

Abstract
Purpose
This study aims to record the current pattern of third molar impactions and relevant reasons for extraction in Riyadh, Saudi Arabia. We hypothesized that the principal reason for extraction was elective.
Material and Methods
Orthopantomograms (OPG) radiographs and electronic files relating to 4000 patients were retrospectively collected from patients between the ages of 21 and 50 years old. Of these, 1014 were included in this study (514 females, 500 males). The classification was determined according to the Winter, Pell, and Gregory classification. The analysis was done using the chi-square (χ2) test, with SPSS version 25 (IBM, Inc, Chicago, IL). A p-value of < 0.05 was considered statistically significant.
Results
A total of 2240 impacted third molars were found with no gender predilection. Impaction was more commonly found in the mandible (58.5%) than the maxilla (41.5%). The most common reason for extraction was ‘asymptomatic; prophylactic indication’ (66.8%), followed by ‘symptomatic’ (33.2%). Vertical angulation was most common in the maxilla (56.5%), and mesioangular impaction in the mandible (40.5%).
Conclusion
There is a high rate of third molar impaction in the central region of Saudi Arabia. It is more likely to occur in the mandible than the maxilla with no gender predilection. The majority of the patients were referred for elective asymptomatic reasons. Mesio-angular impaction is mostly found in the mandible and vertical angulation in the maxilla. Both arches had a C level depth and Class I Ramus relationship. Further studies should be conducted with the wider Kingdom of Saudi Arabia so that the population can be more accurately represented.
Keywords: Third molar, Impacted, Prevalence, Extraction, Saudi Arabia, Winter classification, Pell and Gregory classification, Referral
1. Introduction
The term impacted tooth defines a tooth’s failure to erupt within the expected amount of time into the dental arch unless intervened with treatment (Mustafa, 2015). Failure to erupt, followed by impaction is a common dental anomaly (Akarslan and Kocabay, 2009, Bishara and Andreasen, 1983, Fardi et al., 2011, Hashemipour et al., 2013, van der Linden et al., 1995). Interestingly, the incidence of impacted teeth differs across different populations and ethnic groups (Bishara and Ortho, 1992). This failure of the eruption could be due to many systemic and local factors, such as cleidocranial dysplasia, Down’s syndrome, and arch-length deficiency (Hassan, 2010). There is a correlation between the development of pericoronitis, cystic lesions, and caries with impacted teeth (Al-Anqudi et al., 2014). Moreover, third molars have been found to be the most commonly impacted teeth in the oral cavity (Bishara and Andreasen, 1983, van der Linden et al., 1995).
In the Pell & Gregory classification system, third molar impaction is classified according to its depth level in relation to the occlusal surface of the second molar vertically, and the relation of the impaction to the body of the Ramus horizontally (Pell and Gregory, 1933). As for angulation, third molar impaction was classified by the Winter’s classification system in 1926 (Winter, 1926).
In Saudi Arabia, the latest assessment of third molar impactions was published more than 30 years ago (Haidar and Shalhoub, 1986) However, recently there have not been any articles that discuss this matter, and none which target the central area of Saudi Arabia. This study aims to record the current occurrence pattern of third molar impactions and the relevant extraction reasons in a sample living in Riyadh, Saudi Arabia
We hypothesize that the principal reason for extraction is elective. The results of this study can help to achieve more relevant information, of many factors, such as gender, age, systemic disease, number of areas and angulation, and pathological occurrence.
2. Materials and methods
In this study, retrospective data were collected on 4000 patients between the ages of 21 and 50 years old who visited the Riyadh Elm University dental clinics between the years of 2015–2017 and had an electronic record. Of the 4000 patients screened, 1014 were included in the study as they had at least 1 impacted third molar. (514 females, 500 males). The data were collected from all branches of Riyadh Elm University which are located in three different districts in Riyadh city.
The estimated eruption time of third molars ranges between the ages of 17 and 21 years old. Since our study targets impacted third molars, patients less than 21 years old were excluded from this study. Other exclusion criteria included syndromes (such as Down’s syndrome), if they had received orthodontic treatment, had craniofacial anomalies, incomplete root formation of the third molars, or were higher than ASA III under the Society of Anesthesiologists (ASA) classification. Data was collected by examining the patients’ Orthopantomograms (OPG) radiographs and accessing their electronic files which included the details of each procedure and electronic referral forms, which includes the referral reasons. As these OPG radiographs were taken with routine documentation during treatment, no consent form was required. Approval was given to conduct this study from the Riyadh Elm University Institutional Review Board. Patients were also interviewed over the phone for further confirmation regarding their referral/extraction reason and diagnosis.
The reason for extraction was classified as either symptomatic or asymptomatic. Symptomatic third molars were considered to be those that triggered pain or impaired mastication and/or were associated with a cyst or tumor lesions.
The angle was assessed using the Winter Classification, which measures the angle formed between the long axis of the third molar and the second molar, relatively with an orthodontic protractor (Fig. 1a). The impaction was classified using the Pell & Gregory Classification system for the depth of the third molar’s cementoenamel junction (CEJ) level in the alveolar bone compared to the second molar (Fig. 1b). and to classify the impaction in relation to the anterior border of the Ramus (Fig. 1c).
Fig. 1.

(a) The Winter classification for impacted third molar angulation. (b) The Pell and Gregory Classification of impacted third molar depth in relation to the cementoenamel junction of the second molar. (c) The Pell and Gregory Classification of impacted third molars in relation to the anterior border of the Ramus.
The analysis was done using the chi-square (χ2) test, with SPSS version 25 (IBM, Inc, Chicago, IL). A p-value of < 0.05 was considered statistically significant.
3. Results
Of the 4000 samples reviewed, a total of 1014 patients were found to have 3840 third molars. Of these, 1600 were erupted 41.6% and 2240 were impacted 58.3%. (514 females and 500 males).
The distribution of the impaction between the two genders was almost equal, with 50.7% being females and 49.3% males. The average age was 30.67 ± 8.98 years (p = 0.007). The majority of participants were classified as ASA I (97.8%). Patients more commonly had 2 impacted third molars (35.3%), with the least common being 3 impacted molars (15%, p = 0.00) (Table 1).
Table 1.
Distribution by the number of impaction.
| Number of Impaction | N (%) |
|---|---|
| 1 | 313 (30.9) |
| 2 | 358 (35.3) |
| 3 | 152 (15.0) |
| 4 | 191 (18.8) |
| Total | 1014 (1 0 0) |
| Asymp. sig. (2-tailed)* = 0.000 | |
Asymp. Sig., asymptotic significance.
Also, (Table 2) displays the distribution of the impaction per tooth in regards to the upper and lower jaw. The majority were found in the mandible (58.5%), with less in the maxilla 41.5% (p = 0.018). There was statistical significance between prevalence in the right (59.9%) and left sides (40.1%, p = 0.000).
Table 2.
Distribution of impacted teeth in terms of arch location and gender.
| Gender N (%) | Maxilla N (%) | Mandible N (%) | Total N (%) | |
|---|---|---|---|---|
| Male | 500 (49.3) | 399 (38.6) | 634 (61.4) | 1207 (100) |
| Female | 514 (50.7) | 530 (43.9) | 677 (56.1) | 1033 (100) |
| Total | 1014 (1 0 0) | 929 (41.5) | 1311 (58.5) | 2240 (100) |
| Asymp. sig. (2-tailed)* = 0.011 | ||||
Asymp. Sig., asymptotic significance.
Patients were contacted and asked as to whether they had extracted their impacted teeth and their files were checked for their referral status. From this, 73.2% of patients were not referred for extraction, while 26.8% were. Furthermore, almost all patients that were referred for an extraction have extracted their teeth (91.9%, p = 0.000).
Fig. 2 demonstrates the given extraction reasons from patients. Of these, “asymptomatic; prophylactic indication” was the most common reason at 66.8%, followed by “symptomatic” at 33.2%. On the contrary, 98.8% of those who had not undergone an extraction had “Not indicated” as the main reason for retaining the impacted third molar (Fig. 3).
Fig. 2.
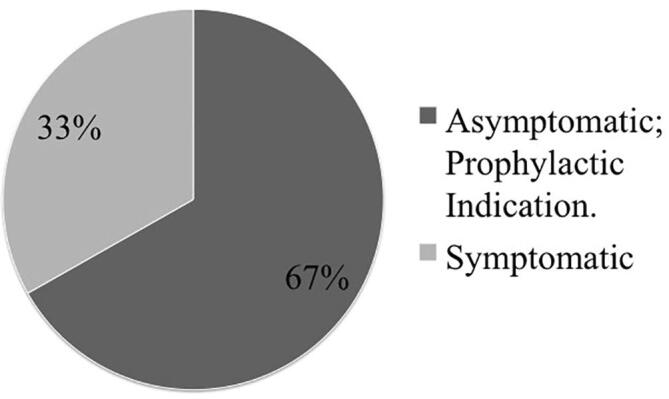
Patients' responses to the reason for extraction.
Fig. 3.
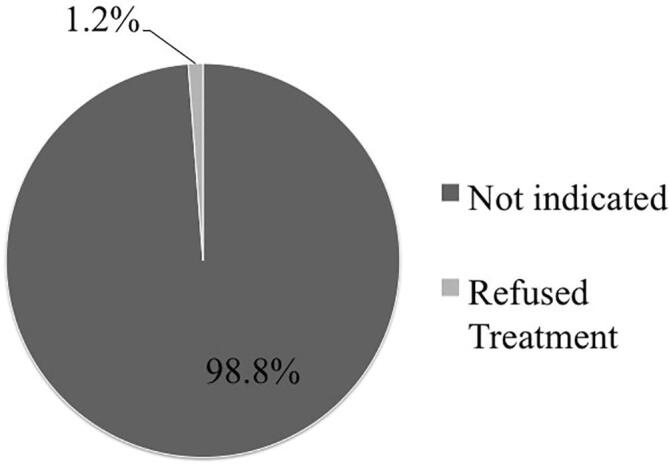
The given reasons for retaining the third molars.
The angulation of impaction was also evaluated (Table 3). Vertical angulation was most frequently found in the maxilla (56.5%), which was followed by disto-angular (31.9%). In the mandible, the most common angulation was mesioangular (40.5%), which was followed by vertical angulation (32.0%, p = 0.000).
Table 3.
Distribution of impacted teeth in term of angulation.
| Angle Classification (Winter’s) N (%) | |||||||
|---|---|---|---|---|---|---|---|
| Location | Vertical | Mesio-angular | Horizontal | Disto-angular | Buccolingual | Inverted | Total |
| Maxilla | 525 (56.5) | 75 (8.1) | 9 (1.0) | 296 (31.9) | 20 (2.2) | 4 (0.4) | 929 (100) |
| Mandible | 420 (32.0) | 531 (40.5) | 302 (23.0) | 41 (3.1) | 11 (0.8) | 6 (0.5) | 1311 (100) |
| Total | 945 (42.2) | 606 (27.1) | 311 (13.9) | 337 (15.0) | 31 (1.4) | 10 (0.4) | 2240 (100) |
| Asymp. sig. (2-tailed)* = 0.000 | |||||||
Asymp. Sig., asymptotic significance.
The different impaction levels are displayed in (Table 4) according to the Pell & Gregory classification. The C level impaction depth was found to be most prevalent in both the mandible and maxilla with 57.3% (p = 0.000). The Ramus relationship classification showed that 66.7% had a class I relationship in both the right and left side of the mandible. (p = 0.011).
Table 4.
Distribution of impaction in term of depth, mandible ramus relationship.
| Impaction Depth (Pell & Gregory) N (%) | ||||
|---|---|---|---|---|
| Location | Level A | Level B | Level C | Total |
| Maxilla | 19 (2.0) | 333 (35.8) | 577 (62.1) | 929 (100) |
| Mandible | 270 (20.6) | 334 (25.5) | 707 (53.9) | 1311 (100) |
| Total | 289 (12.9) | 667 (29.8) | 1284 (57.3) | 2240 (100) |
| Asymp. sig. (2-tailed)* = 0.000 | ||||
| Class I | Class II | Class III | Total | |
| Mandible | 874 (66.7) | 359 (27.4) | 78 (5.9) | 1311 (100) |
| Asymp. sig. (2-tailed)* = 0.011 | ||||
Asymp. Sig., asymptotic significance.
The type of impaction was assessed. This included whether it was fully or only partially impacted and whether the type of overlying tissue was a soft tissue or bony impaction (Table 5). In both jaws full impaction was more prevalent (78.1%) as was completely bony (68.8%, p = 0.000).
Table 5.
Distribution of impaction in terms of type and overlying tissue.
| Impaction Type N (%) | |||
|---|---|---|---|
| Location | Fully Impacted | Partially Impacted | Total |
| Maxilla | 887 (95.5) | 42 (4.5) | 929 (100) |
| Mandible | 862 (65.8) | 449 (34.2) | 1311 (100) |
| Total | 1749 (78.1) | 491 (21.9) | 2240 (100) |
| Asymp. sig. (2-tailed)* = 0.000 | |||
| Location | Bony | Soft Tissue | Total |
| Maxilla | 603 (64.9) | 326 (35.1) | 929 (100) |
| Mandible | 939 (71.6) | 372 (28.4) | 1311 (100) |
| Total | 1542 (68.8) | 698 (31.2) | 2240 (100) |
| Asymp. sig. (2-tailed)* = 0.000 | |||
Asymp. Sig., asymptotic significance.
When evaluating the OPGs for the pathological involvement of an impacted third molar, only 25 patients out of 1014 were found to be associated with a pathological lesion (cyst).
4. Discussion
In a large sample of the population, the chances of finding one or more impacted third molar is quite high. According to Othman R et al., third molars are the most common impacted teeth to be found in humans and their surgical extraction is one of the most common dentoalveolar surgical procedures in the oral maxillofacial surgical field (Jaffar and Tin-Oo , 2009). Multiple factors could be responsible for its etiology (M. and J, 2004, Syed et al., 2013) Therefore, understanding its pattern in various communities is very important (Kumar Pillai et al., 2014).
When evaluating an impacted third molar radiographically, the angulation of the molar should be determined according to the Winter’s classification (Winter, 1926). As well as the depth level in the bone, the relationship of the tooth to the Ramus of the mandible, and the second molar, should be included according to the Pell and Gregory Classification (Pell and Gregory, 1933, Ayrancı et al., 2017).
Other measures were taken in assessing the impaction, such as the association of pathological lesions (cysts, tumor) around the impacted tooth. The normal pericoronal dental follicle is considered to be 2–3 mm radiographically. The evidence of radiolucency around the crown of an unerupted tooth ≥ 5 mm in size is highly suggestive of a dentigerous cyst or odontogenic tumor (Mesgarzadeh et al., 2008, Winter, 1926).
Previously, the prevalence of third molar impactions and its pattern have been studied in different parts of the world by different authors like, (Haidar and Shalhoub, 1986) in Saudi Arabia, (Kumar Pillai et al., 2014) in India, (Arabion et al., 2017) in Iran, and many other countries (Amanat et al., 2014, Ahlqwist and Gröndahl, 1991, Al-Anqudi et al., 2014, Yilmaz et al., 2016). The pattern and prevalence have also been studied in different areas located in Saudi Arabia (El-Khateeb et al., 2015, Haidar and Shalhoub, 1986, Hassan, 2010, Syed et al., 2013).
Our study targets the incidence of impacted teeth in a sample living in the central part of Saudi Arabia. The percentage of impaction found in our sample was 58.3% which is higher than 31.9% that was found by Haidar and Shalhoub (1986) and a study in India (Kumar Pillai et al., 2014). These differences could be due to the sample size.
The mean age, when diagnosed, was 30.67 ± 8.98 years, although it has been shown to slightly differ from 23.25 ± 4.17 years (Arabion et al., 2017) and 28.11 ± 7.25 years (Hassan, 2010).
The impaction incidence between the two genders was found to be almost equal (50.7% females and 49.3% males). This finding agrees with studies done by Haidar and Shalhoub (1986), Hassan (2010), and disagreed with (Quek et al., 2003, Syed et al., 2013) who reported that males were more likely to have impacted teeth. This result could be due to the different growth patterns between the two genders. Females jaw growth, for the most part, ends by the time the third molar erupts. Nevertheless, the jaw growth in males sustains during the eruption of the third molar, giving adequate space for the third molar to erupt (Arabion et al., 2017, Bishara and Andreasen, 1983)
Having at least 1 impacted third molar was the most commonly found in previous studies concluded by Arabion et al. (2017), Hassan (2010). This is in disagreement with our study, which found that having at least 2 impacted third molars, 35.5% was the most common result. This is likely due to the mean age being higher in our study compared to the studies mentioned above.
Furthermore, when comparing the distribution of impaction between the two jaws, our study showed this was higher in the lower jaw (58.5%) than in the upper jaw (41.5%). This finding is in agreement with (Ayrancı et al., 2017, Kumar Pillai et al., 2014) who noted that impaction is 1.33 more likely to happen in the mandible than the maxilla. However, it was the opposite of one study that was conducted by Hattab et al. (1995) who found impaction to be 54% higher in the maxilla.
We found statistical significance between the two sides having the right side more common with 59.9% (p = 0.018), which was found in a previous study as insignificant (Kaomongkolgit and Tantanapornkul, 2017).
Steed (2014) mentioned that practitioners should be extracting impacted third molars when they cause a considerable amount of pain, infection, caries, affect the adjacent second molar or interfere with prosthetic or orthodontic treatments. Also, there are guidelines regarding the indications for impacted third molar extractions set by the National Institute for Clinical Excellence (NICE, 2000). However, evidence to support whether to extract or retain asymptomatic, disease-free impacted third molars is lacking. Many studies have debated whether the extraction of asymptomatic impacted third molars is necessary (Assael, 2005, Steed, 2014).
Previous studies gave the main reason for extraction as pericoronitis, such as (Gbotolorun et al., 2007, Nordenram et al., 1987). In Nordenram et al., 60% were diagnosed with pericoronitis and 4.5% had cysts related to the impaction.
Taking that into consideration, our study focused on the extraction reason and whether patients were referred for an elective reason or an extraction was required. Our results show that 73.2% of our sample was not referred on as 98.8% of them were not indicated for an extraction. Nevertheless, patients who were referred for extraction had ‘Asymptomatic; Prophylactic indication’ as the most prevalent reason (66.8%), which was followed by ‘Symptomatic’ (33.2%).
Additionally, a number of studies observed that vertical angulation is most common in both the maxilla and the mandible (Ayrancı et al., 2017, Šečić et al., 2013). While others reported that mesioangular impaction was the most common pattern of angulation in both jaws (Arabion et al., 2017). However, in this present study vertical angulation was found to be most common in the maxilla (56.5%) and mesioangular impaction was most common in mandibular impaction (40.5%). These results agree with a previous study done in the western region of Saudi Arabia by Hassan (2010) and (Kaomongkolgit and Tantanapornkul, 2017) in Thailand. Meanwhile, Arabion et al. (2017) found that mesioangular impaction was the most common in the mandible, but that disto-angular impaction was more common in the maxilla.
According to the Pell and Gregory classification, the most recurrent depth level in our study was level C in both jaws (57.3%). Other studies showed level B to be more prevalent Hassan (2010), Kaomongkolgit and Tantanapornkul (2017). Furthermore, multiple studies noted class II Ramus classification was the most common (El-Khateeb et al., 2015, Kaomongkolgit and Tantanapornkul, 2017). However, in our study, only class I (66.7%) was statistically significant (p = 0.008).
Third molar impaction can be classified into; (1) partial impaction, where the crown penetrates the mucosa and is partially visible; (2) full impaction, where the tooth is not visible in the oral mucosa. An impacted third molar that is fully enclosed in the jaw’s bone is considered a bony impaction. A soft tissue impaction is considered when the crown of the impacted molar has penetrated the bone but is enclosed in soft tissue (Kaifu et al., 2003). The majority of impaction classified in our study, according to the main overlying tissue, was found to be bony and fully impacted 78.1%, 68.8%, respectively (Bui et al., 2003). observed that this was the most common surgical extraction.
Odontogenic cysts and tumors (>3 mm width) associated with impactions have been observed in multiple studies even though they are quite rare (Nunn et al., 2013, Santosh, 2015, Steed, 2014). 2.5% of patients in our study were found to have some pathological association with their third molar. Of the patients with such pathological changes, 94.4% of them were referred to a surgeon, and their molars extracted.
We recommend further studies should be conducted with the wider Kingdom of Saudi Arabia so that the population can be more accurately represented. Additionally, all dentists should refer back to evidence-based guidelines before referring patients for an extraction.
5. Conclusion
-
(1)
There is a high rate of third molar impactions in the central region of Saudi Arabia. These are more likely to be in the mandible than the maxilla with no gender predilection.
-
(2)
The majority of patients were referred for elective asymptomatic reasons.
-
(3)
Mesio-angular impaction is mostly found in the mandible and vertical angulation in the maxilla.
-
(4)
Both arches had a C level depth and Class I Ramus relationship.
Declaration of Competing Interest
The authors have no conflicts of interest to declare.
Footnotes
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for profit sectors.
Peer review under responsibility of King Saud University.
References
- Ahlqwist M., Gröndahl H.-G. Prevalence of impacted teeth and associated pathology in middle-aged and older Swedish women. Commun. Dent. Oral Epidemiol. 1991 doi: 10.1111/j.1600-0528.1991.tb00124. [DOI] [PubMed] [Google Scholar]
- Akarslan, Z.Z., Kocabay, C., 2009. Assessment of the associated symptoms, pathologies, positions and angulations of bilateral occurring mandibular third molars: Is there any similarity? Oral Surg., Oral Med. Oral Pathol. Oral Radiol. Endodontol. https://doi.org/10.1016/j.tripleo.2009.05.036. [DOI] [PubMed]
- Al-Anqudi, S.M., Al-Sudairy, S., Al-Hosni, A., Al-Maniri, A., 2014. Prevalence and pattern of third molar impaction: a retrospective study of radiographs in Oman. Sultan Qaboos Univ. Med. J. [PMC free article] [PubMed]
- Amanat N., Mirza D., Rizvi K.F. Pattern of third molar impaction: frequency and types among patients attending urban teaching hospital of Karachi. Pakistan Oral Dental J. 2014;34(1) [Google Scholar]
- Arabion H., Gholami M., Dehghan H., Khalife H. Prevalence of impacted teeth among young adults: a retrospective radiographic study. J. Dental Mater. Tech. 2017;6(3):131–137. doi: 10.22038/jdmt.2017.8940. [DOI] [Google Scholar]
- Assael, L.A., 2005. Indications for elective therapeutic third molar removal: The evidence is in. J. Oral Maxillofac. Surg. https://doi.org/10.1016/j.joms.2005.10.001. [DOI] [PubMed]
- Ayrancı F., Omezli M.M., Sivrikaya E.C., Rastgeldi Z. Prevalence of third molar impacted teeth: a cross-sectional study evaluating radiographs of adolescents. J. Clin. Exp. Invest./Klinik ve Deneysel Arastirmalar Dergisi. 2017;8(2) [Google Scholar]
- Bishara S.E., Andreasen G. Third molars: a review. Am. J. Orthod. 1983 doi: 10.1016/S0002-9416(83)90298-1. [DOI] [PubMed] [Google Scholar]
- Bishara S.E., Ortho D. Impacted maxillary canines: a review. Am. J. Orthod. Dentofac. Orthop. 1992 doi: 10.1016/0889-5406(92)70008-X. [DOI] [PubMed] [Google Scholar]
- Bui C.H., Seldin E.B., Dodson T.B. Types, frequencies, and risk factors for complications after third molar extraction. J. Oral Maxillofac. Surg. 2003 doi: 10.1016/j.joms.2003.04.001. [DOI] [PubMed] [Google Scholar]
- El-Khateeb S.M., Arnout E.A., Hifnawy T. Radiographic assessment of impacted teeth and associated pathosis prevalence: pattern of occurrence at different ages in Saudi Male in Western Saudi Arabia. Saudi Med. J. 2015 doi: 10.15537/smj.2015.8.12204. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Fardi A., Kondylidou-Sidira A., Bachour Z., Parisis N., Tsirlis A. Incidence of impacted and supernumerary teeth - a radiographic study in a North Greek population. Med. Oral Patol. Oral Cir. Bucal. 2011 doi: 10.4317/medoral.16.e56. [DOI] [PubMed] [Google Scholar]
- Gbotolorun O.M., Olojede A.C., Arotiba G.T., Ladeinde A.L., Akinwande J.A., Bamgbose B.O. Impacted mandibular third molars: presentation and postoperative complications at the Lagos University Teaching Hospital. Nig Q. J. Hosp. Med. 2007 doi: 10.4314/nqjhm.v17i1.12537. [DOI] [PubMed] [Google Scholar]
- Haidar, Z., Shalhoub, S.Y., 1986. The incidence of impacted wisdom teeth in a Saudi community. Int. J. Oral Maxillofac. Surg. https://doi.org/10.1016/S0300-9785(86)80060-6. [DOI] [PubMed]
- Hashemipour M.A., Tahmasbi-Arashlow M., Fahimi-Hanzaei F. Incidence of impacted mandibular and maxillary third molars: a radiographic study in a southeast iran population. Med. Oral Patol. Oral Cir. Bucal. 2013 doi: 10.4317/medoral.18028. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hassan, A.H., 2010. Pattern of third molar impaction in a Saudi population. Clin. Cosmet. Investig. Dent. https://doi.org/10.2147/cciden.s12394. [DOI] [PMC free article] [PubMed]
- Hattab, F.N., Rawashdeh, M.A., Fahmy, M.S., 1995. Impaction status of third molars in Jordanian students. Oral Surgery, Oral Med. Oral Pathol. Oral Radiol. https://doi.org/10.1016/S1079-2104(05)80068-X. [DOI] [PubMed]
- Kaifu, Y., Kasai, K., Townsend, G.C., Richards, L.C., 2003. Tooth Wear and the “Design” of the Human Dentition: A Perspective from Evolutionary Medicine. Am. J. Phys. Anthropol. https://doi.org/10.1002/ajpa.10329. [DOI] [PubMed]
- Kaomongkolgit, R., Tantanapornkul, W., 2017. Pattern of impacted third molars in Thai population: Retrospective radiographic survey. J. Int. Dent. Med. Res.
- Kumar Pillai, A., Thomas, S., Paul, G., Singh, S.K., Moghe, S., 2014. Incidence of impacted third molars: A radiographic study in People’s Hospital, Bhopal, India. J. Oral Biol. Craniofacial Res. https://doi.org/10.1016/j.jobcr.2014.04.001. [DOI] [PMC free article] [PubMed]
- Linden, W. van der, Cleaton-Jones, P., Lownie, M., 1995. Diseases and lesions associated with third molars. Review of 1001 cases. Oral Surg., Oral Med. Oral Pathol. Oral Radiol. https://doi.org/10.1016/S1079-2104(05)80270-7. [DOI] [PubMed]
- M., S., J., R., 2004. Maxillary impacted canine with congenitally absent premolars. Angle Orthod. [DOI] [PubMed]
- Mesgarzadeh, A., Esmailzadeh, H., Abdolrahimi, M., Shahamfar, M., 2008. Pathosis associated with radiographically normal follicular tissues in third molar impactions: A clinicopathological study. Indian J. Dent. Res. https://doi.org/10.4103/0970-9290.42952. [DOI] [PubMed]
- Mustafa, A.B., 2015. Prevalence of Impacted Pre-Molar Teeth in College of Dentistry, King Khalid University, Abha, Kingdom of Saudi Arabia. J. Int. oral Heal. JIOH. [PMC free article] [PubMed]
- National Institute for Clinical Excellence Guidance on the extraction of wisdom teeth. Online article available at. 2000 http://egap.evidence.nhs.uk/guidance-on-the-extraction-of-wisdom-teeth-ta1 [Google Scholar]
- Nordenram, A., Hultin, M., Kjellman, O., Ramström, G., 1987. Indications for surgical removal of the mandibular third molar. Study of 2,630 cases. Swed. Dent. J. [PubMed]
- Nunn, M.E., Fish, M.D., Garcia, R.I., Kaye, E.K., Figueroa, R., Gohel, A., Ito, M., Lee, H.J., Williams, D.E., Miyamoto, T., 2013. Retained Asymptomatic Third Molars and Risk for Second Molar Pathology. J. Dent. Res. https://doi.org/10.1177/0022034513509281. [DOI] [PMC free article] [PubMed]
- Pell, G.J., Gregory, G.T., 1933. Impacted mandibular third molars: classification and modified technique for removal. Dent. Dig.
- Quek, S.L., Tay, C.K., Tay, K.H., Toh, S.L., Lim, K.C., 2003. Pattern of third molar impaction in a Singapore Chinese population: A retrospective radiographic survey. Int. J. Oral Maxillofac. Surg. https://doi.org/10.1054/ijom.2003.0413. [PubMed]
- Rosfaima Othman Jaffar, Tin-Oo M.M., 2009. Impacted mandibular third molars among patients attending Hospital Universiti Sains Malaysia. Arch. Orofac. Sci.
- Santosh, P., 2015. Impacted mandibular third molars: Review of literature and a proposal of a combined clinical and radiological classification. Ann. Med. Health Sci. Res. https://doi.org/10.4103/2141-9248.160177. [DOI] [PMC free article] [PubMed]
- Šečić, S., Prohić, S., Komšić, S., Vuković, A., 2013. Incidence of impacted mandibular third molars in population of Bosnia and Herzegovina: a retrospective radiographic study. J. Heal. Sci. https://doi.org/10.17532/jhsci.2013.80
- Steed, M.B., 2014. The indications for third-molar extractions. J. Am. Dent. Assoc. https://doi.org/10.14219/jada.2014.18. [DOI] [PubMed]
- Syed, K.B., Zaheer, K.B., Ibrahim, M., Bagi, M.A., Assiri, M.A., 2013. Prevalence of Impacted Molar Teeth among Saudi Population in Asir Region, Saudi Arabia - A Retrospective Study of 3 Years. J. Int. oral Heal. JIOH. [PMC free article] [PubMed]
- Winter, G.B., 1926. Impacted mandibular third molar. St. Louis: American Medical Book, 41.
- Yilmaz, S., Adisen, M.Z., Misirlioglu, M., Yorubulut, S., 2016. Assessment of Third Molar Impaction Pattern and Associated Clinical Symptoms in a Central Anatolian Turkish Population. Med. Princ. Pract. https://doi.org/10.1159/000442416 [DOI] [PMC free article] [PubMed]