

Abstract
Purpose of review
Femoroacetabular impingement is a common cause of hip pain in young patients and has been shown to progress to osteoarthritis. The purpose of this review is to better understand the development of femoroacetabular impingement.
Recent findings
Recent literature shows little genetic transmission of FAI. However, molecular studies show strong similarities with the cartilage in osteoarthritis. The development of cam lesions has a strong association with sports participation, particularly at the time of physeal closure suggesting abnormal development. Lumbar, pelvis, and femoral biomechanics may also play an important role in dynamic impingement.
Summary
In summary, femoroacetabular impingement is a dynamic process with many influences. Further research is needed to clarify the pathophysiology of FAI development in hopes of finding preventative options to reduce symptoms and progression to osteoarthritis.
Keywords: Femoroacetabular impingement, FAI etiology, FAI pathomechanics, FAI pathophysiology, Cam development, Pincer development
Introduction
The concept of femoroacetabular impingement (FAI) was originally described as a femoral head-neck deformity and a major cause of hip osteoarthritis [1, 2]. The abnormal contact between the proximal femur and the acetabulum causes progressive chondrolabral injury potentially leading to osteoarthritis. Ganz proposed that this mechanical stress might be from excessive osteochondral extension at the anterolateral femoral neck, referred to as a cam lesion, or overcoverage of the acetabulum called a pincer lesion (Figs. 1 and 2) [3–5].
Fig. 1.

Cam lesions, identified by the arrows on the AP and frog leg lateral radiographs, are osteochondral extensions along the femoral head-neck junction
Fig. 2.

Pincer lesions, identified by the arrows on the AP pelvis radiograph, are over coverage of the acetabulum
Patients with FAI will often have considerable hip pain causing functional limitations. There is also later concern of the progression to severe osteoarthritis, but not all patients with cam or pincer lesions are symptomatic [6]. With the significant impact that FAI has on young patients and a projected increased rate of total hip arthroplasty to 4 million surgeries in the USA by 2030, it is important to better understand the cause of deformity and the related symptoms in an attempt to potentially prevent or alter the disease process [7].
Recent literature has focused on the underlying causes of FAI with links to specific genes, familial inheritance, and environmental factors particularly sports participation. The purpose of this review is to discuss the current theories and the supporting evidence on the development of femoroacetabular impingement.
Epidemiology
Femoroacetabular impingement is a common issue particularly in young and active patients, but the true prevalence of cam and pincer morphology is difficult to assess as it may or may not be associated with symptoms. As well, different criteria are frequently used to define FAI. A 2016 systematic review of thirty studies found a prevalence of cam deformity between 5 and 75% of the population [8•]. Despite this wide range in this case series and varying definitions of FAI, common findings among these studies are that males are more likely to have a higher alpha angle (Fig. 3), while females are more likely to have a higher lateral center-edge angle (Fig. 4). More recently, a prospective longitudinal cohort of 2596 patients found 25% of men and 10% of women had a cam lesion with an alpha angle > 60° and pincer deformity with lateral center-edge angle > 40° was present in 7% of men and 10% of women on AP radiographs [9•]. This is likely an underestimation of the prevalence of cam deformities as only AP radiographs were used to evaluate the alpha angle (Fig. 5).
Fig. 3.
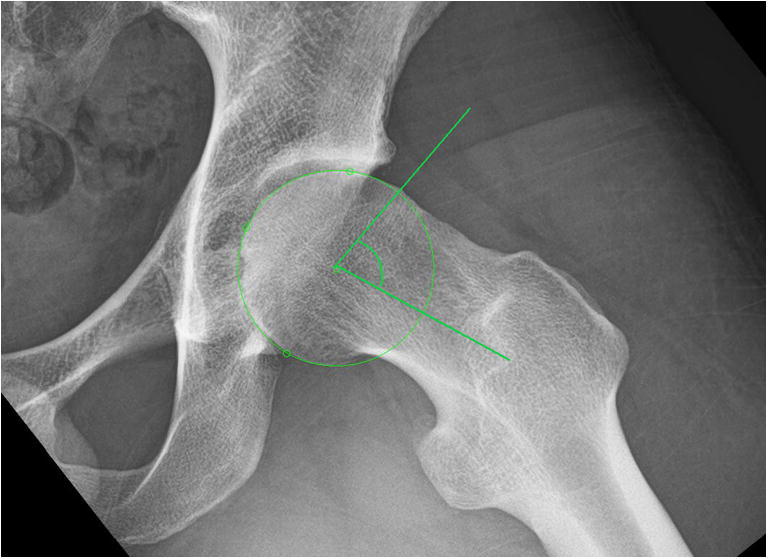
Measuring the alpha angle at 76.9° to evaluate for a cam lesion
Fig. 4.
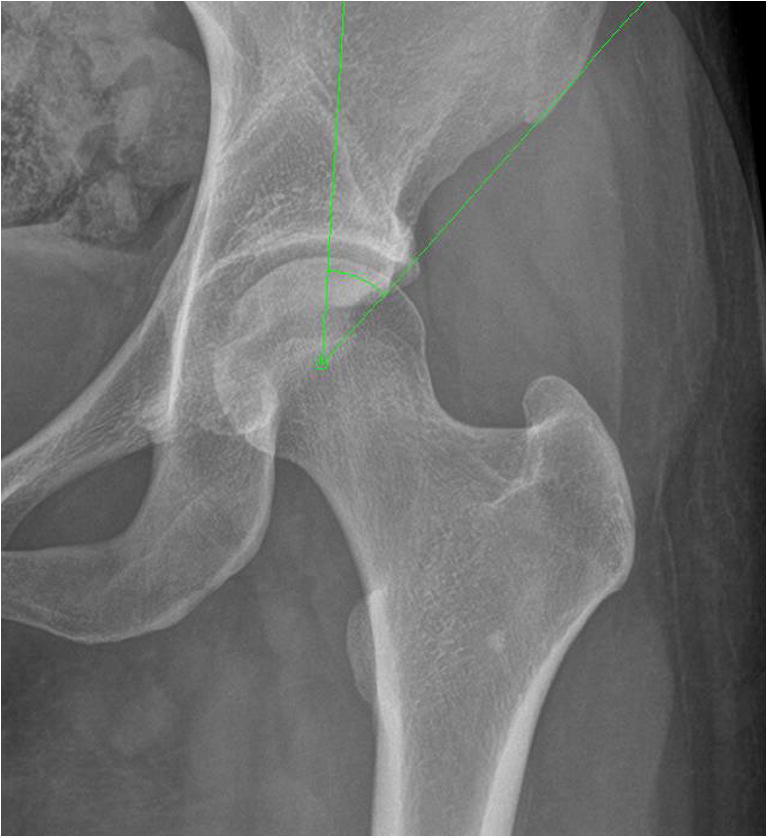
Measuring the lateral center edge angle at 32.9° to evaluate for a pincer lesion
Fig. 5.

AP and frog leg lateral radiographs of a patient’s right hip showing an anterior cam lesion with alpha angles of 44.5° on the AP and 64.4° on the lateral
Radiologic findings are common in the general population, but it is important to understand how often it causes pain. In the Netherlands, 17% of patients presenting to general healthcare professionals with hip pain were diagnosed with FAI [10]. Another population-based study of 20–49-year-old subjects compared those with and without hip pain [11]. Of the 500 study participants, 49% of subjects with hip pain and 44% of subjects without pain had cam and/or pincer morphology. The major risk factor for having hip pain in this cohort was an increase in level of physical activity measured by average energy expenditure.
To better understand the patients who are symptomatic, the characteristics of a North American cohort including 1076 patients undergoing surgery for FAI were examined [12]. This group was 55% female and 45% male with an average age of 28.4 years old and body mass index of 25.1. Cam morphology was most common as the predominant deformity at 47.6%. Combined cam and pincer lesions were the cause in 44.5% and sole pincer lesions in 7.9%. Over 90% of patients had concomitant labral and articular cartilage injury (Fig. 6).
Fig. 6.

Sagittal and coronal T2 MRI images identifying the chondrolabral injury due to femoroacetabular impingement
Genetics
Siblings of patients with symptomatic FAI had a 2.8 times increased risk of having cam lesions with alpha angles > 62.5° compared to spouses [13]. Similarly, siblings of patients with pincer lesions were two times more likely to have similar pathology. The parents of these FAI patients were nearly twice as likely to have osteoarthritis or total hip arthroplasty. There is clearly a strong familial association suggestive of a genetic link; however, environmental influences are a significant confounder. This study also suggests genetics may be involved in the development of symptoms and joint injury as siblings were more likely to have clinical symptoms of FAI compared to controls with the same radiographic morphology (relative risk = 2.5).
There have been specific genes associated with femoroacetabular impingement. The shape of the proximal femur has been correlated with single nucleotide polymorphisms (SNPs) of growth differentiation factor 5 (GDF5), Frizzled transmembrane receptor (FRZB) and deiodinase 2 (D2) [14]. These genes are important in the development of long bones and articular formation. However, Safran et al. found no difference in the SNP frequencies of GDF5 and FRZB compared to the general population in their pilot study [15].
Acetabular overcoverage has been associated with the genotype and allele frequencies of five HOXB9 SNPs (rs8844, rs3826541, rs3826540, rs7405887, rs79931349), while two HOXB9 SNPs were associated with decreased acetabular coverage (rs2303485, rs2303486) showing a strong involvement of HOXB9 in the morphogenesis of acetabulum coverage [16]. Despite several genes being implicated in the morphologic changes of femoroacetabular impingement, it has been postulated that it may be the cartilages vulnerability to these mechanical stresses that cause symptoms and possible progression to osteoarthritis [14].
Pathophysiology
The poroelastic properties of the cartilage at the cam impingement site have been studied to evaluate its structure and response to strain. When compared to cadaver controls, these osteochondral areas show 71% reduced stress-relaxation properties and three times increased permeability [17]. There is decreased proteoglycan concentration with similar fibrillary components. The authors concluded that cam lesions show behaviors and composition similar to osteoarthritis.
At the molecular level, Hashimoto et al. described the articular cartilage at the impingement zone in FAI hips to have high expression of inflammatory, anabolic, and catabolic genes [18]. When directly compared to the cartilage of patients with osteoarthritis undergoing total hip arthroplasty, the femoroacetabular impingement cartilage had elevated mRNA expression of inflammatory cytokines (interleukin-1 beta and interleukin-8) and catabolic genes (metalloproteinase 3 and a disintegrin and metalloproteinase with thrombospondin motifs-4) [19•]. These findings suggest that FAI is a hypermetabolic precursor to hip osteoarthritis.
Femoral and acetabular version
Most of the focus on FAI has been about the femoral head-neck deformity and acetabular coverage; however, more recently, the femoral and acetabular versions have been shown to impact patients. As impingement is a dynamic process through hip range of motion, it is logical that version may influence this motion. Increased femoral anteversion on MRI has been seen in patients with pincer-type FAI compared to cam-type (18.3°–18.7° vs. 10°–11.6°, respectively) [20]. This was also seen in Kraeutler et al.’s prospective study of 440 hips showing femoral version to be an independent predictor of hip internal rotation and cam lesions (alpha angle > 50° on CT) independently associated with decreased hip flexion [21]. This can provide some insight during the clinical assessment of ROM deficits.
Symptoms also correlate with version. A retrospective review of 538 painful hips found 5% with < 0° version and 12% > 35° of femoral anteversion [22]. Less femoral version was seen in cam-type deformity. Normal acetabular version, 10–25°, was most common among this symptomatic cohort (70% of patients) and there was much less variability in acetabular version compared to femoral version.
In 2013, Ejnisman et al. retrospectively reviewed 204 hips who underwent arthroscopy for FAI and found femoral version correlated with preoperative motion; version < 5° had increased external rotation. Femoral version > 15° was associated with larger labral tears at 38 mm and 2.2× more likely to have tears beyond 3 o’clock (more anterior tears), while patients with version < 5° tears had tears averaging 30 mm [23].
Spinopelvic influence
The motion of the lumbar spine and pelvis has a close relation with the hips, particularly in the sagittal plane. The trunk has been shown to have a significant influence on mechanical impingement at the hip. Patients with FAI have less spine flexion (22° ± 12° vs. 35° ± 8°, p = 0.04) and greater hip flexion (72° ± 6° vs. 62° ± 8°, p = .05) [24]. Symptomatic FAI patients also had less spine flexion with a similar amount of hip flexion as asymptomatic patients with cam lesions. FAI subjects required more hip flexion and pelvic tilt to sit to compensate for the lack of lumbar spine flexion potentially leading to more impingement and progression of symptoms.
A 2017 systematic review of pelvic posture and kinematics summarized that lower pelvic incidence is present in FAI patients reducing maximum pelvic back tilt and extenuating proximal femur and acetabulum engagement in dynamic hip flexion [25–27]. Patients with pincer lesions also had lower pelvic incidence than those with cam lesions [28]. Dynamically, the pelvis is seen to have less sagittal rotation while walking and cam impingement limits subjects from squatting as low as non-FAI subjects [29, 30]. Further study is needed to determine if these lumbar and pelvic differences are adaptive changes or causative.
Pincer development
Ponseti originally examined pediatric acetabulums in 1978 identifying the epiphyseal growth plates of the ilium, ischium, and pubis referring to these secondary ossification centers as os acetabuli [31]. Their maturation has been implicated in the development of pincer lesions. In addition to Sekimoto et al. identifying HOXB9’s role in acetabular coverage, recent clinical observations have evaluated the acetabulums morphology during growth. A retrospective review of 225 CT scans of subjects aged 2 to 19 years old revealed increased acetabular coverage and version with age [32].
A prospective look at asymptomatic volunteers aged 7 to 16 with multiple MRIs at least 1 year apart found increased acetabular version as physes went from open to close [33•]. However, no change in version was shown if physes remained open on the subsequent MRI or if the physes were closed on the initial MRI. This study suggests a narrow time frame when acetabular version changes. The increase in acetabular version is likely due to increased posterior acetabulum growth. CT scans of 10 asymptomatic pediatric patients aged 9–18 found greater acetabular anteversion in male and female subjects with closed physes because of increased posterior growth [34]. Therefore, acetabular retroversion may not be due to anterior overgrowth, but more likely under development of the posterior wall.
Cam development
Cam lesions are described as excess osteochondral extension at the head-neck junction causing a loss of sphericity and dynamic abutment of the acetabulum. This deformity is usually at the anterosuperior aspect of the proximal femur. Siebenrock et al. proposed that this lesion is the result of abnormal extension of the femoral head epiphysis due to the extension of the physeal scar in impingement patients not seen in controls [35]. This theory was tested in an animal model with a repetitive load applied to porcine hips [36]. The stresses lead to histological injury around the physes suggesting the potential for aberrant growth. The concept that the cam lesion is developed as the hip skeletally matures was corroborated on MRI of pediatric volunteers between ages 8 and 18. There was a moderate correlation between the physeal grade and alpha angles at the 1:30 and 3 o’clock positions in males, but no correlation in females [37]. However, much of our understanding of cam development comes from studying the hips of young athletes and this study did not report on the activity level of the participants.
Sports participation
Murray et al. first looked at athletic activity in adolescence as a risk factor for hip osteoarthritis in 1971 [38]. Using AP pelvis radiographs, there were increased femoral head ratios in boarding school males competing in aggressive sports versus those in voluntary sports. No increased femoral head ratios were found in Oka et al.’s 1976 study comparing runners, recreational athletes, and army recruits [39]. More recently, a high incidence of cam deformities has been noted in collegiate football and elite male soccer players [40, 41]. Ayeni et al. found a higher prevalence of cam lesions with an alpha angle > 50° in 16- to 30-year-old hockey players compared to controls, 55% vs. 25%, respectively [42].
Additional studies have looked at when the development of cam deformity occurs in sports participation. Siebenrock et al. retrospectively evaluated the proximal femur of basketball players finding an increased incidence of cam lesions compared to controls [43]. Interestingly, these increased alpha angles occurred after skeletal maturity because when this group was further analyzed based on the appearance of the physis, the immature basketball players had similar alpha angles to controls. When specifically looking at the hips of elite basketball players in Germany before and after physeal closure, they found abnormal physeal extension about the anterosuperior femoral neck in athletes with open physes with elevated alpha angles after physeal closure (61° vs. 49° in controls) [44]. This was also performed in youth hockey players finding increased alpha angles following physeal closure. The hockey players with hip pain had even higher alpha angles than asymptomatic players with radiographic signs of impingement [45].
Similarly, Philippon et al. found no difference in rates of cam deformities in asymptomatic youth hockey players compared with controls at a young age (57% vs. 56%, respectively), but increased alpha angles after skeletal maturity in 16 to 19-year-olds (93% vs. 25%, respectively) [46]. The biomechanics of the sprint start in hockey skating has also been identified as potential dynamic cause of impingement [47]. Soccer may not predispose athletes as much as basketball and hockey. Agricola et al. found a slightly higher prevalence of alpha angles > 60° in 89 soccer players when compared to controls; however, this was not statistically significant [48]. Johnson et al. likewise showed no difference in prevalence of cam lesions among elite soccer players [49]. When comparing skeletally immature soccer players to adult players, there was no difference in cam morphology prevalence [50]. A recent study found a 4° increase in alpha angles in English youth soccer players compared to non-athletic controls and 7.7° greater alpha angles in players competing at a national or international level [51]. Overall, Nepple et al.’s meta-analysis of level three evidence found athletes to have 1.9 to 8 times increased risk of developing a cam lesion [52•].
Hip morphology may also lead to instability in athletes. A small cohort of 12 males aged 12 to 16 with sports-related posterior hip dislocations was compared to matched controls with CTs showing higher alpha angles (means 55.5° vs. 4°, respectively) and less acetabular anteversion (9.6° ± 1.4° vs. 15.1° ± 0.8°) [53]. However, this is a small sample due to the rare occurrence of hip dislocation in this age group and it is unclear the level of sports participation of the control group.
Conclusion
Femoroacetabular impingement is a common problem, particularly among young athletes. There is sparse evidence to suggest a genetic inheritance pattern. The most compelling data centers on the development of cam lesions with high impact activity at the time of physeal closure. This window between skeletal immaturity and closure of the femoral head epiphysis appears to be when the cam deformity develops. It is unclear at the molecular level why this occurs or the amount of stress needed to cause the osteochondral extension. There is far less evidence on the cause of pincer impingement. Further research is needed to better understand the pathophysiology of FAI development particularly at the time of physeal closure in hopes of finding a preventative treatment to limit the symptoms and the progression to osteoarthritis.
Compliance with ethical standards
Conflict of interest
W. Jeffrey Grantham declares that he has no conflict of interest. Marc J. Philippon reports royalties from Smith & Nephew, Arthrosurface, Arthrex, Bledsoe, ConMed Linvatec, DonJoy, SLACK Inc., and Elsevier, consultancy fees from Smith & Nephew and MIS, and research support from Smith & Nephew, Ossur, Arthrex, and Siemens.
Human and animal rights and informed consent
This article does not contain any studies with human or animal subjects performed by any of the authors.
Footnotes
This article is part of the Topical Collection on Femoroacetabular Impingement/Labral Tears
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
References
Papers of particular interest, published recently, have been highlighted as: • Of importance
- 1.Murray RO. The aetiology of primary osteoarthritis of the hip. Br J Radiol. 1965;38(455):810–824. doi: 10.1259/0007-1285-38-455-810. [DOI] [PubMed] [Google Scholar]
- 2.Harris WH. Etiology of osteoarthritis of the hip. Clin Orthop Relat Res. 1986;213:20–33. [PubMed] [Google Scholar]
- 3.Beck M, Kalhor M, Leunig M, Ganz R. Hip morphology influences the pattern of damage to the acetabular cartilage: femoroacetabular impingement as a cause of early osteoarthritis of the hip. J Bone Joint Surg Br. 2005;87(7):1012–1018. doi: 10.1302/0301-620X.87B7.15203. [DOI] [PubMed] [Google Scholar]
- 4.Ganz R, Leunig M, Leunig-Ganz K, Harris WH. The etiology of osteoarthritis of the hip: an integrated mechanical concept. Clin Orthop Relat Res. 2008;466(2):264–272. doi: 10.1007/s11999-007-0060-z. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Ganz R, Parvizi J, Beck M, Leunig M, Notzli H, Siebenrock KA. Femoroacetabular impingement: a cause for osteoarthritis of the hip. Clin Orthop Relat Res. 2003;417:112–120. doi: 10.1097/01.blo.0000096804.78689.c2. [DOI] [PubMed] [Google Scholar]
- 6.Agricola R, Heijboer MP, Bierma-Zeinstra SM, Verhaar JA, Weinans H, Waarsing JH. Cam impingement causes osteoarthritis of the hip: a nationwide prospective cohort study (CHECK) Ann Rheum Dis. 2013;72(6):918–923. doi: 10.1136/annrheumdis-2012-201643. [DOI] [PubMed] [Google Scholar]
- 7.Maradit Kremers H, Larson DR, Crowson CS, Kremers WK, Washington RE, Steiner CA, et al. Prevalence of total hip and knee replacement in the United States. The Journal of bone and joint surgery American. 2015;97(17):1386–1397. doi: 10.2106/JBJS.N.01141. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.• Dickenson E, Wall PD, Robinson B, Fernandez M, Parsons H, Buchbinder R, et al. Prevalence of cam hip shape morphology: a systematic review. Osteoarthr Cartil. 2016;24(6):949–61. The systematic review of thirty studies looks at the prevalence of radiographic measures of femoroacetabular impingement noting a wide range in prevalance and significant biases in these studies. [DOI] [PubMed]
- 9.• Raveendran R, Stiller JL, Alvarez C, Renner JB, Schwartz TA, Arden NK, et al. Population-based prevalence of multiple radiographically-defined hip morphologies: the Johnston County Osteoarthritis Project. Osteoarthr Cartil. 2018;26(1):54–61. The study is the first large population-based prospective study of radiographic hip morphology prevalence. Cam morphology on AP radiographs was present in 25% of men and 10% of women while pincer morphology was present in 4.4% of men and 5.5% of women. [DOI] [PMC free article] [PubMed]
- 10.Roling MA, Mathijssen NM, Bloem RM. Incidence of symptomatic femoroacetabular impingement in the general population: a prospective registration study. J Hip Preserv Surg. 2016;3(3):203–207. doi: 10.1093/jhps/hnw009. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Kopec JA, Cibere J, Li LC, Zhang C, Barber M, Qian H, et al. Relationship between physical activity and hip pain in persons with and without cam or pincer morphology: a population-based case-control study. Osteoarthr Cartil. 2017;25(7):1055–1061. doi: 10.1016/j.joca.2017.02.795. [DOI] [PubMed] [Google Scholar]
- 12.Clohisy JC, Baca G, Beaule PE, Kim YJ, Larson CM, Millis MB, et al. Descriptive epidemiology of femoroacetabular impingement: a North American cohort of patients undergoing surgery. Am J Sports Med. 2013;41(6):1348–1356. doi: 10.1177/0363546513488861. [DOI] [PubMed] [Google Scholar]
- 13.Pollard TC, Villar RN, Norton MR, Fern ED, Williams MR, Murray DW, et al. Genetic influences in the aetiology of femoroacetabular impingement: a sibling study. J Bone Joint Surg Br. 2010;92(2):209–216. doi: 10.1302/0301-620X.92B2.22850. [DOI] [PubMed] [Google Scholar]
- 14.Hogervorst T, Eilander W, Fikkers JT, Meulenbelt I. Hip ontogenesis: how evolution, genes, and load history shape hip morphotype and cartilotype. Clin Orthop Relat Res. 2012;470(12):3284–3296. doi: 10.1007/s11999-012-2511-4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Safran MH, Smith LS. Paper 31: Is there a genetic link to FAI: A DNA pilot study of GDF5 and frizzle single nucleotide polymorphisms. Arthroscopy: the journal of arthroscopic & related surgery: official publication of the Arthroscopy Association of North America and the International Arthroscopy Association. 2011;27:e18. doi: 10.1016/j.arthro.2010.11.044. [DOI] [Google Scholar]
- 16.Sekimoto T, Kurogi S, Funamoto T, Ota T, Watanabe S, Sakamoto T, et al. Possible association of single nucleotide polymorphisms in the 3’ untranslated region of HOXB9 with acetabular overcoverage. Bone Joint Res. 2015;4(4):50–55. doi: 10.1302/2046-3758.44.2000349. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Speirs AD, Beaule PE, Huang A, Frei H. Properties of the cartilage layer from the cam-type hip impingement deformity. J Biomech. 2017;55:78–84. doi: 10.1016/j.jbiomech.2017.02.007. [DOI] [PubMed] [Google Scholar]
- 18.Hashimoto S, Rai MF, Gill CS, Zhang Z, Sandell LJ, Clohisy JC. Molecular characterization of articular cartilage from young adults with femoroacetabular impingement. J Bone Joint Surg Am. 2013;95(16):1457–1464. doi: 10.2106/JBJS.L.00497. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.• Chinzei N, Hashimoto S, Fujishiro T, Hayashi S, Kanzaki N, Uchida S, et al. Inflammation and degeneration in cartilage samples from patients with femoroacetabular impingement. J Bone Joint Surg Am. 2016;98(2):135–41. Gene expression from tissue samples of hips undergoing arthroscopy for FAI was compared to those undergoing total hip arthroplasty for osteoarthritis. There was elevated mRNA expression of inflammatory cytokines and catabolic genes in the cartilage of patients with FAI. [DOI] [PubMed]
- 20.Sutter R, Dietrich TJ, Zingg PO, Pfirrmann CW. Femoral antetorsion: comparing asymptomatic volunteers and patients with femoroacetabular impingement. Radiology. 2012;263(2):475–483. doi: 10.1148/radiol.12111903. [DOI] [PubMed] [Google Scholar]
- 21.Kraeutler MJ, Chadayammuri V, Garabekyan T, Mei-Dan O. Femoral version abnormalities significantly outweigh effect of cam impingement on hip internal rotation. J Bone Joint Surg Am. 2018;100(3):205–210. doi: 10.2106/JBJS.17.00376. [DOI] [PubMed] [Google Scholar]
- 22.Lerch TD, Todorski IAS, Steppacher SD, Schmaranzer F, Werlen SF, Siebenrock KA, et al. Prevalence of femoral and acetabular version abnormalities in patients with symptomatic hip disease: a controlled study of 538 hips. Am J Sports Med. 2018;46(1):122–134. doi: 10.1177/0363546517726983. [DOI] [PubMed] [Google Scholar]
- 23.Ejnisman L, Philippon MJ, Lertwanich P, Pennock AT, Herzog MM, Briggs KK, et al. Relationship between femoral anteversion and findings in hips with femoroacetabular impingement. Orthopedics. 2013;36(3):e293–e300. doi: 10.3928/01477447-20130222-17. [DOI] [PubMed] [Google Scholar]
- 24.Fader RR, Tao MA, Gaudiani MA, Turk R, Nwachukwu BU, Esposito CI, et al. The role of lumbar lordosis and pelvic sagittal balance in femoroacetabular impingement. Bone Joint J. 2018;100-B(10):1275–1279. doi: 10.1302/0301-620X.100B10.BJJ-2018-0060.R1. [DOI] [PubMed] [Google Scholar]
- 25.Pierannunzii L. Pelvic posture and kinematics in femoroacetabular impingement: a systematic review. J Orthop Traumatol: official journal of the Italian Society of Orthopaedics and Traumatology. 2017;18(3):187–196. doi: 10.1007/s10195-016-0439-2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Gebhart JJ, Streit JJ, Bedi A, Bush-Joseph CA, Nho SJ, Salata MJ. Correlation of pelvic incidence with cam and pincer lesions. Am J Sports Med. 2014;42(11):2649–2653. doi: 10.1177/0363546514548019. [DOI] [PubMed] [Google Scholar]
- 27.Weinberg DS, Gebhart JJ, Liu RW, Salata MJ. Radiographic signs of femoroacetabular impingement are associated with decreased pelvic incidence. Arthroscopy: the journal of arthroscopic & related surgery: official publication of the Arthroscopy Association of North America and the International Arthroscopy Association. 2016;32(5):806–813. doi: 10.1016/j.arthro.2015.11.047. [DOI] [PubMed] [Google Scholar]
- 28.Hellman MD, Haughom BD, Brown NM, Fillingham YA, Philippon MJ, Nho SJ. Femoroacetabular impingement and pelvic incidence: radiographic comparison to an asymptomatic control. Arthroscopy: the journal of arthroscopic & related surgery: official publication of the Arthroscopy Association of North America and the International Arthroscopy Association. 2017;33(3):545–550. doi: 10.1016/j.arthro.2016.08.033. [DOI] [PubMed] [Google Scholar]
- 29.Kennedy MJ, Lamontagne M, Beaule PE. Femoroacetabular impingement alters hip and pelvic biomechanics during gait walking biomechanics of FAI. Gait Posture. 2009;30(1):41–44. doi: 10.1016/j.gaitpost.2009.02.008. [DOI] [PubMed] [Google Scholar]
- 30.Lamontagne M, Kennedy MJ, Beaule PE. The effect of cam FAI on hip and pelvic motion during maximum squat. Clin Orthop Relat Res. 2009;467(3):645–650. doi: 10.1007/s11999-008-0620-x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Ponseti IV. Growth and development of the acetabulum in the normal child Anatomical, histological, and roentgenographic studies. J Bone Joint Surg Am. 1978;60(5):575–585. doi: 10.2106/00004623-197860050-00001. [DOI] [PubMed] [Google Scholar]
- 32.Monazzam S, Bomar JD, Dwek JR, Hosalkar HS, Pennock AT. Development and prevalence of femoroacetabular impingement-associated morphology in a paediatric and adolescent population: a CT study of 225 patients. Bone Joint J. 2013;95-B(5):598–604. doi: 10.1302/0301-620X.95B5.30118. [DOI] [PubMed] [Google Scholar]
- 33.• Albers CE, Schwarz A, Hanke MS, Kienle KP, Werlen S, Siebenrock KA. Acetabular version increases after closure of the triradiate cartilage complex. Clin Orthop Relat Res. 2017;475(4):983–94. The acetabulums of healthy children were evaluated for the state of the triradiate cartilage and acetabular version. There was significant increase in acetabular version on MRI between the time of open and closing of the physes. [DOI] [PMC free article] [PubMed]
- 34.Hingsammer AM, Bixby S, Zurakowski D, Yen YM, Kim YJ. How do acetabular version and femoral head coverage change with skeletal maturity? Clin Orthop Relat Res. 2015;473(4):1224–1233. doi: 10.1007/s11999-014-4014-y. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.Siebenrock KA, Wahab KH, Werlen S, Kalhor M, Leunig M, Ganz R. Abnormal extension of the femoral head epiphysis as a cause of cam impingement. Clin Orthop Relat Res. 2004;418:54–60. doi: 10.1097/00003086-200401000-00010. [DOI] [PubMed] [Google Scholar]
- 36.Jonasson PS, Ekstrom L, Hansson HA, Sansone M, Karlsson J, Sward L, et al. Cyclical loading causes injury in and around the porcine proximal femoral physeal plate: proposed cause of the development of cam deformity in young athletes. J Exp Orthop. 2015;2(1):6. doi: 10.1186/s40634-015-0022-4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37.Vo A, Beaule PE, Sampaio ML, Rotaru C, Rakhra KS. The femoral head-neck contour varies as a function of physeal development. Bone Joint Res. 2015;4(2):17–22. doi: 10.1302/2046-3758.42.2000356. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 38.Murray RO, Duncan C. Athletic activity in adolescence as an etiological factor in degenerative hip disease. J Bone Joint Surg Br. 1971;53(3):406–419. doi: 10.1302/0301-620X.53B3.406. [DOI] [PubMed] [Google Scholar]
- 39.Oka M, Hatanpaa S. Degenerative hip disease in adolescent athletes. Med Sci Sports. 1976;8(2):77–80. [PubMed] [Google Scholar]
- 40.Gerhardt MB, Romero AA, Silvers HJ, Harris DJ, Watanabe D, Mandelbaum BR. The prevalence of radiographic hip abnormalities in elite soccer players. Am J Sports Med. 2012;40(3):584–588. doi: 10.1177/0363546511432711. [DOI] [PubMed] [Google Scholar]
- 41.Kapron AL, Anderson AE, Aoki SK, Phillips LG, Petron DJ, Toth R, et al. Radiographic prevalence of femoroacetabular impingement in collegiate football players: AAOS Exhibit Selection. J Bone Joint Surg Am. 2011;93(19):e111(1–10). doi: 10.2106/JBJS.K.00544. [DOI] [PubMed] [Google Scholar]
- 42.Ayeni OR, Banga K, Bhandari M, Maizlin Z, de Sa D, Golev D, et al. Femoroacetabular impingement in elite ice hockey players. Knee Surg Sports Traumatol Arthroscopy: official journal of the ESSKA. 2014;22(4):920–925. doi: 10.1007/s00167-013-2598-5. [DOI] [PubMed] [Google Scholar]
- 43.Siebenrock KA, Ferner F, Noble PC, Santore RF, Werlen S, Mamisch TC. The cam-type deformity of the proximal femur arises in childhood in response to vigorous sporting activity. Clin Orthop Relat Res. 2011;469(11):3229–3240. doi: 10.1007/s11999-011-1945-4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 44.Siebenrock KA, Behning A, Mamisch TC, Schwab JM. Growth plate alteration precedes cam-type deformity in elite basketball players. Clin Orthop Relat Res. 2013;471(4):1084–1091. doi: 10.1007/s11999-012-2740-6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 45.Siebenrock KA, Kaschka I, Frauchiger L, Werlen S, Schwab JM. Prevalence of cam-type deformity and hip pain in elite ice hockey players before and after the end of growth. Am J Sports Med. 2013;41(10):2308–2313. doi: 10.1177/0363546513497564. [DOI] [PubMed] [Google Scholar]
- 46.Philippon MJ, Ho CP, Briggs KK, Stull J, LaPrade RF. Prevalence of increased alpha angles as a measure of cam-type femoroacetabular impingement in youth ice hockey players. Am J Sports Med. 2013;41(6):1357–1362. doi: 10.1177/0363546513483448. [DOI] [PubMed] [Google Scholar]
- 47.Stull JD, Philippon MJ, LaPrade RF. “At-risk” positioning and hip biomechanics of the Peewee ice hockey sprint start. Am J Sports Med. 2011;39(Suppl):29S–35S. doi: 10.1177/0363546511414012. [DOI] [PubMed] [Google Scholar]
- 48.Agricola R, Bessems JH, Ginai AZ, Heijboer MP, van der Heijden RA, Verhaar JA, et al. The development of Cam-type deformity in adolescent and young male soccer players. Am J Sports Med. 2012;40(5):1099–1106. doi: 10.1177/0363546512438381. [DOI] [PubMed] [Google Scholar]
- 49.Johnson AC, Shaman MA, Ryan TG. Femoroacetabular impingement in former high-level youth soccer players. Am J Sports Med. 2012;40(6):1342–1346. doi: 10.1177/0363546512439287. [DOI] [PubMed] [Google Scholar]
- 50.Monckeberg J, Amenabar T, Rafols C, Garcia N, Yanez R. Prevalence of FAI radiographic hip abnormalities in elite soccer players: are there differences related to skeletal maturity? BMJ Open Sport Exerc Med. 2016;2(1):e000162. doi: 10.1136/bmjsem-2016-000162. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 51.Palmer A, Fernquest S, Gimpel M, Birchall R, Judge A, Broomfield J, et al. Physical activity during adolescence and the development of cam morphology: a cross-sectional cohort study of 210 individuals. Br J Sports Med. 2018;52(9):601–610. doi: 10.1136/bjsports-2017-097626. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 52.• Nepple JJ, Vigdorchik JM, Clohisy JC. What is the association between sports participation and the development of proximal femoral cam deformity? A systematic review and meta-analysis. Am J Sports Med. 2015;43(11):2833–40. The systematic review evaluates nine studies showing evidence that high impact sports participation increases the risk of developing cam deformity at skeletal maturity. [DOI] [PubMed]
- 53.Mayer SW, Abdo JC, Hill MK, Kestel LA, Pan Z, Novais EN. Femoroacetabular impingement is associated with sports-related posterior hip instability in adolescents: a matched-cohort study. Am J Sports Med. 2016;44(9):2299–2303. doi: 10.1177/0363546516651119. [DOI] [PubMed] [Google Scholar]