

Abstract
This opinionated article reviews current concepts of myocardial ischemia. Specifically, the historical background is briefly presented. Then, the prevailing paradigm of myocardial oxygen-supply-demand imbalance is criticized since demand is a virtual parameter that cannot be measured and data on measurements of myocardial blood flow and contractile function rather support matching between flow and function. Finally, a concept of myocardial ischemia that focusses on the reduction of coronary blood flow to below 8–10 µl/g per beat with consequences for myocardial electrical, metabolic, contractile and morphological features is advocated.
Keywords: coronary blood flow, hibernation, myocardial infarction, myocardial ischemia, reperfusion, stunning
INTRODUCTION
Ischemic heart disease has become the most frequent cause of death worldwide in 2017 (11). In the Western world, the mortality from acute myocardial infarction has decreased over the last 2-3 decades, largely secondary to better interventional therapy and better medication (statins, ACE inhibitors/AT1 antagonists, and antiplatelet drugs), but it has not declined further over the most recent years and persists at a significant level (41, 52), i.e., at around 7% 1-year mortality in trials (12) and around 15% in large registries (54). From a clinical point of view, ischemic heart disease comprises acute myocardial infarction [ST segment elevation myocardial infarction (STEMI) and non-STEMI], stable angina, and ischemic cardiomyopathy. From a conceptual point of view, however, it is not so clear what myocardial ischemia is, other than that it concerns coronary blood flow and the myocardium. In most current textbooks of physiology, internal medicine, or cardiology, myocardial ischemia is defined as an imbalance between supply (of oxygen or of coronary blood flow) and demand (largely for contractile function). While this is an intuitive and persuasive definition, there are in fact a number of conceptual and factual problems with it.
David Hearse collected definitions of myocardial ischemia from a number of “eminent” clinicians and scientists 25 years ago (31), and these definitions varied from short and precise to more lengthy and sophisticated explanations, many of which elaborated on the relation of coronary blood flow to myocardial metabolism and the energetic demand of the myocardium to sustain its function. Hearse grouped my brief definition “myocardial ischemia is any reduction in blood flow that has functional and/or metabolic consequences for the affected myocardium” together with those of Eric Feigl and John Ross, and I felt and still feel very comfortable in that company. I also still stick to my definition from 25 years ago, and I dislike the more popular ideas about “supply-demand imbalance” (39).
HISTORICAL BACKGROUND
Historically, the term “ischemia” (ἰσχαιμία = withholding of blood) goes back to Rudolph Virchow, who in 1858 coined it to characterize reduced perfusion of an organ or tissue with its consequences (31). Of note, ischemia in its strictest sense defines lack of blood, not even blood flow. The Merriam-Webster Dictionary defines ischemia as “deficient supply of blood to the body part (such as the heart or brain) that is due to the obstruction of the inflow of arterial blood” (www.merriam-webster.com/dictionary/ischemia). As for the heart, John Erichsen in 1842 reported on experiments in rabbits and dogs where he observed the rapid cessation of cardiac contraction upon ligation of the coronary arteries (18). Julius Cohnheim in 1881 published experiments in dogs where he induced myocardial infarction by coronary artery ligation (51). Coronary obstruction as the cause of myocardial infarction in patients was established by James Herrick at the end of the nineteenth century (32). Whereas the causal relation of total cessation of coronary blood flow to myocardial infarction was easy to conclude, situations of repeated episodes of angina where the coronary circulation was compromised but not totally obstructed and where the consequences were obviously reversible were more difficult to conceptualize. Hermann Rein in the 1930s developed a technique to measure blood flow without opening the vessel (thermostromuhr), and using this technique in dogs, he found coronary blood flow closely related to cardiac output and not simply dependent on perfusion pressure (29). He proposed that coronary blood flow is adapted to cardiac function by coronary vasomotion. Franz Büchner in the 1950s to 1960s used a combination of reduced oxygen supply (hypoxia, anemia) with exercise in rabbits to induce patchy myocardial necrosis and fibrosis, as typically seen at autopsy in patients with ischemic heart disease. With respect to these experiments, Büchner first used the quantitative relation of coronary blood or oxygen supply to myocardial function as a definition of coronary sufficiency or insufficiency (34). In parallel, in the United States, Eugene Braunwald and his collaborators worked out the determinants of myocardial oxygen consumption (6); of note, they always used global heart preparations, and it was global oxygen consumption. Subsequently, Braunwald and his collaborators found infarct size from coronary artery occlusion in dogs increased, when the hemodynamic determinants of myocardial oxygen consumption were increased, notably by catecholamines, and conversely infarct size reduced when the hemodynamic determinants of myocardial oxygen consumption were decreased, e.g., by beta blockade (4, 60). From such data, Braunwald and collaborators derived and advocated the idea that the fate of myocardial tissue in the face of an obstructed coronary artery depends on the balance between myocardial oxygen supply and demand (5). Of note, this concept simply equates the oxygen consumption which is derived from global hemodynamics with the oxygen demand of the myocardial region which is dependent on the obstructed coronary artery. Many studies were published that reported reduced infarct size after favorable manipulation of the hemodynamic determinants of myocardial consumption and apparently confirmed the concept. However, on rigorous examination in a National Heart, Lung, Blood Institute cooperative study the idea of infarct size reduction by reducing myocardial oxygen consumption (verapamil) was not confirmed (73). More importantly, in an early clinical trial led by Braunwald, the beta blocker propranolol in patients with acute myocardial infarction reduced heart rate but did not reduce infarct size (74). Up until today, infarct size reduction by beta blockade in patients with acute myocardial infarction is equivocal (50, 53, 75), may depend on the specific beta blocker used rather than on reduced systemic hemodynamics, may occur during ischemia and/or during reperfusion when blood flow/supply is no longer limited, may involve complex cardioprotective signaling (40), and may not be related to effects on cardiomyocytes but on neutrophil stunning and attenuation of coronary microvascular obstruction (21). Nevertheless, following the authoritative view of Braunwald, the supply-demand paradigm was generalized from the situation of acute myocardial infarction to all ischemic heart disease and has become textbook knowledge. The paradigm of supply-demand is then often pictured as a scale.
I have never been comfortable with the oxygen supply-demand paradigm as the cornerstone criterion to define myocardial ischemia (31). Of course, oxygen supply can be measured as coronary blood flow × arterial oxygen content. However, myocardial oxygen demand is not a real, but a virtual parameter. What can be measured, is myocardial oxygen consumption (not demand), and all the estimations of myocardial consumption from hemodynamic determinants relate to global heart preparations and not to myocardial regions with truly reduced coronary blood flow. Thus, I find it far-fetched to assume that the demand of a myocardial region with reduced blood flow can be estimated from the hemodynamic determinants of myocardial oxygen consumption in a whole heart with normal or elevated coronary blood flow. As a side note, the picture of a scale is obsolete, because manipulation of one side of the scale moves the other side into the opposite direction: Why would reduced coronary blood flow/oxygen supply increase contractile function/oxygen demand?
THE CORONARY CIRCULATION PER SE
I have now criticized the oxygen supply-demand definition of myocardial ischemia. Can we define myocardial ischemia from coronary blood flow alone?
Coronary blood flow is determined by perfusion pressure and by coronary vasomotion, secondary to multiple vasomotor mechanisms, including autoregulatory/myogenic, metabolic, endothelial, and neurohumoral, as viewed in detail elsewhere (1, 10, 17, 22). Extravascular compression by the contracting myocardium renders coronary blood flow essentially a diastolic phenomenon, and extravascular compression is of particular importance in the inner myocardial layers at reduced perfusion pressure (9). Atherosclerosis impairs each of these regulatory mechanisms and eventually also physically obstructs the coronary circulation. Through autoregulation, coronary blood flow and contractile function are maintained at a plateau over a range of perfusion pressures and becomes pressure dependent below a pressure of around 40–50 mmHg after exhaustion of autoregulatory mechanisms (8). The level of the plateau and also the position of the left knee below which flow becomes pressure dependent are determined by myocardial metabolism (Fig. 1) (9, 67). The left knee below which flow becomes pressure dependent is markedly increased when endothelium-dependent vasomotion is eliminated by inhibition of nitric oxide synthesis (85). One could conceivably define myocardial ischemia as any situation where coronary blood flow is below the left knee of the autoregulatory curve and is pressure dependent. While such definition might be conceptually sound, on the basis of true rather than virtual data, and could be used on a regional level for a given coronary perfusion territory of an epicardial coronary artery, it would be very difficult to use such definition from a pragmatic point of view. One would have to determine at least the lower part of the autoregulatory curve and would also have to consider that the left knee of this curve will move (upward right with higher myocardial metabolism and with endothelial dysfunction, downward left with lower myocardial metabolism). With coronary atherosclerosis, the autoregulatory pressure-flow characteristics are further altered.
Fig. 1.
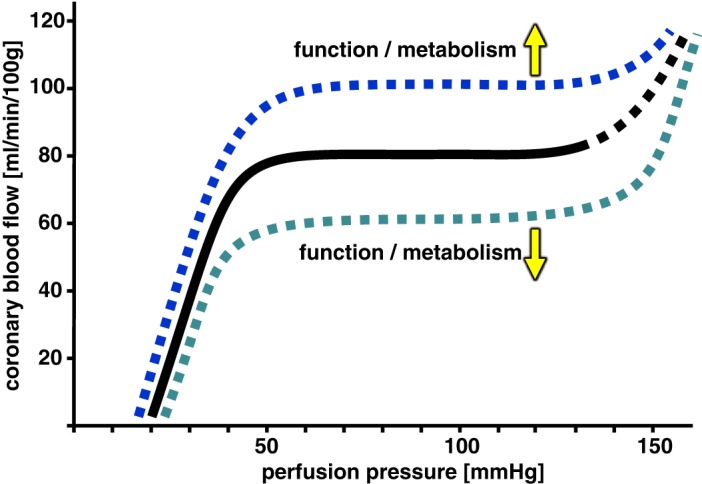
Relationship of coronary blood flow to perfusion pressure. There is an autoregulatory plateau that is shifted upward with increased cardiac function and metabolism and conversely shifted downward with decreased cardiac function and metabolism. Below a perfusion pressure of about 40-50 mmHg flow is pressure-dependent modified. Modified from Mosher et al. (67) with permission.
So, against this background, I am advocating my definition of myocardial ischemia as “any reduction in blood flow that has functional and/or metabolic consequences for the affected myocardium” from both a conceptual and a pragmatic point of view. What exactly are these consequences of reduced coronary blood flow?
ELECTRICAL ACTIVITY
Clearly, the action potential characteristics and the ECG change after reduction of coronary blood flow. However, ECG changes are difficult to interpret mechanistically. The detected changes do not only depend on the relative position of the “ischemic” myocardium to the respective ECG lead. It is also unclear which ECG parameter most sensitively detects “ischemia” and is proportionate to the reduction of coronary blood flow (55). Arrhythmias are a characteristic and often ominous consequence of myocardial ischemia (59).
METABOLISM
The myocardium uses the free-energy change from ATP hydrolysis to sustain its energy-consuming processes, i.e., ion pumps, contractile function, and maintenance of its structure by synthesis, degradation, and recycling processes. Thus, a reduced free-energy change from ATP hydrolysis reflects a lack of adequate energy supply to maintain myocardial functions. During steady-state conditions, such reduced free-energy change of ATP hydrolysis can be calculated from measurements of ATP, creatine phosphate, and inorganic phosphate in biopsies (61) or from nuclear magnetic resonance spectroscopy (25), but such measurements are sophisticated, tedious, and available only in a few centers, and they are certainly not on line with an acute reduction in coronary blood flow. A shift from aerobic to anaerobic glycolysis is more easy to assess from the arterio-coronary venous lactate concentration difference and net lactate production in severe myocardial ischemia. However, with more subtle and only regional ischemia, possibly only in subendocardial layers, net lactate production in some myocardial regions can be obscured by lactate uptake in other regions. A sophisticated lactate labeling technique is then required to ascertain regional myocardial ischemia from lactate production and to distinguish it from reduced lactate uptake in other areas (28).
CONTRACTILE FUNCTION
Within the autoregulatory range and above the left knee of the pressure-flow relationship, metabolic coronary vasodilation increases coronary blood flow in response to increased contractile function, i.e., flow follows function. The reverse causality, i.e., an increase in contractile function in response to increased coronary blood flow within the autoregulatory range (Gregg phenomenon), does not exist in the blood-perfused in situ mammal heart (78). Below the left knee of the pressure-flow relationship where flow is linearly related to perfusion pressure, function follows flow. In fact, there is a more or less linear relationship between regional contractile function, as assessed by sonomicrometry of systolic wall thickening or segment shortening, and regional myocardial blood flow, as assessed by microspheres, with progressive narrowing of an epicardial coronary artery (Fig. 2) (19, 20, 36, 80, 90). Importantly, the regional myocardial blood flow measurement with microspheres also reflects the result of any flow redistribution within the perfusion territory of an obstructed epicardial coronary artery, notably transmural redistribution to subepicardial layers at the expense of subendocardial layers and flow distribution along collaterals between ischemic and nonischemic myocardial regions, i.e., steal and reverse-steal phenomena (2). The geometric shape of the flow-function relationship varied somewhat in different studies. Canty found the relation between subendocardial blood flow and subendocardial segment shortening linear (8), whereas Vatner found it more exponential but again mostly linear at more severe blood flow reduction (90). Transmural contractile function is largely determined by subendocardial blood flow, and there may be subepicardial dysfunction at (near-)normal subepicardial blood flow, possibly through a tethering effect (87, 88). The relation of subendocardial and transmural blood flow to transmural wall thickening was consistently linear (8, 19, 20). Of note, a quantitative relation between regional myocardial blood flow and function can only be determined under steady-state conditions, since the microsphere measurements require steady-state conditions. After acute coronary occlusion or after the onset of exercise-induced ischemia, such steady state is reached after 2-3 minutes. There is therefore a transient early phase where regional contractile function has not completely ceased after coronary occlusion or where it is even increased after the onset of exercise in a perfusion territory with a severely obstructed coronary artery. No data exist for the quantitative relation between oxygen supply and oxygen consumption in such early transient phase of ischemia. I would assume, however, that the myocardium uses the physically dissolved and hemoglobin-bound oxygen in the capillaries, the intracellular myoglobin-bound oxygen and the intracellular energy-rich phosphate stores to sustain or even increase contractile function for a short period of time, and function declines as soon as these energy sources are depleted. A forced increase in contractile function in response to dobutamine accelerates the depletion on energy sources and precipitates contractile dysfunction (79, 80, 82). Thus, again there would be no energetic imbalance but possibly a short-lasting imbalance between oxygen supply by coronary blood flow and contractile function. The transient phase of 2–3 minutes after the onset of exercise probably corresponds to the time until the onset of symptoms in patients with stable angina. The more-or-less linear flow-function relationship that evolves after 2–3 minutes and is seen under steady-state conditions also holds when systemic and regional hemodynamics are largely altered by exercise, as long as both contractile function and blood flow are normalized for a single cardiac cycle, i.e., blood flow is expressed not per minute but divided by heart rate and expressed per beat (20). A reasonable number for a normal regional myocardial blood flow per cardiac cycle is 8–10 µl/g per beat. It is important to note that this is regional myocardial blood flow/perfusion but not epicardial coronary blood flow, and it therefore considers for transmural and/or collateral redistribution of blood flow (39). Even more subtle myocardial ischemia during exercise with only a mild epicardial coronary stenosis is then characterized by decreased blood flow per beat and decreased contractile function (57). Anti-ischemic drug interventions, e.g., by beta blockers (65), calcium antagonists (42, 63), combined beta blockers, calcium antagonists, and nitrates (27, 64), as well as bradycardic agents (23, 46), all operate along a consistent flow (per beat)-function relationship. Very different from the supply-demand paradigm, the attenuation of regional myocardial ischemia by beta blockade is then not explained by reduced demand but in fact not only by increased regional myocardial blood flow per beat but also increased regional myocardial blood flow per minute secondary to heart rate reduction (24, 65), and secondary to a redistribution of blood flow from the nonischemic myocardium that has reduced metabolic vasodilation in the face of beta blockade through collaterals into the ischemic myocardium (Fig. 3) (7). John Ross has termed such consistent linear flow-function relationship in ischemic myocardium “perfusion-contraction matching” (76). Such perfusion-contraction matching for which there is ample and robust experimental evidence firmly contradicts the idea of an imbalance between supply (perfusion) and oxygen consumption, which is largely determined by contractile function. The adaptive nature of the matching of contraction to the available perfusion is evidenced by the fact that contractile function can be artificially enhanced by inotropic stimulation but only briefly (79, 80). Perfusion-contraction matching can be sustained for many hours and is the main characteristic of short-term hibernation (Fig. 2) (45, 62, 81). Short-term hibernation is the mechanism behind the survival of some myocardium that can be rescued even after 24 hours from symptom onset of acute STEMI (68, 77).
Fig. 2:
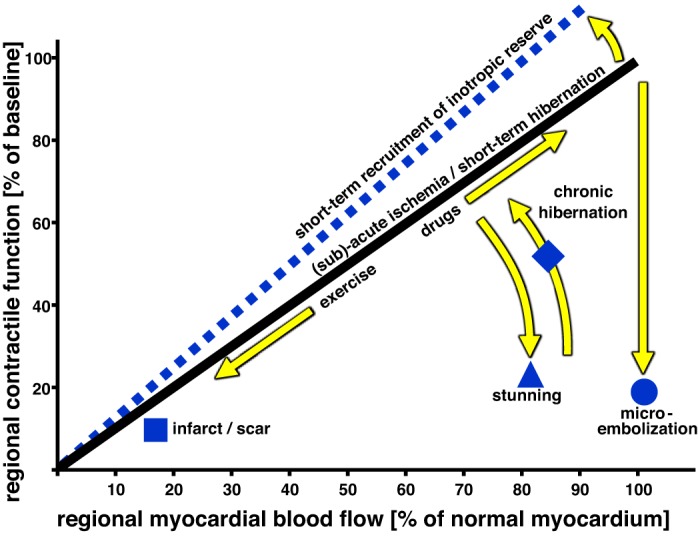
Relationship of regional contractile function to regional myocardial blood flow. There is an almost linear relationship between function and flow such that during exercise-induced ischemia both flow and function are proportionately reduced and conversely proportionately increased by drug treatment. This flow-function relationship can persist for hours during short-term hibernation and can only be briefly shifted upwards by inotropic stimulation. With stunning (postischemic contractile dysfunction) and microembolization, contractile function is decreased in the absence of a detectable flow reduction. With chronic hibernation which results from repetitive stunning, matching of flow and function is restored. From Heusch (36) with permission.
Fig. 3:

In both, nonischemic and ischemic myocardial regions flow and function are proportionately changed, e.g., by beta blockade. In the nonischemic region, beta blockade reduces heart rate and contractile function, and flow follows function by metabolic vasomotion. The ischemic myocardium receives more blood flow through the stenosis and through collaterals at reduced heart rate. Here, function follows flow. From Heusch (39) with permission.
MORPHOLOGY
The duration of cardiomyocyte survival in the face of reduced blood flow depends on the magnitude of flow reduction. With more severe blood flow reduction, cell death occurs, mostly through necrosis, but apoptosis and autophagy also participate in cell death (52, 58, 91). Cell death is not simply secondary to an energetic deficit with failure of ion pumps and cellular maintenance processes, but in fact cell survival and cell death are regulated by complex signaling cascades, involving the mitochondria, cytosolic kinases, and proteinases (37, 52). In fact, regardless of the level of flow reduction, myocardial infarct size can be reduced by ischemia-conditioning interventions, as long as there is eventual reperfusion (35).
TIME COURSE OF MYOCARDIAL CONSEQUENCES
Obviously, the time course of the above consequences of any blood flow reduction varies. Cell death is a final event and can only be detected several hours after the flow reduction (3). In my experience in dogs and pigs, electrical signs of myocardial ischemia, even when derived from the same sonomicrometry that is used for the measurement of regional contractile function, occur slower than the reduction of contractile function that becomes apparent only a few cardiac cycles after a sudden reduction in coronary blood flow. Measurements of myocardial metabolism require steady-state conditions, and data are not readily available. Thus, regional contractile function is best suited to serve as an on-line monitor of the consequences of coronary blood flow reduction (26).
CHRONIC HIBERNATION AND HEART FAILURE
More moderate, prolonged, or repeated brief episodes of coronary blood flow reduction will not affect myocardial viability but may nevertheless cause profound molecular and morphological rearrangements, e.g., in hibernating myocardium and ischemic cardiomyopathy (44, 45). The question of whether or not chronically hibernating myocardium is considered as “ischemic” is somewhat semantic in nature. Clearly, chronically hibernating myocardium has reduced blood flow and reduced blood flow per beat. The reduced blood flow is part of the substantial molecular, metabolic, and structural remodeling (58, 71, 72) that has developed in response to repetitive brief ischemia and reperfusion (16). The hibernating myocardium may have reached a new set point from which a short-lasting submaximal increase in blood flow and contractile function is possible in response to an inotropic challenge (16). Whether the absence of net lactate production during such brief inotropic challenge provides firm evidence against ischemia is questionable (see metabolism). From my personal perspective, chronically hibernating myocardium is ischemic: there is reduced blood flow in the perfusion territory of an obstructed coronary artery with molecular, metabolic, contractile, and structural consequences, and the appropriate treatment is reperfusion/revascularization.
In heart failure of nonischemic origin, myocardial contractile function, oxygen consumption, and blood flow remain also matched at rest and during exercise (89).
MYOCARDIAL ISCHEMIA AT SMALL SCALE
While on the regional level of an obstructed epicardial coronary artery and its perfusion territory, the consistent flow (per beat)-function relationship provides a solid measure of regional myocardial ischemia: the case is not closed. At a smaller regional scale, the situation is more difficult to assess, largely because measurement techniques for flow, function and metabolism are not available at a much smaller and matched scale such that their quantitative relationships cannot be determined. With coronary microembolization, as may occur after spontaneous or iatrogenic erosion/rupture of an epicardial coronary atherosclerotic plaque (43, 47), there will be a microinfarct in the obstructed microvascular territory with a more widespread contractile dysfunction secondary to an inflammatory reaction (14, 15) at an unchanged or even slightly elevated coronary blood flow, reflecting reactive hyperemia in the myocardium surrounding the microinfarct (Fig. 2) (33, 84). More recently, microvascular angina (70) and myocardial infarction (69) in the absence of visible epicardial coronary obstruction have come into the focus of attention. These microvascular ischemic scenarios often develop in the absence of detectable changes in systemic hemodynamics and are therefore probably best characterized as consequences of reduced blood flow at a microvascular level. On an even smaller scale, there is substantial heterogeneity of myocardial blood flow with matched glucose and oxidative metabolism under normal baseline conditions (13, 83), but the respective contractile function in such microregions is not known. Whether microregions with low flow and low oxidative metabolism reflect a state of hibernation under normal baseline conditions at a microlevel is also not known.
Whereas I have dealt so far with the consequences of reduced blood flow in the affected myocardium, the coronary circulation itself is also a target of ischemia. Reduced coronary blood flow results in endothelial dysfunction, enhanced vascular permeability, impaired vasomotion, and even capillary destruction acutely (38) and in vascular wall remodeling in response to prolonged epicardial coronary obstruction more chronically (66, 86). The acute consequences of ischemia in the coronary circulation are augmented and become manifest during reperfusion following ischemia and may induce a no-reflow situation despite a reopened epicardial coronary artery (30, 56). Even when coronary blood flow is normalized during reperfusion, contractile function remains reduced for a prolonged time until it has fully recovered, i.e., there is stunning (48, 49), which is characterized by a mismatch of perfusion and contraction (Fig. 2) (36).
In conclusion, a unifying and fully satisfying definition of myocardial ischemia that would characterize all different scenarios of ischemic heart disease does not yet exist. For the classical scenario of post-stenotic exercise-induced myocardial ischemia, the prevailing paradigm of a supply-demand imbalance is not substantiated by the experimental data since there is obvious perfusion-contraction matching. Therefore, at this point, the definition of myocardial ischemia as a lack of coronary blood flow (to below 8–10 µl/g per beat) with consequences for the myocardium and also the coronary circulation remains the most reasonable one. Consequences, however, are not limited to the contractile function, metabolism, and morphology, but may entail beyond the current energetic situation, signaling events and molecular rearrangements that pave the way for myocardial and coronary vascular repair and/or remodeling.
GRANTS
G. Heusch is supported by the German Research Foundation Grant SFB 1116, B08.
DISCLOSURES
No conflicts of interest, financial or otherwise, are declared by the author.
AUTHOR CONTRIBUTIONS
G.H. prepared figures and drafted, edited, revised, and approved final version of manuscript.
REFERENCES
- 1.Bassenge E, Heusch G. Endothelial and neuro-humoral control of coronary blood flow in health and disease. Rev Physiol Biochem Pharmacol 116: 77–165, 1990. doi: 10.1007/3540528806_4. [DOI] [PubMed] [Google Scholar]
- 2.Baumgart D, Ehring T, Heusch G, Heusch G. A proischaemic action of nisoldipine: relationship to a decrease in perfusion pressure and comparison to dipyridamole. Cardiovasc Res 27: 1254–1259, 1993. doi: 10.1093/cvr/27.7.1254. [DOI] [PubMed] [Google Scholar]
- 3.Bøtker HE, Hausenloy D, Andreadou I, Antonucci S, Boengler K, Davidson SM, Deshwal S, Devaux Y, Di Lisa F, Di Sante M, Efentakis P, Femminò S, García-Dorado D, Giricz Z, Ibanez B, Iliodromitis E, Kaludercic N, Kleinbongard P, Neuhäuser M, Ovize M, Pagliaro P, Rahbek-Schmidt M, Ruiz-Meana M, Schlüter KD, Schulz R, Skyschally A, Wilder C, Yellon DM, Ferdinandy P, Heusch G. Practical guidelines for rigor and reproducibility in preclinical and clinical studies on cardioprotection. Basic Res Cardiol 113: 39, 2018. doi: 10.1007/s00395-018-0696-8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Braunwald E, Maroko PR. The reduction of infarct size–an idea whose time (for testing) has come. Circulation 50: 206–209, 1974. doi: 10.1161/01.CIR.50.2.206. [DOI] [PubMed] [Google Scholar]
- 5.Braunwald E, Maroko PR. Limitation of infarct size. Curr Probl Cardiol 3: 10–51, 1978. doi: 10.1016/0146-2806(78)90025-7. [DOI] [PubMed] [Google Scholar]
- 6.Braunwald E, Sarnoff SJ, Case RB, Stainsby WN, Welch GH Jr. Hemodynamic determinants of coronary flow: effect of changes in aortic pressure and cardiac output on the relationship between myocardial oxygen consumption and coronary flow. Am J Physiol 192: 157–163, 1958. doi: 10.1152/ajplegacy.1957.192.1.157. [DOI] [PubMed] [Google Scholar]
- 7.Buck JD, Hardman HF, Warltier DC, Gross GJ. Changes in ischemic blood flow distribution and dynamic severity of a coronary stenosis induced by beta blockade in the canine heart. Circulation 64: 708–715, 1981. doi: 10.1161/01.CIR.64.4.708. [DOI] [PubMed] [Google Scholar]
- 8.Canty JM Jr. Coronary pressure-function and steady-state pressure-flow relations during autoregulation in the unanesthetized dog. Circ Res 63: 821–836, 1988. doi: 10.1161/01.RES.63.4.821. [DOI] [PubMed] [Google Scholar]
- 9.Canty JM Jr, Giglia J, Kandath D. Effect of tachycardia on regional function and transmural myocardial perfusion during graded coronary pressure reduction in conscious dogs. Circulation 82: 1815–1825, 1990. doi: 10.1161/01.CIR.82.5.1815. [DOI] [PubMed] [Google Scholar]
- 10.Chilian WM, Participants NW. Coronary microcirculation in health and disease. Summary of an NHLBI workshop. Circulation 95: 522–528, 1997. doi: 10.1161/01.CIR.95.2.522. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Collaborators on GBD 2017 Causes of Death . Global, regional, and national age-sex-specific mortality for 282 causes of death in 195 countries and territories, 1980-2017: a systematic analysis for the Global Burden of Disease Study 2017. Lancet 392: 1736–1788, 2018. doi: 10.1016/S0140-6736(18)32203-7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Cung TT, Morel O, Cayla G, Rioufol G, Garcia-Dorado D, Angoulvant D, Bonnefoy-Cudraz E, Guérin P, Elbaz M, Delarche N, Coste P, Vanzetto G, Metge M, Aupetit JF, Jouve B, Motreff P, Tron C, Labeque JN, Steg PG, Cottin Y, Range G, Clerc J, Claeys MJ, Coussement P, Prunier F, Moulin F, Roth O, Belle L, Dubois P, Barragan P, Gilard M, Piot C, Colin P, De Poli F, Morice MC, Ider O, Dubois-Randé JL, Unterseeh T, Le Breton H, Béard T, Blanchard D, Grollier G, Malquarti V, Staat P, Sudre A, Elmer E, Hansson MJ, Bergerot C, Boussaha I, Jossan C, Derumeaux G, Mewton N, Ovize M. Cyclosporine before PCI in patients with acute myocardial infarction. N Engl J Med 373: 1021–1031, 2015. doi: 10.1056/NEJMoa1505489. [DOI] [PubMed] [Google Scholar]
- 13.Deussen A, Flesche CW, Lauer T, Sonntag M, Schrader J. Spatial heterogeneity of blood flow in the dog heart. II. Temporal stability in response to adrenergic stimulation. Pflugers Arch 432: 451–461, 1996. doi: 10.1007/s004240050157. [DOI] [PubMed] [Google Scholar]
- 14.Dörge H, Neumann T, Behrends M, Skyschally A, Schulz R, Kasper C, Erbel R, Heusch G. Perfusion-contraction mismatch with coronary microvascular obstruction: role of inflammation. Am J Physiol Heart Circ Physiol 279: H2587–H2592, 2000. doi: 10.1152/ajpheart.2000.279.6.H2587. [DOI] [PubMed] [Google Scholar]
- 15.Dörge H, Schulz R, Belosjorow S, Post H, van de Sand A, Konietzka I, Frede S, Hartung T, Vinten-Johansen J, Youker KA, Entman ML, Erbel R, Heusch G. Coronary microembolization: the role of TNF-alpha in contractile dysfunction. J Mol Cell Cardiol 34: 51–62, 2002. doi: 10.1006/jmcc.2001.1489. [DOI] [PubMed] [Google Scholar]
- 16.Fallavollita JA, Malm BJ, Canty JM Jr. Hibernating myocardium retains metabolic and contractile reserve despite regional reductions in flow, function, and oxygen consumption at rest. Circ Res 92: 48–55, 2003. doi: 10.1161/01.RES.0000049104.57549.03. [DOI] [PubMed] [Google Scholar]
- 17.Feigl EO. Coronary physiology. Physiol Rev 63: 1–205, 1983. doi: 10.1152/physrev.1983.63.1.1. [DOI] [PubMed] [Google Scholar]
- 18.Fye WB. John Eric Erichsen. Clin Cardiol 20: 665–666, 1997. doi: 10.1002/clc.4960200716. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Gallagher KP, Matsuzaki M, Koziol JA, Kemper WS, Ross J Jr. Regional myocardial perfusion and wall thickening during ischemia in conscious dogs. Am J Physiol 247: H727–H738, 1984. doi: 10.1152/ajpheart.1984.247.5.H727. [DOI] [PubMed] [Google Scholar]
- 20.Gallagher KP, Matsuzaki M, Osakada G, Kemper WS, Ross J Jr. Effect of exercise on the relationship between myocardial blood flow and systolic wall thickening in dogs with acute coronary stenosis. Circ Res 52: 716–729, 1983. doi: 10.1161/01.RES.52.6.716. [DOI] [PubMed] [Google Scholar]
- 21.García-Prieto J, Villena-Gutiérrez R, Gómez M, Bernardo E, Pun-García A, García-Lunar I, Crainiciuc G, Fernández-Jiménez R, Sreeramkumar V, Bourio-Martínez R, García-Ruiz JM, Del Valle AS, Sanz-Rosa D, Pizarro G, Fernández-Ortiz A, Hidalgo A, Fuster V, Ibanez B. Neutrophil stunning by metoprolol reduces infarct size. Nat Commun 8: 14780, 2017. doi: 10.1038/ncomms14780. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Goodwill AG, Dick GM, Kiel AM, Tune JD. Regulation of Coronary Blood Flow. Compr Physiol 7: 321–382, 2017. doi: 10.1002/cphy.c160016. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Guth BD, Heusch G, Seitelberger R, Ross J Jr. Elimination of exercise-induced regional myocardial dysfunction by a bradycardiac agent in dogs with chronic coronary stenosis. Circulation 75: 661–669, 1987. doi: 10.1161/01.CIR.75.3.661. [DOI] [PubMed] [Google Scholar]
- 24.Guth BD, Heusch G, Seitelberger R, Ross J Jr. Mechanism of beneficial effect of beta-adrenergic blockade on exercise-induced myocardial ischemia in conscious dogs. Circ Res 60: 738–746, 1987. doi: 10.1161/01.RES.60.5.738. [DOI] [PubMed] [Google Scholar]
- 25.Guth BD, Martin JF, Heusch G, Ross J Jr. Regional myocardial blood flow, function and metabolism using phosphorus-31 nuclear magnetic resonance spectroscopy during ischemia and reperfusion in dogs. J Am Coll Cardiol 10: 673–681, 1987. doi: 10.1016/S0735-1097(87)80212-7. [DOI] [PubMed] [Google Scholar]
- 26.Guth BD, Schulz R, Heusch G. Time course and mechanisms of contractile dysfunction during acute myocardial ischemia. Circulation 87, Suppl: IV35–IV42, 1993. [PubMed] [Google Scholar]
- 27.Guth BD, Tajimi T, Seitelberger R, Lee JD, Matsuzaki M, Ross J Jr. Experimental exercise-induced ischemia: drug therapy can eliminate regional dysfunction and oxygen supply-demand imbalance. J Am Coll Cardiol 7: 1036–1046, 1986. doi: 10.1016/S0735-1097(86)80221-2. [DOI] [PubMed] [Google Scholar]
- 28.Guth BD, Wisneski JA, Neese RA, White FC, Heusch G, Mazer CD, Gertz EW. Myocardial lactate release during ischemia in swine. Relation to regional blood flow. Circulation 81: 1948–1958, 1990. doi: 10.1161/01.CIR.81.6.1948. [DOI] [PubMed] [Google Scholar]
- 29.Hansson N, Daan S. Politics and physiology: Hermann Rein and the Nobel Prize 1933-1953. J Physiol 592: 2911–2914, 2014. doi: 10.1113/jphysiol.2014.273847. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Hausenloy DJ, Chilian W, Crea F, Davidson SM, Ferdinandy P, Garcia-Dorado D, van Royen N, Schulz R, Heusch G. The coronary circulation in acute myocardial ischaemia/reperfusion injury - a target for cardioprotection. Cardiovasc Res, 2018. doi: 10.1093/cvr/cvy286. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Hearse DJ. Myocardial ischaemia: can we agree on a definition for the 21st century? Cardiovasc Res 28: 1737–1744, 1994. doi: 10.1093/cvr/28.12.1737. [DOI] [PubMed] [Google Scholar]
- 32.Herrick JB. Clinical features of sudden obstruction of the coronary arteries. J Am Med Assoc 59: 2015–2020, 1912. doi: 10.1001/jama.1912.04270120001001. [DOI] [PubMed] [Google Scholar]
- 33.Herrmann J, Haude M, Lerman A, Schulz R, Volbracht L, Ge J, Schmermund A, Wieneke H, von Birgelen C, Eggebrecht H, Baumgart D, Heusch G, Erbel R. Abnormal coronary flow velocity reserve after coronary intervention is associated with cardiac marker elevation. Circulation 103: 2339–2345, 2001. doi: 10.1161/01.CIR.103.19.2339. [DOI] [PubMed] [Google Scholar]
- 34.Heusch B, Guth BD, Heusch G. A brief history of angina pectoris: Change of concepts and ideas. In: Pathophysiology and Rational Pharmacotherapy of Myocardial Ischemia, ed. Heusch G. Darmstadt, Germany/New York: Steinkopff/Springer, 1990. [Google Scholar]
- 35.Heusch G. Cardioprotection: chances and challenges of its translation to the clinic. Lancet 381: 166–175, 2013. doi: 10.1016/S0140-6736(12)60916-7. [DOI] [PubMed] [Google Scholar]
- 36.Heusch G. The regional myocardial flow-function relationship: a framework for an understanding of acute ischemia, hibernation, stunning and coronary microembolization. 1980. Circ Res 112: 1535–1537, 2013. doi: 10.1161/CIRCRESAHA.113.301446. [DOI] [PubMed] [Google Scholar]
- 37.Heusch G. Molecular basis of cardioprotection: signal transduction in ischemic pre-, post-, and remote conditioning. Circ Res 116: 674–699, 2015. doi: 10.1161/CIRCRESAHA.116.305348. [DOI] [PubMed] [Google Scholar]
- 38.Heusch G. The coronary circulation as a target of cardioprotection. Circ Res 118: 1643–1658, 2016. doi: 10.1161/CIRCRESAHA.116.308640. [DOI] [PubMed] [Google Scholar]
- 39.Heusch G. Myocardial ischemia: Lack of coronary blood flow or myocardial oxygen supply/demand imbalance? Circ Res 119: 194–196, 2016. doi: 10.1161/CIRCRESAHA.116.308925. [DOI] [PubMed] [Google Scholar]
- 40.Heusch G. There is more to beta-blockade than just blockade of beta-receptors: A case for cardioprotective cross-signaling. J Am Coll Cardiol 70: 193–195, 2017. doi: 10.1016/j.jacc.2017.05.017. [DOI] [PubMed] [Google Scholar]
- 41.Heusch G, Gersh BJ. The pathophysiology of acute myocardial infarction and strategies of protection beyond reperfusion: a continual challenge. Eur Heart J 38: 774–784, 2017. doi: 10.1093/eurheartj/ehw224. [DOI] [PubMed] [Google Scholar]
- 42.Heusch G, Guth BD, Seitelberger R, Ross J Jr. Attenuation of exercise-induced myocardial ischemia in dogs with recruitment of coronary vasodilator reserve by nifedipine. Circulation 75: 482–490, 1987. doi: 10.1161/01.CIR.75.2.482. [DOI] [PubMed] [Google Scholar]
- 43.Heusch G, Kleinbongard P, Böse D, Levkau B, Haude M, Schulz R, Erbel R. Coronary microembolization: from bedside to bench and back to bedside. Circulation 120: 1822–1836, 2009. doi: 10.1161/CIRCULATIONAHA.109.888784. [DOI] [PubMed] [Google Scholar]
- 44.Heusch G, Libby P, Gersh B, Yellon D, Böhm M, Lopaschuk G, Opie L. Cardiovascular remodelling in coronary artery disease and heart failure. Lancet 383: 1933–1943, 2014. doi: 10.1016/S0140-6736(14)60107-0. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 45.Heusch G, Schulz R, Rahimtoola SH. Myocardial hibernation: a delicate balance. Am J Physiol Heart Circ Physiol 288: H984–H999, 2005. doi: 10.1152/ajpheart.01109.2004. [DOI] [PubMed] [Google Scholar]
- 46.Heusch G, Skyschally A, Gres P, van Caster P, Schilawa D, Schulz R. Improvement of regional myocardial blood flow and function and reduction of infarct size with ivabradine: protection beyond heart rate reduction. Eur Heart J 29: 2265–2275, 2008. doi: 10.1093/eurheartj/ehn337. [DOI] [PubMed] [Google Scholar]
- 47.Heusch G, Skyschally A, Kleinbongard P. Coronary microembolization and microvascular dysfunction. Int J Cardiol 258: 17–23, 2018. doi: 10.1016/j.ijcard.2018.02.010. [DOI] [PubMed] [Google Scholar]
- 48.Heyndrickx GR, Baig H, Nellens P, Leusen I, Fishbein MC, Vatner SF. Depression of regional blood flow and wall thickening after brief coronary occlusions. Am J Physiol 234: H653–H659, 1978. doi: 10.1152/ajpheart.1978.234.6.H653. [DOI] [PubMed] [Google Scholar]
- 49.Heyndrickx GR, Millard RW, McRitchie RJ, Maroko PR, Vatner SF. Regional myocardial functional and electrophysiological alterations after brief coronary artery occlusion in conscious dogs. J Clin Invest 56: 978–985, 1975. doi: 10.1172/JCI108178. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 50.Hoedemaker NP, Roolvink V, de Winter RJ, van Royen N, Fuster V, García-Ruiz JM, Er F, Gassanov N, Hanada K, Okumura K, Ibáñez B, van ’t Hof AW, Damman P. Early intravenous beta-blockers in patients undergoing primary percutaneous coronary intervention for ST-segment elevation myocardial infarction: A patient-pooled meta-analysis of randomized clinical trials. Eur Heart J Acute Cardiovasc Care. 2019 Feb 14 [Epub ahead of print]. doi: 10.1177/2048872619830609. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 51.Hort W. History of cardiovascular pathology. Z Kardiol 91, Suppl 4: 20–24, 2002. doi: 10.1007/s00392-002-1404-z. [DOI] [PubMed] [Google Scholar]
- 52.Ibáñez B, Heusch G, Ovize M, Van de Werf F. Evolving therapies for myocardial ischemia/reperfusion injury. J Am Coll Cardiol 65: 1454–1471, 2015. doi: 10.1016/j.jacc.2015.02.032. [DOI] [PubMed] [Google Scholar]
- 53.Ibanez B, Macaya C, Sánchez-Brunete V, Pizarro G, Fernández-Friera L, Mateos A, Fernández-Ortiz A, García-Ruiz JM, García-Álvarez A, Iñiguez A, Jiménez-Borreguero J, López-Romero P, Fernández-Jiménez R, Goicolea J, Ruiz-Mateos B, Bastante T, Arias M, Iglesias-Vázquez JA, Rodriguez MD, Escalera N, Acebal C, Cabrera JA, Valenciano J, Pérez de Prado A, Fernández-Campos MJ, Casado I, García-Rubira JC, García-Prieto J, Sanz-Rosa D, Cuellas C, Hernández-Antolín R, Albarrán A, Fernández-Vázquez F, de la Torre-Hernández JM, Pocock S, Sanz G, Fuster V. Effect of early metoprolol on infarct size in ST-segment-elevation myocardial infarction patients undergoing primary percutaneous coronary intervention: the Effect of Metoprolol in Cardioprotection During an Acute Myocardial Infarction (METOCARD-CNIC) trial. Circulation 128: 1495–1503, 2013. doi: 10.1161/CIRCULATIONAHA.113.003653. [DOI] [PubMed] [Google Scholar]
- 54.Jernberg T, Wallentin L, Alfredsson J, Hambraeus K, Hellström-Ängerud K, Kellerth T, Leosdottir M, Ravn-Fischer A, James S, Erlinge D. No changes in survival after acute myocardial infarction in the last decade. New data from SWEDEHEART. Munich, Germany: ESC Congress News 2018, 2018. [Google Scholar]
- 55.Klabunde RE. Cardiac electrophysiology: normal and ischemic ionic currents and the ECG. Adv Physiol Educ 41: 29–37, 2017. doi: 10.1152/advan.00105.2016. [DOI] [PubMed] [Google Scholar]
- 56.Kloner RA, Ganote CE, Jennings RB. The “no-reflow” phenomenon after temporary coronary occlusion in the dog. J Clin Invest 54: 1496–1508, 1974. doi: 10.1172/JCI107898. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 57.Lee JD, Tajimi T, Guth B, Seitelberger R, Miller M, Ross J Jr. Exercise-induced regional dysfunction with subcritical coronary stenosis. Circulation 73: 596–605, 1986. doi: 10.1161/01.CIR.73.3.596. [DOI] [PubMed] [Google Scholar]
- 58.Lim H, Fallavollita JA, Hard R, Kerr CW, Canty JM Jr. Profound apoptosis-mediated regional myocyte loss and compensatory hypertrophy in pigs with hibernating myocardium. Circulation 100: 2380–2386, 1999. doi: 10.1161/01.CIR.100.23.2380. [DOI] [PubMed] [Google Scholar]
- 59.Lindsey ML, Bolli R, Canty JM Jr, Du XJ, Frangogiannis NG, Frantz S, Gourdie RG, Holmes JW, Jones SP, Kloner RA, Lefer DJ, Liao R, Murphy E, Ping P, Przyklenk K, Recchia FA, Schwartz Longacre L, Ripplinger CM, Van Eyk JE, Heusch G. Guidelines for experimental models of myocardial ischemia and infarction. Am J Physiol Heart Circ Physiol 314: H812–H838, 2018. doi: 10.1152/ajpheart.00335.2017. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 60.Maroko PR, Kjekshus JK, Sobel BE, Watanabe T, Covell JW, Ross J Jr, Braunwald E. Factors influencing infarct size following experimental coronary artery occlusions. Circulation 43: 67–82, 1971. doi: 10.1161/01.CIR.43.1.67. [DOI] [PubMed] [Google Scholar]
- 61.Martin C, Schulz R, Rose J, Heusch G. Inorganic phosphate content and free energy change of ATP hydrolysis in regional short-term hibernating myocardium. Cardiovasc Res 39: 318–326, 1998. doi: 10.1016/S0008-6363(98)00086-8. [DOI] [PubMed] [Google Scholar]
- 62.Matsuzaki M, Gallagher KP, Kemper WS, White F, Ross J Jr. Sustained regional dysfunction produced by prolonged coronary stenosis: gradual recovery after reperfusion. Circulation 68: 170–182, 1983. doi: 10.1161/01.CIR.68.1.170. [DOI] [PubMed] [Google Scholar]
- 63.Matsuzaki M, Gallagher KP, Patritti J, Tajimi T, Kemper WS, White FC, Ross J Jr. Effects of a calcium-entry blocker (diltiazem) on regional myocardial flow and function during exercise in conscious dogs. Circulation 69: 801–814, 1984. doi: 10.1161/01.CIR.69.4.801. [DOI] [PubMed] [Google Scholar]
- 64.Matsuzaki M, Guth B, Tajimi T, Kemper WS, Ross J Jr. Effect of the combination of diltiazem and atenolol on exercise-induced regional myocardial ischemia in conscious dogs. Circulation 72: 233–243, 1985. doi: 10.1161/01.CIR.72.1.233. [DOI] [PubMed] [Google Scholar]
- 65.Matsuzaki M, Patritti J, Tajimi T, Miller M, Kemper WS, Ross J Jr. Effects of beta-blockade on regional myocardial flow and function during exercise. Am J Physiol 247: H52–H60, 1984. doi: 10.1152/ajpheart.1984.247.1.H52. [DOI] [PubMed] [Google Scholar]
- 66.Mills I, Fallon JT, Wrenn D, Sasken H, Gray W, Bier J, Levine D, Berman S, Gilson M, Gewirtz H. Adaptive responses of coronary circulation and myocardium to chronic reduction in perfusion pressure and flow. Am J Physiol 266: H447–H457, 1994. doi: 10.1152/ajpheart.1994.266.2.H447. [DOI] [PubMed] [Google Scholar]
- 67.Mosher P, Ross J Jr, McFate PA, Shaw RF. Control of coronary blood flow by an autoregulatory mechanism. Circ Res 14: 250–259, 1964. doi: 10.1161/01.RES.14.3.250. [DOI] [PubMed] [Google Scholar]
- 68.Ndrepepa G, Kastrati A, Mehilli J, Antoniucci D, Schömig A. Mechanical reperfusion and long-term mortality in patients with acute myocardial infarction presenting 12 to 48 hours from onset of symptoms. JAMA 301: 487–488, 2009. doi: 10.1001/jama.2009.32. [DOI] [PubMed] [Google Scholar]
- 69.Niccoli G, Scalone G, Crea F. Acute myocardial infarction with no obstructive coronary atherosclerosis: mechanisms and management. Eur Heart J 36: 475–481, 2015. doi: 10.1093/eurheartj/ehu469. [DOI] [PubMed] [Google Scholar]
- 70.Ong P, Camici PG, Beltrame JF, Crea F, Shimokawa H, Sechtem U, Kaski JC, Bairey Merz CN; Coronary Vasomotion Disorders International Study Group (COVADIS) . International standardization of diagnostic criteria for microvascular angina. Int J Cardiol 250: 16–20, 2018. doi: 10.1016/j.ijcard.2017.08.068. [DOI] [PubMed] [Google Scholar]
- 71.Page B, Young R, Iyer V, Suzuki G, Lis M, Korotchkina L, Patel MS, Blumenthal KM, Fallavollita JA, Canty JM Jr. Persistent regional downregulation in mitochondrial enzymes and upregulation of stress proteins in swine with chronic hibernating myocardium. Circ Res 102: 103–112, 2008. doi: 10.1161/CIRCRESAHA.107.155895. [DOI] [PubMed] [Google Scholar]
- 72.Qu J, Young R, Page BJ, Shen X, Tata N, Li J, Duan X, Fallavollita JA, Canty JM Jr. Reproducible ion-current-based approach for 24-plex comparison of the tissue proteomes of hibernating versus normal myocardium in swine models. J Proteome Res 13: 2571–2584, 2014. doi: 10.1021/pr5000472. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 73.Reimer KA, Jennings RB, Cobb FR, Murdock RH, Greenfield JC Jr, Becker LC, Bulkley BH, Hutchins GM, Schwartz RP Jr, Bailey KR, Passamani ER. Animal models for protecting ischemic myocardium: results of the NHLBI Cooperative Study. Comparison of unconscious and conscious dog models. Circ Res 56: 651–665, 1985. doi: 10.1161/01.RES.56.5.651. [DOI] [PubMed] [Google Scholar]
- 74.Roberts R, Croft C, Gold HK, Hartwell TD, Jaffe AS, Muller JE, Mullin SM, Parker C, Passamani ER, Poole WK, Raabe DS Jr, Rude RE, Stone PH, Turi ZG, Sobel BE, Willerson JT, Braunwald E. Effect of propranolol on myocardial-infarct size in a randomized blinded multicenter trial. N Engl J Med 311: 218–225, 1984. doi: 10.1056/NEJM198407263110403. [DOI] [PubMed] [Google Scholar]
- 75.Roolvink V, Ibanez B, Ottervanger JP, Pizarro G, van Royen N, Mateos A, Dambrink JHE, Escalera N, Lipsic E, Albarran A, Fernández-Ortiz A, Fernández-Avilés F, Goicolea J, Botas J, Remkes W, Hernandez-Jaras V, Kedhi E, Zamorano JL, Navarro F, Alfonso F, García-Lledó A, Alonso J, van Leeuwen M, Nijveldt R, Postma S, Kolkman E, Gosselink M, de Smet B, Rasoul S, Piek JJ, Fuster V, van ’t Hof AWJ. Early administration of intravenous beta blockers in patients with ST-elevation myocardial infarction before primary PCI. J Am Coll Cardiol 67: 2705–2715, 2016. doi: 10.1016/j.jacc.2016.03.522. [DOI] [PubMed] [Google Scholar]
- 76.Ross J Jr. Myocardial perfusion-contraction matching. Implications for coronary heart disease and hibernation. Circulation 83: 1076–1083, 1991. doi: 10.1161/01.CIR.83.3.1076. [DOI] [PubMed] [Google Scholar]
- 77.Schömig A, Mehilli J, Antoniucci D, Ndrepepa G, Markwardt C, Di Pede F, Nekolla SG, Schlotterbeck K, Schühlen H, Pache J, Seyfarth M, Martinoff S, Benzer W, Schmitt C, Dirschinger J, Schwaiger M, Kastrati A; Beyond 12 hours Reperfusion AlternatiVe Evaluation (BRAVE-2) Trial Investigators . Mechanical reperfusion in patients with acute myocardial infarction presenting more than 12 hours from symptom onset: a randomized controlled trial. JAMA 293: 2865–2872, 2005. doi: 10.1001/jama.293.23.2865. [DOI] [PubMed] [Google Scholar]
- 78.Schulz R, Guth BD, Heusch G. No effect of coronary perfusion on regional myocardial function within the autoregulatory range in pigs. Evidence against the Gregg phenomenon. Circulation 83: 1390–1403, 1991. doi: 10.1161/01.CIR.83.4.1390. [DOI] [PubMed] [Google Scholar]
- 79.Schulz R, Guth BD, Pieper K, Martin C, Heusch G. Recruitment of an inotropic reserve in moderately ischemic myocardium at the expense of metabolic recovery. A model of short-term hibernation. Circ Res 70: 1282–1295, 1992. doi: 10.1161/01.RES.70.6.1282. [DOI] [PubMed] [Google Scholar]
- 80.Schulz R, Miyazaki S, Miller M, Thaulow E, Heusch G, Ross J Jr, Guth BD. Consequences of regional inotropic stimulation of ischemic myocardium on regional myocardial blood flow and function in anesthetized swine. Circ Res 64: 1116–1126, 1989. doi: 10.1161/01.RES.64.6.1116. [DOI] [PubMed] [Google Scholar]
- 81.Schulz R, Post H, Neumann T, Gres P, Lüss H, Heusch G. Progressive loss of perfusion-contraction matching during sustained moderate ischemia in pigs. Am J Physiol Heart Circ Physiol 280: H1945–H1953, 2001. doi: 10.1152/ajpheart.2001.280.5.H1945. [DOI] [PubMed] [Google Scholar]
- 82.Schulz R, Rose J, Martin C, Brodde OE, Heusch G. Development of short-term myocardial hibernation. Its limitation by the severity of ischemia and inotropic stimulation. Circulation 88: 684–695, 1993. doi: 10.1161/01.CIR.88.2.684. [DOI] [PubMed] [Google Scholar]
- 83.Schwanke U, Deussen A, Heusch G, Schipke JD. Heterogeneity of local myocardial flow and oxidative metabolism. Am J Physiol Heart Circ Physiol 279: H1029–H1035, 2000. doi: 10.1152/ajpheart.2000.279.3.H1029. [DOI] [PubMed] [Google Scholar]
- 84.Skyschally A, Schulz R, Erbel R, Heusch G. Reduced coronary and inotropic reserves with coronary microembolization. Am J Physiol Heart Circ Physiol 282: H611–H614, 2002. doi: 10.1152/ajpheart.00797.2001. [DOI] [PubMed] [Google Scholar]
- 85.Smith TP Jr, Canty JM Jr. Modulation of coronary autoregulatory responses by nitric oxide. Evidence for flow-dependent resistance adjustments in conscious dogs. Circ Res 73: 232–240, 1993. doi: 10.1161/01.RES.73.2.232. [DOI] [PubMed] [Google Scholar]
- 86.Sorop O, Merkus D, de Beer VJ, Houweling B, Pistea A, McFalls EO, Boomsma F, van Beusekom HM, van der Giessen WJ, VanBavel E, Duncker DJ. Functional and structural adaptations of coronary microvessels distal to a chronic coronary artery stenosis. Circ Res 102: 795–803, 2008. doi: 10.1161/CIRCRESAHA.108.172528. [DOI] [PubMed] [Google Scholar]
- 87.Stirling MC, Choy M, McClanahan TB, Schott RJ, Gallagher KP. Effects of ischemia on epicardial segment shortening. J Surg Res 50: 30–39, 1991. doi: 10.1016/0022-4804(91)90006-8. [DOI] [PubMed] [Google Scholar]
- 88.Torry RJ, Myers JH, Adler AL, Liut CL, Gallagher KP. Effects of nontransmural ischemia on inner and outer wall thickening in the canine left ventricle. Am Heart J 122: 1292–1299, 1991. doi: 10.1016/0002-8703(91)90568-3. [DOI] [PubMed] [Google Scholar]
- 89.Traverse JH, Melchert P, Pierpont GL, Jones B, Crampton M, Bache RJ. Regulation of myocardial blood flow by oxygen consumption is maintained in the failing heart during exercise. Circ Res 84: 401–408, 1999. doi: 10.1161/01.RES.84.4.401. [DOI] [PubMed] [Google Scholar]
- 90.Vatner SF. Correlation between acute reductions in myocardial blood flow and function in conscious dogs. Circ Res 47: 201–207, 1980. doi: 10.1161/01.RES.47.2.201. [DOI] [PubMed] [Google Scholar]
- 91.Weil BR, Young RF, Shen X, Suzuki G, Qu J, Malhotra S, Canty JMJ Jr. Brief myocardial ischemia produces cardiac troponin I release and focal myocyte apoptosis in the absence of pathological infarction in swine. JACC Basic Transl Sci 2: 105–114, 2017. doi: 10.1016/j.jacbts.2017.01.006. [DOI] [PMC free article] [PubMed] [Google Scholar]