

Abstract
We reviewed technical parameters, acquisition protocols and adverse reactions (ARs) for contrast-enhanced spectral mammography (CESM). A systematic search in databases, including MEDLINE/EMBASE, was performed to extract publication year, country of origin, study design; patients; mammography unit/vendor, radiation dose, low-/high-energy tube voltage; contrast molecule, concentration and dose; injection modality, ARs and acquisition delay; order of views; examination time. Of 120 retrieved articles, 84 were included from 22 countries (September 2003–January 2019), totalling 14012 patients. Design was prospective in 44/84 studies (52%); in 70/84 articles (83%), a General Electric unit with factory-set kVp was used. Per-view average glandular dose, reported in 12/84 studies (14%), ranged 0.43–2.65 mGy. Contrast type/concentration was reported in 79/84 studies (94%), with Iohexol 350 mgI/mL mostly used (25/79, 32%), dose and flow rate in 72/84 (86%), with 1.5 mL/kg dose at 3 mL/s in 62/72 studies (86%). Injection was described in 69/84 articles (82%), automated in 59/69 (85%), manual in 10/69 (15%) and flush in 35/84 (42%), with 10–30 mL dose in 19/35 (54%). An examination time < 10 min was reported in 65/84 studies (77%), 120 s acquisition delay in 65/84 (77%) and order of views in 42/84 (50%) studies, beginning with the craniocaudal view of the non-suspected breast in 7/42 (17%). Thirty ARs were reported by 14/84 (17%) studies (26 mild, 3 moderate, 1 severe non-fatal) with a pooled rate of 0.82% (fixed-effect model). Only half of CESM studies were prospective; factory-set kVp, contrast 1.5 mL/kg at 3 mL/s and 120 s acquisition delay were mostly used; only 1 severe AR was reported. CESM protocol standardisation is advisable.
Keywords: Breast, Contrast media, Drug-related side effects and adverse reactions, Mammography, Radiation dosage
Key points
Eighty-four articles on CESM totalling 14012 patients were reviewed
A 1.5 mL/kg contrast dose automatically injected at 3 mL/s was generally adopted
Per-view average glandular dose ranged from 0.43 to 2.65 mGy
Studies for contrast agent dose-finding and view acquisition ordering are lacking
Adverse reaction rate (only one severe) was similar to that reported for CT
Background
During the 1960s and 1970s, randomised controlled trials proved that screen-film mammography for breast cancer screening yields a reduction in breast cancer mortality [1]. Since the early 2000s, screen-film mammography was progressively replaced by digital mammography (DM), which improved performance especially in women under 50 years of age and in case of dense breasts, even though providing an intrinsically inferior spatial resolution [2]. In the last two decades, digital breast tomosynthesis brought substantial further improvements [3, 4], increasing cancer detection rate and reducing the recall rate [5].
Contrast-enhanced mammography is the combination of X-ray mammography with intravenous administration of iodinated contrast agent (ICA) [6]. It was first attempted using a digital subtraction technique [7–9], but this approach was soon abandoned due to difficulties in co-registration of unenhanced and contrast-enhanced images [10, 11]. In the last two decades, contrast-enhanced spectral mammography (CESM) has been introduced, based on dual-energy breast exposure (about 26–33 kVp and 44–50 kVp) after contrast administration, so that the pre-contrast exposure was no longer needed [10, 12]. CESM allows for the visualisation of enhancing findings over the normal unenhancing breast tissue, exploiting the increased contrast uptake of malignancies [6, 10, 13].
Original studies have investigated the use of CESM in a number of settings, such as evaluation of symptomatic women [14–17], screening recalls [18–22], local staging [23–32], pre- and post-operative evaluations [23, 24, 33–36] and neoadjuvant chemotherapy response monitoring [37–40]. In 2016, a first meta-analysis on CESM described a high pooled sensitivity (98%) albeit with a relatively low specificity (58%) [41], the latter partly caused by inexperience. A more recent meta-analysis [42] reported globally satisfying data for CESM-pooled sensitivity (89%) and specificity (84%), proposing it as an alternative to contrast-enhanced magnetic resonance imaging (MRI) and even suggesting CESM as a “useful triage test for initial breast lesions assessment” [41].
A time delay between the first appearance of new imaging techniques and their implementation in diagnostic routine is expected for many reasons, including not only the definition of indications but also the reproducibility of results. The latter is strongly influenced by technique details, such as contrast agent concentration, dose and injection rate, breast compression and positioning, exposure parameters and acquisition protocol. Indeed, the fact that CESM is variably performed across different centres, without an agreed and standardised technique, does not come as a surprise: this circumstance echoes the one observed for contrast-enhanced breast MRI in the 1990s, now settled by the publication of detailed international guidelines [43–46].
Therefore, the aim of this work was to review CESM studies focusing on adopted technique, contrast agent issues and acquisition workflow. This effort is crucial for future CESM investigations to be reproducible and comparable.
Methods
Study protocol
No ethics committee approval was needed for this systematic review. The study protocol was registered on PROSPERO (protocol CRD42018118554), the international prospective register of systematic reviews [47]. This systematic review was reported according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) statement [48].
Search strategy and eligibility criteria
In February 2019, a systematic search was performed on MEDLINE (PubMed, https://www.ncbi.nlm.nih.gov/pubmed/), EMBASE (Elsevier), the Cochrane Library (Cochrane Database of Systematic Reviews) and the Cochrane Central Register of Controlled Trials for articles that reported or may have reported CESM technique. A controlled vocabulary (medical subject headings in PubMed and EMBASE thesaurus keywords in EMBASE) was used. The search string was (cesm OR ‘contrast enhanced spectral mammography’/exp. OR ‘dual energy mammography’ OR ‘contrast enhanced digital mammography’/exp. OR ‘contrast-enhanced mammography’ OR ‘dual-energy subtraction mammography’ OR cedm OR cedsm OR ‘contrast enhanced spectral imaging’ OR ‘high energy and low energy digital mammography’) AND (‘procedures’/exp. OR ‘method’ OR ‘methods’ OR ‘procedure’ OR ‘procedures’ OR ‘technique’ OR ‘acquisition’/exp. OR ‘contrast medium’/exp. OR ‘contrast agent’ OR ‘contrast dye’ OR ‘contrast material’ OR ‘contrast media’ OR ‘contrast medium’ OR ‘radiocontrast medium’ OR ‘radiography contrast medium’ OR ‘roentgen contrast medium’ OR ‘image processing’/exp. OR ‘image processing’ OR ‘image processing, computer-assisted’ OR ‘processing, image’).
The search was limited to original studies on humans published in English, French and Spanish on peer-reviewed journals, with an available abstract. No publication date limits were applied. First article screening was performed by two independent readers (A.C. and M.Z., with 1- and 3-year experience in breast imaging, respectively) considering only title and abstract. Eligible articles were those that reported in the title or in the abstract the use of CESM technique or that could have contained these data in the manuscript. After downloading eligible articles, the full text was read for a complete assessment. Finally, references of included articles were hand-searched to check for further eligible studies.
Data extraction
Data extraction was performed independently by the same two readers who performed the literature search. Disagreements were settled by consensus. For each analysed article, year of publication, institution (such as hospitals, imaging facilities, breast units including radiology sections or any other type of centre in which CESM is performed) and country origin as well as research groups, design, number of patients and demographics were retrieved. Mammography unit, vendor, radiation dose and technical features such as low- and high-energy peak kilovoltage (kVp), anode/filter combinations and exposure parameters were also extracted. Moreover, contrast agent type, dose and concentration were retrieved, as well as injection modality, if manual or automated, flow rate and additional post-contrast saline flush or “bolus chaser” if present. Furthermore, mild, moderate or severe adverse reactions to ICAs were extracted alongside strategies for their prevention. Regarding the acquisition protocol, time between contrast injection and first image acquisition and maximum examination duration were extracted. Regarding the order of views, we reported the acquisition sequence of the standard mammographic projections considering the craniocaudal (CC) and the mediolateral oblique (MLO) views, including the first side acquired. Missing data were requested to authors.
Evidence synthesis
To avoid risk of data duplication bias, in case of articles published by the same research group, we considered the possibility of performing subgroup analysis: therefore, before delving into further analysis of protocol description, we chose to change our viewpoint from the number of articles reporting a specific protocol to the minimum number of times a protocol was reported by a single research group.
Regarding the pooled rate of adverse reactions related to ICA administration across studies, statistical analysis was performed using Comprehensive Meta-Analysis v2.2.057 (Biostat, Englewood, NJ, USA) using the meta-analysis model “Number of events and study population”. I2 statistics was first calculated to assess heterogeneity and the fixed-effect model was used to provide the rate of adverse reactions and 95% of confidence intervals (CI). The risk of publication bias was assessed by visually inspecting funnel plot and performing the Egger test [49].
Results
Studies
A flowchart of study selection is shown in Fig. 1. Of 120 retrieved articles, 84 (70%), published between September 2003 and January 2019, were analysed [7–10, 13–40, 50–101]; 40/84 (48%) being retrospective and 44/84 (52%) prospective (43/44 monocentric (98%) and 1/44 multicentric (2%); 54/84 (64%) articles investigated CESM diagnostic performance, whereas 30/84 (36%) focused on technical features. The geographic distribution of research groups is depicted in Fig. 2.
Fig. 1.

Flowchart of the study selection and exclusion for articles on contrast-enhanced spectral mammography
Fig. 2.

Geographic distribution of research groups which published results of clinical applications of contrast-enhanced spectral mammography. From very light blue to dark blue, the number of groups progressively increases from 1 to 7; grey colour means no publications
Populations and settings
Data synthesis is reported in Table 1. The number of patients ranged from 5 [63] to 2303 [13], for a total of 14,012 patients, with mean or median age ranging from 45 years [40] to 66 years [23]. In 29/84 studies (35%), CESM was performed on patients from comprehensive databases of heterogeneous settings, such as pre- or post-operative evaluation, adjuvant or neoadjuvant chemotherapy response monitoring and equivocal findings at conventional imaging. The remaining 55 studies (65%) were individually centred on a unique setting. Twenty-seven studies (32%) performed CESM on suspicious cases from conventional imaging and screening recalls, 11 studies (13%) in a first-line screening setting, 7 (8%) performed CESM exclusively for known cancer staging, 4 (5%) in a pre-operative setting, 4 (5%) to assess and monitor the response to adjuvant chemotherapy and 2 (2%) in a post-operative setting.
Table 1.
Main characteristics of the 84 analysed studies
| Author/year | Ref. | Study design | Country of research group | Number of patients | Mean or median age (years) | Contrast agent type | Concentration (mgI/mL) | Dose (mL/kg) | Flow rate (mL/s) | Delay after injection (s) | Total exam time |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Houben 2019 | [22] | R | The Netherlands | 147 | 61 | Iopromide | 300 | 1.5 | 3 | 120 | |
| Barra 2018 | [40] | P mono | Brazil | 33 | 45 | Iohexol | 300 | 1.5 | 3 | 120 | B |
| Bicchierai 2018 | [93] | R | Italy | 40 | 50 | Iopromide | 370 | 1.5 | 3 | 120 | B |
| Danala 2018 | [69] | R | USA | 111 | Iohexol | 350 | 1.5 | 3 | 120 | B | |
| Deng 2018 | [78] | R | Taiwan | 141 | 48 | Iohexol | 350 | 1.5 | 3 | 120 | B |
| Helal 2018 | [25] | P mono | Egypt | 300 | 54 | Iohexol | 300 | 1.5 | 3 | 120 | B |
| Kim 2018 | [87] | P mono | South Korea | 84 | 51 | Iohexol | 350 | 1.5 | 2 | 120 | B |
| Klang 2018 | [88] | R | Israel | 953 | 51 | Iopamidol | 370 | 1.5 | 3 | 120 | B |
| Łuczyńska 2018 | [36] | R | Poland | 82 | 57 | Iopromide | 370 | 1.5 | 3 | 120 | B |
| Moustafa 2018 | [17] | P mono | Egypt | 160 | Iohexol | 300 | 1.5 | 3 | 120 | B | |
| Navarro 2018 | [90] | P mono | Chile | 465 | 53 | Ioversol | 320 | 1.5 | B | ||
| Patel 2018 (01) | [38] | P mono | USA | 65 | 53 | Iohexol | 350 | 1.5 | 3 | 120 | A |
| Patel 2018 (02) | [34] | R | USA | 50 | 57 | Iohexol | 350 | 1.5 | 3 | 120 | B |
| Patel 2018 (03) | [23] | R | USA | 30 | 66 | Iohexol | 350 | 1.5 | 3 | 120 | B |
| Phillips 2018 | [82] | R | USA | 45 | 53 | Iohexol | 350 | 1.5 | 3 | 120 | |
| Sorin 2018 | [92] | R | Israel | 611 | 54 | Iopamidol | 370 | 1.5 | 3 | 120 | B |
| Tohamey 2018 | [51] | P mono | Egypt | 178 | 46 | Iohexol | 300 | 1.5 | 3 | 120 | B |
| Travieso-Aja 2018 | [24] | R | Spain | 158 | 51 | 1.5 | 3 | 120 | B | ||
| Xing 2018 | [84] | P mono | China | 235 | 51 | Iohexol | 350 | 1.5 | 3 | 120 | B |
| Barra 2017 | [39] | R | Brazil | 11 | 46 | Iohexol | 300 | 1–2 | 3 | 120 | B |
| Bhimani 2017 | [13] | R | USA | 2303 | Iopamidol | 370 | 1.5 | 2 | 120 | B | |
| Fallenberg 2017 | [76] | P multi | Germany | 155 | 53 | Iobitridol | 300 | 1.5 | 3 | 120 | A |
| Gluskin 2017 | [63] | R | USA | 5 | 59 | Iohexol | 350 | 1.5 | 3 | 150–180 | A |
| Helal 2017 (01) | [28] | P mono | Egypt | 98 | 50 | Iohexol | 300 | 1.5 | 3 | 120 | B |
| Helal 2017 (02) | [99] | P mono | Egypt | 30 | 47 | Iohexol | 300 | 1.5 | 120 | ||
| Houben 2017 | [58] | R | The Netherlands | 839 | 60 | Iopromide | 300 | 1.5 | 3 | 120 | |
| Iotti 2017 | [37] | P mono | Italy | 54 | 54 | Ioversol | 350 | 1.5 | 120 | ||
| James 2017 | [56] | R | USA | 173 | Iohexol | 350 | 1.5 | 3 | 120 | A | |
| Jochelson 2017 | [54] | P mono | USA | 309 | 51 | Iohexol | 350 | 1.5 | 3 | 150–180 | B |
| Knogler 2017 | [94] | P mono | Austria | 11 | 58 | Iomeprol | 400 | 2 | 3.5 | 90 | |
| Lee-Felker 2017 | [26] | R | USA | 52 | 50 | Iohexol | 350 | 3 | 120 | B | |
| Lewis 2017 | [16] | R | USA | 208 | Iohexol | 350 | 1.5 | 3 | 120 | B | |
| Li 2017 | [100] | R | USA | 48 | 56 | Iopamidol | 370 | 1.5 | 1.5–2 | B | |
| Mori 2017 | [74] | P mono | Japan | 72 | 48 | Iohexol | 300 | 1.5 | 3 | 120 | |
| Patel 2017 (01) | [27] | R | USA | 88 | 62 | Iohexol | 350 | 1.5 | 3 | 120 | B |
| Patel 2017 (02) | [65] | R | USA | 410 | Iohexol | 350 | 1.5 | 3 | 120 | B | |
| Phillips 2017 | [70] | P mono | USA | 38 | 53 | Iohexol | 350 | 1.5 | 3 | 120 | B |
| Richter 2017 | [62] | R | Germany | 118 | 58 | Iopromide | 300 | 1.5 | 2–3 | 120 | |
| Saraya 2017 | [18] | P mono | Egypt | 34 | 54 | Iohexol | 300 | 1.5 | 4 | C | |
| Savaridas 2017 | [75] | P mono | Australia | 66 | 54 | 1.5 | 3 | 120 | B | ||
| Sogani 2017 | [80] | R | USA | 278 | 51 | Iohexol | 350 | 1.5 | 3 | 150 | A |
| Ali-Mucheru 2016 | [33] | R | USA | 351 | 62 | Iohexol | 350 | 1.5 | 3 | 120 | B |
| Ambicka 2016 | [29] | R | Poland | 82 | 57 | Iopromide | 370 | 1.5 | 3 | 120 | B |
| Brandan 2016 | [77] | P mono | Mexico | 18 | 51 | Ioversol | 300 | 4 | 60 | B | |
| Cheung 2016 (01) | [72] | R | Taiwan | 256 | 48 | Iohexol | 350 | 1.5 | 3 | 120 | A |
| Cheung 2016 (02) | [98] | R | Taiwan | 87 | 54 | Iohexol | 350 | 1.5 | 3 | 120 | B |
| Kamal 2016 | [95] | R | Egypt | 239 | 48 | Iohexol | 300 | 1.5 | 3 | 120 | B |
| Kariyappa 2016 | [68] | P mono | India | 44 | Iomeprol | 350 | 1.5 | 3 | 120 | B | |
| Knogler 2016 | [83] | P mono | Austria | 15 | 58 | Iomeprol | 400 | 2 | 3.5 | 60–90 | |
| Lalji 2016 | [21] | R | The Netherlands | 199 | 58 | Iopromide | 300 | 1.5 | 3 | 120 | |
| Łuczyńska 2016 (01) | [50] | P mono | Poland | 116 | 55 | Iopromide | 370 | 1.5 | 3 | 120 | B |
| Łuczyńska 2016 (02) | [67] | P mono | Poland | 193 | 55 | Iopromide | 370 | 1.5 | 3 | 120 | B |
| Tardivel 2016 | [19] | R | France | 195 | 56 | Iobitridol | 300 | 1.5 | 3 | 120 | B |
| Tennant 2016 | [15] | R | UK | 99 | 49 | ||||||
| Tsigginou 2016 | [89] | P mono | Greece | 216 | 55 | Iopromide | 300 | 1.5 | 2–3 | 120 | B |
| Wang 2016 | [97] | P mono | China | 68 | 53 | Iohexol | 350 | 1.5 | 3 | 120 | A |
| Yagil 2016 | [71] | R | Israel | 200 | 51 | Iopamidol | 370 | 1.5 | 3 | 120 | B |
| Chou 2015 | [14] | P mono | Taiwan | 185 | 51 | Iohexol | 300 | 1.5 | 2 | 120 | B |
| Elsaid 2015 | [73] | P mono | Egypt | 34 | 55 | Iohexol | 300 | 1.5 | 3 | B | |
| Hobbs 2015 | [81] | P mono | Australia | 49 | 55 | Iohexol | 350 | 1.5 | 3 | 120 | B |
| Kamal 2015 | [79] | R | Egypt | 168 | Iohexol | 300 | 1.5 | 3 | 120 | B | |
| Lobbes 2015 | [30] | R | The Netherlands | 87 | 62 | Iopromide | 300 | 1.5 | 3 | 120 | |
| Łuczyńska 2015 (01) | [91] | P mono | Poland | 174 | 56 | Iopromide | 370 | 1.5 | 3 | 120 | B |
| Łuczyńska 2015 (02) | [53] | P mono | Poland | 102 | Iopromide | 370 | 1.5 | 3 | 120 | ||
| Badr 2014 | [101] | P mono | France | 75 | 54 | Iohexol | 300 | 1.5 | 120 | B | |
| Blum 2014 | [31] | P mono | Germany | 20 | 57 | Iopamidol | 300 | 1.5 | 3 | 120 | |
| Cheung 2014 | [86] | R | Taiwan | 89 | 48 | Iohexol | 350 | 1.5 | 3 | 120–180 | B |
| Fallenberg 2014 (01) | [85] | P mono | Germany | 118 | 53 | Iobitridol | 300 | 1.5 | 3 | 120 | B |
| Fallenberg 2014 (02) | [32] | P mono | Germany | 80 | 54 | Iobitridol | 300 | 1.5 | 3 | 120 | B |
| Francescone 2014 | [66] | R | USA | 88 | 50 | ||||||
| Jeukens 2014 | [60] | R | The Netherlands | 47 | 58 | Iopromide | 300 | 1.5 | 3 | 120 | |
| Lobbes 2014 | [20] | R | The Netherlands | 113 | 57 | Iopromide | 300 | 1.5 | 3 | 120 | |
| Łuczyńska 2014 | [35] | P mono | Poland | 152 | 56 | Iopromide | 370 | 1.5 | 3 | 120 | B |
| Mokhtar 2014 | [57] | P mono | Egypt | 60 | Iohexol | 300 | 1.5 | 120 | A | ||
| Travieso-Aja 2014 | [64] | R | Spain | 136 | 49 | 1.5 | 3 | 120 | B | ||
| Hill 2013 | [10] | R | Canada | 98 | 57 | Iobitridol | 300 | 1.5 | 3 | 120 | B |
| Jochelson 2013 | [55] | P mono | USA | 82 | 50 | Iohexol | 350 | 1.5 | 3 | 150–300 | B |
| Dromain 2012 | [52] | P mono | France | 110 | 57 | Iobitridol | 300 | 1.5 | 3 | 120 | A |
| Diekmann 2011 | [61] | P mono | Germany | 70 | 55 | Iopromide | 370 | 1 | 4 | 60/120/180 | A |
| Dromain 2011 | [59] | P mono | France | 120 | 56 | Iobitridol | 300 | 1.5 | 3 | 120 | A |
| Dromain 2006 | [9] | P mono | France | 20 | 63 | Iohexol | 300 | 3 | 30 | B | |
| Diekmann 2005 | [8] | P mono | Germany | 21 | Iopromide | 370 | 1 | 4 | 60/120/180 | A | |
| Jong 2003 | [7] | P mono | Canada | 22 | Iohexol | 300 | 60 | B | |||
| Lewin 2003 | [96] | P mono | USA | 26 | 51 | Iohexol | 350 | 4–5 | 150 |
R retrospective, P mono prospective monocentric, P multi prospective multicentric, A = total exam time < 5 min, B = total exam time between 5 and 10 min, C = total exam time > 10 min
Timing of CESM examination with menstrual cycle was reported only in 18/84 studies (21%). In 10/18 (56%) articles, it was mentioned but not applied; in 6/18 (33%), it was applied with a feasibility window between the 5th and 14th day of menstrual cycle; in 2/18 (11%), CESM was synchronously performed with MRI in different phases of menstrual cycle to evaluate and compare background parenchymal enhancement.
Technical features and parameters
In 70 out of 84 studies (83%), different systems from General Electric Healthcare (Chicago, IL, USA) were used, all with a prototype or a commercial release of the SenoBright upgrade which is required to perform dual-energy contrast-enhanced imaging. Twelve out of 84 articles (14%) reported the adoption of Selenia Dimensions Mammography Unit (Hologic Inc., Marlborough, MA, USA), while the remaining 2/84 (3%) studies were conducted with a Siemens Healthineers (Erlangen, Germany) Mammography System (Mammomat or Mammomat Inspiration).
The type of ICA used was not reported in five articles [15, 24, 64, 66, 75], while in the remaining 79 studies (94%), for a total of 13465 patients (96%), six different molecules were used: Iohexol was the most frequently employed, being used in 42/79 studies (53%) for a total of 5049/13465 patients (37%), followed by Iopromide (18/79 studies, 23%; 2798/13465 patients, 21%), while Iobitridol, Iomeprol, Iopamidol and Ioversol were administered in the remaining studies (19/79 studies, 24%; 5618/13465 patients, 42%). Iohexol was utilised at a concentration of 350 mg iodine/mL (25/42 studies, 60%; 3330/5049 patients, 66%) or 300 mg iodine/mL (17/42 studies, 40%; 1719/5049 patients, 34%). Iopromide was also administered at two different concentrations: 370 mg iodine/mL (10/18 studies, 56%; 1032/2798 patients, 37%) and 300 mg iodine/mL (8/18 studies, 44%; 1766/2798 patients, 63%).
Of the 69 studies including a specification of the contrast injection modality, 59 (85%) utilised an automated power injector (10584/11725 patients, 90%) while manual contrast injection was carried out in the remaining 10 (15%) [7, 9, 17, 25, 28, 51, 57, 73, 95, 99] for a total of 1141/11725 patients (10%).
Contrast agent dose, detailed in 77 studies, was fixed at 1.5 mL/kg in 72 (93%) of them for a total of 13559/13687 (99%) patients. Contrast agent flow rate, reported in 76/84 studies (90%), was most frequently fixed at 3 mL/s (65/76 studies, 86%); the 11 remaining articles detailed a flow rate ranging from 2 to 5 mL/s. Thirty-five out of 84 (42%) articles for a total 8734/14012 patients (62%) also mentioned the use of additional post-contrast saline flush or “bolus chaser,” 19 of them (54%, for a total 4477/8734 patients, 51%) likewise detailing a saline amount ranging from 10 to 30 mL.
Of 69 studies detailing the tube voltage of both low- and high-energy acquisitions, all but one (99%) acquired low-energy images between 26 and 33.2 kVp, which is the peak kilovoltage threshold of iodine, while all 69 acquired high-energy images well above this threshold, i.e. between 44 and 50 kVp. The anode/filter combination was reported by 42/84 studies. Exposure parameters were unambiguously reported only in one study [10], whereas in 5 early studies [7, 8, 32, 59, 85], they were manually adjusted according to breast thickness and density; thirty-five other studies declared an automatic regulation of these parameters performed by the mammography unit.
Regarding radiation dose, data were scarcer: even though 45/84 articles (54%) mentioned this aspect, 17/45 (31%) did it without exhibiting original information but reporting observations from previous studies, therefore restricting the number of studies with new data to 28/84 (33%). Of these 28 studies, 19 (68%) provided an average glandular dose (AGD), 3 (16%) of them calculating it per-patient and ranging 1.5–6.9 mGy [8, 9, 58], 5/19 (26%) calculating it per-breast ranging 2.19–7.15 mGy and the remaining 11 (58%) reporting a per-view AGD ranging from 0.43 [61] to 2.65 mGy [101]. A comparison with DM was mentioned in 17 studies: only 1 (6%) documented a dose reduction (− 2%) for CESM compared to DM [32], while other 16 (94%) reported an increase in AGD ranging between 6.2% [85] and 100% [77]. However, it is worth to notice that 3 studies specifically contrived to assess CESM radiation doses reported an AGD increase of 42% [56], 78% [82] and 80% [60].
Acquisition protocols
Studies reporting the time interval between contrast injection and the first image acquisition were 78 out of 84 (93%), for a total 13244/14012 patients (95%) and 65 (83%) of them (12278/13244 patients, 93%) had it fixed at 120 s.
Sixty-six out of 84 articles (79%, 11900/14012 patients, 85%) gave an indication of the acquisition time after contrast injection: in 12/66 (18%, 1381/11900 patients, 11.6%), the exam was completed in less than 5 min; in 52/66 (80%, for total of 10485/11900 patients, 88.1%) between 5 and 10 min, while in 1/66 (2%, 34/11900 patients, 0.3%) the duration exceeded 10 min.
The outline of the image acquisition sequence remains more variable. Ten out of 84 studies (12%), accounting for 2734 patients (19%) did not clearly describe it and did not provide a reference to other protocols, while 3/84 (4%, 103/14012 patients, 1%) employed a curtailed and side-insensitive acquisition sequence. Adherence to standard but unspecified digital mammography protocols was declared by 29/84 (34%) studies, for total 3741/14012 patients (27%). The other half of the articles analysed (42/84, accounting for 7434/14012 patients, 53%) unequivocally detailed an acquisition sequence. Of these 42 studies, 14 (34%, 2048/7434 patients, 28%) adopted a projection order that was conventionally agreed upon, while the other 28 (66%, accounting for 5386/7434 patients, 72%) based their acquisition sequence on the presence of previous suspect or clearly pathologic findings.
Eighty-four articles came from 38 different research groups. Subgroup analysis according to research groups showed that 17 acquisition sequences based on a conventionally agreed projection order were executed in 15 research groups. As described in Fig. 3, the most common sequence description, reported by 6/17 (35%) institutions, was MLO - MLO - CC - CC (in order of acquisition), without any further indication about the first side to be examined (right or left or side with/without suspicious lesion or already diagnosed cancer). The second most common sequence (4/17, 24%) was CC - CC - MLO - MLO with the first projection standardised on the right side (independently of pathology or with suspected pathology).
Fig. 3.

Graphical summary of conventionally agreed view acquisition orders for contrast-enhanced spectral mammography: CC craniocaudal view, MLO mediolateral oblique view, L left, R right
Among the 22 acquisition sequences (coming from 20 institutions) centred on the presence of previous suspect or clearly pathologic findings, we found substantial variability between different orders of acquisition, as shown in Fig. 4. However, the most common sequence, adopted by 4/22 (19%) research groups, was 1) CC, suspected side; 2) CC, non-suspected side; 3) MLO, suspected side; and 4) MLO, non-suspected side.
Fig. 4.

Graphical summary of pathology-oriented view acquisition orders for contrast-enhanced spectral mammography: CC craniocaudal view, MLO mediolateral oblique view, S suspicious breast, NS not suspicious breast
Contrast agent adverse reaction rate meta-analysis
Regarding side effects from ICA administration, 48/84 studies (57%) declared a preventive anamnestic screening for previous adverse reactions or general contraindications to ICA administration. Pre-examination tests of renal function was mentioned in 39/84 studies (46%). Of note, 14/84 studies (29%) reported 30 adverse reactions out of 14012 patients, of which 26/30 (87%) were mild reactions limited to pruritus, hives, “scratchy throat” or other minor skin flushing that resolved promptly even when antihistamines or corticosteroids were not administered. In 3/30 (10%) cases [54, 58, 87], side effects were of moderate importance with nausea and vomiting, widespread urticaria resolved only after antihistamines and corticosteroids per os, and dyspnea that equally responded to oral antihistamine administration. Only 1/30 (3%) severe adverse reaction, requiring “intensive care” but resolved after short time, occurred in 14012 patients (0.007%) [61].
Therefore, the number of adverse reactions related to ICA administration ranged from 0, reported by 70 (88%) studies, to a maximum of 6 adverse reactions [14] with a total of 30 adverse reactions, showing no heterogeneity (Q = 64, degree of freedom 83, τ = 2.0972, I2 = 0%, p = 0.931). As shown in the forest plot of Fig. 5, using fixed-effect model, the pooled rate of adverse reactions across studies was 0.82%, with 0.64% and 1.05% as 95% CI.
Fig. 5.
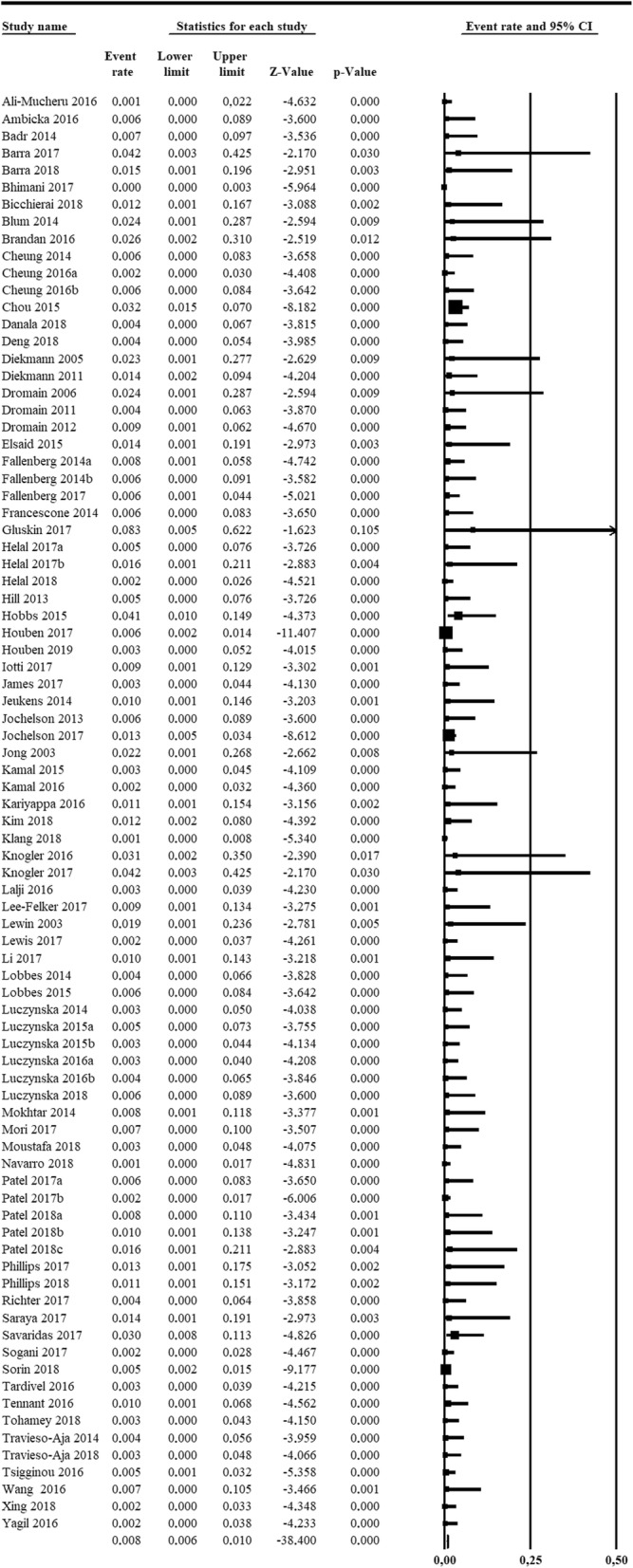
Forest plot of the 84 analysed articles on contrast-enhanced spectral mammography. No heterogeneity was found among studies (I2 = 0%). The last row shows the pooled rate for adverse reactions arising from iodinated contrast agent administration, calculated using the fixed-effect model
Visually inspecting the funnel plot in Fig. 6, risk of publication bias was found, as confirmed by the Egger test (p = 0.00028).
Fig. 6.

Funnel plot showing risk of publication bias in articles on contrast-enhanced spectral mammography, confirmed by the Egger test (p < 0.001)
Discussion
Our systematic review included 84 articles, accounting for 14012 patients, reporting the use of CESM in various settings. The sheer number of studies and, as depicted in Fig. 7, their increase in the last 3 years (27 studies between 2003 and December 2015, 57 from January 2016 to January 2019) points out a considerable interest in this emerging breast imaging modality.
Fig. 7.

Graphic showing the number of articles published per year regarding contrast-enhanced spectral mammography
A number of narrative reviews [6, 42, 102–106] favourably outlined CESM future perspectives in several clinical settings (e.g. recall work-up, pre-operative staging, and monitoring the effect of neoadjuvant therapy) as a potential alternative to MRI.
In the first phase of CESM development, some non-fixed parameters regarding contrast agent administration (i.e. contrast agent molecule, concentration, dose, flow rate, and injection modality) and some acquisition features (i.e. time between contrast injection and first acquisition, kVp ranges for low- and high-energy acquisitions) gained an international agreement. However, in the framework of comprehensive optimisation and standardisation of CESM, large-scale studies are undoubtedly needed to address the knowledge gap concerning the choice of technical parameters.
Our data show a consensus among studies (93%) on the choice of 1.5 mL/kg contrast dose administered with a 3 mL/s flow rate (74%) and a less extensive agreement on the use of Iohexol (53% of all studies) at a concentration of 350 mg iodine/mL (30% of all studies). However, these parameters have probably been empirically adopted from CT protocols, as the first investigators plainly stated [7], without any other particular explication or justification. No dose-finding studies have been published yet.
Similarly, the common use of a power contrast injector (87% of all studies, with the remaining 13% coming from a single research group) is assumed from CT and MRI protocols in which it has been demonstrated to be effective in obtaining a stable contrast inflow and bolus shape [107–109]. Moreover, the use of a power injector allows for the administration of a bolus chaser, reported only in 42% of all articles, a technical refinement that has shown good results in CT [110, 111].
Two other points need to be mentioned. The first one is the correlation between menstrual cycle phase and background parenchymal enhancement, explored in a few studies [10, 75, 80] and/or fluctuations of lesion contrast uptake. Secondly, since CESM is based on a dual X-ray exposure, of which the low-energy one has been demonstrated to be equal to standard DM [66], an increase in radiation dose is expected. However, while preliminary studies estimated a negligible [7] or curtailed AGD increase, studies specifically devised to ascertain CESM effective AGD found a substantial AGD increment ranging 42–80% [56, 60, 82]. While CESM AGDs remain under the threshold stated by European guidelines for screening mammography [112], further studies are needed to investigate CESM AGD [56, 82].
Furthermore, we remark the absence of standardised protocols. This methodological void, especially regarding the acquisition workflow, represents a threat to reproducibility and comparison of imaging results. While 98% of all studies reporting the total examination time completed the examination before 10 min from contrast administration, and while some studies presented evidence on the irrelevance of the acquisition order [55, 64], there are no studies comparing different approaches.
The pooled rate of adverse reactions to ICA administration was 0.82% (0.64–1.05% 95% CI) with a total of 30 adverse reactions in 14012 patients, a rate similar to that reported for CT 0.6% [113] in 84928 adult patients or 0.7% [114] in 29508 patients (given Iopromide, which is also used for CESM). Particularly, considering only severe adverse reactions in CT, Wang et al. [113] reported 11/84928 (0.0129%) reactions, as well as Mortelé et al. [114] 4/29508 (0.0135%). These rates seem to be higher than that found in our meta-analysis 1/14012 (0.007%), a comparison to consider with caution due to the nature of rare events such as severe reactions to ICA. One aspect to consider is the different profile of patients undergoing CESM compared to those requiring contrast-enhanced CT, the former being that of basically “healthy” subjects, the latter implying the possibility of relevant disease, including also serious emergency conditions.
This review has limitations. Patient data are probably shared and duplicate among some studies from the same research group. This has been shown to negatively impact on review quality [115, 116] and could only be prevented via individual patient data sharing [117]. However, for technical aspects of this systematic review, our choice to evaluate study groups rather than single articles should have mitigated this bias. Conversely, our pooled rate of adverse reactions could be underestimated.
In conclusion, our review shows that CESM is unevenly performed across different centres, in terms of contrast agent type and concentration and order of view acquisition. However, most research groups performed CESM using a contrast dose of 1.5 mL/kg, factory-set kVp ranges for low- and high-energy acquisitions, beginning image acquisition after 120 s from contrast agent injection and completing the examination within 10 min. Further studies are needed to investigate the role of background parenchymal enhancement and to harvest data that can firmly back up subsequent technical guidelines and consensus statements for standardised CESM protocols.
Abbreviations
- AGD
Average glandular dose
- CC
Craniocaudal
- CESM
Contrast-enhanced spectral mammography
- CI
Confidence interval
- CT
Computed tomography
- DM
Digital mammography
- ICA
Iodinated contrast agent
- kVp
Peak kilovoltage
- MLO
Mediolateral oblique
- MRI
Magnetic resonance imaging
- PRISMA
Preferred Reporting Items for Systematic Reviews and Meta-Analyses
Authors’ contributions
Each author has participated sufficiently in this work to take public responsibility for its content. The manuscript is approved by all authors and by the responsible authorities. All authors read and approved the final manuscript.
Funding
This research did not receive any specific grant from funding agencies in the public, commercial or not-for-profit sectors.
Availability of data and materials
The datasets used and analysed during the current study are available from the corresponding author on reasonable request.
Ethics approval and consent to participate
Not applicable
Consent for publication
Not applicable
Competing interests
FS declares to have received grants from or to be member of speakers’ bureau/advisory board for Bayer, Bracco, and General Electric. All other authors declare that they have no competing interests.
Footnotes
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
References
- 1.Frigerio Alfonso, Sardanelli Francesco, Podo Franca. Breast Cancer. Cham: Springer International Publishing; 2017. Radiological Screening of Breast Cancer: Evolution; pp. 171–203. [Google Scholar]
- 2.Pisano ED, Gatsonis C, Hendrick E, et al. Diagnostic performance of digital versus film mammography for breast-cancer screening. N Engl J Med. 2005;353:1773–1783. doi: 10.1056/NEJMoa052911. [DOI] [PubMed] [Google Scholar]
- 3.Gilbert FJ, Tucker L, Young KC. Digital breast tomosynthesis (DBT): a review of the evidence for use as a screening tool. Clin Radiol. 2016;71:141–150. doi: 10.1016/j.crad.2015.11.008. [DOI] [PubMed] [Google Scholar]
- 4.Pattacini P, Nitrosi A, Giorgi Rossi P, et al. Digital mammography versus digital mammography plus tomosynthesis for breast cancer screening: the Reggio Emilia Tomosynthesis randomized trial. Radiology. 2018;288:375–385. doi: 10.1148/radiol.2018172119. [DOI] [PubMed] [Google Scholar]
- 5.Marinovich M Luke, Hunter Kylie E, Macaskill Petra, Houssami Nehmat. Breast Cancer Screening Using Tomosynthesis or Mammography: A Meta-analysis of Cancer Detection and Recall. JNCI: Journal of the National Cancer Institute. 2018;110(9):942–949. doi: 10.1093/jnci/djy121. [DOI] [PubMed] [Google Scholar]
- 6.Patel Bhavika K., Lobbes M.B.I., Lewin John. Contrast Enhanced Spectral Mammography: A Review. Seminars in Ultrasound, CT and MRI. 2018;39(1):70–79. doi: 10.1053/j.sult.2017.08.005. [DOI] [PubMed] [Google Scholar]
- 7.Jong RA, Yaffe MJ, Skarpathiotakis M, et al. Contrast-enhanced digital mammography: initial clinical experience. Radiology. 2003;228:842–850. doi: 10.1148/radiol.2283020961. [DOI] [PubMed] [Google Scholar]
- 8.Diekmann Felix, Diekmann Susanne, Jeunehomme Fanny, Muller Serge, Hamm Bernd, Bick Ulrich. Digital Mammography Using Iodine-Based Contrast Media. Investigative Radiology. 2005;40(7):397–404. doi: 10.1097/01.rli.0000167421.83203.4e. [DOI] [PubMed] [Google Scholar]
- 9.Dromain Clarisse, Balleyguier Corrine, Muller Serge, Mathieu Marie-Christine, Rochard France, Opolon Paule, Sigal Robert. Evaluation of Tumor Angiogenesis of Breast Carcinoma Using Contrast-Enhanced Digital Mammography. American Journal of Roentgenology. 2006;187(5):W528–W537. doi: 10.2214/AJR.05.1944. [DOI] [PubMed] [Google Scholar]
- 10.Hill Melissa L., Mainprize James G., Carton Ann-Katherine, Saab-Puong Sylvie, Iordache Răzvan, Muller Serge, Jong Roberta A., Dromain Clarisse, Yaffe Martin J. Anatomical noise in contrast-enhanced digital mammography. Part II. Dual-energy imaging. Medical Physics. 2013;40(8):081907. doi: 10.1118/1.4812681. [DOI] [PubMed] [Google Scholar]
- 11.Dromain C, Balleyguier C, Adler G, Garbay JR, Delaloge S. Contrast-enhanced digital mammography. Eur J Radiol. 2009;69:34–42. doi: 10.1016/j.ejrad.2008.07.035. [DOI] [PubMed] [Google Scholar]
- 12.Skarpathiotakis M, Yaffe MJ, Bloomquist AK, et al. Development of contrast digital mammography. Med Phys. 2002;29:2419–2426. doi: 10.1118/1.1510128. [DOI] [PubMed] [Google Scholar]
- 13.Bhimani C, Matta D, Roth RG, et al. Contrast-enhanced spectral mammography. Acad Radiol. 2017;24:84–88. doi: 10.1016/j.acra.2016.08.019. [DOI] [PubMed] [Google Scholar]
- 14.Chou C-P, Lewin JM, Chiang C-L, et al. Clinical evaluation of contrast-enhanced digital mammography and contrast enhanced tomosynthesis—comparison to contrast-enhanced breast MRI. Eur J Radiol. 2015;84:2501–2508. doi: 10.1016/j.ejrad.2015.09.019. [DOI] [PubMed] [Google Scholar]
- 15.Tennant SL, James JJ, Cornford EJ, et al. Contrast-enhanced spectral mammography improves diagnostic accuracy in the symptomatic setting. Clin Radiol. 2016;71:1148–1155. doi: 10.1016/j.crad.2016.05.009. [DOI] [PubMed] [Google Scholar]
- 16.Lewis TC, Pizzitola VJ, Giurescu ME, et al. Contrast-enhanced digital mammography: a single-institution experience of the first 208 cases. Breast J. 2017;23:67–76. doi: 10.1111/tbj.12681. [DOI] [PubMed] [Google Scholar]
- 17.Moustafa AFI, Kamal EF, Hassan MM, Sakr M, Gomaa MMM. The added value of contrast enhanced spectral mammography in identification of multiplicity of suspicious lesions in dense breast. Egypt J Radiol Nucl Med. 2018;49:259–264. doi: 10.1016/j.ejrnm.2017.10.003. [DOI] [Google Scholar]
- 18.Saraya S, Adel L, Mahmoud A. Indeterminate breast lesions: can contrast enhanced digital mammography change our decisions? Egypt J Radiol Nucl Med. 2017;48:547–552. doi: 10.1016/j.ejrnm.2017.03.006. [DOI] [Google Scholar]
- 19.Tardivel A-M, Balleyguier C, Dunant A, et al. Added value of contrast-enhanced spectral mammography in postscreening assessment. Breast J. 2016;22:520–528. doi: 10.1111/tbj.12627. [DOI] [PubMed] [Google Scholar]
- 20.Lobbes MB, Lalji U, Houwers J et al (2014) Contrast-enhanced spectral mammography in patients referred from the breast cancer screening programme. Eur Radiol 24:1668–1676 [DOI] [PubMed]
- 21.Lalji U. C., Houben I. P. L., Prevos R., Gommers S., van Goethem M., Vanwetswinkel S., Pijnappel R., Steeman R., Frotscher C., Mok W., Nelemans P., Smidt M. L., Beets-Tan R. G., Wildberger J. E., Lobbes M. B. I. Contrast-enhanced spectral mammography in recalls from the Dutch breast cancer screening program: validation of results in a large multireader, multicase study. European Radiology. 2016;26(12):4371–4379. doi: 10.1007/s00330-016-4336-0. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Houben IP, Vanwetswinkel S, Kalia V et al (2019) Contrast-enhanced spectral mammography in the evaluation of breast suspicious calcifications: diagnostic accuracy and impact on surgical management. Acta Radiol. [Epub ahead of print] [DOI] [PMC free article] [PubMed]
- 23.Patel BK, Davis J, Ferraro C, et al. Value added of preoperative contrast-enhanced digital mammography in patients with invasive lobular carcinoma of the breast. Clin Breast Cancer. 2018;18:e1339–e1345. doi: 10.1016/j.clbc.2018.07.012. [DOI] [PubMed] [Google Scholar]
- 24.Travieso-Aja M. del Mar, Naranjo-Santana P., Fernández-Ruiz C., Severino-Rondón W., Maldonado-Saluzzi D., Rodríguez Rodríguez M., Vega-Benítez V., Luzardo O.P. Factors affecting the precision of lesion sizing with contrast-enhanced spectral mammography. Clinical Radiology. 2018;73(3):296–303. doi: 10.1016/j.crad.2017.10.017. [DOI] [PubMed] [Google Scholar]
- 25.Helal MH, Mansour SM, Salaleldin LA, Alkalaawy BM, Salem DS, Mokhtar NM (2018) The impact of contrast-enhanced spectral mammogram (CESM) and three-dimensional breast ultrasound (3DUS) on the characterization of the disease extend in cancer patients. Br J Radiol 91:20170977 [DOI] [PMC free article] [PubMed]
- 26.Lee-Felker SA, Tekchandani L, Thomas M, et al. Newly diagnosed breast cancer: comparison of contrast-enhanced spectral mammography and breast MR imaging in the evaluation of extent of disease. Radiology. 2017;285:389–400. doi: 10.1148/radiol.2017161592. [DOI] [PubMed] [Google Scholar]
- 27.Patel BK, Garza SA, Eversman S, Lopez-Alvarez Y, Kosiorek H, Pockaj BA. Assessing tumor extent on contrast-enhanced spectral mammography versus full-field digital mammography and ultrasound. Clin Imaging. 2017;46:78–84. doi: 10.1016/j.clinimag.2017.07.001. [DOI] [PubMed] [Google Scholar]
- 28.Helal Maha H, Mansour Sahar M, Zaglol Mai, Salaleldin Lamia A, Nada Omniya M, Haggag Marwa A. Staging of breast cancer and the advanced applications of digital mammogram: what the physician needs to know? The British Journal of Radiology. 2017;90(1071):20160717. doi: 10.1259/bjr.20160717. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Ambicka Aleksandra, Luczynska Elzbieta, Adamczyk Agnieszka, Harazin-Lechowska Agnieszka, Sas-Korczynska Beata, Niemiec Joanna. The tumour border on contrast-enhanced spectral mammography and its relation to histological characteristics of invasive breast cancer. Polish Journal of Pathology. 2016;3:295–299. doi: 10.5114/pjp.2016.63783. [DOI] [PubMed] [Google Scholar]
- 30.Lobbes Marc B.I., Lalji Ulrich C., Nelemans Patty J., Houben Ivo, Smidt Marjolein L., Heuts Esther, de Vries Bart, Wildberger Joachim E., Beets-Tan Regina G. The Quality of Tumor Size Assessment by Contrast-Enhanced Spectral Mammography and the Benefit of Additional Breast MRI. Journal of Cancer. 2015;6(2):144–150. doi: 10.7150/jca.10705. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Blum KS, Rubbert C, Mathys B, Antoch G, Mohrmann S, Obenauer S. Use of contrast-enhanced spectral mammography for intramammary cancer staging. Acad Radiol. 2014;21:1363–1369. doi: 10.1016/j.acra.2014.06.012. [DOI] [PubMed] [Google Scholar]
- 32.Fallenberg EM, Dromain C, Diekmann F, et al. Contrast-enhanced spectral mammography versus MRI: initial results in the detection of breast cancer and assessment of tumour size. Eur Radiol. 2014;24:256–264. doi: 10.1007/s00330-013-3007-7. [DOI] [PubMed] [Google Scholar]
- 33.Ali-Mucheru M, Pockaj B, Patel B, et al. Contrast-enhanced digital mammography in the surgical management of breast cancer. Ann Surg Oncol. 2016;23:649–655. doi: 10.1245/s10434-016-5567-7. [DOI] [PubMed] [Google Scholar]
- 34.Patel BK, Ranjbar S, Wu T, et al. Computer-aided diagnosis of contrast-enhanced spectral mammography: a feasibility study. Eur J Radiol. 2018;98:207–213. doi: 10.1016/j.ejrad.2017.11.024. [DOI] [PubMed] [Google Scholar]
- 35.Luczyńska E, Heinze-Paluchowska S, Dyczek S, Blecharz P, Rys J, Reinfuss M. Contrast-enhanced spectral mammography: comparison with conventional mammography and histopathology in 152 women. Korean J Radiol. 2014;15:689. doi: 10.3348/kjr.2014.15.6.689. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36.Luczynska E, Niemiec J, Heinze S, et al. Intensity and pattern of enhancement on CESM: prognostic significance and its relation to expression of podoplanin in tumor stroma - a preliminary report. Anticancer Res. 2018;38:1085–1095. doi: 10.21873/anticanres.12327. [DOI] [PubMed] [Google Scholar]
- 37.Iotti V, Ravaioli S, Vacondio R, et al. Contrast-enhanced spectral mammography in neoadjuvant chemotherapy monitoring: a comparison with breast magnetic resonance imaging. Breast Cancer Res. 2017;19:106. doi: 10.1186/s13058-017-0899-1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 38.Patel BK, Hilal T, Covington M, et al. Contrast-enhanced spectral mammography is comparable to MRI in the assessment of residual breast cancer following neoadjuvant systemic therapy. Ann Surg Oncol. 2018;25:1350–1356. doi: 10.1245/s10434-018-6413-x. [DOI] [PubMed] [Google Scholar]
- 39.Barra Filipe Ramos, Souza Fernanda Freire de, Camelo Rosimara Eva Ferreira Almeida, Ribeiro Andrea Campos de Oliveira, Farage Luciano. Accuracy of contrast-enhanced spectral mammography for estimating residual tumor size after neoadjuvant chemotherapy in patients with breast cancer: a feasibility study. Radiologia Brasileira. 2017;50(4):224–230. doi: 10.1590/0100-3984.2016-0029. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 40.Barra FR, Sobrinho AB, Barra RR, et al. Contrast-enhanced mammography (CEM) for detecting residual disease after neoadjuvant chemotherapy: a comparison with breast magnetic resonance imaging (MRI) Biomed Res Int. 2018;2018:1–9. doi: 10.1155/2018/8531916. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 41.Tagliafico AS, Bignotti B, Rossi F, et al. Diagnostic performance of contrast-enhanced spectral mammography: systematic review and meta-analysis. Breast. 2016;28:13–19. doi: 10.1016/j.breast.2016.04.008. [DOI] [PubMed] [Google Scholar]
- 42.Zhu Xiao, Huang Jun-ming, Zhang Kun, Xia Long-jie, Feng Lan, Yang Ping, Zhang Meng-ya, Xiao Wei, Lin Hui-xia, Yu Ying-hua. Diagnostic Value of Contrast-Enhanced Spectral Mammography for Screening Breast Cancer: Systematic Review and Meta-analysis. Clinical Breast Cancer. 2018;18(5):e985–e995. doi: 10.1016/j.clbc.2018.06.003. [DOI] [PubMed] [Google Scholar]
- 43.Sardanelli F, Boetes C, Borisch B, et al. Magnetic resonance imaging of the breast: recommendations from the EUSOMA working group. Eur J Cancer. 2010;46:1296–1316. doi: 10.1016/j.ejca.2010.02.015. [DOI] [PubMed] [Google Scholar]
- 44.Mann RM, Kuhl CK, Kinkel K, Boetes C. Breast MRI: guidelines from the European Society of Breast Imaging. Eur Radiol. 2008;18:1307–1318. doi: 10.1007/s00330-008-0863-7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 45.The American Society of Breast Surgeons. Consensus guideline on diagnostic and screening magnetic resonance imaging of the breast. https://www.breastsurgeons.org/about/statements/PDF_Statements/MRI.pdf. Accessed 30 May 2019.
- 46.American College of Radiology. ACR practice parameter for the performance of contrast-enhanced magnetic resonance imaging (MRI) of the breast. Available from: https://www.acr.org/-/media/ACR/Files/Practice-Parameters/mr-contrast-breast.pdf. Accessed 30 May 2019.
- 47.Zanardo M, Cozzi A, Trimboli RM, Carbonaro LA, Sardanelli F. Technique and diagnostic performance of contrast-enhanced spectral mammography: a systematic review. PROSPERO 2018 CRD42018118554. Available from: https://www.crd.york.ac.uk/PROSPERO/display_record.php?ID=CRD42018118554. Accessed 30 May 2019.
- 48.Moher D, Liberati A, Tetzlaff J, Altman DG. Preferred Reporting Items for Systematic Reviews and Meta-Analyses: the PRISMA statement. PLoS Med. 2009;6:e1000097. doi: 10.1371/journal.pmed.1000097. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 49.Egger M., Smith G. D., Schneider M., Minder C. Bias in meta-analysis detected by a simple, graphical test. BMJ. 1997;315(7109):629–634. doi: 10.1136/bmj.315.7109.629. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 50.Luczyńska E, Heinze S, Adamczyk A, Rys J, Mitus JW, Hendrick E. Comparison of the mammography, contrast-enhanced spectral mammography and ultrasonography in a group of 116 patients. Anticancer Res. 2016;36:4359–4366. [PubMed] [Google Scholar]
- 51.Tohamey YM, Youssry SW, Abd El Aziz AI. Interpretation of patterns of enhancement on contrast-enhanced spectral mammography: an approach to a standardized scheme. Egypt J Radiol Nucl Med. 2018;49:854–868. doi: 10.1016/j.ejrnm.2018.03.004. [DOI] [Google Scholar]
- 52.Dromain C, Thibault F, Diekmann F, et al. Dual-energy contrast-enhanced digital mammography: initial clinical results of a multireader, multicase study. Breast Cancer Res. 2012;14:R94. doi: 10.1186/bcr3210. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 53.Łuczyńska E, Heinze-Paluchowska S, Hendrick E, et al. Comparison between breast MRI and contrast-enhanced spectral mammography. Med Sci Monit. 2015;21:1358–1367. doi: 10.12659/MSM.893018. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 54.Jochelson MS, Pinker K, Dershaw DD, et al. Comparison of screening CEDM and MRI for women at increased risk for breast cancer: a pilot study. Eur J Radiol. 2017;97:37–43. doi: 10.1016/j.ejrad.2017.10.001. [DOI] [PubMed] [Google Scholar]
- 55.Jochelson MS, Dershaw DD, Sung JS, et al. Bilateral contrast-enhanced dual-energy digital mammography: feasibility and comparison with conventional digital mammography and MR imaging in women with known breast carcinoma. Radiology. 2013;266:743–751. doi: 10.1148/radiol.12121084. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 56.James Judy R., Pavlicek William, Hanson James A., Boltz Thomas F., Patel Bhavika K. Breast Radiation Dose With CESM Compared With 2D FFDM and 3D Tomosynthesis Mammography. American Journal of Roentgenology. 2017;208(2):362–372. doi: 10.2214/AJR.16.16743. [DOI] [PubMed] [Google Scholar]
- 57.Mokhtar O, Mahmoud S. Can contrast enhanced mammography solve the problem of dense breast lesions? Egypt J Radiol Nucl Med. 2014;45:1043–1052. doi: 10.1016/j.ejrnm.2014.04.007. [DOI] [Google Scholar]
- 58.Houben IPL, Van de Voorde P, Jeukens CRLPN, et al. Contrast-enhanced spectral mammography as work-up tool in patients recalled from breast cancer screening has low risks and might hold clinical benefits. Eur J Radiol. 2017;94:31–37. doi: 10.1016/j.ejrad.2017.07.004. [DOI] [PubMed] [Google Scholar]
- 59.Dromain C, Thibault F, Muller S, et al. Dual-energy contrast-enhanced digital mammography: initial clinical results. Eur Radiol. 2011;21:565–574. doi: 10.1007/s00330-010-1944-y. [DOI] [PubMed] [Google Scholar]
- 60.Jeukens Cécile R.L.P.N., Lalji Ulrich C., Meijer Eduard, Bakija Betina, Theunissen Robin, Wildberger Joachim E., Lobbes Marc B.I. Radiation Exposure of Contrast-Enhanced Spectral Mammography Compared With Full-Field Digital Mammography. Investigative Radiology. 2014;49(10):659–665. doi: 10.1097/RLI.0000000000000068. [DOI] [PubMed] [Google Scholar]
- 61.Diekmann F, Freyer M, Diekmann S, et al. Evaluation of contrast-enhanced digital mammography. Eur J Radiol. 2011;78:112–121. doi: 10.1016/j.ejrad.2009.10.002. [DOI] [PubMed] [Google Scholar]
- 62.Richter V, Hatterman V, Preibsch H, et al. Contrast-enhanced spectral mammography in patients with MRI contraindications. Acta Radiol. 2018;59:798–805. doi: 10.1177/0284185117735561. [DOI] [PubMed] [Google Scholar]
- 63.Gluskin J, Click M, Fleischman R, Dromain C, Morris EA, Jochelson MS. Contamination artifact that mimics in-situ carcinoma on contrast-enhanced digital mammography. Eur J Radiol. 2017;95:147–154. doi: 10.1016/j.ejrad.2017.08.002. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 64.Travieso Aja M.M., Rodríguez Rodríguez M., Alayón Hernández S., Vega Benítez V., Luzardo O.P. Dual-energy contrast-enhanced mammography. Radiología (English Edition) 2014;56(5):390–399. doi: 10.1016/j.rxeng.2014.05.007. [DOI] [PubMed] [Google Scholar]
- 65.Patel BK, Naylor ME, Kosiorek HE, et al. Clinical utility of contrast-enhanced spectral mammography as an adjunct for tomosynthesis-detected architectural distortion. Clin Imaging. 2017;46:44–52. doi: 10.1016/j.clinimag.2017.07.003. [DOI] [PubMed] [Google Scholar]
- 66.Francescone MA, Jochelson MS, Dershaw DD, et al. Low energy mammogram obtained in contrast-enhanced digital mammography (CEDM) is comparable to routine full-field digital mammography (FFDM) Eur J Radiol. 2014;83:1350–1355. doi: 10.1016/j.ejrad.2014.05.015. [DOI] [PubMed] [Google Scholar]
- 67.Łuczyńska E, Niemiec J, Hendrick E, et al. Degree of enhancement on contrast enhanced spectral mammography (CESM) and lesion type on mammography (MG): comparison based on histological results. Med Sci Monit. 2016;22:3886–3893. doi: 10.12659/MSM.900371. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 68.Kariyappa Kalpana D, Gnanaprakasam Francis, Anand Subhapradha, Krishnaswami Murali, Ramachandran Madan. Contrast enhanced dual energy spectral mammogram, an emerging addendum in breast imaging. The British Journal of Radiology. 2016;89(1067):20150609. doi: 10.1259/bjr.20150609. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 69.Danala G, Patel B, Aghaei F, et al. Classification of breast masses using a computer-aided diagnosis scheme of contrast enhanced digital mammograms. Ann Biomed Eng. 2018;46:1419–1431. doi: 10.1007/s10439-018-2044-4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 70.Phillips J, Miller MM, Mehta TS, et al. Contrast-enhanced spectral mammography (CESM) versus MRI in the high-risk screening setting: patient preferences and attitudes. Clin Imaging. 2017;42:193–197. doi: 10.1016/j.clinimag.2016.12.011. [DOI] [PubMed] [Google Scholar]
- 71.Yagil Y, Shalmon A, Rundstein A, et al. Challenges in contrast-enhanced spectral mammography interpretation: artefacts lexicon. Clin Radiol. 2016;71:450–457. doi: 10.1016/j.crad.2016.01.012. [DOI] [PubMed] [Google Scholar]
- 72.Cheung Y-C, Tsai H-P, Lo Y-F, Ueng S-H, Huang P-C, Chen S-C. Clinical utility of dual-energy contrast-enhanced spectral mammography for breast microcalcifications without associated mass: a preliminary analysis. Eur Radiol. 2016;26:1082–1089. doi: 10.1007/s00330-015-3904-z. [DOI] [PubMed] [Google Scholar]
- 73.ElSaid NAE, Farouk S, Shetat OMM, Khalifa NM, Nada OM. Contrast enhanced digital mammography: is it useful in detecting lesions in edematous breast? Egypt J Radiol Nucl Med. 2015;46:811–819. doi: 10.1016/j.ejrnm.2015.04.002. [DOI] [Google Scholar]
- 74.Mori M, Akashi-Tanaka S, Suzuki S, et al. Diagnostic accuracy of contrast-enhanced spectral mammography in comparison to conventional full-field digital mammography in a population of women with dense breasts. Breast Cancer. 2017;24:104–110. doi: 10.1007/s12282-016-0681-8. [DOI] [PubMed] [Google Scholar]
- 75.Savaridas SL, Taylor DB, Gunawardana D, Phillips M. Could parenchymal enhancement on contrast-enhanced spectral mammography (CESM) represent a new breast cancer risk factor? Correlation with known radiology risk factors. Clin Radiol. 2017;72:1085.e1–1085.e9. doi: 10.1016/j.crad.2017.07.017. [DOI] [PubMed] [Google Scholar]
- 76.Fallenberg EM, Schmitzberger FF, Amer H, et al. Contrast-enhanced spectral mammography vs. mammography and MRI – clinical performance in a multi-reader evaluation. Eur Radiol. 2017;27:2752–2764. doi: 10.1007/s00330-016-4650-6. [DOI] [PubMed] [Google Scholar]
- 77.Brandan María-Ester, Cruz-Bastida Juan P, Rosado-Méndez Iván M, Villaseñor-Navarro Yolanda, Pérez-Ponce Héctor, Galván Héctor A, Trujillo-Zamudio Flavio E, Sánchez-Suárez Patricia, Benítez-Bribiesca Luis. Clinical study of contrast-enhanced digital mammography and the evaluation of blood and lymphatic microvessel density. The British Journal of Radiology. 2016;89(1065):20160232. doi: 10.1259/bjr.20160232. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 78.Deng C-Y, Juan Y-H, Cheung Y-C et al (2018) Quantitative analysis of enhanced malignant and benign lesions on contrast-enhanced spectral mammography. Br J Radiol 91:20170605 [DOI] [PMC free article] [PubMed]
- 79.Mohamed Kamal R, Hussien Helal M, Wessam R, Mahmoud Mansour S, Godda I, Alieldin N. Contrast-enhanced spectral mammography: impact of the qualitative morphology descriptors on the diagnosis of breast lesions. Eur J Radiol. 2015;84:1049–1055. doi: 10.1016/j.ejrad.2015.03.005. [DOI] [PubMed] [Google Scholar]
- 80.Sogani J, Morris EA, Kaplan JB, et al. Comparison of background parenchymal enhancement at contrast-enhanced spectral mammography and breast MR imaging. Radiology. 2017;282:63–73. doi: 10.1148/radiol.2016160284. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 81.Hobbs MM, Taylor DB, Buzynski S, Peake RE. Contrast-enhanced spectral mammography (CESM) and contrast enhanced MRI (CEMRI): patient preferences and tolerance. J Med Imaging Radiat Oncol. 2015;59:300–305. doi: 10.1111/1754-9485.12296. [DOI] [PubMed] [Google Scholar]
- 82.Phillips Jordana, Mihai Georgeta, Hassonjee Sarah Esaa, Raj Sean D., Palmer Matthew R., Brook Alexander, Zhang Da. Comparative Dose of Contrast-Enhanced Spectral Mammography (CESM), Digital Mammography, and Digital Breast Tomosynthesis. American Journal of Roentgenology. 2018;211(4):839–846. doi: 10.2214/AJR.17.19036. [DOI] [PubMed] [Google Scholar]
- 83.Knogler T, Homolka P, Hörnig M, et al. Contrast-enhanced dual energy mammography with a novel anode/filter combination and artifact reduction: a feasibility study. Eur Radiol. 2016;26:1575–1581. doi: 10.1007/s00330-015-4007-6. [DOI] [PubMed] [Google Scholar]
- 84.Xing Dong, Lv Yongbin, Sun Bolin, Xie Haizhu, Dong Jianjun, Hao Cuijuan, Chen Qianqian, Chi Xiaoxiao. Diagnostic Value of Contrast-Enhanced Spectral Mammography in Comparison to Magnetic Resonance Imaging in Breast Lesions. Journal of Computer Assisted Tomography. 2019;43(2):245–251. doi: 10.1097/RCT.0000000000000832. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 85.Fallenberg EM, Dromain C, Diekmann F, et al. Contrast-enhanced spectral mammography: does mammography provide additional clinical benefits or can some radiation exposure be avoided? Breast Cancer Res Treat. 2014;146:371–381. doi: 10.1007/s10549-014-3023-6. [DOI] [PubMed] [Google Scholar]
- 86.Cheung Y-C, Lin Y-C, Wan Y-L, et al. Diagnostic performance of dual-energy contrast-enhanced subtracted mammography in dense breasts compared to mammography alone: interobserver blind-reading analysis. Eur Radiol. 2014;24:2394–2403. doi: 10.1007/s00330-014-3271-1. [DOI] [PubMed] [Google Scholar]
- 87.Kim EY, Youn I, Lee KH, et al. Diagnostic value of contrast-enhanced digital mammography versus contrast-enhanced magnetic resonance imaging for the preoperative evaluation of breast cancer. J Breast Cancer. 2018;21:453. doi: 10.4048/jbc.2018.21.e62. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 88.Klang E., Krosser A., Amitai M.M., Sorin V., Halshtok Neiman O., Shalmon A., Gotlieb M., Sklair-Levy M. Utility of routine use of breast ultrasound following contrast-enhanced spectral mammography. Clinical Radiology. 2018;73(10):908.e11-908.e16. doi: 10.1016/j.crad.2018.05.031. [DOI] [PubMed] [Google Scholar]
- 89.Tsigginou Alexandra, Gkali Christina, Chalazonitis Athanasios, Feida Eleni, Vlachos Dimitrios Efthymios, Zagouri Flora, Rellias Ioannis, Dimitrakakis Constantine. Adding the power of iodinated contrast media to the credibility of mammography in breast cancer diagnosis. The British Journal of Radiology. 2016;89(1067):20160397. doi: 10.1259/bjr.20160397. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 90.Navarro ME, Razmilic D, Araos I, Rodrigo A, Andia ME (2018) Contrast-enhanced spectral mammography. Experience in 465 examinations. Rev Med Chil 146:141–149 [DOI] [PubMed]
- 91.Luczynska Elzbieta, Niemiec Joanna, Ambicka Aleksandra, Adamczyk Agnieszka, Walasek Tomasz, Ryś Janusz, Sas-Korczyńska Beata. Correlation between blood and lymphatic vessel density and results of contrast-enhanced spectral mammography. Polish Journal of Pathology. 2015;3:310–322. doi: 10.5114/pjp.2015.54965. [DOI] [PubMed] [Google Scholar]
- 92.Sorin Vera, Yagil Yael, Yosepovich Ady, Shalmon Anat, Gotlieb Michael, Neiman Osnat Halshtok, Sklair-Levy Miri. Contrast-Enhanced Spectral Mammography in Women With Intermediate Breast Cancer Risk and Dense Breasts. American Journal of Roentgenology. 2018;211(5):W267–W274. doi: 10.2214/AJR.17.19355. [DOI] [PubMed] [Google Scholar]
- 93.Bicchierai G, Nori J, De Benedetto D et al (2018) Role of contrast-enhanced spectral mammography in the post biopsy management of B3 lesions: preliminary results. Tumori J. [Epub ahead of print] [DOI] [PubMed]
- 94.Knogler Thomas, Homolka Peter, Hoernig Mathias, Leithner Robert, Langs Georg, Waitzbauer Martin, Pinker Katja, Leitner Sabine, Helbich Thomas H. Application of BI-RADS Descriptors in Contrast-Enhanced Dual-Energy Mammography: Comparison with MRI. Breast Care. 2017;12(4):212–216. doi: 10.1159/000478899. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 95.Kamal Rasha M, Helal Maha H, Mansour Sahar M, Haggag Marwa A, Nada Omniya M, Farahat Iman G, Alieldin Nelly H. Can we apply the MRI BI-RADS lexicon morphology descriptors on contrast-enhanced spectral mammography? The British Journal of Radiology. 2016;89(1064):20160157. doi: 10.1259/bjr.20160157. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 96.Lewin JM, Isaacs PK, Vance V, Larke FJ. Dual-energy contrast-enhanced digital subtraction mammography: feasibility. Radiology. 2003;229:261–268. doi: 10.1148/radiol.2291021276. [DOI] [PubMed] [Google Scholar]
- 97.Wang Q, Li K, Wang L, Zhang J, Zhou Z, Feng Y. Preclinical study of diagnostic performances of contrast-enhanced spectral mammography versus MRI for breast diseases in China. Springerplus. 2016;5:763. doi: 10.1186/s40064-016-2385-0. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 98.Cheung Yun-Chung, Juan Yu-Hsiang, Lin Yu-Ching, Lo Yung-Feng, Tsai Hsiu-Pei, Ueng Shir-Hwa, Chen Shin-Cheh. Dual-Energy Contrast-Enhanced Spectral Mammography: Enhancement Analysis on BI-RADS 4 Non-Mass Microcalcifications in Screened Women. PLOS ONE. 2016;11(9):e0162740. doi: 10.1371/journal.pone.0162740. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 99.Helal Maha, Abu Samra Manal F., Ibraheem Mohammed A., Salama Asmaa, Hassan Ebtesam Esmail, Hassan Nour El-Huda. Accuracy of CESM versus conventional mammography and ultrasound in evaluation of BI-RADS 3 and 4 breast lesions with pathological correlation. The Egyptian Journal of Radiology and Nuclear Medicine. 2017;48(3):741–750. doi: 10.1016/j.ejrnm.2017.03.004. [DOI] [Google Scholar]
- 100.Li L, Roth R, Germaine P, et al. Contrast-enhanced spectral mammography (CESM) versus breast magnetic resonance imaging (MRI): a retrospective comparison in 66 breast lesions. Diagn Interv Imaging. 2017;98:113–123. doi: 10.1016/j.diii.2016.08.013. [DOI] [PubMed] [Google Scholar]
- 101.Badr S, Laurent N, Régis C, Boulanger L, Lemaille S, Poncelet E. Dual-energy contrast-enhanced digital mammography in routine clinical practice in 2013. Diagn Interv Imaging. 2014;95:245–258. doi: 10.1016/j.diii.2013.10.002. [DOI] [PubMed] [Google Scholar]
- 102.Covington Matthew F., Pizzitola Victor J., Lorans Roxanne, Pockaj Barbara A., Northfelt Donald W., Appleton Catherine M., Patel Bhavika K. The Future of Contrast-Enhanced Mammography. American Journal of Roentgenology. 2018;210(2):292–300. doi: 10.2214/AJR.17.18749. [DOI] [PubMed] [Google Scholar]
- 103.Lancaster RB, Gulla S, De Los Santos J, Umphrey HR. Contrast-enhanced spectral mammography in breast imaging. Semin Roentgenol. 2018;53:294–300. doi: 10.1053/j.ro.2018.08.003. [DOI] [PubMed] [Google Scholar]
- 104.James JJ, Tennant SL. Contrast-enhanced spectral mammography (CESM) Clin Radiol. 2018;73:715–723. doi: 10.1016/j.crad.2018.05.005. [DOI] [PubMed] [Google Scholar]
- 105.Patel Bhavika K., Gray Richard J., Pockaj Barbara A. Potential Cost Savings of Contrast-Enhanced Digital Mammography. American Journal of Roentgenology. 2017;208(6):W231–W237. doi: 10.2214/AJR.16.17239. [DOI] [PubMed] [Google Scholar]
- 106.Lewin J. Comparison of contrast-enhanced mammography and contrast-enhanced breast MR imaging. Magn Reson Imaging Clin N Am. 2018;26:259–263. doi: 10.1016/j.mric.2017.12.005. [DOI] [PubMed] [Google Scholar]
- 107.Minsinger KD, Kassis HM, Block CA, Sidhu M, Brown JR. Meta-analysis of the effect of automated contrast injection devices versus manual injection and contrast volume on risk of contrast-induced nephropathy. Am J Cardiol. 2014;113:49–53. doi: 10.1016/j.amjcard.2013.08.040. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 108.Endrikat Jan, Barbati Ron, Scarpa Marcella, Jost Gregor, (Ned) Uber Arthur E. Accuracy and Repeatability of Automated Injector Versus Manual Administration of an MRI Contrast Agent—Results of a Laboratory Study. Investigative Radiology. 2018;53(1):1–5. doi: 10.1097/RLI.0000000000000403. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 109.Jost G, Endrikat J, Pietsch H. The impact of injector-based contrast agent administration on bolus shape and magnetic resonance angiography image quality. Magn Reson Insights. 2017;10:1178623X1770589. doi: 10.1177/1178623X17705894. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 110.Auler MA, Heagy T, Aganovic L, Brothers R, Costello P, Schoepf UJ. Saline chasing technique with dual-syringe injector systems for multi-detector row computed tomographic angiography: rationale, indications, and protocols. Curr Probl Diagn Radiol. 2006;35:1–11. doi: 10.1067/j.cpradiol.2005.10.001. [DOI] [PubMed] [Google Scholar]
- 111.Kidoh M, Nakaura T, Awai K, et al. Novel connecting tube for saline chaser in contrast-enhanced CT: the effect of spiral flow of saline on contrast enhancement. Eur Radiol. 2013;23:3213–3218. doi: 10.1007/s00330-013-2923-x. [DOI] [PubMed] [Google Scholar]
- 112.Perry N, Broeders M, de Wolf C, Tornberg S, Holland R, von Karsa L. European guidelines for quality assurance in breast cancer screening and diagnosis. Fourth edition--summary document. Ann Oncol. 2007;19:614–622. doi: 10.1093/annonc/mdm481. [DOI] [PubMed] [Google Scholar]
- 113.Wang Carolyn L., Cohan Richard H., Ellis James H., Caoili Elaine M., Wang George, Francis Isaac R. Frequency, Outcome, and Appropriateness of Treatment of Nonionic Iodinated Contrast Media Reactions. American Journal of Roentgenology. 2008;191(2):409–415. doi: 10.2214/AJR.07.3421. [DOI] [PubMed] [Google Scholar]
- 114.Mortelé Koenraad J., Oliva Maria-Raquel, Ondategui Silvia, Ros Pablo R., Silverman Stuart G. Universal Use of Nonionic Iodinated Contrast Medium for CT: Evaluation of Safety in a Large Urban Teaching Hospital. American Journal of Roentgenology. 2005;184(1):31–34. doi: 10.2214/ajr.184.1.01840031. [DOI] [PubMed] [Google Scholar]
- 115.Huston P, Moher D. Redundancy, disaggregation, and the integrity of medical research. The Lancet. 1996;347(9007):1024–1026. doi: 10.1016/S0140-6736(96)90153-1. [DOI] [PubMed] [Google Scholar]
- 116.Murphy L, Wyllie A. Duplicate patient data in a meta-analysis: a threat to validity. J Crit Care. 2009;24:466–467. doi: 10.1016/j.jcrc.2008.12.012. [DOI] [PubMed] [Google Scholar]
- 117.Sardanelli F, Alì M, Hunink MG, Houssami N, Sconfienza LM, Di Leo G. To share or not to share? Expected pros and cons of data sharing in radiological research. Eur Radiol. 2018;28:2328–2335. doi: 10.1007/s00330-017-5165-5. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Data Availability Statement
The datasets used and analysed during the current study are available from the corresponding author on reasonable request.