

Abstract
Background:
Functional outcomes following J-pouch for ulcerative colitis have been studied, but lack standardization in which symptoms are reported. Furthermore, the selection of symptoms studied has not been patient-centered.
Objective:
Utilize a validated bowel function survey to determine which symptoms are present after J-pouch, and whether patients display a functional profile similar to Low Anterior Resection Syndrome.
Design:
Retrospective analysis of a prospectively maintained single center database
Settings:
Colorectal surgery center of a tertiary care academic hospital
Patients:
159 J-pouch patients, ≥6 months after ileostomy reversal
Main Outcome Measures:
Memorial Sloan Kettering Cancer Center Bowel Function Instrument; original Bowel Function Instrument validation cohort used as historical comparison (n=127)
Results:
The mean total Bowel Function Instrument score for the J-pouch cohort was 59.9+/−9.7 compared to a reported average score of 63.7+/−11.6 for low anterior resection patients in the validation cohort (p<0.001), indicating worse bowel function in J-pouch patients. When evaluating the Bowel Function Instrument subscales, J-pouch patients reported frequency subscale scores of 18.2+/−3.8, diet scores of 12.2+/−3.8, and urgency scores of 15.9+/−3.7, compared to 21.7+/−4.5 (p<0.001), 14.1+/−3.7 (p<0.001), and 15.0+/−3.9 (p=0.04) respectively for rectal resection patients. Furthermore, 90.4% of J-pouch patients state that they are sometimes, rarely, or never able to wait 15 minutes to get to the toilet. Additionally, 56.4% of patients report having another bowel movement within 15 minutes of the last bowel movement, sometimes, always, or most of the time, and 50.6% of patients say that they sometimes, rarely, or never feel like their bowels have been totally emptied after a bowel movement.
Limitations:
Single center study, Bowel Function Instrument only validated for rectal resection patients
Conclusions:
Patients that undergo J-pouch exhibit a constellation of bowel function symptoms that is more complex than fecal incontinence and frequency alone, despite the focus on these functional outcomes in the literature. See Video Abstract at http://links.lww.com/DCR/B73.
Keywords: Bowel function, Clustering, Urgency, Incomplete emptying, J-pouch, Ulcerative colitis
Abstract
ANTECEDENTES:
Se han estudiado los resultados funcionales después de la bolsa en J para la colitis ulcerosa, pero carecen de estandarización en la que se informen los síntomas. Además, la selección de los síntomas estudiados no se ha centrado en el paciente.
OBJETIVO:
Utilizar una encuesta validada de la función intestinal para determinar qué síntomas están presentes después de la bolsa en J y si los pacientes muestran un perfil funcional similar al síndrome de resección anterior baja.
DISEÑO:
Análisis retrospectivo de una base de datos de un solo centro mantenida prospectivamente.
AJUSTES:
Centro de cirugía colorrectal de un hospital académico de atención terciaria.
PACIENTES:
159 pacientes con bolsa en J, ≥6 meses después de la reversión de ileostomía.
PRINCIPALES MEDIDAS DE RESULTADO:
Instrumento para la función intestinal del “Memorial Sloan Kettering Cancer Center”; cohorte de validación original de instrumentos de función intestinal utilizada como comparación histórica (n = 127).
RESULTADOS:
La puntuación media total del instrumento de función intestinal para la cohorte de bolsa J fue 59.9 +/− 9.7 en comparación con un puntaje promedio reportado de 63.7 +/− 11.6 para pacientes con resección anterior baja en la cohorte de validación (p <0.001), lo que indica peor función intestinal en pacientes con bolsa en J. Al evaluar las subescalas del instrumento de función intestinal, los pacientes con bolsa en J informaron puntuaciones de subescala de frecuencia de 18.2 +/− 3.8, puntuaciones de dieta de 12.2 +/− 3.8 y puntuaciones de urgencia de 15.9 +/− 3.7, en comparación con 21.7 +/− 4.5 (p <0.001), 14.1 +/− 3.7 (p <0.001) y 15.0 +/− 3.9 (p = 0.04) respectivamente para pacientes con resección rectal. Además, el 90.4% de los pacientes con bolsa en J afirman que a veces, rara vez o nunca pueden esperar 15 minutos para llegar al baño. Además, el 56.4% de los pacientes reportan haber tenido otra evacuación intestinal dentro de los 15 minutos posteriores a la última evacuación intestinal, a veces, siempre o la mayor parte del tiempo, y el 50.6% de los pacientes dicen que a veces, rara vez o nunca sienten que sus intestinos han sido vaciados totalmente después de una evacuación intestinal.
LIMITACIONES:
Estudio en un solo centro, instrumento de función intestinal validado solo para pacientes con resección rectal
CONCLUSIONES:
Los pacientes que se someten a una bolsa en J exhiben una constelación de síntomas de la función intestinal que es más compleja que la incontinencia fecal y la frecuencia sola, a pesar del enfoque en estos resultados funcionales en la literatura. Vea el resumen del video en http://links.lww.com/DCR/B73.
INTRODUCTION
Since it was first described 40 years ago,1 the restorative proctocolectomy with ileal pouch-anal anastomosis (IPAA) in a J-pouch configuration has become the definitive procedure for patients with ulcerative colitis (UC) requiring surgery. Removal of the rectum inherently results in a loss of sensation and associated reservoir capacity, along with subsequent changes in bowel function. The ileoanal J-pouch was developed to re-create this lost reservoir physiology; however, despite a generally acceptable functional profile, it does not quite compensate for loss of patients’ native rectums. Although technical advances have led to improved postoperative and functional outcomes with overall patient satisfaction, the alteration in bowel habits after IPAA with J-pouch can be drastic and have a significant impact on a patient’s daily life.
Studies in the surgical literature focusing on outcomes after J-pouch creation frequently report on short and long-term bowel function as a measure of patient quality of life,2–5 but the field lacks standardization in the reporting of functional measures. The current literature is focused mostly on a defined set of measures deemed important by surgeons, particularly fecal incontinence (FI) and frequency of bowel movements. However, recent literature has shown that surgeons do not have an accurate understanding of what aspects of bowel function are most important to patients.6,7
In contrast, “Low Anterior Resection Syndrome” (LARS) after proctectomy for rectal cancer has been rigorously studied and validated, revealing a myriad of additional bowel dysfunction symptoms after removal of the rectum.8,9 Since UC patients undergo both proctectomy and total colectomy, their bowel symptoms are likely to be similar to patients with LARS, but more severe. At present, a complete understanding of which bowel symptoms are present in the population of patients with J-pouches is lacking, representing an essential gap in our knowledge that should be filled to better inform patients and manage expectations for outcomes after surgery. We hypothesized that J-pouch patients would display bowel dysfunction across a wide range of domains, beyond fecal incontinence and frequency of bowel movements. The aim of this study was to, therefore, utilize validated patient surveys to determine which bowel symptoms are present in J-pouch patients, and whether or not these patients display a functional profile similar to patients with LARS.
METHODS
Cohort
We conducted a retrospective study of a cohort of patients who underwent ileal pouch-anal anastomosis with J-pouch for ulcerative colitis at the Massachusetts General Hospital from September 2000 to June 2016, whose data were recorded in a prospectively-maintained institutional database. Inclusion criteria were diagnosis of UC, IPAA with J-pouch, and subsequent ileostomy reversal. Exclusion criteria were diagnosis of Crohn’s or indeterminate colitis (these patients were not entered into our UC database). At our institution, all J-pouch reconstructions are performed with a stapled anastomosis.
Survey tool
Surveys were sent to patients at least six months following ileostomy reversal, and included questions regarding general quality of life and patient-reported outcomes, including the Memorial Sloan-Kettering Cancer Center Bowel Function Instrument (MSKCC BFI).10,11 The MSKCC BFI was designed to measure bowel function after sphincter-preserving surgery for rectal cancer and includes several items focusing on LARS symptoms, such as fragmentation, clustering, urgency, and dietary changes.
The MSKCC investigators used factor analysis to group questions into three “subscales”: frequency (number of bowel movements, diarrhea, ability to delay bowel movement by 15 minutes, ability to get to toilet in time), dietary (do certain liquids or solids increase the number of bowel movements per day, has the patient limited liquids or solids to control their bowel movements), and urgency/soilage (daytime soilage, nighttime soilage, use of pads, altering activities because of bowel function).11 The MSKCC BFI’s accuracy in evaluating bowel function has been confirmed through stringent validation.10 Though the MSKCC BFI was developed for patients undergoing rectal cancer surgery, it has been used in the past to assess functional symptoms in patients who undergo colorectal resection for benign conditions.12,13 Calculated scores were compared to historical scores from the patient cohort undergoing sphincter sparing surgery for rectal cancer in the original MSKCC BFI validation (n=127).11
For patients who did not respond to the initial surveys, follow-up letters were mailed six weeks later in order to increase response rate. A translator phone number was provided for patients who did not speak English. This study was approved by the Institutional Review Board (Protocols #2008P002110 and #2011P001407).
Variable definitions
Demographic information that was recorded included body mass index (BMI), American Society of Anesthesiologists (ASA) score, and age-adjusted Charlson Comorbidity Index (CCI).14 The use of steroids, anti-tumor necrosis factor (TNF) agents (such as infliximab, golimumab, certolizumab, and adalimumab), and other immunomodulators (such as methotrexate, 6-mercaptopurine, azathioprine, cyclosporine, and tacrolimus) at the time of surgery were also recorded. An operation was considered urgent if the patient underwent surgery during an unplanned admission. Disease severity of the overall specimen and at the anastomosis, based on final pathology of the ring of tissue removed after firing the circular stapler, was determined by a board-certified pathologist.
Primary and secondary outcomes
Primary outcomes were individual answers to the MSKCC BFI questions, BFI subscale scores, and the BFI total score.
Secondary outcomes included perioperative (within 30 days of an operation) and late (>30 days after surgery) complications. Anastomotic leak was defined as radiologic evidence of extravasation of enteral contrast, reoperation with identification of anastomotic perforation, and pelvic abscess adjacent to anastomosis. Infectious complications included surgical site infection, urinary tract infection, pneumonia, and line infections. Ileus was defined as ≥3 days between the operation and tolerance of a solid diet.15 Thrombotic complications included line-associated thrombus, deep vein thrombosis, and pulmonary embolism. Pouchitis was defined as symptoms of pouchitis confirmed by inflammation on endoscopy and/or biopsy.16 Other late complications included abscess or fistula, anal stricture, incisional hernia, and small bowel obstruction (SBO). Pouch failure was defined as requiring ileostomy creation or pouch excision.
Statistical analysis
Variables were summarized as median (interquartile range (IQR)) or count (percentage) as appropriate. Statistical analysis was performed using Stata software, version SE 14.0 (StataCorp, College Station, TX, USA). Statistical significance was accepted at the p<0.05 level, and all tests were 2-sided.
RESULTS
Surveys were sent to 350 patients who underwent IPAA with J-pouch for UC and subsequent ileostomy reversal. There were 159 (45%) survey responders. The median time between ileostomy reversal and survey completion was 21.5 months (IQR 12.2–39.5 months).
Cohort demographics
Of the 159 patients in the cohort, the median age was 37 years (IQR 25–48) and 45.3% of patients were female (Table 1). Median BMI was 25.4 (IQR 21.8–28.0). Approximately 66.4% of patients were taking steroids at the time of colorectal resection, and resection was performed urgently in 39.2% of patients. Most patients had a two or three stage procedure (71.3% and 19.8%, respectively).
Table 1.
Patient demographics and disease characteristics of survey responders.
| Patient Demographics | Survey Responders (n=159) |
|---|---|
| Age (years), median (IQR) | 37 (25–48) |
| Female gender, N (%) | 72 (45.3%) |
| Race | |
| Body mass index (kg/m2), median (IQR) | 25.4 (21.8–28.0) |
| Current smoker, N (%) | 5 (3.6%) |
| Age-adjusted CCI ≥1, N (%) | 48 (34.3%) |
| ASA ≥3, N (%) | 18 (13.5%) |
| History of prior abdominal surgery, N (%) | 53 (33.5%) |
| Disease and Operative Characteristics | Survey Responders (n=159) |
| Steroid use at first operation, N (%) | 93 (66.4%) |
| Anti-TNF agent use at first operation, N (%) | 38 (27.1%) |
| Other immunomodulator use at first operation, N (%) | 47 (33.6%) |
| Indication for surgery | |
| Urgent procedure, N (%) | 51 (39.2%) |
| Laparoscopic procedure, N (%) | 37 (26.2%) |
| Two-stage IPAA, N (%) | 112 (71.3%) |
| Severe disease in specimen, N (%) | 104 (73.8%) |
| Severe disease in cuff, N (%) | 59 (44.0%) |
| Any disease in cuff, N (%) | 113 (84.3%) |
IQR: interquartile range; CCI: Charlson Comorbidity Index; ASA: American Society of Anesthesiologists; TNF: tumor necrosis factor; IPAA: ileal pouch-anal anastomosis
In terms of perioperative complications, 64.8% of patients had any perioperative complication (Table 2). The anastomotic leak rate was 10%. Late complications were also recorded; with a median follow-up time of 4.3 years (IQR 2.4–6.1 years), the rate of pouchitis was 43.8%, fistula or abscess was 12.1%, anal stricture was 13.6%, and pouch failure was 7.6%.
Table 2.
Perioperative and late outcomes after IPAA in survey responders.
| Perioperative Outcomes | Survey Responders (n=159) |
|---|---|
| Any perioperative complication, N (%) | 103 (64.8%) |
| Total perioperative complications per patient, after all stages, median (IQR) | 1 (0–2) |
| Anastomotic leak, N (%) | 14 (10.0%) |
| Other infections, N (%) | 23 (16.4%) |
| Thrombotic complications, N (%) | 7 (5.0%) |
| Ileus or SBO, N (%) | 56 (40.0%) |
| Postoperative length of stay (days) | |
| After IPAA, median (IQR) | 5 (4–8) |
| Total, median (IQR) | 10 (7–14) |
| Any readmission within 30 days of operation, N (%) | 48 (34.0%) |
| Total readmissions within 30 days of any operation, median (IQR) | 0 (0–1) |
| Late Outcomes | Survey Responders (n=159) |
| Follow-up time (years), median (IQR) | 4.3 (2.4–6.1) |
| Pouchitis | 56 (43.8%) |
| Fistula or abscess | 17 (12.1%) |
| Small bowel obstruction | 19 (14.4%) |
| Incisional hernia | 6 (4.6%) |
| Anal stricture | 18 (13.6%) |
| Pouch failure | 10 (7.6%) |
IPAA: ileal pouch-anal anastomosis; IQR: interquartile range; SBO: small bowel obstruction
MSKCC Bowel Function Instrument results
Individual questions from the MSKCC BFI revealed granular details about bowel function in patients with IPAA with J-pouch (Table 3). J-pouch patients reported a median of 8 bowel movements in 24 hours (IQR 6–10). Approximately 90.4% of patients state that they are sometimes, rarely, or never able to wait 15 minutes to get to the toilet (Figure 1). Furthermore, 56.4% of patients report that they have another bowel movement within 15 minutes of the last bowel movement, sometimes, always, or most of the time, and 50.6% of patients say that they sometimes, rarely, or never feel like their bowels have been totally emptied after a bowel movement. Over half of patients sometimes, rarely, or never know the difference between having to pass flatus versus have a bowel movement, and 43.9% of patients sometimes, rarely, or never are able to control the passage of gas.
Table 3.
Specific aspects of bowel function after IPAA and ileostomy reversal, based on the MSKCC BFI.
| MSKCC BFI Questions | N (%) |
|---|---|
| Number of BMs in 24 hours (median (IQR)) | 8 (6–10) |
| Certain solid foods increase # of BMs in a day - sometimes, always, or most of the time | 121 (77.1%) |
| Certain liquids increase # of BMs in a day - sometimes, always, or most of the time | 107 (68.2%) |
| Sometimes, rarely, or never feel like bowels have been totally emptied after a BM | 79 (50.6%) |
| Sometimes, rarely, or never get to the toilet on time | 14 (8.9%) |
| Have another BM within 15 minutes of last BM - sometimes, always, or most of the time | 88 (56.4%) |
| Sometimes, rarely, or never know the difference between having to pass gas and needing to have a BM | 79 (50.6%) |
| Used medicines to decrease # of BMs - sometimes, always, or most of the time | 104 (66.2%) |
| Had diarrhea (no form, watery stool) - sometimes, always, or most of the time | 126 (80.3%) |
| Had loose stool (slight form, but mushy) - sometimes, always, or most of the time | 145 (92.4%) |
| Sometimes, rarely, or never able to wait 15 minutes to get to the toilet | 142 (90.4%) |
| Sometimes, rarely, or never able to control the passage of gas | 69 (43.9%) |
| Limited the types of solid foods you eat to control BMs - sometimes, always, or most of the time | 98 (62.4%) |
| Limited the types of liquids you drink to control BMs - sometimes, always, or most of the time | 88 (56.1%) |
| Had soilage of undergarments during the day - sometimes, always, or most of the time | 29 (18.6%) |
| Used a tissue, napkin, and/or pad in undergarments during the day in case of stool leakage - sometimes, always, or most of the time | 37 (23.7%) |
| Had soilage of undergarments when you go to bed - sometimes, always, or most of the time | 43 (27.6%) |
| Had to alter activities because of bowel function - sometimes, always, or most of the time | 75 (47.8%) |
IPAA: ileal pouch-anal anastomosis; MSKCC BFI: Memorial Sloan-Kettering Cancer Center Bowel Function Instrument; BM: bowel movement; IQR: interquartile range
Figure 1.
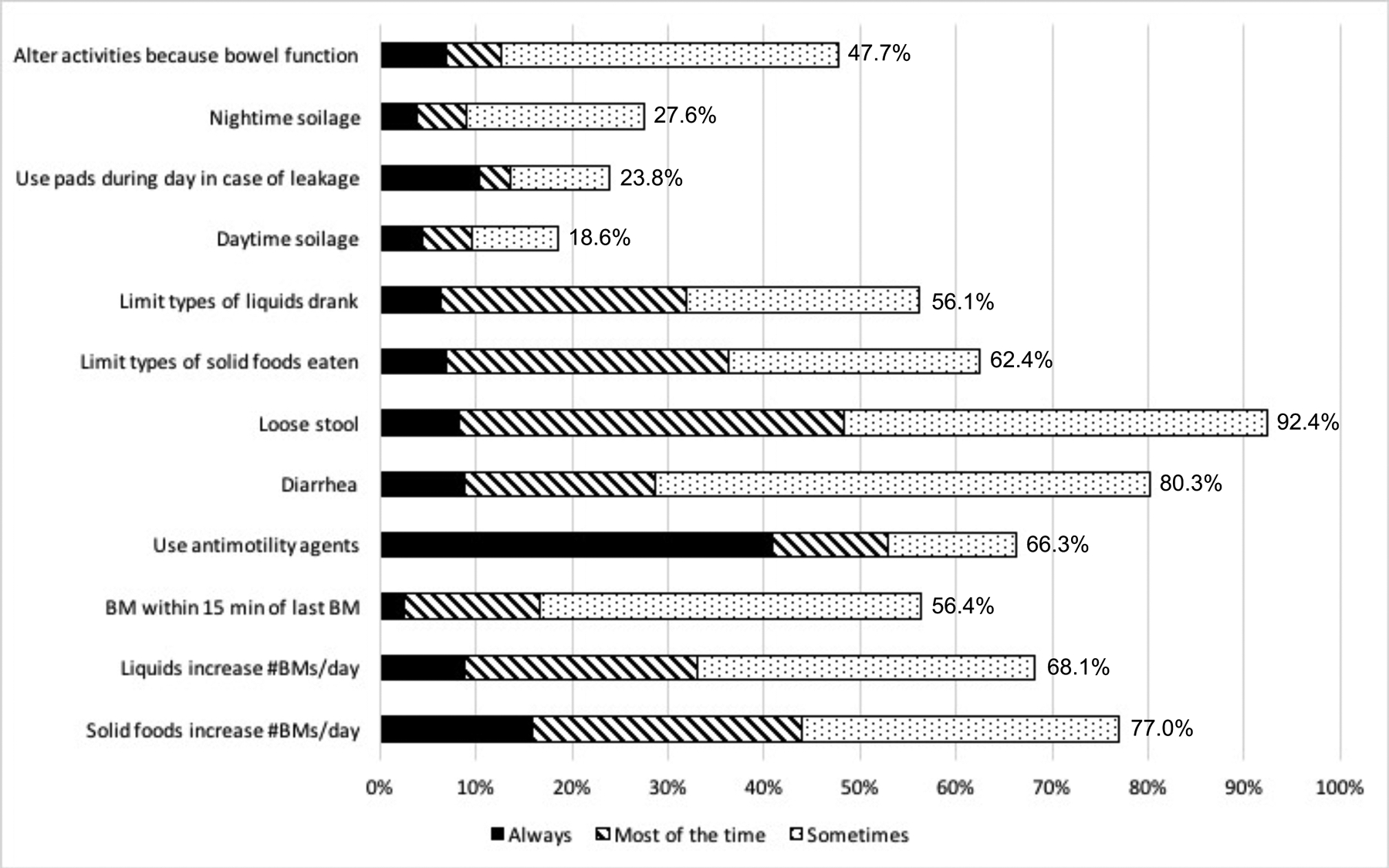
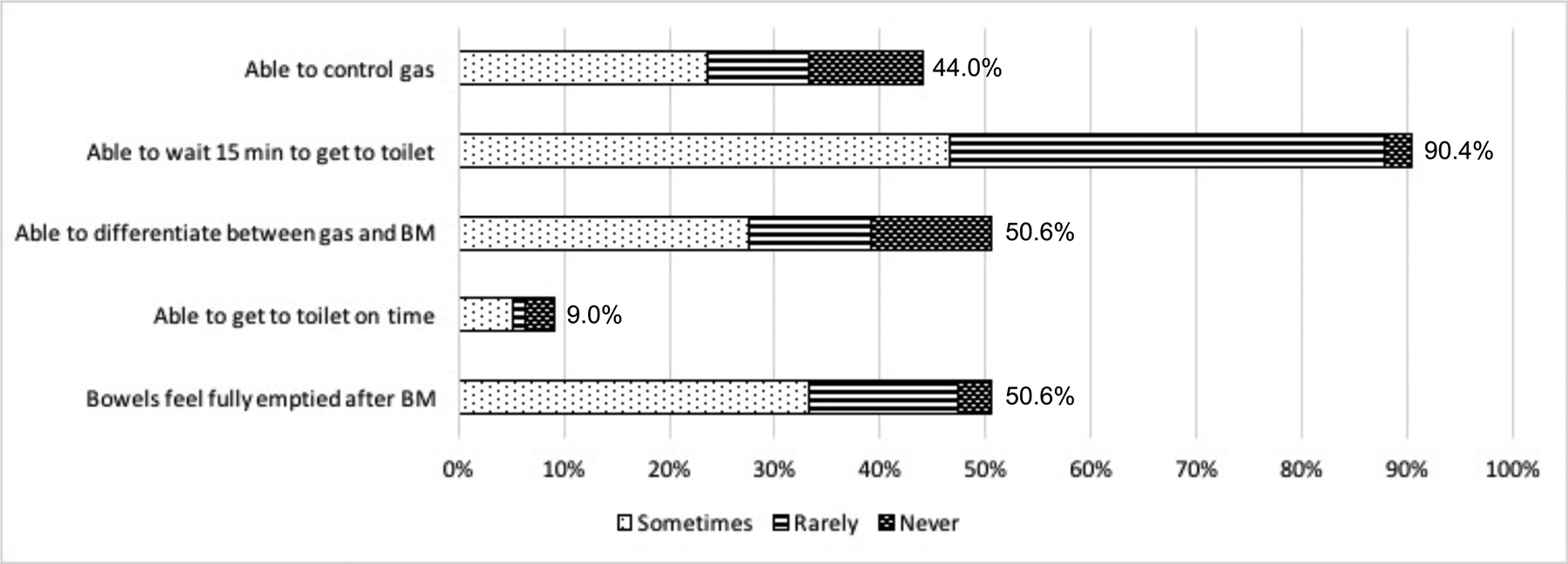
Responses to specific questions about bowel function using the MSKCC BFI, in patients after IPAA and ileostomy reversal. Higher percentages and longer bars imply worse function in both (A) and (B).
In our cohort of J-pouch patients, the mean total MSKCC BFI score was 59.9+/−9.7 (Table 4). In comparison, the patients with resected rectal cancer from the MSKCC BFI validation cohort (n=127) reported a mean score of 63.7+/−11.6, indicating worse bowel function in J-pouch patients (p<0.001). When evaluating the MSKCC BFI subscales, our J-pouch patients reported a mean frequency subscale score of 18.2+/−3.8 and diet score of 12.2+/−3.8, which also demonstrated worse bowel function compared to the rectal cancer group (frequency score 21.7+/−4.5 and diet score 14.1+/−3.7) (both p<0.001). In contrast, the mean urgency score of the J-pouch patients was 15.9+/−3.7, which compares favorably to that subset score in the rectal cancer patients (15.0+/−3.9, p=0.04).
Table 4.
Bowel function after IPAA and ileostomy reversal versus LAR, based on the MSKCC BFI.
| MSKCC BFI subscales | IPAA Cohort | LAR Cohorta | P-value |
|---|---|---|---|
| Frequency score (mean (SD)) | 18.2 (3.8) | 21.7 (4.5) | <0.001 |
| Diet score (mean (SD)) | 12.2 (3.8) | 14.1 (3.7) | <0.001 |
| Urgency/soilage score (mean (SD)) | 15.9 (3.7) | 15.0 (3.9) | 0.04 |
| Total score (sum of all scores) (mean (SD)) | 59.9 (9.7) | 63.7 (11.6) | <0.001 |
Data for the LAR cohort was abstracted from the MSKCC BFI validation study.11
IPAA: ileal pouch-anal anastomosis; LAR: low anterior resection; MSKCC BFI: Memorial Sloan-Kettering Cancer Center Bowel Function Instrument; SD: standard deviation
Quality of life results
In terms of quality of life (QOL), the majority of survey respondents stated that their QOL improved after J-pouch creation (Table 5). Specifically, 57.2% of patients said their QOL was much better after surgery and 25.7% reported that their QOL was somewhat better after surgery. When asked to rate their QOL at the time of survey completion compared to what they expected, their answers were more evenly distributed. Approximately 50.6% reported their QOL was somewhat or much better than expected, 21.8% stated that it was as expected, and 27.6% reported that it was somewhat or much worse than expected.
Table 5.
Quality of life results in patients who underwent IPAA and subsequent ileostomy reversal.
| Quality of life (QOL)-related questions | N (%) |
|---|---|
| How would you rate your QOL now compared to before your surgery? | |
| Much better | 87 (57.2%) |
| Somewhat better | 39 (25.7%) |
| Same | 6 (4.0%) |
| Somewhat worse | 14 (9.2%) |
| Much worse | 6 (4.0%) |
| How would you rate your QOL now compared to what you expected? | |
| Much better than expected | 44 (28.2%) |
| Somewhat better than expected | 35 (22.4%) |
| As expected | 34 (21.8%) |
| Somewhat worse than expected | 32 (20.5%) |
| Much worse than expected | 11 (7.1%) |
IPAA: ileal pouch-anal anastomosis; QOL: quality of life
DISCUSSION
This study of 159 patients with ulcerative colitis who underwent IPAA with J-pouch and subsequent ileostomy reversal demonstrates significant bowel dysfunction among a variety of subscales in the MSKCC BFI,11 which has not been previously described. Though the MSKCC BFI is only validated in patients who undergo rectal resection for malignancy, this tool provides a glimpse at the functional outcomes of patients who have J-pouches, and reveals that their bowel function is impacted in many ways beyond fecal incontinence and number of bowel movements.
Our data demonstrate that J-pouch patients have significantly worse total bowel function scores, as well as significantly worse frequency sub-scores and diet sub-scores, than patients who undergo proctectomy for cancer. While it is unclear if the mean difference of 4 points represents a clinically significant difference between groups, this difference could represent a change from “most of the time” to “sometimes”, or “sometimes” to “rarely” for 4 domains. Therefore, it may represent a clinically important change in function for individual patients and their quality of life.
The only sub-score in which our J-pouch cohort had improved function compared to the rectal resection cohort was the urgency score. However, 90.4% of our J-pouch patients still report that they are sometimes, rarely, or never able to wait 15 minutes to get to the toilet. Furthermore, 47.8% of our J-pouch patients had to alter their activities due to their bowel function. Additionally, the MSKCC BFI questions reveal notable problems with clustering after J-pouch (56.4% of patients) and incomplete emptying (50.6% of patients), two domains that are important to patients but may be drastically underappreciated by surgeons.6 The functional outcomes of our cohort are likely representative of other J-pouch cohorts as, for example, our 43.8% incidence of chronic pouchitis is consistent with that of other studies.17
It is important to acknowledge that despite the seemingly worse function in the J-pouch cohort when compared to the historical rectal cancer cohort, 83% of J-pouch patients rated that their quality of life improved after surgery. The quality of life improvement highlights that clinicians do not necessarily need to counsel patients that their bowel function after surgery will be debilitating, rather that it will be much different than before, and expectations can be accurately set.
A review of the literature uncovers a plethora of studies focusing on a set of functional outcomes chosen by clinicians who study J-pouch patients. Present in most evaluations of bowel function are parameters such as FI, 24-hour stool frequency, urgency, seepage, and the use of anti-diarrheals. Some studies include voidance postponement, anal irritation, and dietary restriction. Others attempt to quantify pouch function with clinically useful scoring systems. Two scores are widely reported in the literature. The Oresland score is a non-validated tool that was developed in 1989 by surgeons and has been utilized in a number of studies to analyze determinants of pouch dysfunction.18 A second score, the Pouch Function Score (PFS),19 was developed to assess pouch function using symptoms that correlate with the Cleveland Global Quality of Life (CGQL) score. Similar to the Oresland score, the starting list of symptoms used to derive the PFS was chosen by surgeons conducting the study and again includes 24-hour stool frequency, nocturnal stool frequency, FI, and the use of anti-diarrheal medications as the major domains comprising the score. There is one additional score, the Pouch Dysfunction Score (PDS), which was developed in Denmark, with functional domains ranked by 1,757 patients using a list generated by a combination of 6 expert surgeons and 10 randomly selected pouch patients; however, this score is not widely used and the initial list of symptoms was created without patient input and was not a complete catalogue of possible changes in bowel function.20 Table 6 summarizes the existing literature on bowel function after J-pouch.4,5,13,20–39
Table 6.
Summary of published literature on functional outcomes after IPAA with J-pouch.
| Author | Year | N | UC/FAP | Validated score? | Fecal Incontinence | Number of BMs/day | Clustering | Urgency | Dietary Changes | Evacuation issues | Anti-motility agents | Soilage/Pad usage | Pouchitis | Perianal skin irritation |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 2000 | 1,454 | UC | No | Yes | Yes | Yes | Yes | |||||||
| 2003 | 1,895 | 72% UC | No | Yes | Yes | Yes | Yes | Yes | ||||||
| 2004 | 409 | UC | No | Yes | Yes | Yes | Yes | Yes | ||||||
| 2008 | 345 | 60% UC | No | Yes | Yes | Yes | Yes | |||||||
| 2009 | 412 | 93% UC | Oresland | Yes | Yes | Yes | Yes | Yes | Yes | Yes | ||||
| 2009 | 179 | UC | No | Yes | Yes | Yes | Yes | Yes | Yes | |||||
| 2010 | 315 | 91% UC | No | Yes | Yes | Yes | Yes | Yes | Yes | |||||
| 2010 | 63 | UC | Global Assessment of Function Scale | Yes | Yes | Yes | Yes | Yes | Yes | |||||
| 2012 | 139 | UC | No | Yes | Yes | Yes | Yes | Yes | Yes | Yes | ||||
| 2013 | 1047 | UC | Developed score | Yes | Yes | Yes | Yes | Yes | Yes | Yes | ||||
| 2013 | 3707 | 80% UC | No | Yes | Yes | Yes | Yes | Yes | ||||||
| 2013 | 1047 | UC | Inflammatory Bowel Disease Questionnaire | Yes | Yes | Yes | Yes | Yes | Yes | |||||
| 2014 | 191 | UC | Oresland and PFS | Yes | Yes | Yes | Yes | Yes | Yes | Yes | ||||
| 2014 | 433 | 78% UC, 16% FAP, 5% CD | No | Yes | Yes | Yes | Yes | |||||||
| 2014 | 89 | UC | MSKCC BFI, FIQOL, FISI | Yes | Yes | Yes | Yes | Yes | ||||||
| 2016 | 4840 | UC | No | Yes | Yes | Yes | Yes | Yes | ||||||
| 2017 | 297 | UC | Colorectal Functional Outcome Questionnaire | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | ||
| 2017 | 448 | 50% UC | Cleveland Clinic pouch questionnaire | Yes | Yes | Yes | Yes | |||||||
| 2017 | 149 | UC | No | Yes | Yes | Yes | Yes | Yes | ||||||
| 2018 | 282 | UC | Oresland | Yes | Yes | Yes | Yes | Yes | Yes | Yes | ||||
| 2018 | 911 | UC | No | Yes | Yes | Yes | Yes | |||||||
| 2018 | 79 | UC | No | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | |||
| Dafnis39 | 2019 | 100 | 90% UC | St Mark’s incontinence score, Wexner score | Yes | Yes | Yes | Yes | Yes |
IPAA: ileal pouch-anal anastomosis; UC: ulcerative colitis; FAP: familial adenomatous polyposis; BM: bowel movement; CD: Crohn’s disease; PFS: Pouch Functional Score; MSKCC BFI: Memorial Sloan-Kettering Cancer Center Bowel Function Instrument; FIQOL: Fecal Incontinence Quality of Life; FISI: Fecal Incontinence Severity Index
Based on our data, patients that undergo IPAA with J-pouch exhibit a constellation of bowel function symptoms that is more complex than fecal incontinence and frequency alone, despite the focus on these specific outcomes in the literature. The identification of a large portion of pouch patients with symptoms that are not commonly studied begs the question: are patients experiencing additional dysfunction symptoms that we are simply not studying? It is evident from our survey responses that J-pouch patients experience clustering and incomplete evacuation; these symptoms have seldom been reported in J-pouch patients, but are clearly an important component of overall bowel function. This amalgamation of bowel function symptoms is analogous to LARS, and may represent a previously undescribed “Ileoanal J-pouch Syndrome.” Furthermore, this study highlights the similarity of rates of these symptoms with LAR patients and the need for recognition, definition, score development, monitoring and treatment of symptoms that J-pouch patients perceive to most affect quality of life.
It is critical to highlight that essentially all of the prior studies evaluating outcomes and creating scores for pouch function are hampered by two important limitations: (1) lack of standardized outcome measurements – the heterogeneity of outcomes reported limits effective analysis and comparison of techniques and leads to a high risk of reporting bias; and (2) more importantly, the selection of which outcomes are reported has been devoid of meaningful patient input. This is a major gap in the current surgical literature. Brandsborg et al. studied differences in perception of pouch dysfunction between clinicians and patients with striking results – clinicians performed no better than random probability at choosing the 5 most important symptoms to patients out of a list of 12 symptoms generated by patients.6 Clinicians tended to overestimate the importance of frequent bowel movements and seepage of stool, two of the most widely reported outcomes, while they underestimated the importance of urgency and incomplete evacuation. Furthermore, surgeons often focus on short-term technical outcomes, while patients focus on factors affecting long-term quality of life.40
Our study does have limitations. Although this was a prospective study, the cohort of patients were identified at a single academic medical center in the northeast United States and were operated on by specialized colorectal surgeons, therefore their functional outcomes may not be generalizable to the overall UC population. Furthermore, as previously stated, the MSKCC BFI is a survey that has been developed and validated for rectal cancer patients undergoing rectal resection, not in J-pouch patients. However, we believe that the tool has utility in identifying rarely-studied domains of bowel function in J-pouch patients, to lay the groundwork for creation of a consensus J-pouch syndrome score. We did not administer the MSKCC BFI questionnaire to our cohort of rectal cancer patients at the study institution, and we therefore are limited in comparing our J-pouch patients to historical cohorts.
Additionally, our survey response rate of 45% may have led to a response bias. However, we believe that our cohort accurately represents the pouch population, as we found similar complication and chronic pouchitis rates as described in the literature.17 Furthermore, we did not observe any differences in demographics, disease characteristics, or complications between survey responders and non-responders (p>0.05). Another limitation is that our study was underpowered to compare differences in bowel function based on complications, anastomotic leak, pouchitis, and time since IPAA and ileostomy takedown. After creating a consensus tool for evaluating bowel function after J-pouch, we hope to examine the relationship between these covariates and bowel function.
CONCLUSION
Taken together, it is clear that the outcomes used to define bowel function and dysfunction should not be determined unilaterally by surgeons, and the views of UC patients with J-pouches must be considered. Surgeons’ prior attempts to quantify outcomes after IPAA have likely been heavily influenced by our perceptions – as clinicians – of quality of life and measures of acceptable bowel function. It is time to investigate the aspects of bowel function that truly matter to our patients. We have been inspired by Tripartite 2020 Vision Project supported by the American Society of Colon and Rectal Surgeons (ASCRS), European Society of Coloproctology, Colorectal Surgical Society of Australia and New Zealand, and the Association of Coloproctology of Great Britain and Ireland to utilize a Delphi consensus process to incorporate patient and expert perspectives into a definition of LARS. The Surgery Research Network has been fortunate to receive support from the Crohn’s & Colitis Foundation and ASCRS to fund an effort to define the true range of bowel function after J-pouch based on a similar Delphi process, which will begin this year. By quantifying bowel function in a validated, consistent, patient-centered manner, we hope to provide clinicians and patients with a tool to help with the difficult decision of the appropriate time to perform a J-pouch.
Supplementary Material
{kind=link}
ACKNOWLEDGMENTS
We would like to thank Kevin Kennedy, who provided statistical support for this project.
Funding/Support: GCL and PMC are currently receiving support from an NIH T32 grant (Research Training in Alimentary Tract Surgery, DK007754-13). The authors have no conflicts of interests to report.
Footnotes
Podium presentation at the 2019 Annual Meeting of the American Society of Colon & Rectal Surgeons, June 1–5, 2019, Cleveland, OH.
REFERENCES
- 1.Parks AG, Nicholls RJ. Proctocolectomy without ileostomy for ulcerative colitis. BMJ. 1978;2:85–88. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Fazio VW, Ziv Y, Church JM, et al. Ileal pouch-anal anastomoses complications and function in 1005 patients. Ann Surg. 1995;222:120–127. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Fazio VW, O’Riordain MG, Lavery IC, et al. Long-term functional outcome and quality of life after stapled restorative proctocolectomy. Ann Surg. 1999;230:575–584. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.McKenna NP, Dozois EJ, Pemberton JH, Lightner AL. Impact of sex on 30-day complications and long-term functional outcomes following ileal pouch-anal anastomosis for chronic ulcerative colitis. Int J Colorectal Dis. 2018;33:619–625. [DOI] [PubMed] [Google Scholar]
- 5.Buck van Overstraeten A, Wolthuis AM, Vermeire S, et al. Long-term functional outcome after ileal pouch anal anastomosis in 191 patients with ulcerative colitis. J Crohn’s Colitis. 2014;8:1261–1266. [DOI] [PubMed] [Google Scholar]
- 6.Brandsborg S, Chen TY, Nicholls RJ, Laurberg S. Difference between patients’ and clinicians’ perception of pouch dysfunction and its impact on quality of life following restorative proctocolectomy. Colorectal Dis. 2015;17:O136–O140. [DOI] [PubMed] [Google Scholar]
- 7.Elfeki H, Thyø A, Nepogodiev D, et al. ; Colostomy Impact Score study group. Patient and healthcare professional perceptions of colostomy-related problems and their impact on quality of life following rectal cancer surgery. BJS Open. 2018;2:336–344. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Juul T, Ahlberg M, Biondo S, et al. International validation of the low anterior resection syndrome score. Ann Surg. 2014;259:728–734. [DOI] [PubMed] [Google Scholar]
- 9.Emmertsen KJ, Laurberg S. Low anterior resection syndrome score: development and validation of a symptom-based scoring system for bowel dysfunction after low anterior resection for rectal cancer. Ann Surg. 2012;255:922–928. [DOI] [PubMed] [Google Scholar]
- 10.Zotti P, Del Bianco P, Serpentini S, et al. Validity and reliability of the MSKCC Bowel Function instrument in a sample of Italian rectal cancer patients. Eur J Surg Oncol. 2011;37:589–596. [DOI] [PubMed] [Google Scholar]
- 11.Temple LK, Bacik J, Savatta SG, et al. The development of a validated instrument to evaluate bowel function after sphincter-preserving surgery for rectal cancer. Dis Colon Rectum. 2005;48:1353–1365. [DOI] [PubMed] [Google Scholar]
- 12.Lee GC, Deery SE, Kunitake H, et al. Comparable perioperative outcomes, long-term outcomes, and quality of life in a retrospective analysis of ulcerative colitis patients following 2-stage versus 3-stage proctocolectomy with ileal pouch-anal anastomosis. Int J Colorectal Dis. 2019;34:491–499. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Hicks CW, Hodin RA, Savitt L, Bordeianou L. Does intramesorectal excision for ulcerative colitis impact bowel and sexual function when compared with total mesorectal excision? Am J Surg. 2014;208:499–504.e4. [DOI] [PubMed] [Google Scholar]
- 14.St-Louis E, Iqbal S, Feldman LS, et al. Using the age-adjusted Charlson comorbidity index to predict outcomes in emergency general surgery. J Trauma Acute Care Surg. 2015;78:318–323. [DOI] [PubMed] [Google Scholar]
- 15.Livingston EH, Passaro EP Jr. Postoperative ileus. Dig Dis Sci. 1990;35:121–132. [DOI] [PubMed] [Google Scholar]
- 16.Lipman JM, Kiran RP, Shen B, Remzi F, Fazio VW. Perioperative factors during ileal pouch-anal anastomosis predict pouchitis. Dis Colon Rectum. 2011;54:311–317. [DOI] [PubMed] [Google Scholar]
- 17.Dalal RL, Shen B, Schwartz DA. Management of pouchitis and other common complications of the pouch. Inflamm Bowel Dis. 2018;24:989–996. [DOI] [PubMed] [Google Scholar]
- 18.Oresland T, Fasth S, Nordgren S, Hultén L. The clinical and functional outcome after restorative proctocolectomy. A prospective study in 100 patients. Int J Colorectal Dis. 1989;4:50–56. [DOI] [PubMed] [Google Scholar]
- 19.Lovegrove RE, Fazio VW, Remzi FH, Tilney HS, Nicholls RJ, Tekkis PP. Development of a pouch functional score following restorative proctocolectomy. Br J Surg. 2010;97:945–951. [DOI] [PubMed] [Google Scholar]
- 20.Brandsborg S, Nicholls RJ, Mortensen LS, Laurberg S. Restorative proctocolectomy for ulcerative colitis: development and validation of a new scoring system for pouch dysfunction and quality of life. Colorectal Dis. 2013;15:e719–e725. [DOI] [PubMed] [Google Scholar]
- 21.Farouk R, Pemberton JH, Wolff BG, Dozois RR, Browning S, Larson D. Functional outcomes after ileal pouch-anal anastomosis for chronic ulcerative colitis. Ann Surg. 2000;231:919–926. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Delaney CP, Fazio VW, Remzi FH, et al. Prospective, age-related analysis of surgical results, functional outcome, and quality of life after ileal pouch-anal anastomosis. Ann Surg. 2003;238:221–228. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Hahnloser D, Pemberton JH, Wolff BG, Larson DR, Crownhart BS, Dozois RR. The effect of ageing on function and quality of life in ileal pouch patients: a single cohort experience of 409 patients with chronic ulcerative colitis. Ann Surg. 2004;240:615–621. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Kiran RP, Remzi FH, Fazio VW, et al. Complications and functional results after ileoanal pouch formation in obese patients. J Gastrointest Surg. 2008;12:668–674. [DOI] [PubMed] [Google Scholar]
- 25.Block M, Börjesson L, Lindholm E, Oresland T. Pouch design and long-term functional outcome after ileal pouch-anal anastomosis. Br J Surg. 2009;96:527–532. [DOI] [PubMed] [Google Scholar]
- 26.Fichera A, Silvestri MT, Hurst RD, Rubin MA, Michelassi F. Laparoscopic restorative proctocolectomy with ileal pouch anal anastomosis: a comparative observational study on long-term functional results. J Gastrointest Surg. 2009;13:526–532. [DOI] [PubMed] [Google Scholar]
- 27.Wasmuth HH, Tranø G, Midtgård TM, Wibe A, Endreseth BH, Myrvold HE. Long-term function after ileal pouch-anal anastomosis - function does not deteriorate with time. Colorectal Dis. 2010;12:e283–e290. [DOI] [PubMed] [Google Scholar]
- 28.Tulchinsky H, Dotan I, Halpern Z, Klausner JM, Rabau M. A longitudinal study of quality of life and functional outcome of patients with ulcerative colitis after proctocolectomy with ileal pouch-anal anastomosis. Dis Colon Rectum. 2010;53:866–873. [DOI] [PubMed] [Google Scholar]
- 29.Karlbom U, Lindfors A, Påhlman L. Long-term functional outcome after restorative proctocolectomy in patients with ulcerative colitis. Colorectal Dis. 2012;14:977–984. [DOI] [PubMed] [Google Scholar]
- 30.Fazio VW, Kiran RP, Remzi FH, et al. Ileal pouch anal anastomosis: analysis of outcome and quality of life in 3707 patients. Ann Surg. 2013;257:679–685. [DOI] [PubMed] [Google Scholar]
- 31.Brandsborg S, Tøttrup A, Nicholls J, Laurberg S. Restorative proctocolectomy in patients with ulcerative colitis: a cross-sectional Danish population study on function and quality of life. Colorectal Dis. 2013;15:e453–e461. [DOI] [PubMed] [Google Scholar]
- 32.Ozdemir Y, Kiran RP, Erem HH, et al. Functional outcomes and complications after restorative proctocolectomy and ileal pouch anal anastomosis in the pediatric population. J Am Coll Surg. 2014;218:328–335. [DOI] [PubMed] [Google Scholar]
- 33.Ramage L, Qiu S, Georgiou P, Tekkis P, Tan E. Functional outcomes following ileal pouch-anal anastomosis (IPAA) in older patients: a systematic review. Int J Colorectal Dis. 2016;31:481–492. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34.van Gennep S, Sahami S, Buskens CJ, et al. Comparison of health-related quality of life and disability in ulcerative colitis patients following restorative proctocolectomy with ileal pouch-anal anastomosis versus anti-tumor necrosis factor therapy. Eur J Gastroenterol Hepatol. 2017;29:338–344. [DOI] [PubMed] [Google Scholar]
- 35.Jackson KL, Stocchi L, Duraes L, Rencuzogullari A, Bennett AE, Remzi FH. Long-term outcomes in indeterminate colitis patients undergoing ileal pouch-anal anastomosis: function, quality of life, and complications. J Gastrointest Surg. 2017;21:56–61. [DOI] [PubMed] [Google Scholar]
- 36.Baek SJ, Lightner AL, Boostrom SY, et al. Functional outcomes following laparoscopic ileal pouch-anal anastomosis in patients with chronic ulcerative colitis: long-term follow-up of a case-matched study. J Gastrointest Surg. 2017;21:1304–1308. [DOI] [PubMed] [Google Scholar]
- 37.Helavirta I, Hyöty M, Oksanen P, Huhtala H, Haapamäki J, Aitola P. Health-related quality of life after restorative proctocolectomy: a cross-sectional study. Scand J Surg. 2018;107:315–321. [DOI] [PubMed] [Google Scholar]
- 38.Watanabe K, Nagao M, Suzuki H, et al. The functional outcome and factors influencing the quality of life after ileal pouch anal anastomosis in patients with ulcerative colitis. Surg Today. 2018;48:455–461. [DOI] [PubMed] [Google Scholar]
- 39.Dafnis G. Functional outcome and quality of life after ileal pouch-anal anastomosis within a defined population in sweden. Dig Dis. 2019;37:1–10. [DOI] [PubMed] [Google Scholar]
- 40.McNair AG, Whistance RN, Forsythe RO, et al. Core outcomes for colorectal cancer surgery: a consensus study. PLoS Med. 2016;13:e1002071. [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.