et al. Which Sleep Health Characteristics Predict All-Cause Mortality in Older Men? An Application of Flexible Multivariable Approaches. Sleep 2018;41(1). doi: 10.1093/sleep/zsx189. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Harvey AG, Buysse DJ. Treating Sleep Problems: A Transdiagnostic Approach New York, NY: The Guilford Press; 2017. [Google Scholar]
- 9.Asarnow LD, McGlinchey E, Harvey AG. Evidence for a Possible Link between Bedtime and Change in Body Mass Index. Sleep 2015:1523–1527. http://www.ncbi.nlm.nih.gov/pubmed/26194568. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Harvey AG, Hein K, Dolsen M, et al. Modifying the Impact of Eveningness Chronotype (‘Night-Owls’) in Youth: A Randomized Controlled Trial. J Am Acad Child Adolesc Psychiatry August 2018. doi: 10.1016/j.jaac.2018.04.020. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Dagys N, McGlinchey EL, Talbot LS, Kaplan KA, Dahl RE, Harvey AG. Double trouble? The effects of sleep deprivation and chronotype on adolescent affect. J Child Psychol Psychiatry Allied Discip 2012;53(6):660–667. doi: 10.1111/j.1469-7610.2011.02502.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Giannotti F, Cortesi F, Sebastiani T, Ottaviano S. Circadian preference, sleep and daytime behaviour in adolescence. J Sleep Res 2002;11(3):191–199. doi: 10.1046/j.1365-2869.2002.00302.x. [DOI] [PubMed] [Google Scholar]
- 13.Maslowsky J, Ozer EJ. Developmental trends in sleep duration in adolescence and young adulthood: Evidence from a national United States sample. J Adolesc Heal 2014;54(6):691–697. doi: 10.1016/j.jadohealth.2013.10.201. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Carney CE, Buysse DJ, Ancoli-Israel S, et al. The Consensus Sleep Diary: Standardizing Prospective Sleep Self-Monitoring. Sleep 2012;35(2):287–302. doi: 10.5665/sleep.1642. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Buysse DJ, Reynolds CF, Monk TH, et al. The Pittsburgh Sleep Quality Index: a new instrument for psychiatric practice and research. Psychiatry Res 1989;28(2):193–213. doi: 10.1016/0165-1781(89)90047-4. [DOI] [PubMed] [Google Scholar]
- 16.Wolfson AR, Carskadon MA. Sleep Schedules and Daytime Functioning in Adolescents. Child Dev 1998;69(4):875–887. doi: 10.1111/j.1467-8624.1998.tb06149.x. [DOI] [PubMed] [Google Scholar]
- 17.Carskadon MA, Vieira C, Acebo C. Association between puberty and delayed phase preference. Sleep 1993;16(3):258–262. http://www.ncbi.nlm.nih.gov/pubmed/8506460. [DOI] [PubMed] [Google Scholar]
- 18.Song M, Lin F, Ward SE, Fine JP. Composite Variables. Nurs Res 2013;62(1):45–49. doi: 10.1097/NNR.0b013e3182741948. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Kaufman J, Birmaher B, Brent D, et al. Schedule for Affective Disorders and Schizophrenia for School-Age Children-Present and Lifetime Version (K-SADS-PL): initial reliability and validity data. J Am Acad Child Adolesc Psychiatry 1997;36(7):980–988. doi: 10.1097/00004583-199707000-00021. [DOI] [PubMed] [Google Scholar]
- 20.Merikangas KR, He J, Burstein M, et al. Lifetime Prevalence of Mental Disorders in U.S. Adolescents: Results from the National Comorbidity Survey Replication–Adolescent Supplement (NCS-A). J Am Acad Child Adolesc Psychiatry 2010;49(10):980–989. doi: 10.1016/j.jaac.2010.05.017. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Kuczmarski RJ, Ogden CL, Guo SS, et al. 2000 CDC Growth Charts for the United States: Methods and Development Vol 11; 2002. doi:12043359. [PubMed] [Google Scholar]
- 22.Evans GW, Li D, Whipple SS. Cumulative Risk and Child Development. Psychol Bull 2013;139(6):1342–1396. doi: 10.1037/a0031808. [DOI] [PubMed] [Google Scholar]
- 23.Crowley SJ, Acebo C, Carskadon MA. Sleep, circadian rhythms, and delayed phase in adolescence. Sleep Med 2007;8(6):602–612. doi: 10.1016/j.sleep.2006.12.002. [DOI] [PubMed] [Google Scholar]
- 24.Bei B, Manber R, Allen NB, Trinder J, Wiley JF. Too long, too short, or too variable? Sleep intraindividual variability and its associations with perceived sleep quality and mood in adolescents during naturalistically unconstrained sleep. Sleep 2016;5(2). doi: 10.1093/sleep/zsw067. [DOI] [PubMed] [Google Scholar]
- 25.Gradisar M, Wolfson AR, Harvey AG, Hale L, Rosenberg R, Czeisler CA. The sleep and technology use of Americans: Findings from the National Sleep Foundation’s 2011 sleep in America poll. J Clin Sleep Med 2013;9(12):1291–1299. doi: 10.5664/jcsm.3272. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Hysing M, Pallesen S, Stormark KM, Lundervold AJ, Sivertsen B. Sleep patterns and insomnia among adolescents: A population-based study. J Sleep Res 2013;22(5):549–556. doi: 10.1111/jsr.12055. [DOI] [PubMed] [Google Scholar]
- 27.Lovato N, Gradisar M, Short M, Dohnt H, Micic G. Delayed Sleep Phase Disorder in an Australian School-Based Sample of Adolescents. J Clin Sleep Med 2013;9(9):939–944. doi: 10.5664/jcsm.2998. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Hirshkowitz M, Whiton K, Albert SM, et al. National Sleep Foundation’s updated sleep duration recommendations: Final report. Sleep Heal 2015;1(4):233–243. doi: 10.1016/j.sleh.2015.10.004. [DOI] [PubMed] [Google Scholar]
- 29.Paruthi S, Brooks LJ, D’Ambrosio C, et al. Consensus Statement of the American Academy of Sleep Medicine on the Recommended Amount of Sleep for Healthy Children: Methodology and Discussion. J Clin Sleep Med 2016;12(11):1549–1561. doi: 10.5664/jcsm.6288. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Knutson KL, Turek FW. The U-shaped association between sleep and health: the 2 peaks do not mean the same thing. Sleep 2006;29(7):878–879. [DOI] [PubMed] [Google Scholar]
- 31.Fabbian F, Zucchi B, De Giorgi A, et al. Chronotype, gender and general health. Chronobiol Int 2016;33(7):863–882. doi: 10.1080/07420528.2016.1176927. [DOI] [PubMed] [Google Scholar]
- 32.Baglioni C, Battagliese G, Feige B, et al. Insomnia as a predictor of depression: A meta-analytic evaluation of longitudinal epidemiological studies. J Affect Disord 2011;135(1–3):10–19. doi: 10.1016/j.jad.2011.01.011. [DOI] [PubMed] [Google Scholar]
- 33.Cox RC, Olatunji BO. A systematic review of sleep disturbance in anxiety and related disorders. J Anxiety Disord 2016;37:104–129. doi: 10.1016/j.janxdis.2015.12.001. [DOI] [PubMed] [Google Scholar]
- 34.Poznanski EO, Grossman JA, Buchsbaum Y, Banegas M, Freeman L, Gibbons R. Preliminary studies of the reliability and validity of the children’s depression rating scale. J Am Acad Child Psychiatry 1984;23(2):191–197. doi: 10.1097/00004583-198403000-00011. [DOI] [PubMed] [Google Scholar]
- 35.March JS, Sullivan K, Parker J. Test-Retest Reliability of the Multidimensional Anxiety Scale for Children. J Anxiety Disord 1999;13(4):349–358. doi: 10.1016/S0887-6185(99)00009-2. [DOI] [PubMed] [Google Scholar]
- 36.Russo MF, Stokes GS, Lahey BB, et al. A sensation seeking scale for children: Further refinement and psychometric development. J Psychopathol Behav Assess 1993;15(2):69–86. doi: 10.1007/BF00960609. [DOI] [Google Scholar]
- 37.Stephenson MT, Hoyle RH, Palmgreen P, Slater MD. Brief measures of sensation seeking for screening and large-scale surveys. Drug Alcohol Depend 2003;72(3):279–286. doi: 10.1016/j.drugalcdep.2003.08.003. [DOI] [PubMed] [Google Scholar]
- 38.Becker SP, Ramsey RR, Byars KC. Convergent validity of the Child Behavior Checklist sleep items with validated sleep measures and sleep disorder diagnoses in children and adolescents referred to a sleep disorders center. Sleep Med 2015;16(1):79–86. doi: 10.1016/j.sleep.2014.09.008. [DOI] [PubMed] [Google Scholar]
- 39.Kroenke K, Spitzer RL, Williams JBW. The PHQ-15: validity of a new measure for evaluating the severity of somatic symptoms. Psychosom Med 2002;64(2):258–266. doi: 10.1097/00006842-200203000-00008. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.